
The Effects of the ‘Catabolic Crisis’ on Patients’ Prolonged Immobility after COVID-19 Infection

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
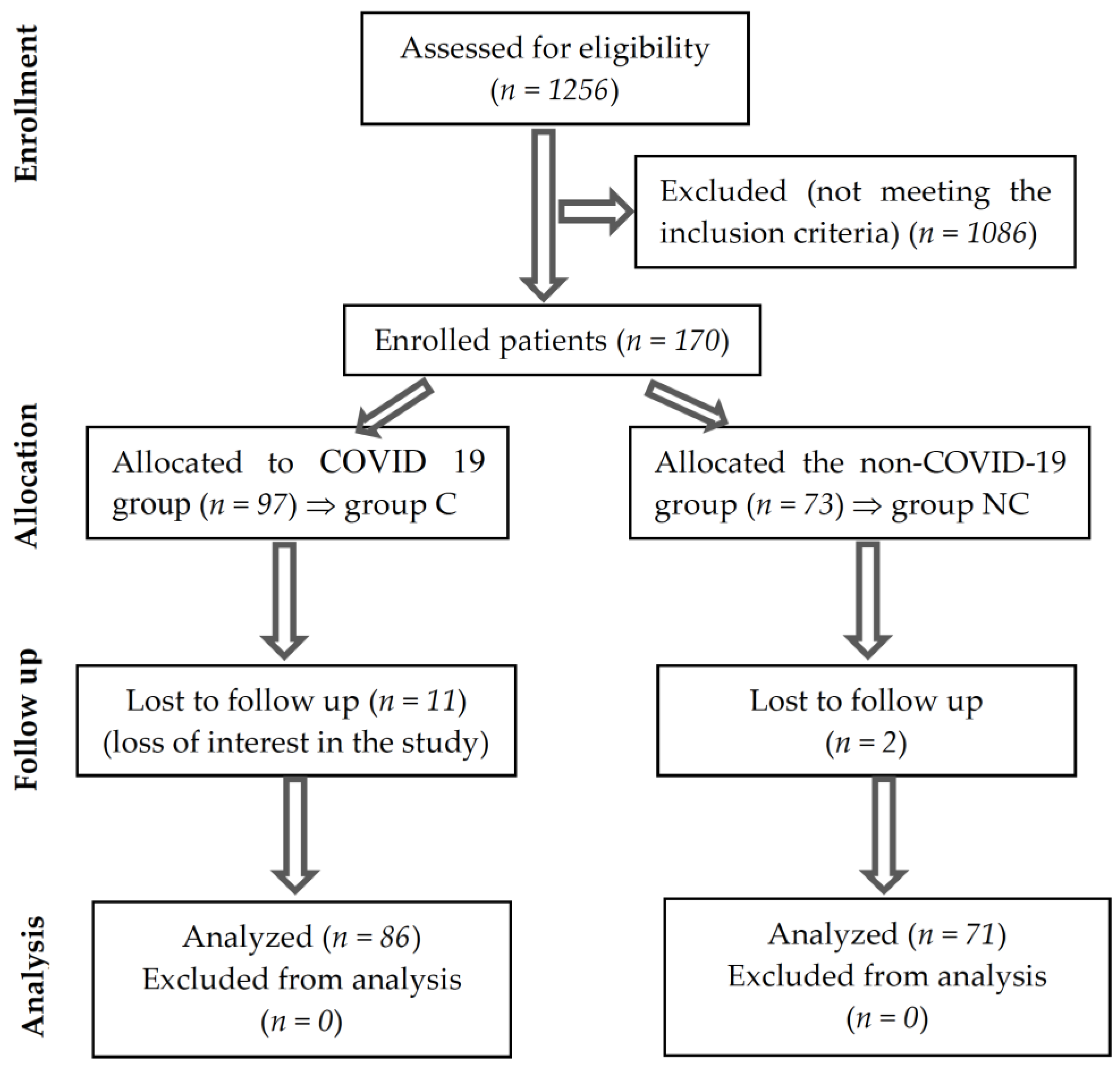
2.1. Study Design
- -
- Non-COVID-19 group (group NC) of patients who had no clinical signs of respiratory infection, had not been quarantined/hospitalized in the last 3 months, and at the time of evaluation, had no positive SARS-CoV-2 antibodies (immunoglobulin M or G) (rapid chromatographic immunoassay, Hoffmann-La Roche Ltd., Basel, Switzerland).
- -
- COVID-19 (group C) group of patients who were diagnosed with SARS-CoV-2 respiratory infection within the last 30 days. The diagnosis was based on confirmation of COVID-19 using a single positive test, which highlights the RNA/antigen of the virus in the upper respiratory tract specimens (nasopharyngeal and oropharyngeal) using the real-time polymerase chain reaction/rapid chromatographic immunoassay.
2.2. Inclusion/Exclusion Criteria
2.3. Sample Size
2.4. Study Tools
2.5. Ethical Approval
2.6. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Waters, D.; Baumgartner, R.; Garry, P.; Vellas, B. Advantages of dietary, exercise-related, and therapeutic interventions to prevent and treat sarcopenia in adult patients: An update. Clin. Interv. Aging 2010, 5, 259. [Google Scholar] [CrossRef] [Green Version]
- Beaudart, C.; Dawson, A.; Shaw, S.; Harvey, N.C.; Kanis, J.; Binkley, N.; Reginster, J.Y.; Chapurlat, R.; Chan, D.; Bruyère, O. Nutrition and physical activity in the prevention and treatment of sarcopenia: Systematic review. Osteoporos. Int. 2017, 28, 1817–1833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafiee, G.; Keshtkar, A.; Soltani, A.; Ahadi, Z.; Larijani, B.; Heshmat, R. Prevalence of sarcopenia in the world: A systematic review and meta-analysis of general population studies. J. Diabetes Metab. Disord. 2017, 16, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schweighofer, N.; Colantonio, C.; Haudum, C.W.; Hutz, B.; Kolesnik, E.; Mursic, I.; Pilz, S.; Schmidt, A.; Stadlbauer, V.; Zirlik, A. DXA-Derived indices in the characterisation of sarcopenia. Nutrients 2021, 14, 186. [Google Scholar] [CrossRef] [PubMed]
- Delmonico, M.J.; Harris, T.B.; Lee, J.S.; Visser, M.; Nevitt, M.; Kritchevsky, S.B.; Tylavsky, F.A.; Newman, A.B.; Health, A.; Study, B.C. Alternative definitions of sarcopenia, lower extremity performance, and functional impairment with aging in older men and women. J. Am. Geriatr. Soc. 2007, 55, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Shepard, D.S.; Katzmarzyk, P.T.; Roubenoff, R. The healthcare costs of sarcopenia in the United States. J. Am. Geriatr. Soc. 2004, 52, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Trends, G. Public health and aging: Trends in aging—United States and worldwide. Public Health 2003, 347, 921–925. [Google Scholar]
- Ghitea, T.C.; Vlad, S.; Birle, D.; Tit, D.M.; Lazar, L.; Nistor-Cseppento, C.; Behl, T.; Bungau, S. The influence of diet therapeutic intervention on the sarcopenic index of patients with metabolic syndrome. Acta Endocrinol. 2020, 16, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Deschenes, M.R.; Roby, M.A.; Eason, M.K.; Harris, M.B. Remodeling of the neuromuscular junction precedes sarcopenia related alterations in myofibers. Exp. Gerontol. 2010, 45, 389–393. [Google Scholar] [CrossRef] [Green Version]
- Kirwan, R.; McCullough, D.; Butler, T.; Perez de Heredia, F.; Davies, I.G.; Stewart, C. Sarcopenia during COVID-19 lockdown restrictions: Long-term health effects of short-term muscle loss. Geroscience 2020, 42, 1547–1578. [Google Scholar] [CrossRef] [PubMed]
- Moga, T.D.; Ioana, M.; Sabau, M.; Nistor-Cseppento, C.D.; Iovanovici, D.C.; Cavalu, S.; Dogaru, B.G. Sarcopenia, a major clinical problem in old age, potential causes, clinical consequences and therapeutic possibilities. Balneo PRM Res. J. 2022, 13, 492. [Google Scholar] [CrossRef]
- An, H.J.; Tizaoui, K.; Terrazzino, S.; Cargnin, S.; Lee, K.H.; Nam, S.W.; Kim, J.S.; Yang, J.W.; Lee, J.Y.; Smith, L.; et al. Sarcopenia in Autoimmune and Rheumatic Diseases: A Comprehensive Review. Int. J. Mol. Sci. 2020, 21, 5678. [Google Scholar] [CrossRef] [PubMed]
- Radu, A.-F.; Bungau, S.G. Management of Rheumatoid Arthritis: An Overview. Cells 2021, 10, 2857. [Google Scholar] [CrossRef]
- Tit, D.M.; Bungau, S.; Iovan, C.; Nistor Cseppento, D.C.; Endres, L.; Sava, C.; Sabau, A.M.; Furau, G.; Furau, C. Effects of the hormone replacement therapy and of soy isoflavones on bone resorption in postmenopause. J. Clin. Med. 2018, 7, 297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Sandler, C.X.; Wyller, V.B.B.; Moss-Morris, R.; Buchwald, D.; Crawley, E.; Hautvast, J.; Katz, B.Z.; Knoop, H.; Little, P.; Taylor, R.; et al. Long COVID and post-infective fatigue syndrome: A review. Open Forum Infect. Dis. 2021, 8, ofab440. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Maeda, K.; Satake, S.; Matsui, Y.; Arai, H. Osteosarcopenia, the co-existence of osteoporosis and sarcopenia, is associated with social frailty in older adults. Aging Clin. Exp. Res. 2022, 34, 535–543. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M. Sarcopenia: European consensus on definition and diagnosis Report of the European Working Group on Sarcopenia in Older PeopleA. J. Cruz-Gentoft et al. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Rolland, Y.; Czerwinski, S.; Abellan Van Kan, G.; Morley, J.E.; Cesari, M.; Onder, G.; Woo, J.; Baumgartner, R.; Pillard, F.; Boirie, Y.; et al. Sarcopenia: Its assessment, etiology, pathogenesis, consequences and future perspectives. J. Nutr. Health Aging 2008, 12, 433–450. [Google Scholar] [CrossRef] [Green Version]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; McLean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M. The FNIH sarcopenia project: Rationale, study description, conference recommendations, and final estimates. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2014, 69, 547–558. [Google Scholar] [CrossRef]
- Dionyssiotis, Y.; Prokopidis, K.; Vorniotakis, P.; Bakas, E. Osteosarcopenia School. J. Frailty Sarcopenia Falls 2021, 6, 231. [Google Scholar] [CrossRef]
- Imamura, K.; Yamamoto, S.; Suzuki, Y.; Matsuzawa, R.; Harada, M.; Yoshikoshi, S.; Yoshida, A.; Matsunaga, A. Limitations of SARC-F as a Screening Tool for Sarcopenia in Patients on Hemodialysis. Nephron 2022, 146, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.; Leung, J.; Morley, J.E. Validating the SARC-F: A suitable community screening tool for sarcopenia? J. Am. Med. Dir. Assoc. 2014, 15, 630–634. [Google Scholar] [CrossRef]
- Beaudart, C.; McCloskey, E.; Bruyère, O.; Cesari, M.; Rolland, Y.; Rizzoli, R.; de Carvalho, I.A.; Thiyagarajan, J.A.; Bautmans, I.; Bertière, M.-C. Sarcopenia in daily practice: Assessment and management. BMC Geriatr. 2016, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.; Ferrucci, L.; Simonsick, E.; Salive, M.; Wallace, R. Short Physical Performance Battery Protocol and Score Sheet. 1994. Available online: https://www.mcroberts.nl/wp-content/uploads/2016/11/SPPB_form.pdf (accessed on 10 January 2020).
- World Medical Association declaration of Helsinki. Recommendations guiding physicians in biomedical research involving human subjects. JAMA 1997, 277, 925–926. [Google Scholar] [CrossRef]
- English, K.L.; Paddon-Jones, D. Protecting muscle mass and function in older adults during bed rest. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 34. [Google Scholar] [CrossRef] [PubMed]
- Dodds, R.M.; Syddall, H.E.; Cooper, R.; Benzeval, M.; Deary, I.J.; Dennison, E.M.; Der, G.; Gale, C.R.; Inskip, H.M.; Jagger, C. Grip strength across the life course: Normative data from twelve British studies. PLoS ONE 2014, 9, e113637. [Google Scholar] [CrossRef] [Green Version]
- Kara, M.; Ata, A.M.; Özçakar, L. Sarcopenic obesity is the real problem in COVID-19! Eur. J. Intern. Med. 2021, 93, 103. [Google Scholar] [CrossRef]
- Molfino, A.; Imbimbo, G.; Rizzo, V.; Muscaritoli, M.; Alampi, D. The link between nutritional status and outcomes in COVID-19 patients in ICU: Is obesity or sarcopenia the real problem? Eur. J. Intern. Med. 2021, 91, 93–95. [Google Scholar] [CrossRef]
- Hampson, G.; Stone, M.; Lindsay, J.; Crowley, R.; Ralston, S. Diagnosis and management of osteoporosis during COVID-19: Systematic review and practical guidance. Calcif. Tissue Int. 2021, 109, 351–362. [Google Scholar] [CrossRef]
- di Filippo, L.; Formenti, A.M.; Doga, M.; Pedone, E.; Rovere-Querini, P.; Giustina, A. Radiological thoracic vertebral fractures are highly prevalent in COVID-19 and predict disease outcomes. J. Clin. Endocrinol. Metab. 2021, 106, e602–e614. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.; Hu, K.; Yan, C.; Zhao, B.; Mei, F.; Chen, F.; Zhao, L.; Shang, Y.; Ma, Y.; Ma, B. Associated Factors of Sarcopenia in Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 4291. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.-Y.; Shin, S. Association of Sarcopenia with Osteopenia and Osteoporosis in Community-Dwelling Older Korean Adults: A Cross-Sectional Study. J. Clin. Med. 2021, 11, 129. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Huang, P.; Dou, Q.; Wang, C.; Zhang, W.; Yang, Y.; Wang, J.; Xie, X.; Zhou, J.; Zeng, Y. Falls among older adults with sarcopenia dwelling in nursing home or community: A meta-analysis. Clin. Nutr. 2020, 39, 33–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beaudart, C.; Rolland, Y.; Cruz-Jentoft, A.J.; Bauer, J.M.; Sieber, C.; Cooper, C.; Al-Daghri, N.; Araujo de Carvalho, I.; Bautmans, I.; Bernabei, R. Assessment of muscle function and physical performance in daily clinical practice. Calcif. Tissue Int. 2019, 105, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qaisar, R.; Karim, A.; Muhammad, T.; Shah, I.; Iqbal, M.S. The coupling between sarcopenia and COVID-19 is the real problem. Eur. J. Intern. Med. 2021, 93, 105–106. [Google Scholar] [CrossRef]
- Gill, T.M.; Allore, H.; Guo, Z. The deleterious effects of bed rest among community-living older persons. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, M755–M761. [Google Scholar] [CrossRef]
- Kemmler, W.; Kohl, M.; Fröhlich, M.; Jakob, F.; Engelke, K.; von Stengel, S.; Schoene, D. Effects of high-intensity resistance training on osteopenia and sarcopenia parameters in older men with osteosarcopenia—one-year results of the randomized controlled Franconian Osteopenia and Sarcopenia Trial (FrOST). J. Bone Miner. Res. 2020, 35, 1634–1644. [Google Scholar] [CrossRef]
- Aryana, I.G.P.S.; Setiati, S.; Rini, S.S. Molecular Mechanism of Acute Sarcopenia in Elderly Patient with COVID-19. Acta Med. Indones. 2021, 53, 481–492. [Google Scholar]
- Piotrowicz, K.; Gąsowski, J.; Michel, J.-P.; Veronese, N. Post-COVID-19 acute sarcopenia: Physiopathology and management. Aging Clin. Exp. Res. 2021, 33, 2887–2898. [Google Scholar] [CrossRef]
- Welch, C.; Greig, C.; Masud, T.; Wilson, D.; Jackson, T. COVID-19 and Acute Sarcopenia. Aging Dis. 2020, 11, 1345–1351. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.; Giannini, M.; Oulehri, W.; Riou, M.; Marcot, C.; Pizzimenti, M.; Debrut, L.; Charloux, A.; Geny, B.; Meyer, A. Long Term Follow-Up of Sarcopenia and Malnutrition after Hospitalization for COVID-19 in Conventional or Intensive Care Units. Nutrients 2022, 14, 912. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Component | Question | Scoring |
|---|---|---|
| Strength | How much difficulty do you have in lifting and carrying 4.5 kg? | None = 0 Some = 1 A lot or unable = 2 |
| Assistance in walking | How much difficulty do you have walking across a room? | None = 0 Some = 1 A lot, use aids, or unable = 2 |
| Rise from a chair | How much difficulty do you have transferring from a chair or bed? | None = 0 Some = 1 A lot, or unable without help = 2 |
| Climb stairs | How much difficulty do you have climbing a flight of 10 stairs? | None = 0 Some = 1 A lot or unable = 2 |
| Falls | How many times have you fallen in the past year? | None = 0 1–3 falls = 1 ≥4 falls = 2 |
| Component | Question | Scoring Points |
|---|---|---|
| Balance | Held for 10 s | 4 |
| Held for 3 to 9.99 s | 3 | |
| Held for <than 3 s | 2 | |
| Not attempted | 1 | |
| For 4-Meter Walk | If time is >8.70 s | 1 |
| If time is between 6.21 and 8.70 s | 2 | |
| If time is between 4.82 and 6.20 s | 3 | |
| If time is <4.82 s | 4 | |
| Chair Stand Test | Participant unable to complete 5 chair stands or completes stands in >60 s | |
| If chair stand time is ≥16.70 s | 1 | |
| If chair stand time is between 13.70 and 16.69 s | 2 | |
| If chair stand time is between 11.20 and 13.69 s | 3 | |
| If chair stand time is ≤11.19 s | 4 |
| Parameter | Group C | Group NC | p |
|---|---|---|---|
| Age, M, SD | 66.56 ± 7.49 (86) | 66.79 ± 7.61(71) | 0.853 * |
| Age groups | |||
| <60, M, SD (N) | 55.67 ± 4.43 (15) | 55.50 ± 4.10 (12) | 0.920 * |
| 60–70, M, SD (N) | 65.45 ± 2.66 (47) | 65.46 ± 3.92 (39) | 0.980 * |
| >70, M, SD (N) | 75.96 ± 3.26 (23) | 76.15 ± 3.34 (20) | 0.849 * |
| Female, N (%) | 47 (54.65%) | 41 (57.74%) | 0.522 ** |
| Rural area, N (%) | 40 (46.51%) | 35 (49.30%) | 0.563 ** |
| BMI, M, SD | 28.42 ± 4.78 | 28.07 ± 4.69 | 0.647 * |
| Smoker, N (%) | 21 (24.42%) | 11 (15.49%) | 0.077 ** |
| Alcohol user, N (%) | 8 (9.30%) | 14 (19.72%) | 0.200 ** |
| Coffee user, N (%) | 23 (26.74%) | 13 (18.31%) | 0.095 ** |
| PMH, N (%) | |||
| Kyphosis | 81 (94.19%) | 68 (95.77%) | 0.286 ** |
| Scoliosis | 54 (62.79%) | 43 (60.56%) | 0.264 ** |
| Bone fractures | 18 (20.93%) | 13 (18.31%) | 0.369 ** |
| Parameter | Group C | Group NC | p |
|---|---|---|---|
| SPPB | |||
| Score values, M, SD | 6.00 ± 2.01 | 6.27 ± 2.05 | 0.414 * |
| Low performance, values 0–6, N (%) | 50 (58.14) | 49 (69.01) | 0.919 ** |
| Intermediate performance, values 7–9, N (%) | 36 (41.86) | 22 (30.99) | 0.066 ** |
| High performance, values 10–12, N (%) | 0 (0) | 0 (0) | - |
| Balance, M, SD | 1.58 ± 0.61 | 1.75 ± 0.53 | 0.063 * |
| 4-m walk, M, SD | 2.02 ± 0.92 | 1.99 ± 0.92 | 0.798 * |
| Chair standing, M, SD | 2.43 ± 1.44 | 2.54 ± 1.45 | 0.648 * |
| SARC-F | |||
| Score values, M, SD | 5.04 ± 2.17 | 4.24 ± 2.43 | 0.035 * |
| Sarcopenie, values ≥ 4, N (%) | 32 (37.21) | 23 (32.39) | 0.224 ** |
| Strength, M, SD | 1.25 ± 0.67 | 0.92 ± 0.63 | 0.002 * |
| Assistance walking, M, SD | 0.71 ± 0.63 | 0.68 ± 0.65 | 0.773 * |
| Rise from a chair, M, SD | 1.26 ± 0.56 | 1.04 ± 0.46 | 0.009 * |
| Climb stairs, M, SD | 1.32 ± 0.52 | 1.14 ± 0.49 | 0.030 * |
| Falls, M, SD | 0.52 ± 0.65 | 0.46 ± 0.67 | 0.620 * |
| Parameter | Group C | Group NC | p |
|---|---|---|---|
| Patients’ Number (%) | |||
| Arm Force | |||
| Female, <18 N | 0 | 0 | - |
| Male, <28 N | 16 (41.03) | 9 (30) | 0.161 * |
| Forearm force | |||
| Female, <18 N | 0 | 1(2.44) | 0.890 * |
| Male, <28 N | 26 (66.67) | 27 (90) | 0.317 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moga, T.D.; Nistor-Cseppento, C.D.; Bungau, S.G.; Tit, D.M.; Sabau, A.M.; Behl, T.; Nechifor, A.C.; Bungau, A.F.; Negrut, N. The Effects of the ‘Catabolic Crisis’ on Patients’ Prolonged Immobility after COVID-19 Infection. Medicina 2022, 58, 828. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060828
Moga TD, Nistor-Cseppento CD, Bungau SG, Tit DM, Sabau AM, Behl T, Nechifor AC, Bungau AF, Negrut N. The Effects of the ‘Catabolic Crisis’ on Patients’ Prolonged Immobility after COVID-19 Infection. Medicina. 2022; 58(6):828. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060828
Chicago/Turabian StyleMoga, Titus David, Carmen Delia Nistor-Cseppento, Simona Gabriela Bungau, Delia Mirela Tit, Anca Maria Sabau, Tapan Behl, Aurelia Cristina Nechifor, Alexa Florina Bungau, and Nicoleta Negrut. 2022. "The Effects of the ‘Catabolic Crisis’ on Patients’ Prolonged Immobility after COVID-19 Infection" Medicina 58, no. 6: 828. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060828