
Clinicopathologic Characteristics Associated with Prognosis in Ocular Extranodal Marginal Zone B Cell Lymphoma

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Features
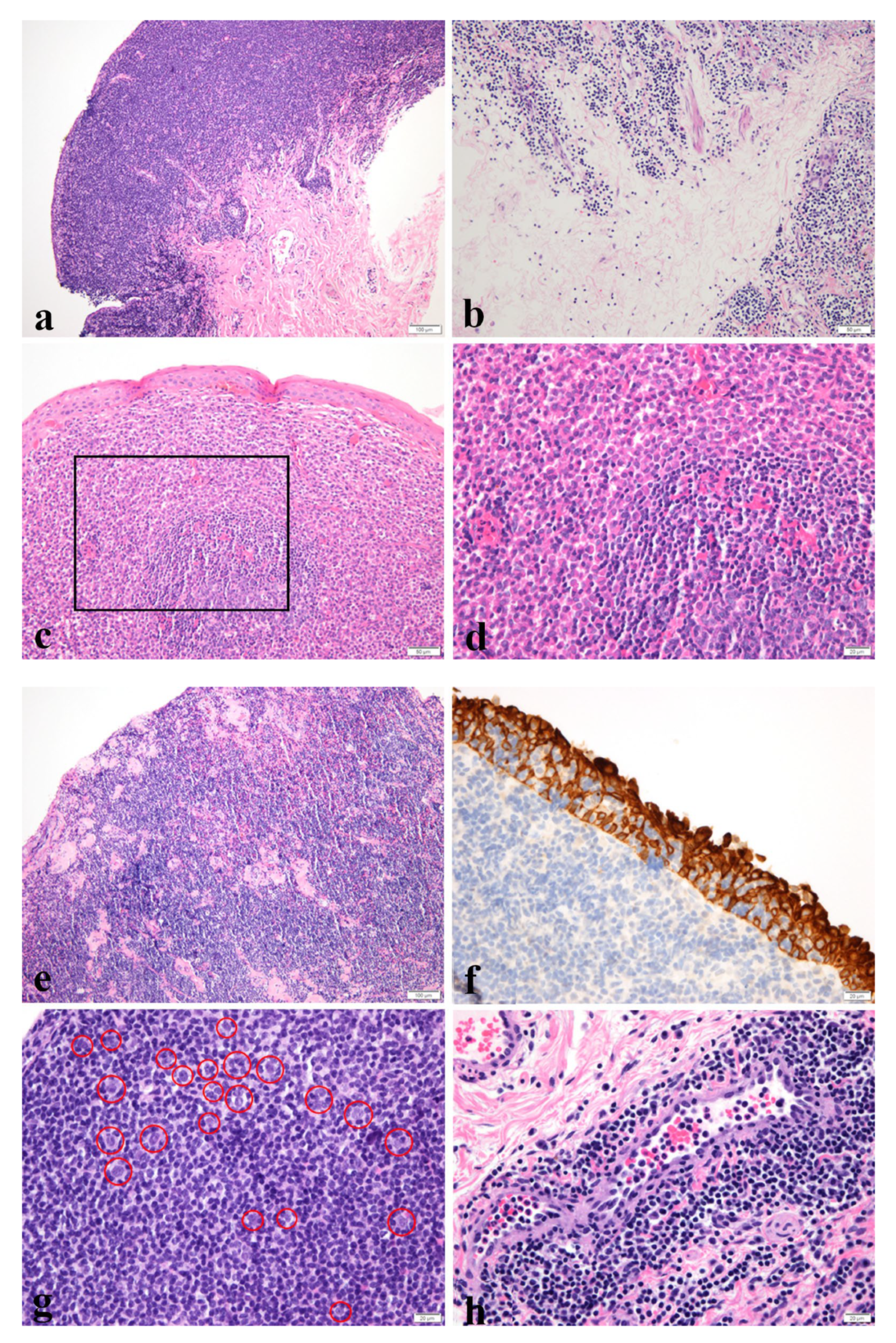
2.2. Histological Features
2.2.1. Confluent or Nonconfluent
2.2.2. Plasma Cells
2.2.3. Sclerosis
2.2.4. Lymphoepithelial Lesion
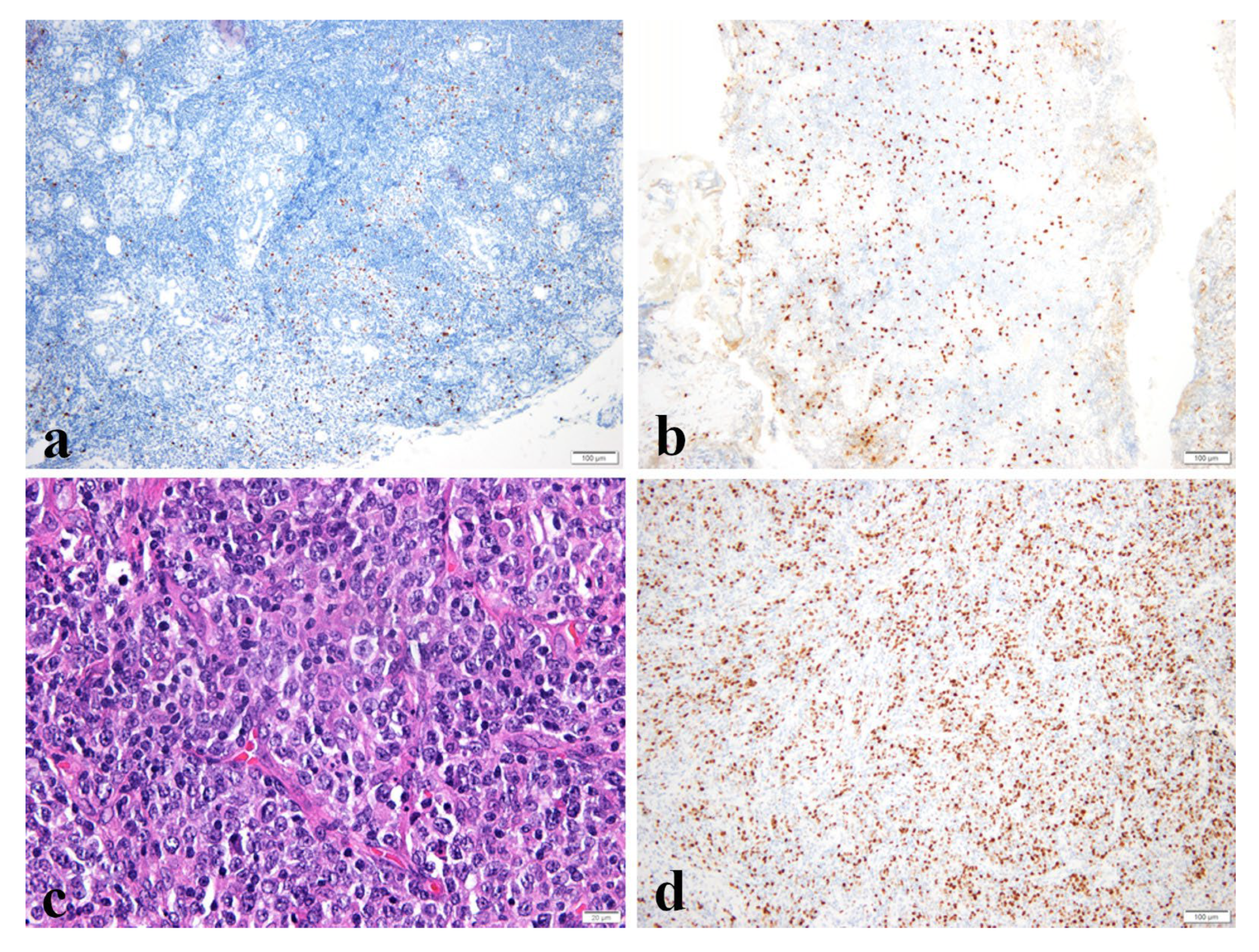
2.2.5. Large Cell Change
2.2.6. Lymphovascular Invasion
2.3. Immunohistochemistry
2.3.1. Ki-67 Labeling Index
2.3.2. IgG4/IgG Ratio
2.4. IgH Gene Rearrangement Study
2.5. Treatment and Follow-Up
2.6. Statistical Analysis
3. Results
3.1. Clinicopathologic Characteristics of Patients
3.2. Clinicopathologic Characteristics and Risk Factors for Non-CR in Conjunctiva and Non-Conjunctiva Groups
3.3. Clinicopathologic Characteristics in Recurred Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shields, C.L.; Chien, J.L.; Surakiatchanukul, T.; Sioufi, K.; Lally, S.E.; Shields, J.A. Conjunctival Tumors: Review of Clinical Features, Risks, Biomarkers, and Outcomes—The 2017 J. Donald M. Gass Lecture. Asia-Pac. J. Ophthalmol. 2017, 6, 109–120. [Google Scholar] [CrossRef]
- Verdijk, R.M. Lymphoproliferative Tumors of the Ocular Adnexa. Asia-Pac. J. Ophthalmol. 2017, 6, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Olsen, T.G.; Holm, F.; Mikkelsen, L.H.; Rasmussen, P.K.; Coupland, S.E.; Esmaeli, B.; Finger, P.T.; Graue, G.F.; Grossniklaus, H.E.; Honavar, S.G.; et al. Orbital Lymphoma-An International Multicenter Retrospective Study. Am. J. Ophthalmol. 2019, 199, 44–57. [Google Scholar] [CrossRef]
- Oh, D.E.; Kim, Y.D. Lymphoproliferative diseases of the ocular adnexa in Korea. Arch. Ophthalmol. 2007, 125, 1668–1673. [Google Scholar] [CrossRef] [Green Version]
- Ferry, J.A.; Fung, C.Y.; Zukerberg, L.; Lucarelli, M.J.; Hasserjian, R.P.; Preffer, F.I.; Harris, N.L. Lymphoma of the ocular adnexa: A study of 353 cases. Am. J. Surg. Pathol. 2007, 31, 170–184. [Google Scholar] [CrossRef] [PubMed]
- Kirkegaard, M.M.; Rasmussen, P.K.; Coupland, S.E.; Esmaeli, B.; Finger, P.T.; Graue, G.F.; Grossniklaus, H.E.; Honavar, S.G.; Khong, J.J.; McKelvie, P.A.; et al. Conjunctival Lymphoma—An International Multicenter Retrospective Study. JAMA Ophthalmol. 2016, 134, 406–414. [Google Scholar] [CrossRef] [Green Version]
- Graue, G.F.; Finger, P.T.; Maher, E.; Della Rocca, D.; Della Rocca, R.; Lelli, G.J., Jr.; Milman, T. Ocular adnexal lymphoma staging and treatment: American Joint Committee on Cancer versus Ann Arbor. Eur. J. Ophthalmol. 2013, 23, 344–355. [Google Scholar] [CrossRef]
- Cerhan, J.R.; Habermann, T.M. Epidemiology of Marginal Zone Lymphoma. Ann. Lymphoma 2021, 5, 1–19. [Google Scholar] [CrossRef]
- Stefanovic, A.; Lossos, I.S. Extranodal marginal zone lymphoma of the ocular adnexa. Blood 2009, 114, 501–510. [Google Scholar] [CrossRef] [Green Version]
- Parikh, R.R.; Moskowitz, B.K.; Maher, E.; Della Rocca, D.; Della Rocca, R.; Culliney, B.; Shapira, I.; Grossbard, M.L.; Harrison, L.B.; Hu, K. Long-term outcomes and patterns of failure in orbital lymphoma treated with primary radiotherapy. Leuk. Lymphoma 2015, 56, 1266–1270. [Google Scholar] [CrossRef]
- Niwa, M.; Ishikura, S.; Tatekawa, K.; Takama, N.; Miyakawa, A.; Kubota, T.; Kato, E.; Shibamoto, Y. Radiotherapy alone for stage IE ocular adnexal mucosa-associated lymphoid tissue lymphomas: Long-term results. Radiat. Oncol. 2020, 15, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagoo, A.S.; Haggerty, C.; Kim, Y.; Hammons, M.; Neufeld, K.; Redher, C.; Woodward, J.; Klintworth, G.K. Morphologic features of 115 lymphomas of the orbit and ocular adnexa categorized according to the World Health Organization classification: Are marginal zone lymphomas in the orbit mucosa-associated lymphoid tissue-type lymphomas? Arch. Pathol. Lab. Med. 2008, 132, 1405–1416. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, V.; Zen, Y.; Chan, J.K.; Yi, E.E.; Sato, Y.; Yoshino, T.; Kloppel, G.; Heathcote, J.G.; Khosroshahi, A.; Ferry, J.A.; et al. Consensus statement on the pathology of IgG4-related disease. Mod. Pathol. 2012, 25, 1181–1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheson, B.D.; Pfistner, B.; Juweid, M.E.; Gascoyne, R.D.; Specht, L.; Horning, S.J.; Coiffier, B.; Fisher, R.I.; Hagenbeek, A.; Zucca, E.; et al. Revised response criteria for malignant lymphoma. J. Clin. Oncol. 2007, 25, 579–586. [Google Scholar] [CrossRef]
- Kwon, M.; Lee, J.S.; Lee, C.; Yoon, D.H.; Sa, H.S. Prognostic factors for relapse and survival among patients with ocular adnexal lymphoma: Validation of the eighth edition of the American Joint Committee on Cancer (AJCC) TNM classification. Br. J. Ophthalmol. 2021, 105, 279–284. [Google Scholar] [CrossRef]
- Asadi-Amoli, F.; Nozarian, Z.; Bonaki, H.N.; Mehrtash, V.; Entezari, S. Clinicopathologic Assessment of Ocular Adnexal Lymphoproliferative Lesions at a Tertiary Eye Hospital in Iran. Asian Pac. J. Cancer Prev. 2016, 17, 3727–3731. [Google Scholar]
- Ueda, S.; Usui, Y.; Nagai, T.; Diaz-Aguilar, D.; Nagao, T.; Goto, H. Immunophenotypic profiles for distinguishing orbital mucosa-associated lymphoid tissue lymphoma from benign lymphoproliferative tumors. Jpn. J. Ophthalmol. 2017, 61, 354–360. [Google Scholar] [CrossRef]
- Mannami, T.; Yoshino, T.; Oshima, K.; Takase, S.; Kondo, E.; Ohara, N.; Nakagawa, H.; Ohtsuki, H.; Harada, M.; Akagi, T. Clinical, histopathological, and immunogenetic analysis of ocular adnexal lymphoproliferative disorders: Characterization of malt lymphoma and reactive lymphoid hyperplasia. Mod. Pathol. 2001, 14, 641–649. [Google Scholar] [CrossRef] [Green Version]
- Qu, X.L.; Hei, Y.; Kang, L.; Yang, X.J.; Wang, Y.; Lu, X.Z.; Xiao, L.H.; Yang, G. Establishment of a combination scoring method for diagnosis of ocular adnexal lymphoproliferative disease. PLoS ONE 2017, 12, e0160175. [Google Scholar] [CrossRef]
- Klavdianou, O.; Kondylis, G.; Georgopoulos, V.; Palioura, S. Bilateral benign reactive lymphoid hyperplasia of the conjunctiva: A case treated with oral doxycycline and review of the literature. Eye Vis. 2019, 6, 26. [Google Scholar] [CrossRef] [Green Version]
- Petit, B.; Chaury, M.P.; Le Clorennec, C.; Jaccard, A.; Gachard, N.; Moalic-Judge, S.; Labrousse, F.; Cogne, M.; Bordessoule, D.; Feuillard, J. Indolent lymphoplasmacytic and marginal zone B-cell lymphomas: Absence of both IRF4 and Ki67 expression identifies a better prognosis subgroup. Haematologica 2005, 90, 200–206. [Google Scholar] [PubMed]
- Albano, D.; Bosio, G.; Camoni, L.; Farina, M.; Re, A.; Tucci, A.; Giubbini, R.; Bertagna, F. Prognostic role of baseline (18) F-FDG PET/CT parameters in MALT lymphoma. Hematol. Oncol. 2019, 37, 39–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Maldegem, F.; van Dijk, R.; Wormhoudt, T.A.; Kluin, P.M.; Willemze, R.; Cerroni, L.; van Noesel, C.J.; Bende, R.J. The majority of cutaneous marginal zone B-cell lymphomas expresses class-switched immunoglobulins and develops in a T-helper type 2 inflammatory environment. Blood 2008, 112, 3355–3361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenner, I.; Roth, S.; Puppe, B.; Wobser, M.; Rosenwald, A.; Geissinger, E. Primary cutaneous marginal zone lymphomas with plasmacytic differentiation show frequent IgG4 expression. Mod. Pathol. 2013, 26, 1568–1576. [Google Scholar] [CrossRef] [Green Version]
- Sumii, Y.; Asada, N.; Sato, Y.; Ohshima, K.I.; Makita, M.; Yoshimoto, Y.; Sogabe, Y.; Imajo, K.; Meguri, Y.; Ennishi, D.; et al. Treatment outcomes of IgG4-producing marginal zone B-cell lymphoma: A retrospective case series. Int. J. Hematol. 2020, 112, 780–786. [Google Scholar] [CrossRef]
- Lee, M.J.; Kim, N.; Choe, J.Y.; Khwarg, S.I.; Jeon, Y.K.; Choung, H.K.; Kim, J.E. Clinicopathological Analysis of Ocular Adnexal Extranodal Marginal Zone B-Cell Lymphoma with IgG4-Positive Cells. PLoS ONE 2015, 10, e0131458. [Google Scholar] [CrossRef] [Green Version]
- Kubota, T.; Moritani, S.; Yoshino, T.; Nagai, H.; Terasaki, H. Ocular adnexal marginal zone B cell lymphoma infiltrated by IgG4-positive plasma cells. J. Clin. Pathol. 2010, 63, 1059–1065. [Google Scholar] [CrossRef]
- Li, K.M.; Xu, M.H.; Wu, X.; He, W.M. The Expression of IgG and IgG4 in Orbital MALT Lymphoma: The Similarities and Differences of IgG4-Related Diseases. OncoTargets Ther. 2020, 13, 5755–5761. [Google Scholar] [CrossRef]
- Nakayama, R.; Matsumoto, Y.; Horiike, S.; Kobayashi, S.; Nakao, R.; Nagoshi, H.; Tsutsumi, Y.; Nishimura, A.; Shimura, K.; Kobayashi, T.; et al. Close pathogenetic relationship between ocular immunoglobulin G4-related disease (IgG4-RD) and ocular adnexal mucosa-associated lymphoid tissue (MALT) lymphoma. Leuk. Lymphoma 2014, 55, 1198–1202. [Google Scholar] [CrossRef]
- Ohno, K.; Sato, Y.; Ohshima, K.; Takata, K.; Miyata-Takata, T.; Takeuchi, M.; Gion, Y.; Tachibana, T.; Orita, Y.; Ito, T.; et al. A subset of ocular adnexal marginal zone lymphomas may arise in association with IgG4-related disease. Sci. Rep. 2015, 5, 13539. [Google Scholar] [CrossRef] [Green Version]
- Go, H.; Kim, J.E.; Kim, Y.A.; Chung, H.K.; Khwarg, S.I.; Kim, C.W.; Jeon, Y.K. Ocular adnexal IgG4-related disease: Comparative analysis with mucosa-associated lymphoid tissue lymphoma and other chronic inflammatory conditions. Histopathology 2012, 60, 296–312. [Google Scholar] [CrossRef] [PubMed]
- Bertoni, F.; Cotter, F.E.; Zucca, E. Molecular genetics of extranodal marginal zone (MALT-type) B-cell lymphoma. Leuk. Lymphoma 1999, 35, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Forkasiewicz, A.; Dorociak, M.; Stach, K.; Szelachowski, P.; Tabola, R.; Augoff, K. The usefulness of lactate dehydrogenase measurements in current oncological practice. Cell. Mol. Biol. Lett. 2020, 25, 35. [Google Scholar] [CrossRef] [PubMed]
- Bayraktar, S.; Bayraktar, U.D.; Stefanovic, A.; Lossos, I.S. Primary ocular adnexal mucosa-associated lymphoid tissue lymphoma (MALT): Single institution experience in a large cohort of patients. Br. J. Haematol. 2011, 152, 72–80. [Google Scholar] [CrossRef] [Green Version]
- Thieblemont, C.; Cascione, L.; Conconi, A.; Kiesewetter, B.; Raderer, M.; Gaidano, G.; Martelli, M.; Laszlo, D.; Coiffier, B.; Lopez Guillermo, A.; et al. A MALT lymphoma prognostic index. Blood 2017, 130, 1409–1417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, M.; Kletter, K.; Becherer, A.; Jager, U.; Chott, A.; Raderer, M. 18F-fluorodeoxyglucose positron emission tomography (18F-FDG-PET) for staging and follow-up of marginal zone B-cell lymphoma. Oncology 2003, 64, 336–340. [Google Scholar] [CrossRef]
- Albano, D.; Bosio, G.; Giubbini, R.; Bertagna, F. 18F-FDG PET/CT and extragastric MALT lymphoma: Role of Ki-67 score and plasmacytic differentiation. Leuk. Lymphoma 2017, 58, 2328–2334. [Google Scholar] [CrossRef]
- Masuda, Y.; Takeuchi, K.; Kodama, T.; Fujisaki, T.; Imaizumi, Y.; Otsuka, E.; Ozaki, S.; Hasebe, S.; Yakushijin, Y. Treatment-associated outcomes of patients with primary ocular adnexal MALT lymphoma after accurate diagnosis. Int. J. Clin. Oncol. 2019, 24, 1620–1628. [Google Scholar] [CrossRef]
- Hindso, T.G.; Esmaeli, B.; Holm, F.; Mikkelsen, L.H.; Rasmussen, P.K.; Coupland, S.E.; Finger, P.T.; Graue, G.F.; Grossniklaus, H.E.; Honavar, S.G.; et al. International multicentre retrospective cohort study of ocular adnexal marginal zone B-cell lymphoma. Br. J. Ophthalmol. 2020, 104, 357–362. [Google Scholar] [CrossRef]
- Lee, J.L.; Kim, M.K.; Lee, K.H.; Hyun, M.S.; Chung, H.S.; Kim, D.S.; Shin, S.O.; Cho, H.S.; Bae, S.H.; Ryoo, H.M. Extranodal marginal zone B-cell lymphomas of mucosa-associated lymphoid tissue-type of the orbit and ocular adnexa. Ann. Hematol. 2005, 84, 13–18. [Google Scholar] [CrossRef]
- Desai, A.; Joag, M.G.; Lekakis, L.; Chapman, J.R.; Vega, F.; Tibshirani, R.; Tse, D.; Markoe, A.; Lossos, I.S. Long-term course of patients with primary ocular adnexal MALT lymphoma: A large single-institution cohort study. Blood 2017, 129, 324–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harada, K.; Murakami, N.; Kitaguchi, M.; Sekii, S.; Takahashi, K.; Yoshio, K.; Inaba, K.; Morota, M.; Ito, Y.; Sumi, M.; et al. Localized ocular adnexal mucosa-associated lymphoid tissue lymphoma treated with radiation therapy: A long-term outcome in 86 patients with 104 treated eyes. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 650–654. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.K.; Paik, J.S.; Park, G.S.; Cho, S.G.; Yang, S.W. Refractory follicular conjunctival lesions: Overlook as just inflammation or not? Br. J. Ophthalmol. 2019, 103, 1660–1665. [Google Scholar] [CrossRef] [PubMed]
- Collina, F.; De Chiara, A.; De Renzo, A.; De Rosa, G.; Botti, G.; Franco, R. Chlamydia psittaci in ocular adnexa MALT lymphoma: A possible role in lymphomagenesis and a different geographical distribution. Infect. Agents Cancer 2012, 7, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | Response, n (%) | p-Value | ||
|---|---|---|---|---|
| Total (n = 48) | CR (n = 33) | Non-CR (n = 15) | ||
| Age | 52.08 (14.95) | 52.36 (14.60) | 51.47 (16.19) | 0.850 |
| Sex, n (%) | 0.367 | |||
| Male | 27 (56.3%) | 20 (60.6%) | 7 (46.7%) | |
| Female | 21 (43.8%) | 13 (39.4%) | 8 (53.3%) | |
| Laterality, n (%) | 0.857 | |||
| Unilateral | 36 (75.0%) | 25 (75.8%) | 11 (73.3%) | |
| Bilateral | 12 (25.0%) | 8 (24.2%) | 4 (26.7%) | |
| T stage | 1.000ᵇ | |||
| T1 | 22 (45.8%) | 15 (45.5%) | 7 (46.7%) | |
| T2 | 23 (47.9%) | 15 (45.5%) | 8 (53.3%) | |
| T3 | 2 (4.2%) | 2 (6.1%) | 0 (0%) | |
| T4 | 1 (2.1%) | 1 (3.0%) | 0 (0%) | |
| Management | 0.043 ᵇ* | |||
| Observation | 15 (31.3%) | 7 (21.2%) | 8 (53.3%) | |
| Treatment | 33 (66.8%) | 26 (78.8%) | 7 (46.7%) | |
| Radiotherapy | 31 (64.6%) | 24 (72.7%) | 7 (46.7%) | |
| Chemotherapy | 2 (4.2%) | 2 (6.1%) | 0 (0%) | |
| RT dose (Gy) (n = 23, 7) | 26.64 (3.38) | 26.61 (3.54) | 26.74 (3.08) | 0.635 ᵃ |
| SUVmax (n = 32, 12) | 2.55 (1.42) | 2.52 (1.30) | 2.64 (1.78) | 0.822 ᵃ |
| SUVmax (post-RT) (n = 14, 4) | 2.27 (0.99) | 1.98 (0.77) | 3.27 (1.13) | 0.016 * |
| LDH (U/L) (n = 33, 13) | 252.48 (82.65) | 237.33 (75.51) | 290.91 (90.44) | 0.042 ᵃ* |
| ß2MG >2.19 (mg/L) (n = 31, 13) | 6 (13.6%) | 5 (16.1%) | 1 (7.7%) | 0.457 |
| CRP >0.50 (mg/dL) (n = 33, 13) | 2 (4.3%) | 1 (3.0%) | 1 (7.7%) | 0.490 ᵇ |
| Serum IgG4 >135 (mg/dL)(n = 22, 6) | 7 (25.0%) | 4 (18.2%) | 3 (50.0%) | 0.144 ᵇ |
| Failure-free survival (months) | 38.00 (21.67) | 40.58 (21.83) | 32.33 (20.93) | 0.222 |
| Follow-up period (month) | 43.33 (24.35) | 40.58 (21.83) | 49.40 (29.06) | 0.249 |
| Variable | Response, n (%) | p-Value | ||
|---|---|---|---|---|
| Total (n = 48) | CR (n = 33) | Non-CR (n = 15) | ||
| Histologic pattern | 0.151 | |||
| Confluent | 10 (20.8%) | 5 (15.2%) | 5 (33.3%) | |
| Nonconfluent | 38 (79.2%) | 28 (84.8%) | 10 (66.7%) | |
| Plasma cells | 0.531 | |||
| Absent | 17 (35.4%) | 13 (39.4%) | 4 (26.7%) | |
| Patchy | 20 (41.7%) | 12 (36.4%) | 8 (53.3%) | |
| Sheet | 11 (22.9%) | 8 (24.2%) | 3 (20.0%) | |
| Sclerosis | 0.306 | |||
| Absent | 16 (33.3%) | 9 (27.3%) | 7 (46.7%) | |
| Mild | 12 (25.0%) | 10 (30.3%) | 2 (13.3%) | |
| Moderate to severe | 20 (41.7%) | 14 (42.4%) | 6 (40.0%) | |
| Lymphoepithelial lesion | 31 (64.6%) | 20 (60.6%) | 11 (73.3%) | 0.393 |
| Large cell change | 4 (8.3%) | 2 (6.1%) | 2 (13.3%) | 0.579 ᵇ |
| Lymphovascular invasion | 46 (95.8%) | 31 (93.9%) | 15 (100.0%) | 1.000 ᵇ |
| Ki-67 | 10.44 (10.69) | 9.40 (9.53) | 11.53 (13.21) | 0.588 ᵃ |
| IgG4/IgG ≥ 0.4 (n = 33, 13) | 4 (8.7%) | 4 (12.1%) | 0 (0.0%) | 0.313 ᵇ |
| IgH rearrangement (n = 26, 10) | 0.900 | |||
| Monoclonal | 15 (41.7%) | 11 (43.3%) | 4 (40.0%) | |
| Polyclonal | 21 (58/3%) | 15 (57.7%) | 6 (60.0%) |
| Variable | Odd Ratio | 95% CI | p-Value |
|---|---|---|---|
| LDH >225 U/L | 4.142 | 0.807–21.269 | 0.089 |
| Ki-67 ≥ 5% | 0.678 | 0.133–3.447 | 0.639 |
| Treatment (RT or CT with immunotherapy) | 7.301 | 1.273–41.862 | 0.026 * |
| SUVmax | 1.349 | 0.769–2.365 | 0.296 |
| Conjunctival MALT Lymphoma (n = 22) | Non-Conjunctival MALT Lymphoma (n = 26) | |||||
|---|---|---|---|---|---|---|
| Variable | CR (n = 15) | Non-CR (n = 7) | p-Value | CR (n = 18) | Non-CR (n = 8) | p-Value |
| Histologic pattern | 0.145 ᵇ | 1.000 ᵇ | ||||
| Confluent | 3 (20.0%) | 4 (57.1%) | 2 (11.1%) | 1 (12.5%) | ||
| Nonconfluent | 12 (80.0%) | 3 (42.9%) | 16 (88.9%) | 7 (87.5%) | ||
| Plasma cells | 0.310 ᵇ | 0.704 ᵇ | ||||
| Absent | 5 (33.3%) | 0 (0.0%) | 8 (44.4%) | 4 (50.0%) | ||
| Patchy | 5 (33.3%) | 4 (57.1%) | 7 (38.9%) | 4 (50.0%) | ||
| Sheet | 5 (33.3%) | 3 (42.9%) | 3 (16.7%) | 0 (0.0%) | ||
| Sclerosis | 0.165 ᵇ | 0.856 ᵇ | ||||
| Absent | 6 (40.0%) | 5 (71.4%) | 3 (16.7%) | 2 (25.0%) | ||
| Mild | 6 (40.0%) | 0 (0.0%) | 4 (22.2%) | 2 (25.0%) | ||
| Moderate to severe | 3 (20.0%) | 2 (28.6%) | 11 (61.1%) | 4 (50.0%) | ||
| Lymphoepithelial lesion | 14 (93.3%) | 7 (100.0%) | 1.000 ᵇ | 6 (33.3%) | 4 (50.0%) | 0.664 ᵇ |
| Large cell change | 0 (0%) | 2 (28.6%) | 0.091 ᵇ | 2 (11.1%) | 0 (0.0%) | 1.000 ᵇ |
| Lymphovascular invasion | 13 (86.7%) | 7 (100.0%) | 1.000 ᵇ | 18 (100.0%) | 8 (100.0%) | |
| Ki-67 | 9.73 (12.08) | 15.00 (15.73) | 0.722 ᵃ | 10.11 (7.12) | 8.50 (10.69) | 0.221 ᵃ |
| IgG4/IgG ≥ 0.4 (n = 15, 6 and n = 18, 7) | 1 (6.3%) | 0 (0%) | 1.000 ᵇ | 3 (16.7%) | 0 (0.0%) | 0.534 ᵇ |
| Laterality | 0.376 ᵇ | 0.529 ᵇ | ||||
| Unilateral | 10 (66.7%) | 3 (42.9%) | 15 (83.3%) | 8 (100.0%) | ||
| Bilateral | 5 (33.3%) | 4 (57.1%) | 3 (16.7%) | 0 (0.0%) | ||
| Management | 0.165 ᵇ | 0.086 ᵇ | ||||
| Observation | 7 (46.7%) | 6 (85.7%) | 0 (0.0%) | 2 (25.0%) | ||
| Treatment | 8 (53.3%) | 1 (14.3%) | 18 (100.0%) | 6 (75.0%) | ||
| Radiotherapy | 8 (53.3%) | 1 (14.3%) | 16 (88.9%) | 6 (75.0%) | ||
| Chemotherapy | 0 (0.0%) | 0 (0.0%) | 2 (11.1%) | 0 (0.0%) | ||
| SUVmax (n = 14, 6 and n = 18, 6) | 1.86 (0.37) | 1.75 (0.25) | 0.533 | 3.03 (1.52) | 3.53 (2.24) | 0.617 ᵃ |
| SUVmax (post-RT) (n = 3, 0 and n = 11, 4) | 1.23 (1.07) | 2.18 (0.58) | 3.27 (1.13) | 0.026 * | ||
| LDH (U/L) (n = 15, 6 and n = 18, 7) | 257.13 (94.62) | 291.33 (110.49) | 0.483ᵃ | 220.83 (52.20) | 290.57 (78.64) | 0.037 ᵃ* |
| ß2MG > 2.19 (mg/L) (n = 13, 6 and n = 18, 7) | 3 (23.1%) | 0 (0.0%) | 0.200 | 2 (11.1%) | 1 (14.3%) | 0.826 |
| Failure-free survival (month) | 44.87 (28.63) | 30.00 (24.68) | 0.252 | 37.00 (13.85) | 34.38 (18.55) | 0.691 |
| Follow-up period (month) | 44.87 (28.12) | 42.71 (28.12) | 0.871 | 37.00 (13.85) | 55.25 (30.46) | 0.142 |
| Patient # | Age/Sex | Primary Site | Treatment | Time to Relapse (Month) | Recur Site | Treatment | Outcome |
|---|---|---|---|---|---|---|---|
| 1 | 32/M | Right conjunctiva | Observation (Antibiotics) | 80 | Right conjunctiva | Radiation | CR |
| 2 | 64/F | Left conjunctiva | Observation (Antibiotics) | 27 | Right conjunctiva | Observation (Excision) | CR |
| 3 | 35/F | Right conjunctiva | Observation (Excision) | 6 | Right conjunctiva | Radiotherapy | CR |
| 4 | 56/F | Left orbit | Radiotherapy | 35 | Both conjunctiva | NA | NA |
| 5 | 74/F | Left orbit | Radiotherapy | 9 | Right conjunctiva | Radiotherapy | CR |
| 6 | 47/F | Right lacrimal gland | Observation (Antibiotics) | 35 and 67 | Left eyelid and lung (multiple) | Obervation (Antibiotics) and Surgery | PR |
| 7 | 65/F | Right lacrimal gland | Radiotherapy | 48 and 26 | Right cheek and lung (DLBCL transformation) | Radiotherapy and surgery with chemotherapy and immunotherapy | CR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, S.; Seo, M.; Park, S.H.; Jo, J.-C.; Chae, S.W.; Lee, J.-H.; Cha, H.J. Clinicopathologic Characteristics Associated with Prognosis in Ocular Extranodal Marginal Zone B Cell Lymphoma. Medicina 2022, 58, 818. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060818
Choi S, Seo M, Park SH, Jo J-C, Chae SW, Lee J-H, Cha HJ. Clinicopathologic Characteristics Associated with Prognosis in Ocular Extranodal Marginal Zone B Cell Lymphoma. Medicina. 2022; 58(6):818. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060818
Chicago/Turabian StyleChoi, Soyeon, Minjung Seo, Seol Hoon Park, Jae-Cheol Jo, Seoung Wan Chae, Ju-Hyang Lee, and Hee Jeong Cha. 2022. "Clinicopathologic Characteristics Associated with Prognosis in Ocular Extranodal Marginal Zone B Cell Lymphoma" Medicina 58, no. 6: 818. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060818