
Image-Less THA Cup Navigation in Clinical Routine Setup: Individual Adjustments, Accuracy, Precision, and Robustness

 , and
, and
Abstract
:1. Introduction
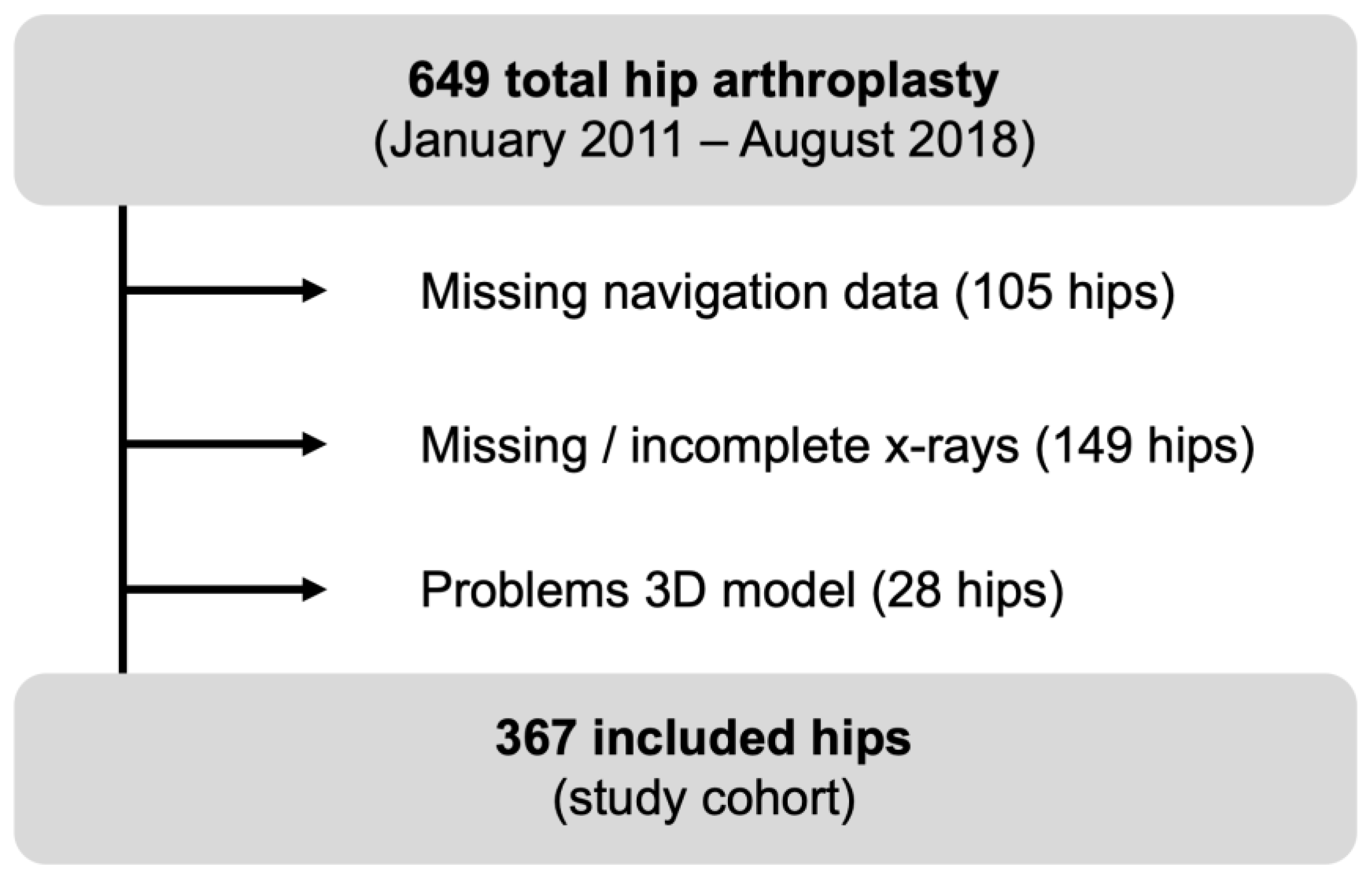
2. Material and Methods
3. Statistics
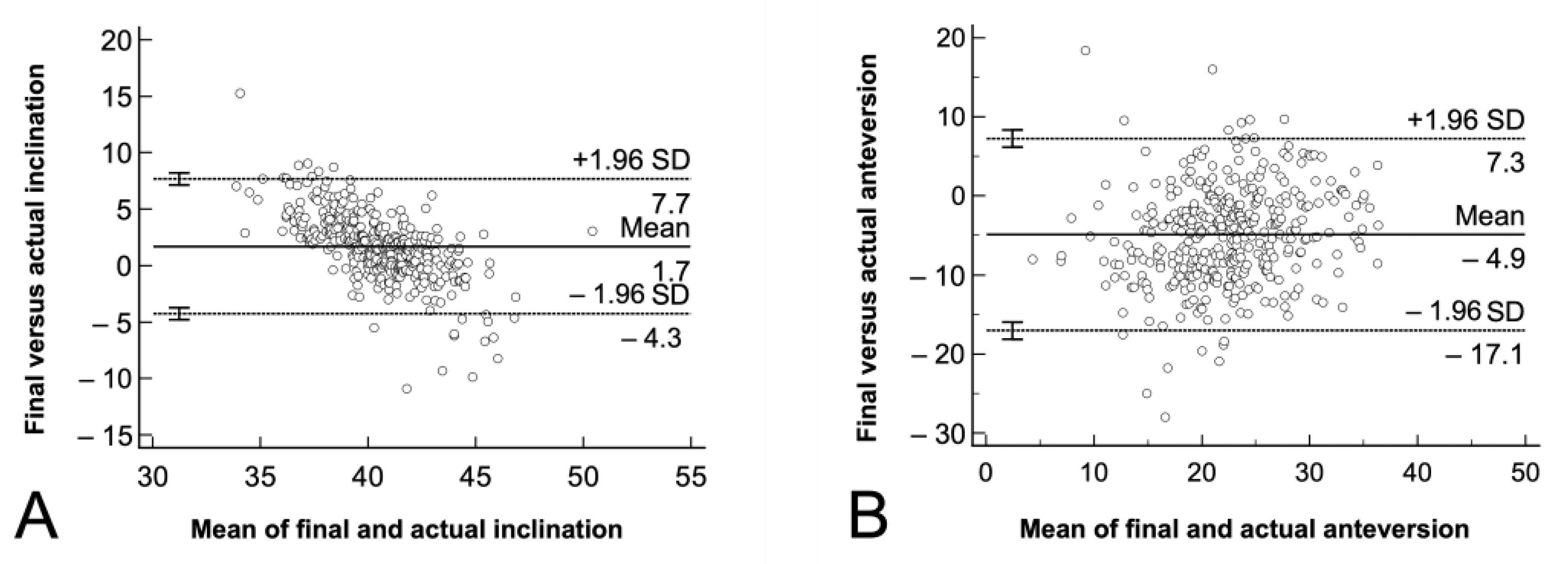
4. Results
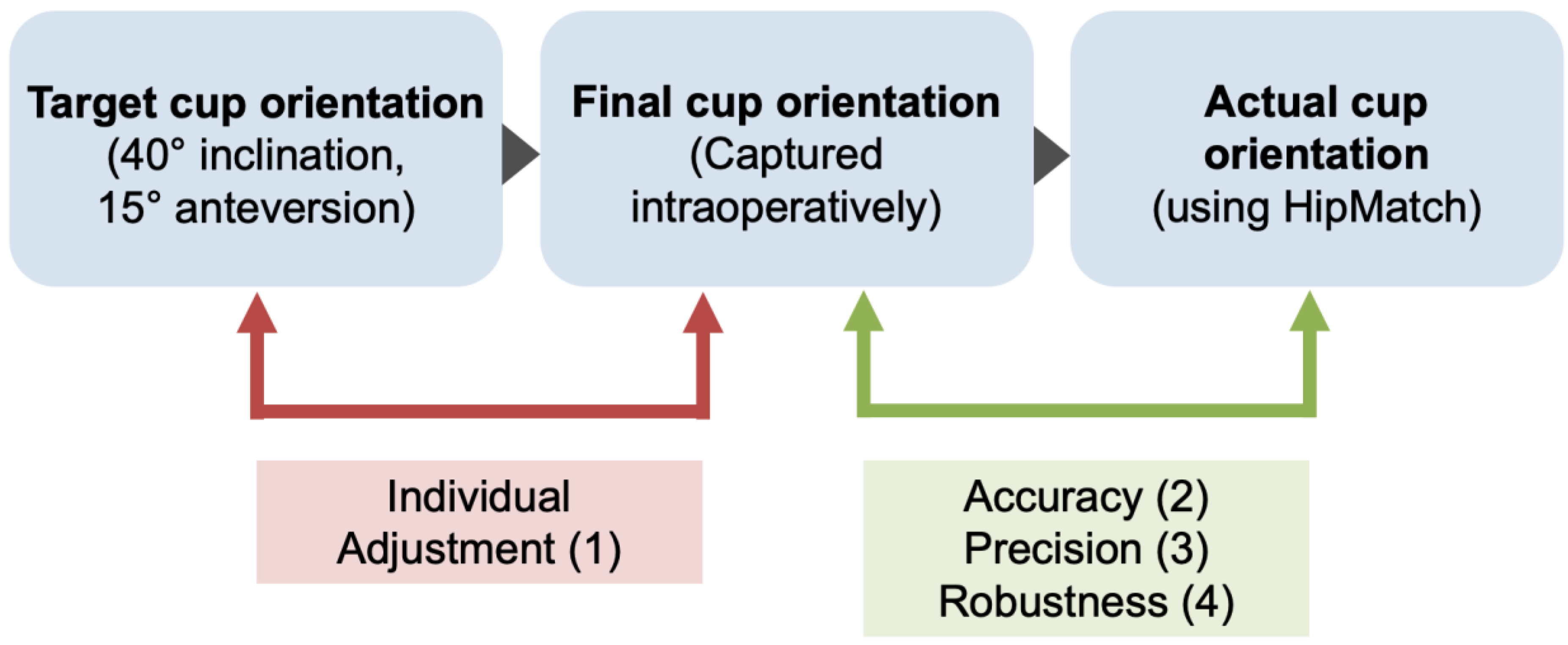
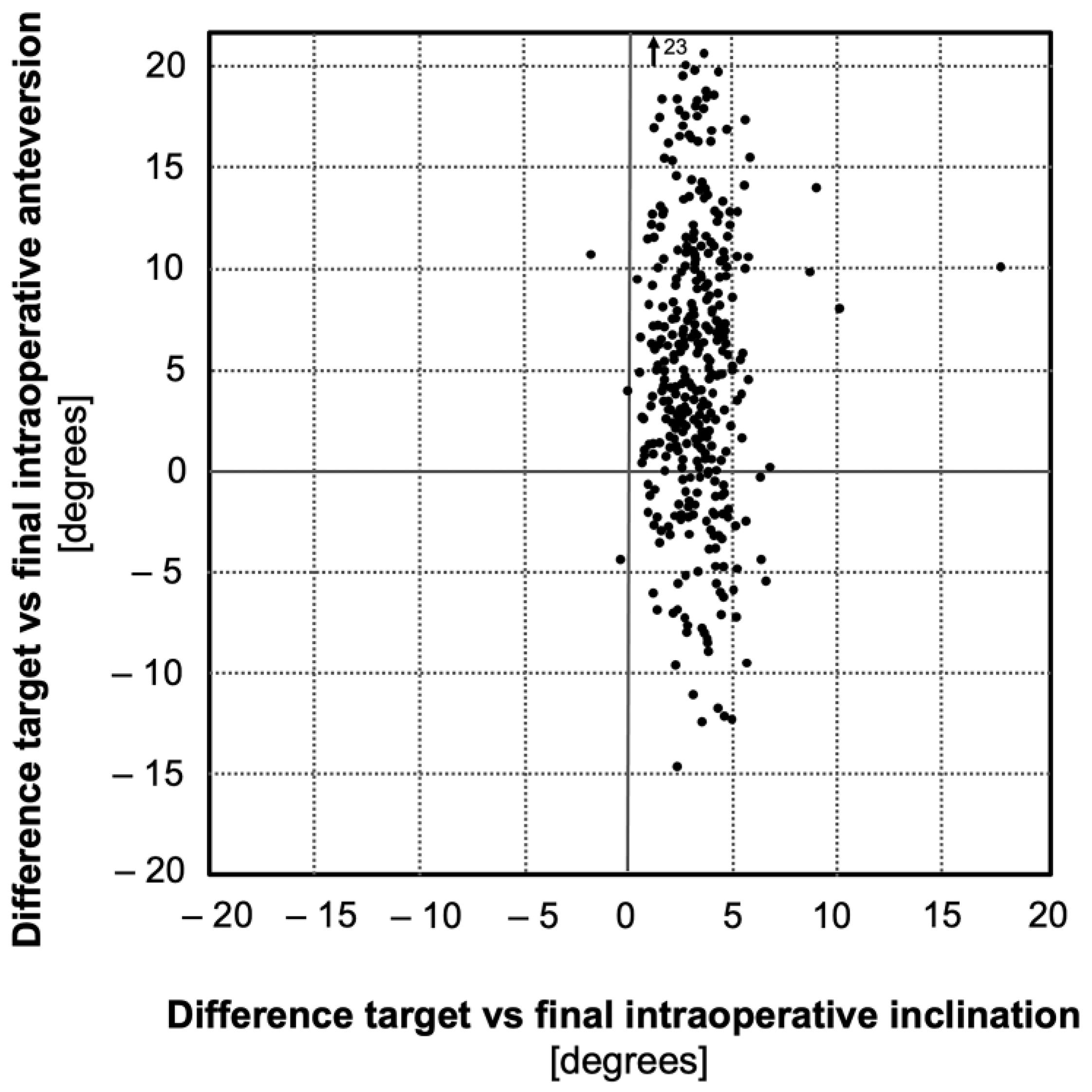
4.1. Individual Adjustment
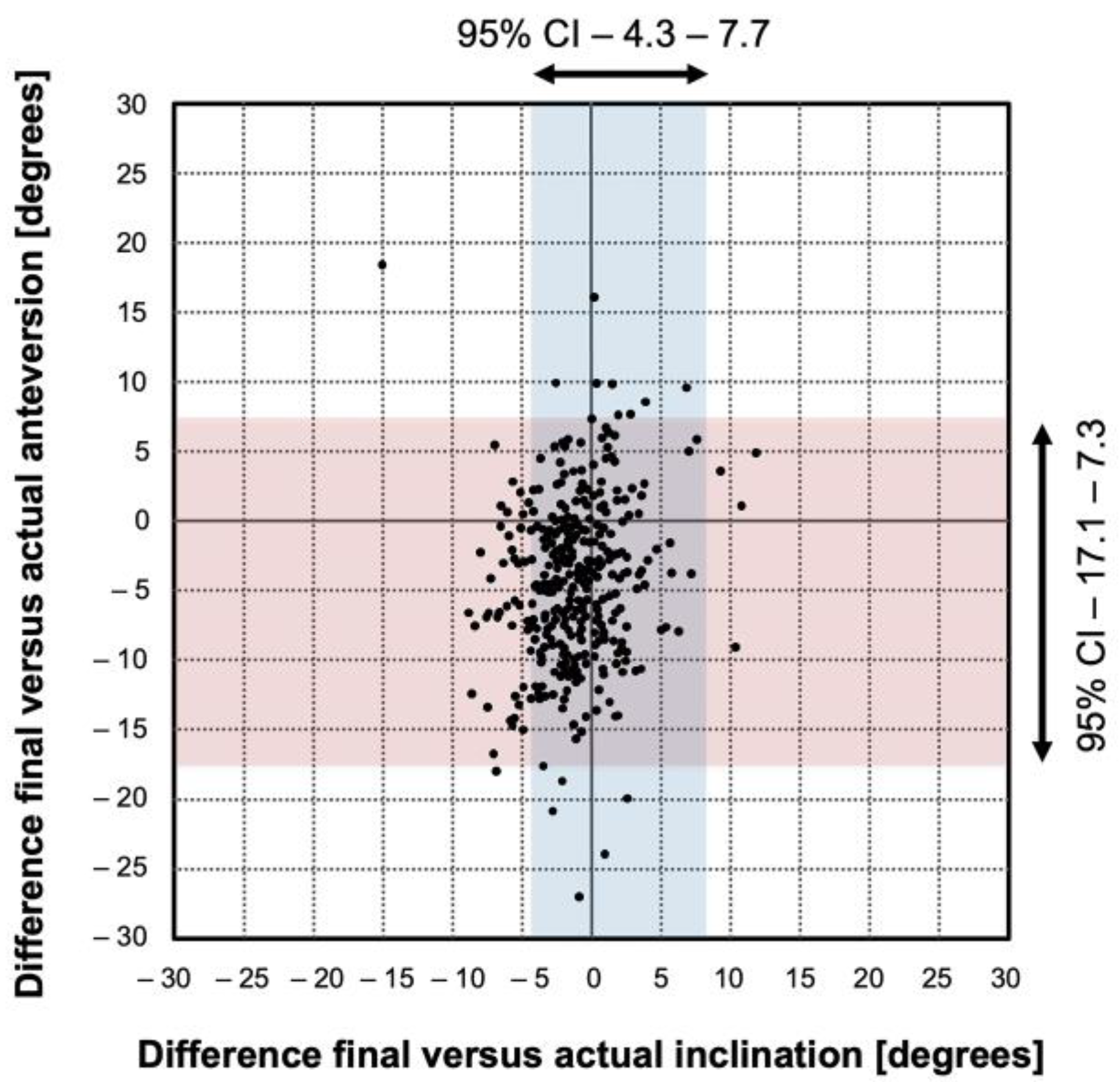
4.2. Accuracy
4.3. Precision
4.4. Robustness
5. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dorr, L.D.; Callaghan, J.J. Death of the Lewinnek “Safe Zone”. J. Arthroplast. 2019, 34, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Tannast, M.; Langlotz, U.; Siebenrock, K.A.; Wiese, M.; Bernsmann, K.; Langlotz, F. Anatomic Referencing of Cup Orientation in Total Hip Arthroplasty. Clin. Orthop. Relat. Res. 2005, 436, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G.; von Recum, J.; Nolte, L.-P.; Grützner, P.A.; Steppacher, S.D.; Franke, J. Validation of a statistical shape model-based 2D/3D reconstruction method for determination of cup orientation after THA. Int. J. Comput. Assist. Radiol. Surg. 2011, 7, 225–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steppacher, S.D.; Tannast, M.; Zheng, G.; Zhang, X.; Kowal, J.; Anderson, S.E.; Siebenrock, K.A.; Murphy, S.B. Validation of a new method for determination of cup orientation in THA. J. Orthop. Res. 2009, 27, 1583–1588. [Google Scholar] [CrossRef] [Green Version]
- Murray, D.W. The definition and measurement of acetabular orientation. J. Bone Joint. Surg. Br. 1993, 75, 228–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdel, M.P.; von Roth, P.; Jennings, M.T.; Hanssen, A.D.; Pagnano, M.W. What Safe Zone? The Vast Majority of Dislocated THAs Are Within the Lewinnek Safe Zone for Acetabular Component Position. Clin. Orthop. Relat. Res. 2015, 474, 386–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewinnek, G.E.; Lewis, J.L.; Tarr, R.; Compere, C.L.; Zimmerman, J.R. Dislocations after total hip-replacement arthroplasties. J. Bone Joint Surg Am 1978, 60, 217–220. [Google Scholar] [CrossRef]
- Tukey, J.W. Exploratory Data Analysis; Addison-Wesley Pub. Co.: Reading, MS, USA, 1977. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Lerch, T.; Todorski, I.A.; Steppacher, S.D.; Schmaranzer, F.; Werlen, S.F.; Siebenrock, K.A.; Tannast, M. Prevalence of Femoral and Acetabular Version Abnormalities in Patients with Symptomatic Hip Disease: A Controlled Study of 538 Hips. Am. J. Sports Med. 2017, 46, 122–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tannast, M.; Hanke, M.S.; Zheng, G.; Steppacher, S.D.; Siebenrock, K.A. What Are the Radiographic Reference Values for Acetabular Under- and Overcoverage? Clin. Orthop. Relat. Res. 2015, 473, 1234–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saxler, G.; Marx, A.; Vandevelde, D.; Langlotz, U.; Tannast, M.; Wiese, M.; Michaelis, U.; Kemper, G.; Grützner, P.A.; Steffen, R.; et al. The accuracy of free-hand cup positioning—A CT based measurement of cup placement in 105 total hip arthroplasties. Int. Orthop. 2004, 28, 198–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tannast, M.; Langlotz, F.; Kubiak-Langer, M.; Langlotz, U.; Siebenrock, K.-A. Accuracy and potential pitfalls of fluoroscopy-guided acetabular cup placement. Comput. Aided Surg. 2005, 10, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Kalteis, T.; Handel, M.; Herold, T.; Perlick, L.; Paetzel, C.; Grifka, J. Position of the acetabular cup—accuracy of radiographic calculation compared to CT-based measurement. Eur. J. Radiol. 2006, 58, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Fukunishi, S.; Nishio, S.; Fujihara, Y.; Okahisa, S.; Takeda, Y.; Fukui, T.; Yoshiya, S. Accuracy of combined anteversion in image-free navigated total hip arthroplasty: Stem-first or cup-first technique? Int. Orthop. 2015, 40, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Takeda, Y.; Fukunishi, S.; Nishio, S.; Fujihara, Y.; Yoshiya, S. Accuracy of Component Orientation and Leg Length Adjustment in Total Hip Arthroplasty Using Image-free Navigation. Open Orthop. J. 2017, 11, 1432–1439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenny, J.-Y.; Boeri, C.; Dosch, J.-C.; Uscatu, M.; Ciobanu, E. Navigated non-image-based positioning of the acetabulum during total hip replacement. Int. Orthop. 2007, 33, 83–87. [Google Scholar] [CrossRef] [Green Version]
- Ybinger, T.; Kumpan, W.; Hoffart, H.; Muschalik, B.; Bullmann, W.; Zweymüller, K. Accuracy of Navigation-Assisted Acetabular Component Positioning Studied by Computed Tomography Measurements: Methods and Results. J. Arthroplast. 2007, 22, 812–817. [Google Scholar] [CrossRef] [PubMed]
- Iwana, D.; Nakamura, N.; Miki, H.; Kitada, M.; Hananouchi, T.; Sugano, N. Accuracy of angle and position of the cup using computed tomography-based navigation systems in total hip arthroplasty. Comput. Aided Surg. 2013, 18, 187–194. [Google Scholar] [CrossRef]
- Sendtner, E.; Schuster, T.; Wörner, M.; Kalteis, T.; Grifka, J.; Renkawitz, T. Accuracy of acetabular cup placement in computer-assisted, minimally-invasive THR in a lateral decubitus position. Int. Orthop. 2010, 35, 809–815. [Google Scholar] [CrossRef] [Green Version]
- Hasegawa, M.; Tone, S.; Naito, Y.; Wakabayashi, H.; Sudo, A. Comparison of the accuracies of computed tomography-based navigation and image-free navigation for acetabular cup insertion in total hip arthroplasty in the lateral decubitus position. Comput. Assist. Surg. 2021, 26, 69–76. [Google Scholar] [CrossRef]
- Tetsunaga, T.; Yamada, K.; Tetsunaga, T.; Sanki, T.; Kawamura, Y.; Ozaki, T. An accelerometer-based navigation system provides acetabular cup orientation accuracy comparable to that of computed tomography-based navigation during total hip arthroplasty in the supine position. J. Orthop. Surg. Res. 2020, 15, 147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okamoto, M.; Kawasaki, M.; Okura, T.; Ochiai, S.; Yokoi, H. Comparison of accuracy of cup position using portable navigation versus alignment guide in total hip arthroplasty in supine position. HIP Int. 2020, 31, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Endo, H.; Tetsunaga, T.; Miyake, T.; Sanki, T.; Ozaki, T. Accuracy of Cup Positioning With the Computed Tomography-Based Two-dimensional to Three-Dimensional Matched Navigation System: A Prospective, Randomized Controlled Study. J. Arthroplast. 2017, 33, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Nakahara, I.; Kyo, T.; Kuroda, Y.; Miki, H. Effect of improved navigation performance on the accuracy of implant placement in total hip arthroplasty with a CT-based navigation system. J. Artif. Organs 2018, 21, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Parratte, S.; Argenson, J.-N.; Flecher, X.; Aubaniac, J.-M. Positionnement acétabulaire assisté par ordinateur dans les prothèses totales de hanche. Rev. Chir. Orthop. Reparatrice App. Mot. 2007, 93, 238–246. [Google Scholar] [CrossRef]
- Ryan, J.A.; Jamali, A.A.; Bargar, W.L. Accuracy of Computer Navigation for Acetabular Component Placement in THA. Clin. Orthop. Relat. Res. 2010, 468, 169–177. [Google Scholar] [CrossRef] [Green Version]
- Lin, F.; Lim, D.; Wixson, R.L.; Milos, S.; Hendrix, R.W.; Makhsous, M. Limitations of Imageless Computer-Assisted Navigation for Total Hip Arthroplasty. J. Arthroplast. 2011, 26, 596–605. [Google Scholar] [CrossRef] [PubMed]
- Hananouchi, T.; Takao, M.; Nishii, T.; Miki, H.; Iwana, D.; Yoshikawa, H.; Sugano, N. Comparison of navigation accuracy in THA between the mini-anterior and -posterior approaches. Int. J. Med. Robot. 2008, 5, 20–25. [Google Scholar] [CrossRef]
- Hirasawa, N.; Matsubara, M.; Ishii, K.; Hagio, S.; Okuda, N.; Sekiya, I.; Muneta, T. Effect of CT slice thickness on accuracy of implant positioning in navigated total hip arthroplasty. Comput. Aided Surg. 2010, 15, 83–89. [Google Scholar] [CrossRef]
- Kitada, M.; Nakamura, N.; Iwana, D.; Kakimoto, A.; Nishii, T.; Sugano, N. Evaluation of the Accuracy of Computed Tomography–Based Navigation for Femoral Stem Orientation and Leg Length Discrepancy. J. Arthroplast. 2011, 26, 674–679. [Google Scholar] [CrossRef]
- Kajino, Y.; Kabata, T.; Maeda, T.; Iwai, S.; Kuroda, K.; Tsuchiya, H. Does Degree of the Pelvic Deformity Affect the Accuracy of Computed Tomography-Based Hip Navigation? J. Arthroplast. 2012, 27, 1651–1657. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value(s) |
|---|---|
| Number of patients | 340 |
| Number of hips | 367 |
| Age at operation (years) | 68 ± 10 (42–91) |
| Gender (percentage male of all hips) | 52 |
| Weight (kg) | 78 ± 17 (46–140) |
| Height (m) | 1.70 ± 0.10 (1.50–2.00) |
| BMI (m/kg2) | 27 ± 5 (16–48) |
| Side (percentage right of all hips) | 52 |
| Parameter | Degrees |
|---|---|
| Target inclination (degree) | 40 |
| Target anteversion | 15 |
| Final intraoperative cup inclination (degree) | 41.4 ± 2 (36–52) |
| Final intraoperative cup anteversion (degree) | 20.0 ± 7 (0–38) |
| Actual cup inclination (degree) | 39.7 ± 4 (26–50) |
| Actual cup anteversion (degree) | 24.9 ± 6 (0–41) |
| Study | Year | Number of Hips | Type | Navigation System | Postoperative Evaluation | Reference Value Inclination | Range Inclination | Accuracy (p-Value) | Reference Value Anteversion | Range Anteversion | Accuracy (p-Value) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Tetsunaga et al. [22] | 2020 | 35 | CT-based | BrainLAB VectorVision 3.5.2 | CT-Based | 2.7° ± 2.0° | 0.16 | 2.8° ± 2.6° | <0.001 | ||
| 35 | Accelerometer-based | accelerometer-based navigation | CT-Based | 3.3° ± 2.4° | 3.4° ± 2.2° | ||||||
| Okamoto M et al. [23] | 2019 | 113 | Portable navigation | Protable navigation | CT-Based | 40° | 3.1 ± 2.2 | 0.304 | 15–20° | 2.8 ± 2.3 | 0.005 |
| 102 | Alignment guide | HipAlign | CT-Based | 40° | 2.9 ± 2.3 | 15–20° | 3.7 ± 2.7 | ||||
| Yamada et al. [24] | 2017 | 40 | CT-based | BrainLAB VectorVision 3.5.2 (2D-3D group) | CT-Based | 2.5° ± 2.2° | 0.0016 | 2.3° ± 1.7° | 0.0009 | ||
| 40 | CT-based | BrainLAB VectorVision 3.5.2 (PPM group) | CT-Based | 4.6° ± 3.3° | 4.4° ± 3.3° | ||||||
| Kalteis et al. [14] | 2006 | 30 | Free hand | - | CT-Based | 45° | 15° | ||||
| 30 | CT-based | BrainLAB VectorVision 3.0 | CT-Based | 45° | 3.0° ± 2.6 | 15° | 3.3° ± 2.3° | ||||
| 30 | Imageless | BrainLAB VectorVision 3.0 | CT-Based | 45° | 2.9° ± 2.2° | 15° | 4.2° ± 3.3° | ||||
| Iwana et al. [19] | 2013 | 87 | CT-based | Stryker CT-Hip System (older version) | CT-Based | 40° | 1.8° ± 1.6° | 0.98 | 10° | 1.2° ± 1.1° | 0.39 |
| Nakahara et al. [25] | 2017 | 49 | CT-based | Stryker CT-Hip System (older version) | CT-Based | 1.9° ± 1.6° | 1.6° ± 1.4° | ||||
| 49 | CT-based | Stryker CT-Hip System (newer version) | CT-Based | 1.2° ± 1.3 | 1.0 ± 0.8° | ||||||
| Ybinger et al. [18] | 2007 | 37 | Imageless | Plus Orthopaedics PiGalileo | CT-Based | 3.5° ± 4.4° | 6.5° ± 7.3° | ||||
| Parratte et al. [26] | 2007 | 30 | Imageless | Hiplogics Universal Protocol (BMI < 27) | CT-Based | 4.0° ± 2.8° | 3.4° ± 3.6° | ||||
| 30 | Hiplogics Universal Protocol (BMI ≥ 27) | CT-Based | 3.3° ± 3.1 | 11.6° ± 6.1° | |||||||
| Ryan et al. [27] | 2010 | 26 | Imageless | Ci System | CT-Based | 1.8° ± 1.2° | 2.0° ± 2.0 | ||||
| Jenny et al. [17] | 2007 | 48 | Imageless | B. Braun Aesculap OrthoPilot | CT-Based | −2° ± 4° | −4° ± 8° | ||||
| Fukunishi et al. [15] | 2015 | 83 | Imageless | B. Braun Aesculap OrthoPilot | CT-Based | 35–45° | 3.0° ± 2.6° | 15–25° | 5.0° ± 3.5° | ||
| Takeda et al. [16] | 2017 | 108 | Imageless | B. Braun Aesculap OrthoPilot | CT-Based | 3.7° ± 2.7° | 6.8° ± 3.6° | ||||
| Lin et al. [28] | 2011 | 25 | Imageless | Stryker Imageless Navigation System | CT-Based | 0.0° ± 2.8° | 3.4° ± 3.6° | ||||
| Sendtner et al. [20] | 2010 | 32 | Imageless | BrainLAB Hip unlimited 5.0 | CT-Based | 0.4° ± 3.3° | −5.6° ± 6.5° | ||||
| Sendtner et al. [20] | 2010 | 32 | CT-based | CT-Based | |||||||
| Hananouchi et al. [29] | 2009 | 40 | CT-based | Stryker CT-Hip System (older version) mini posterior approach | CT-Based | 2.4° ± 2.0° | 2.0° ± 1.4° | ||||
| Stryker CT-Hip System (older version) mini anterior approach | CT-Based | 2.0° ± 1.4° | 2.7° ± 1.9° | ||||||||
| Hirasawa et al. [30] | 2010 | 56 | CT-based | Stryker CT-Hip System (older version) | CT-Based | 3.2° ± 2.7° | 3.8° ± 3.4° | ||||
| Kitada et al. [31] | 2011 | 54 | CT-based | Stryker CT-Hip System (older version) | CT-Based | 0.4° ± 2.5° | −0.8° ± 4.1° | ||||
| Kajino et al. [32] | 2012 | 25 | CT-based | Stryker CT-Hip System (older version) for severe pelvic deformities | CT-Based | 1.5° ± 1.2° | 2.5° ± 1.7° | ||||
| 25 | CT-based | Stryker CT-Hip System (older version) low grad subluxation | CT-Based | 1.4° ± 1.1° | 2.7° ± 1.4° |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zurmühle, C.A.; Zickmantel, B.; Christen, M.; Christen, B.; Zheng, G.; Schwab, J.M.; Tannast, M.; Steppacher, S.D. Image-Less THA Cup Navigation in Clinical Routine Setup: Individual Adjustments, Accuracy, Precision, and Robustness. Medicina 2022, 58, 832. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060832
Zurmühle CA, Zickmantel B, Christen M, Christen B, Zheng G, Schwab JM, Tannast M, Steppacher SD. Image-Less THA Cup Navigation in Clinical Routine Setup: Individual Adjustments, Accuracy, Precision, and Robustness. Medicina. 2022; 58(6):832. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060832
Chicago/Turabian StyleZurmühle, Corinne A., Benjamin Zickmantel, Matthias Christen, Bernhard Christen, Guoyan Zheng, Joseph M. Schwab, Moritz Tannast, and Simon D. Steppacher. 2022. "Image-Less THA Cup Navigation in Clinical Routine Setup: Individual Adjustments, Accuracy, Precision, and Robustness" Medicina 58, no. 6: 832. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060832