
A New Trial to Measure ABO Antibodies Using Complement-Dependent Cytotoxicity

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Samples
2.2. Measurement of Isoagglutinin Titer
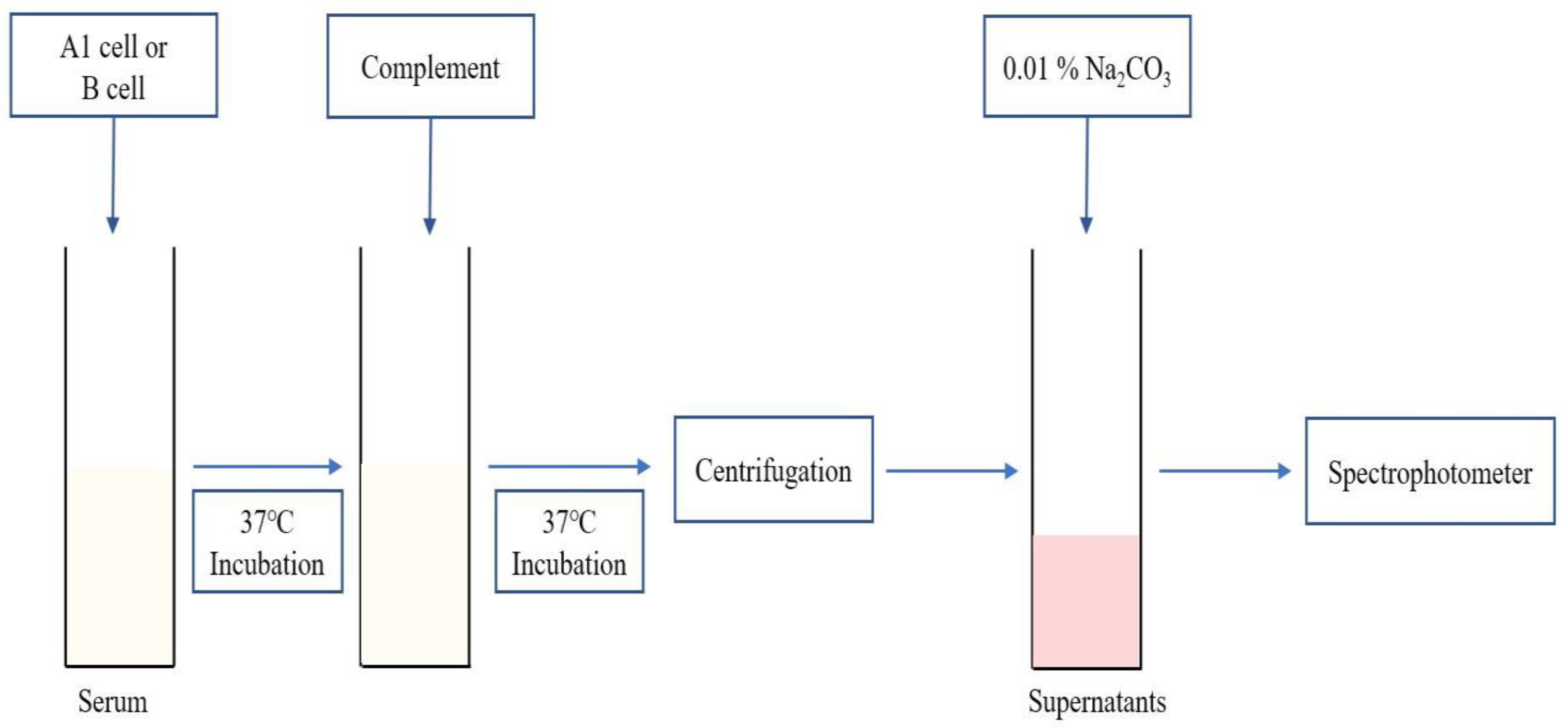
2.3. Plasma Hb Level Measurement Using CDC Test and Hemolysis (%) Calculation
2.4. Statistical Analysis
3. Results
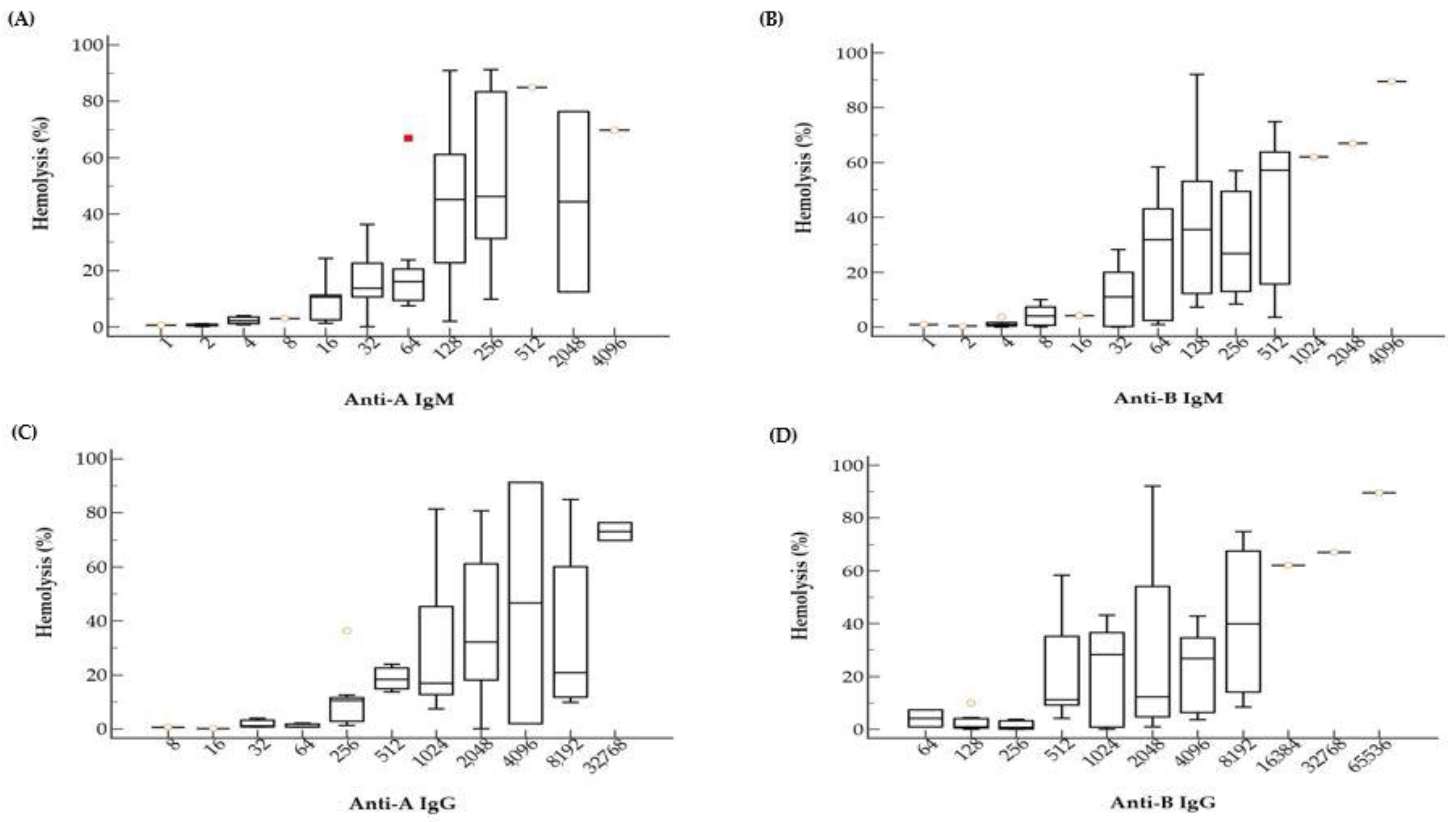
3.1. Hemolysis (%) According to ABO Ab Titers
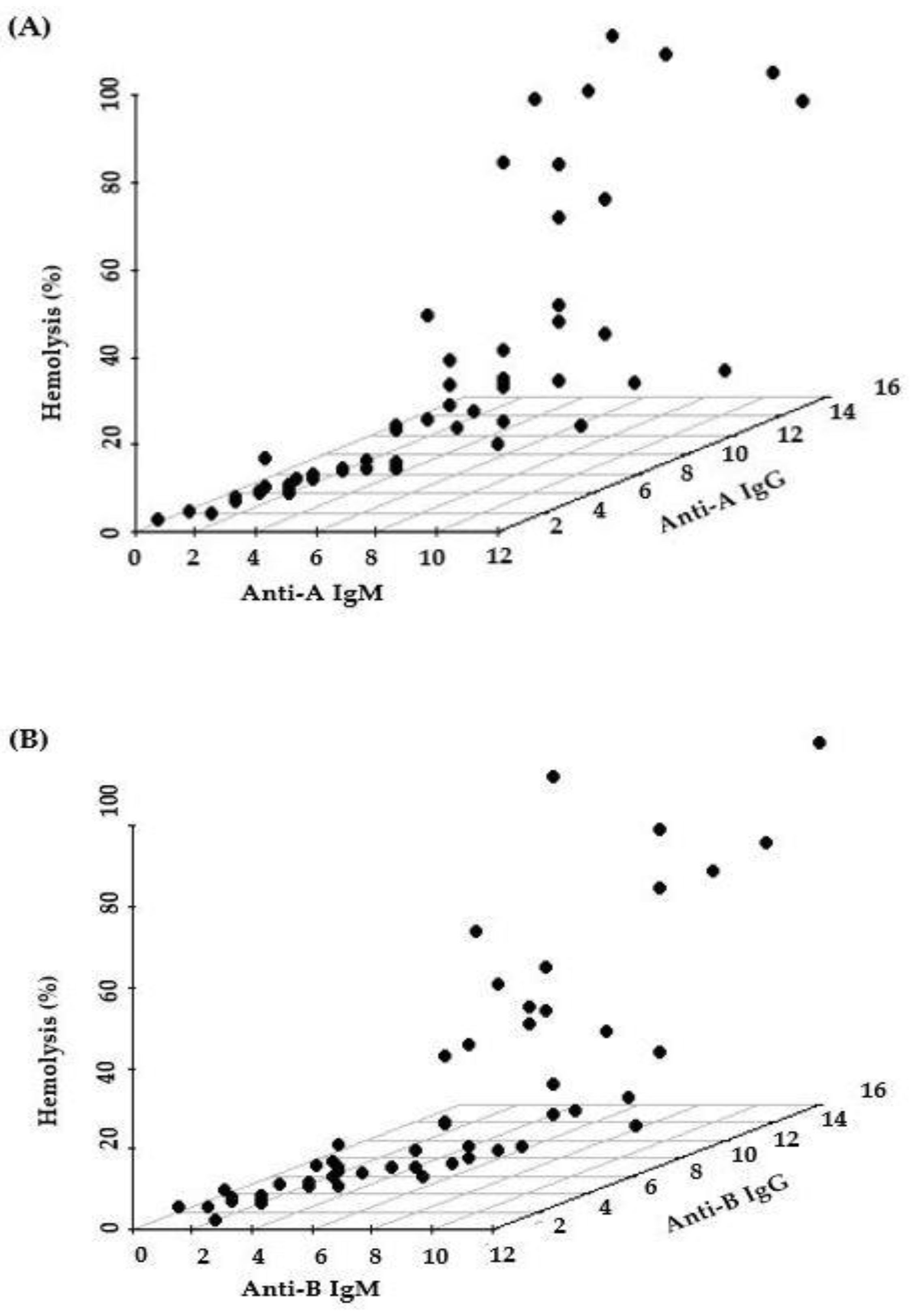
3.2. Relative Contribution of IgM and IgG for Hemolysis Activity
3.3. Comparison between Pre- and Post-Transplantation Samples
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Branch, D.R. Anti-A and anti-B: What are they and where do they come from? Transfusion 2015, 55, S74–S79. [Google Scholar] [CrossRef] [PubMed]
- Brouwers, H.A.A.; Overbeeke, M.A.M.; Gemke, R.J.B.J.; Maas, C.J.; Leeuwen, E.F.; Engelfriet, C.P. Sensitive methods for determining subclasses of IgG anti-A and anti-B in sera of blood-group-O women with a blood-group-A or -B child. Br. J. Haematol. 1987, 66, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Holgersson, J.; Rydberg, L.; Breimer, M.E. Molecular deciphering of the ABO system as a basis for novel diagnostics and therapeutics in ABO incompatible transplantation. Int. Rev. Immunol. 2014, 33, 174–194. [Google Scholar] [CrossRef] [PubMed]
- Vidarsson, G.; Dekkers, G.; Rispens, T. IgG subclasses and allotypes: From structure to effector functions. Front. Immunol. 2014, 5, 520. [Google Scholar] [CrossRef] [Green Version]
- Bachegowda, L.S.; Cheng, Y.H.; Long, T.; Shaz, B.H. Impact of uniform methods on interlaboratory antibody titration variability: Antibody titration and uniform methods. Arch. Pathol. Lab. Med. 2017, 141, 131–138. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.; Park, Y.J.; Kim, J.J.; Lee, E.; Kim, S.; Kim, H.O. Evaluation of the automated immunohematology analyzer ORTHO VISION for ABO antibody titration. Korean J. Blood Transfus. 2015, 26, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Zarzoso, M.; Gómez-Seguí, I.; De La Rubia, J. Therapeutic plasma exchange: Review of current indications. Transfus. Apher. Sci. 2019, 58, 247–253. [Google Scholar] [CrossRef]
- Zachary, A.A.; Leffell, M.S. Desensitization for solid organ and hematopoietic stem cell transplantation. Immunol. Rev. 2014, 258, 183–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stussi, G.; Huggel, K.; Lutz, H.U.; Schanz, U.; Rieben, R.; Seebach, J.D. Isotype-specific detection of ABO blood group antibodies using a novel flow cytometric method. Br. J. Haematol. 2005, 130, 954–963. [Google Scholar] [CrossRef]
- Pandey, P.; Setya, D.; Ranjan, S.; Singh, M.K.; Singh, M.K. Comparison of ABO isoagglutinin titres by three different methods in group O blood donors. ISBT Sci. Ser. 2021, 16, 76–84. [Google Scholar] [CrossRef]
- Kang, M.G.; Lee, S.J.; Oh, J.S.; Lim, Y.A. Comparison of ABO isoagglutinin titers by different tube hemagglutination techniques. Korean J. Blood Transfus. 2009, 20, 227–234. [Google Scholar]
- Lee, E.Y.; Kim, S.; Kim, H.O.; Kwon, S.W.; Kim, D.W.; Han, K.S. Survey analysis of ABO antibody titration at four university hospitals in Korea. Korean J. Blood Transfus. 2011, 22, 24–30. [Google Scholar]
- Terasaki, P.I.; McClelland, J.D. Microdroplet assay of human serum cytotoxins. Nature 1964, 204, 998–1000. [Google Scholar] [CrossRef] [PubMed]
- Harboe, M. A method for determination of hemoglobin in plasma by near-ultraviolet spectrophotometry. Scand. J. Clin. Lab. Investig. 1959, 11, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.J.; Chung, J.W.; Yi, J.; Hur, M.; Lee, T.H.; Hwang, S.H.; Song, Y.K.; Lee, D.H. Automation of Harboe method for the measurement of plasma free hemoglobin. J. Clin. Lab. Anal. 2020, 34, e23242. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Choe, W.; Shin, S.; Kim, Y.H.; Han, D.-J.; Park, S.-K.; Kwon, S.-W.; Ko, D.-H. ABO-incompatible kidney transplantation can be successfully conducted by monitoring IgM isoagglutinin titers during desensitization. Transfusion 2020, 60, 598–606. [Google Scholar] [CrossRef]
- Morath, C.; Zeier, M.; Döhler, B.; Opelz, G.; Süsal, C. ABO-incompatible kidney transplantation. Front. Immunol. 2017, 8, 234. [Google Scholar] [CrossRef] [Green Version]
- Kumlien, G.; Wilpert, J.; Säfwenberg, J.; Tydén, G. Comparing the tube and gel techniques for ABO antibody titration, as performed in three European centers. Transplantation 2007, 84, S17–S19. [Google Scholar] [CrossRef]
- AuBuchon, J.P.; de Wildt-Eggen, J.; Dumont, L.J. Reducing the variation in performance of antibody titrations. Arch. Pathol. Lab. Med. 2008, 132, 1194–1201. [Google Scholar] [CrossRef]
- Kang, S.J.; Lim, Y.A.; Baik, S.Y. Comparison of ABO antibody titers on the basis of the antibody detection method used. Ann. Lab. Med. 2014, 34, 300–306. [Google Scholar] [CrossRef]
- Lim, Y.A.; Kang, S.J. Standardization of ABO antibody titer measurement at laboratories in Korea. Ann. Lab. Med. 2014, 34, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Koch, C.A.; Khalpey, Z.I.; Platt, J.L. Accommodation: Preventing injury in transplantation and disease. J. Immunol. 2004, 172, 5143–5148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meny, G. Review: Transfusing incompatible RBCs-clinical aspects. Immunohematology 2004, 20, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Flegel, W.A. Pathogenesis and mechanisms of antibody-mediated hemolysis. Transfusion 2015, 55, S47–S58. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Pre-Transplantation | Post-Transplantation | ||||||
|---|---|---|---|---|---|---|---|---|
| Slope | 95% CI | p-Value | R2 | Slope | 95% CI | p-Value | R2 | |
| Anti-A IgM | 23.2 | 15.4–31.0 | <0.0001 | 0.4267 | 8.1 | −3.1–16.5 | 0.0583 | 0.1952 |
| Anti-A IgG | 19.9 | 11.7–28.0 | <0.0001 | 0.3660 | −4.9 | −15.3–5.4 | 0.2740 | 0.2318 |
| Anti-B IgM | 23.2 | 16.2–30.1 | <0.0001 | 0.4968 | 1.2 | −0.2–2.6 | 0.0850 | 0.2676 |
| Anti-B IgG | 23.3 | 15.0–31.5 | <0.0001 | 0.4439 | 1.2 | -0.4–2.8 | 0.0970 | 0.5382 |
| Variable | Multiple Linear Regression | |||
|---|---|---|---|---|
| Coefficient | t | p-Value | R2 | |
| Anti-A IgM | 12.9 | 3.282 | 0.0018 | 0.5216 |
| Anti-A IgG | −3.4 | −0.894 | 0.3752 | |
| Anti-B IgM | 8.7 | 2.631 | 0.0110 | 0.5114 |
| Anti-B IgG | 0.0 | −0.014 | 0.9889 | |
| Variable | Titer | Pre-Transplantation | Post-Transplantation | ||
|---|---|---|---|---|---|
| Hemolysis Range (%) | Median (%) | Hemolysis Range (%) | Median (%) | ||
| Anti-A IgM | 2 | 0.11–1.11 | 0.73 | 0.00–2.79 | 0.71 |
| 4 | 0.80–3.93 | 2.14 | 0.10–13.02 | 1.77 | |
| 8 | 2.94 | 2.94 | 1.11–23.40 | 3.28 | |
| 16 | 1.30–24.31 | 10.58 | 7.25–9.16 | 7.25 | |
| Anti-B IgM | 1 | 0.89 | 0.89 | 0.20–1.28 | 0.74 |
| 2 | 0.391 | 0.39 | 0.15–1.52 | 0.87 | |
| 4 | 0.00–3.72 | 0.83 | 0.00–2.34 | 1.42 | |
| 8 | 0.00–10.01 | 4.01 | 1.20–1.26 | 1.23 | |
| 16 | 4.13 | 4.13 | 0.00–2.20 | 1.10 | |
| 32 | 0.00–28.25 | 11.00 | 2.85 | 2.85 | |
| Anti-A IgG | 8 | 0.61 | 0.61 | 2.79 | 2.79 |
| 32 | 0.73–3.93 | 1.11 | 1.30–10.31 | 5.41 | |
| 64 | 0.74–2.14 | 0.80 | 0.00–1.89 | 0.81 | |
| 256 | 1.30–36.34 | 10.51 | 1.11 | 1.11 | |
| Anti-B IgG | 128 | 0.00–10.01 | 0.89 | 0.00 | 0.00 |
| 256 | 0.00–3.72 | 0.68 | 2.20 | 2.20 | |
| 512 | 4.13–58.38 | 11.16 | 0.00 | 0.00 | |
| 1,024 | 0.00–43.20 | 28.25 | 2.85 | 2.85 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Youk, H.-J.; Ryu, H.-y.; Seo, S.W.; Kim, J.S.; Chung, Y.; Kim, H.; Hwang, S.-H.; Oh, H.-B.; Min, W.-K.; Ko, D.-H. A New Trial to Measure ABO Antibodies Using Complement-Dependent Cytotoxicity. Medicina 2022, 58, 830. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060830
Youk H-J, Ryu H-y, Seo SW, Kim JS, Chung Y, Kim H, Hwang S-H, Oh H-B, Min W-K, Ko D-H. A New Trial to Measure ABO Antibodies Using Complement-Dependent Cytotoxicity. Medicina. 2022; 58(6):830. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060830
Chicago/Turabian StyleYouk, Hee-Jeong, Ho-yoon Ryu, Suk Won Seo, Jin Seok Kim, Yousun Chung, Hyungsuk Kim, Sang-Hyun Hwang, Heung-Bum Oh, Won-Ki Min, and Dae-Hyun Ko. 2022. "A New Trial to Measure ABO Antibodies Using Complement-Dependent Cytotoxicity" Medicina 58, no. 6: 830. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060830