
Robotic versus Laparoscopic Gastrectomy for Gastric Cancer: An Updated Systematic Review

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
- -
- PubMed/MEDLINE
- -
- Scopus
- -
- Cochrane Library
- -
- Web of Science
2.2. Inclusion Criteria
2.3. Data Extraction
- -
- demographic data: author’s surname and year of publication, database used, included studies [number, type, period, country, language], surgical procedure, population size;
- -
- meta-analyses data: operative outcomes [operative time, estimated blood loss, conversion to open surgery, number of retrieved lymph nodes, length of proximal and distal resection margins]; perioperative outcomes [time to first flatus, time to restart oral intake, length of hospitalization, overall complications, Clavien-Dindo (CD) ≥ III complications, mortality, reoperation, anastomotic leakage, pancreatic complications, delayed gastric emptying, intestinal obstruction, wound infection, intra-abdominal infection, duodenal stump leakage, anastomotic stenosis, abdominal bleeding, ileus, pneumonia]; long-term outcomes [overall survival, recurrence-free survival, recurrences, costs]. Sample size, heterogeneity, overall effect size, 95% of overall effect, p-value were included into the study number.
2.4. Quality Assessment
3. Results
3.1. Search Results and Study Characteristics
3.2. General Population Characteristics
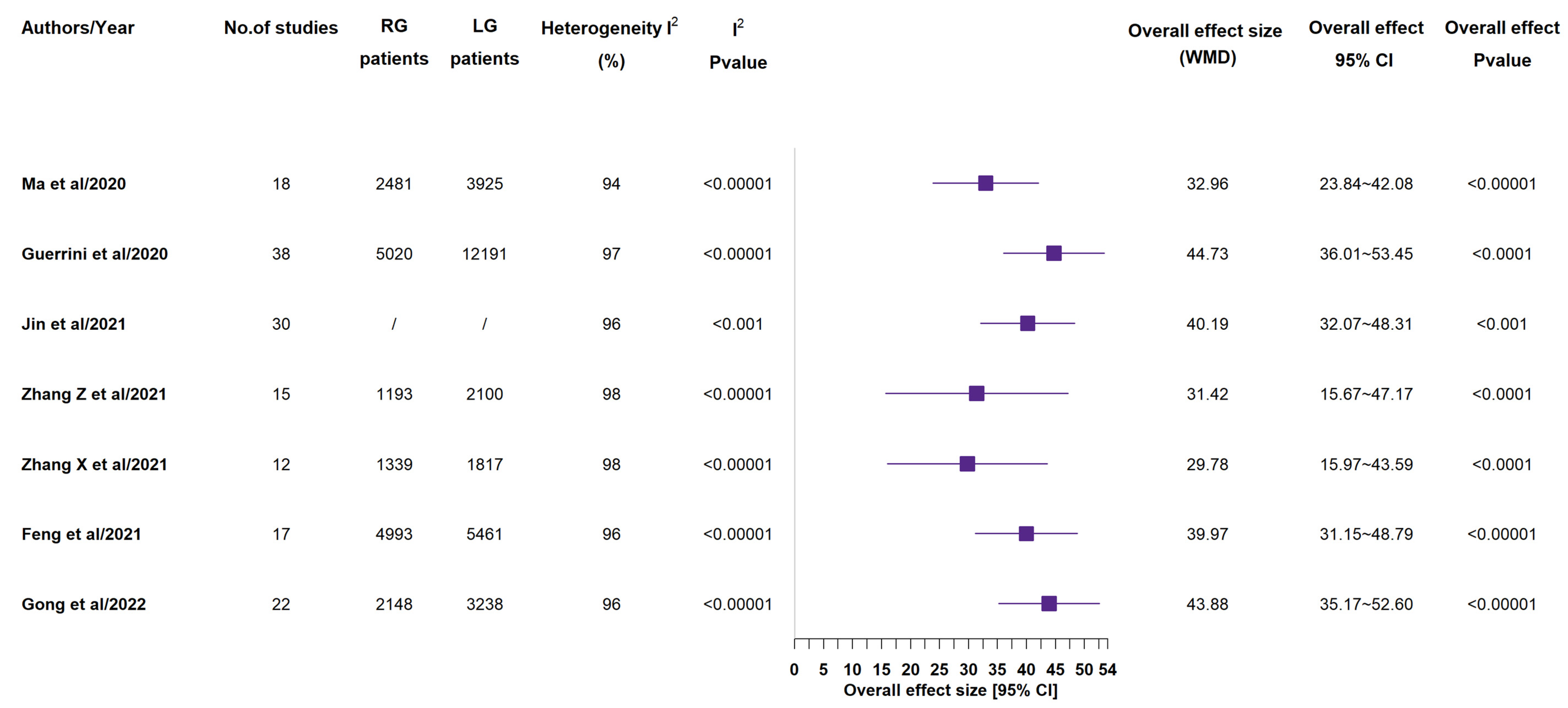
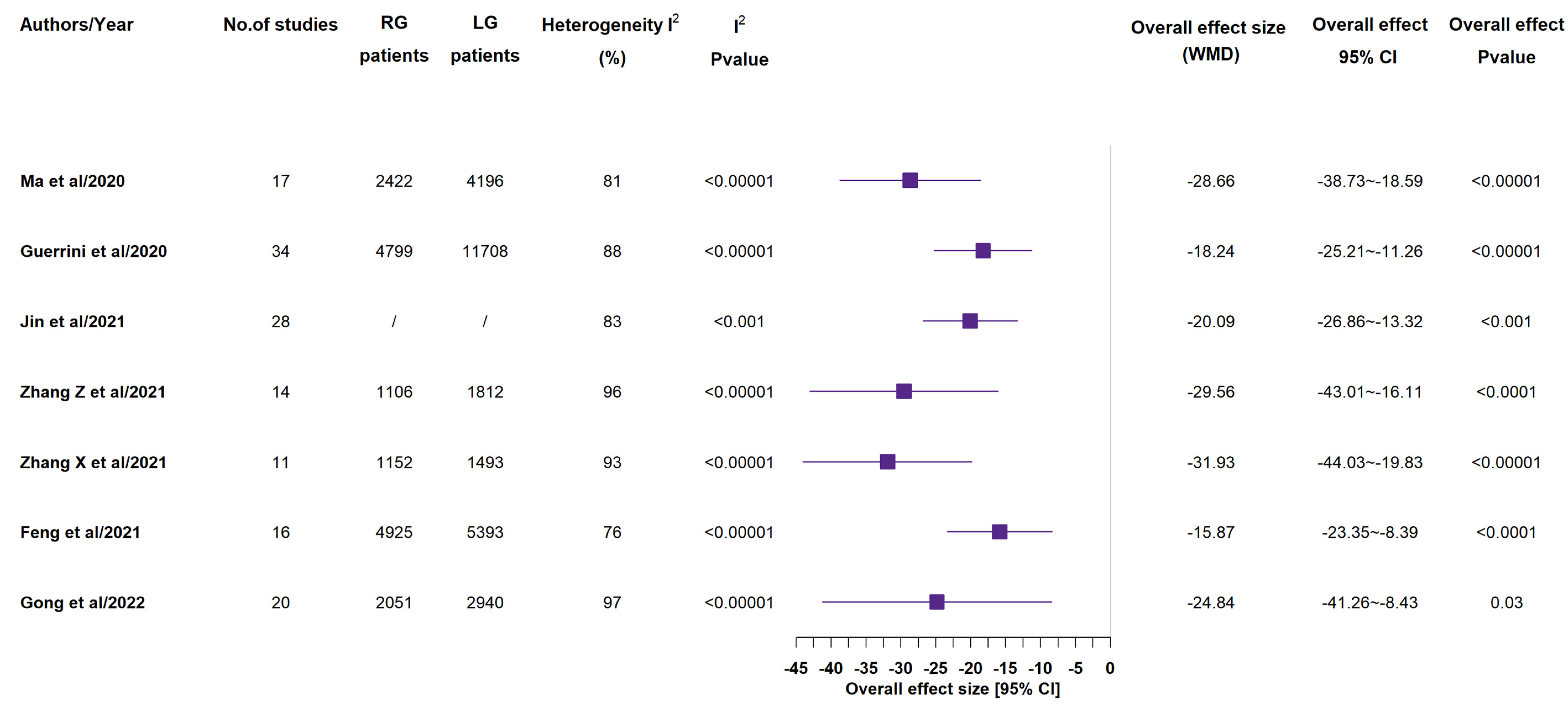
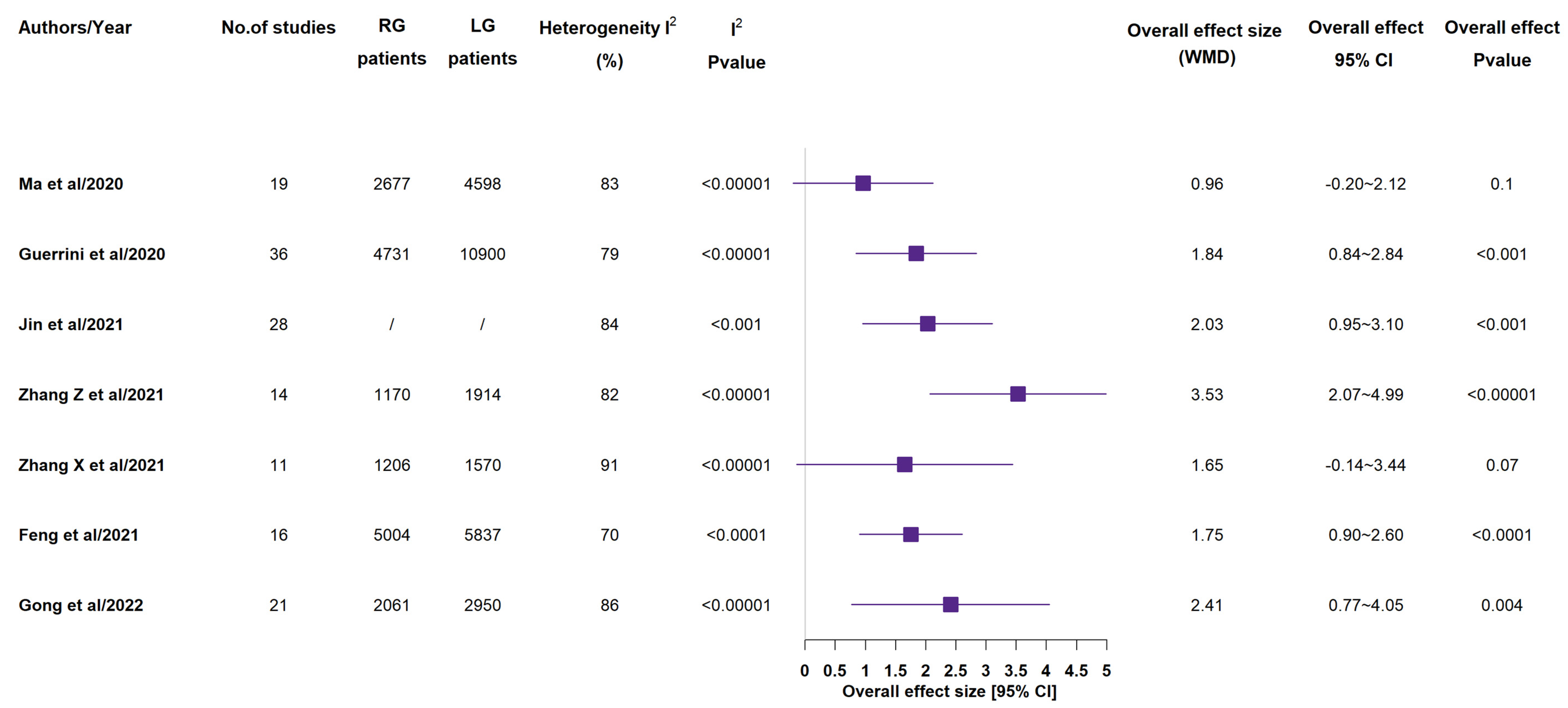
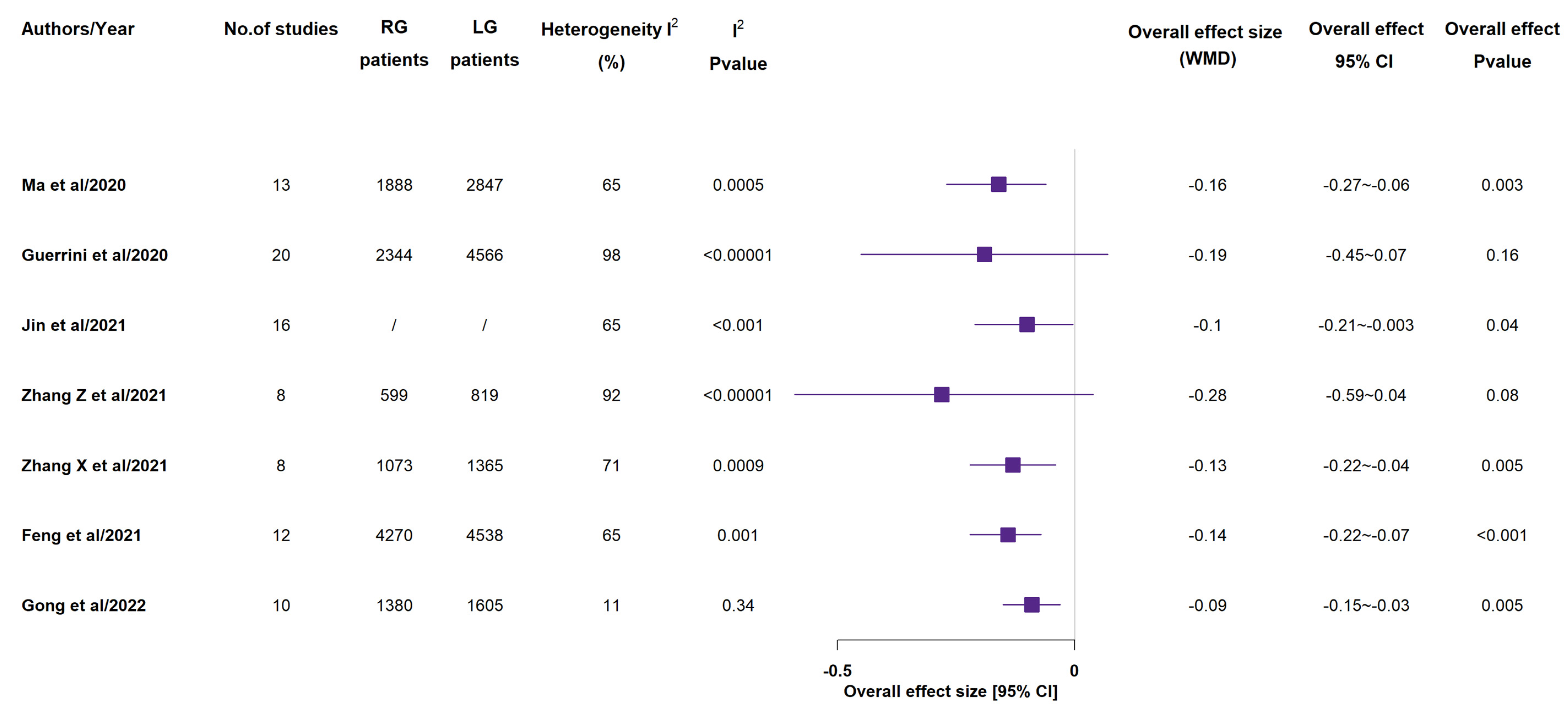
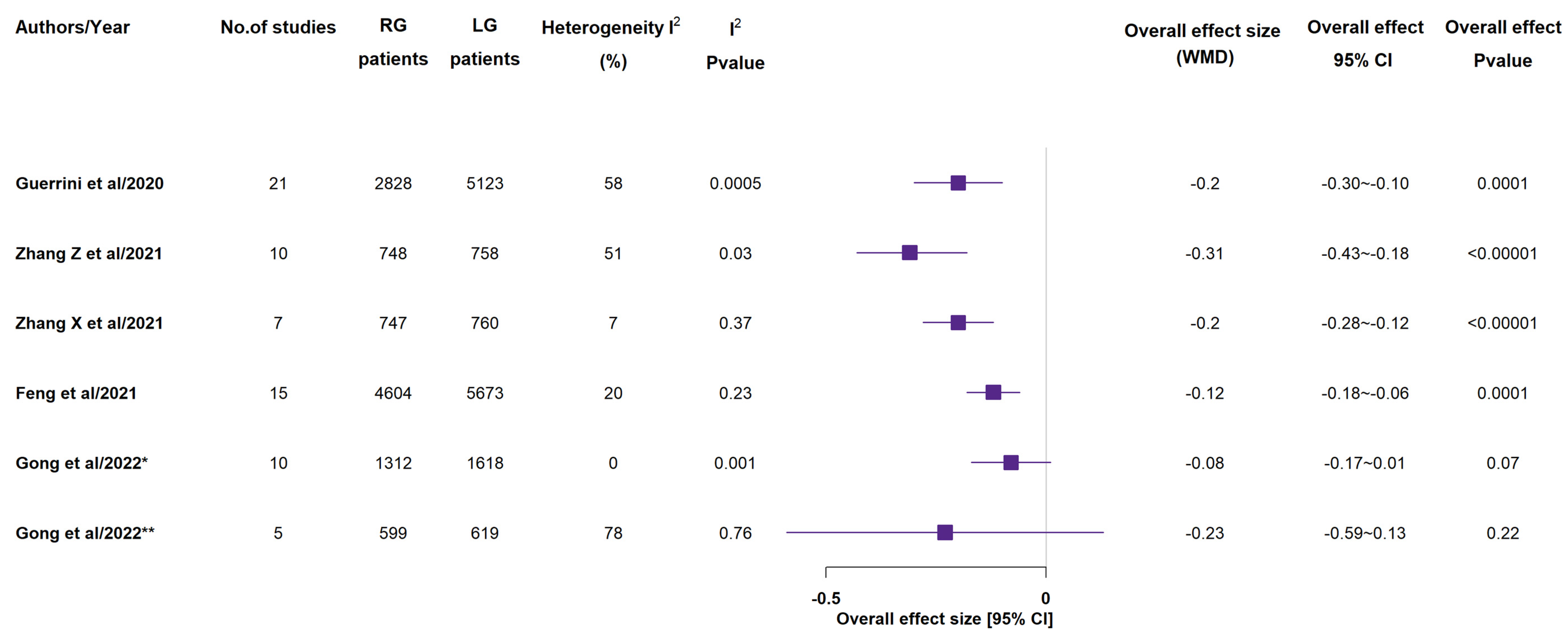
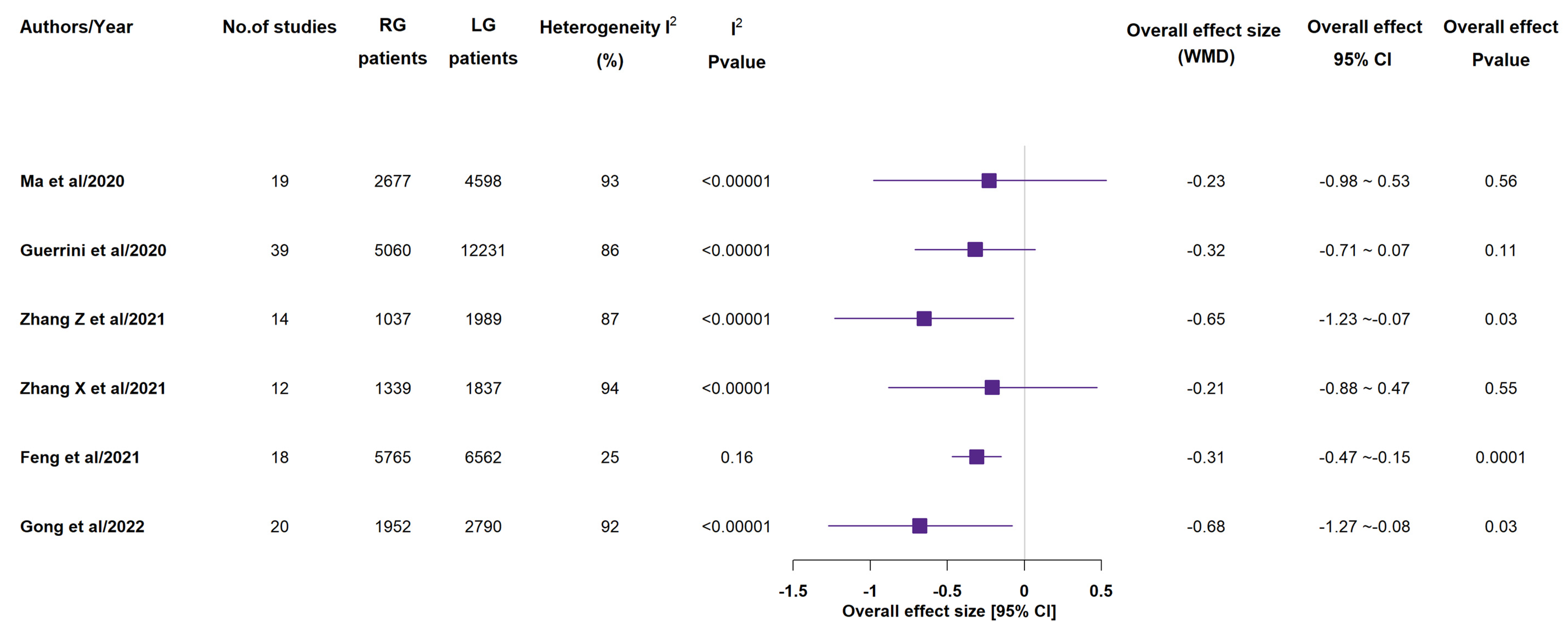
3.3. Operative Outcomes
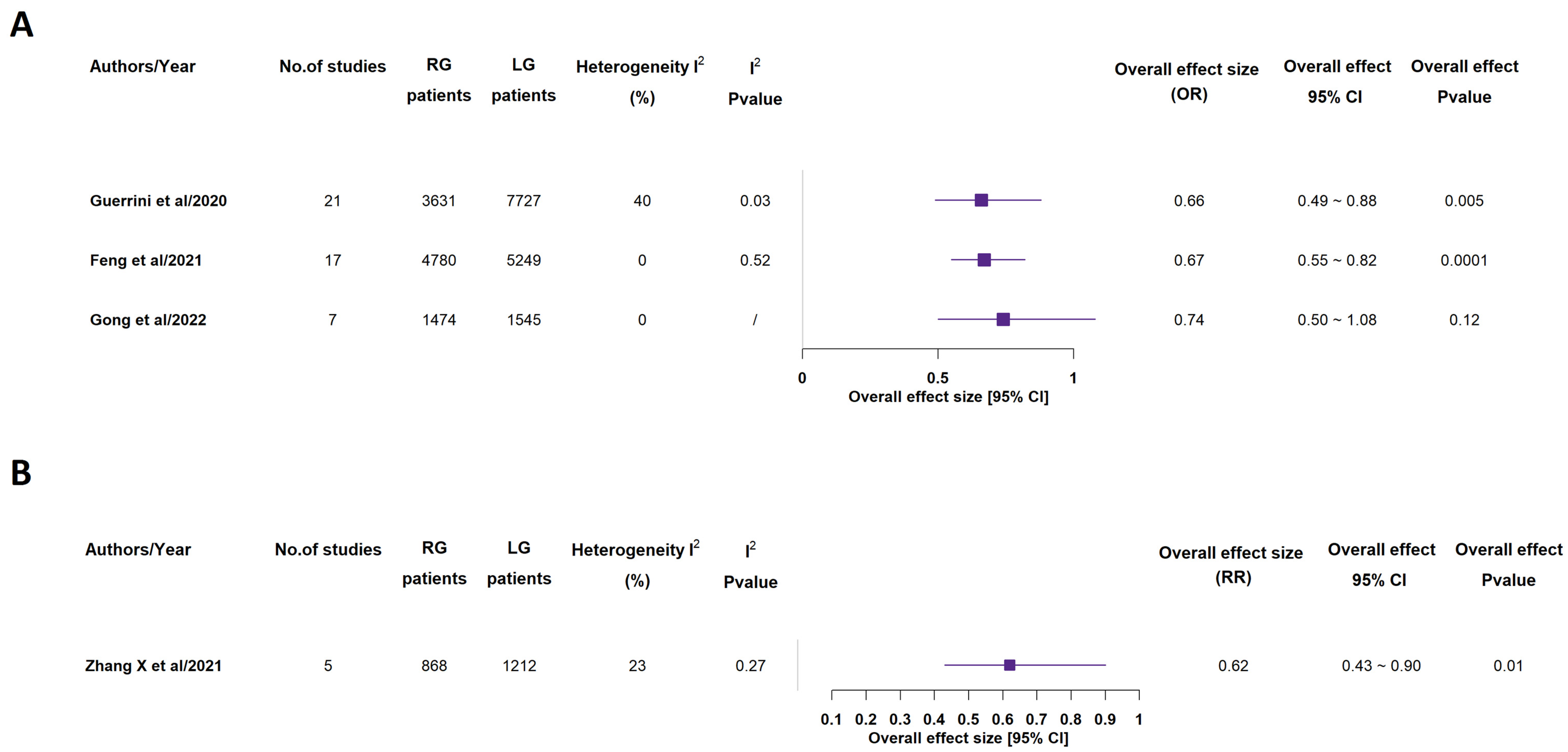
3.4. Perioperative Outcomes
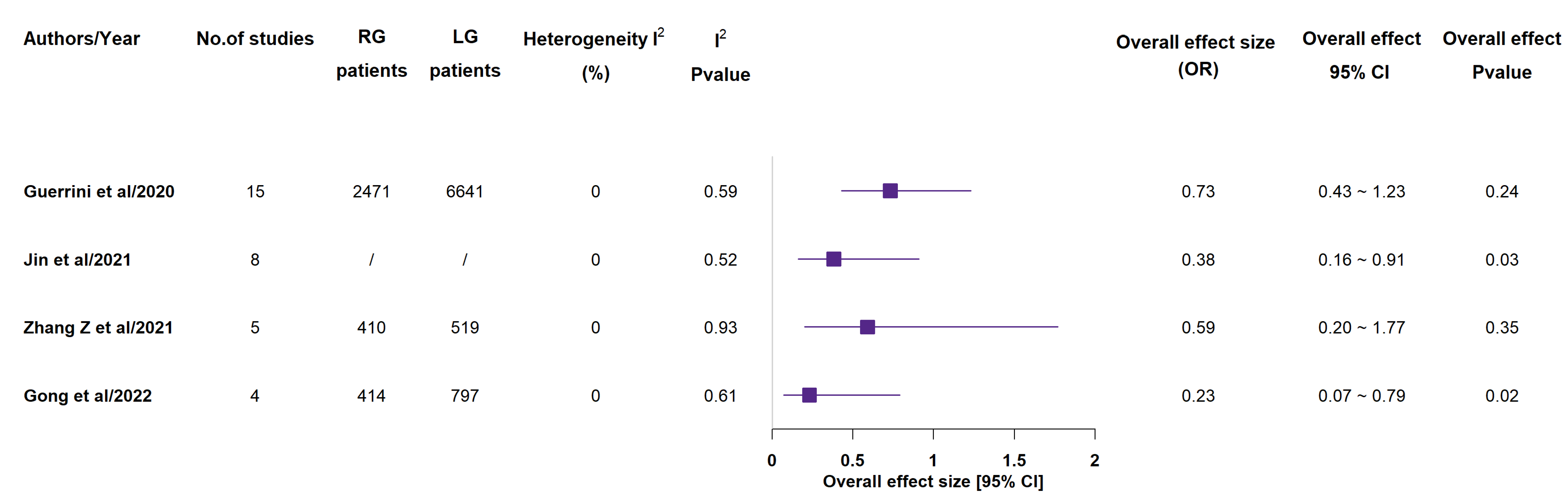
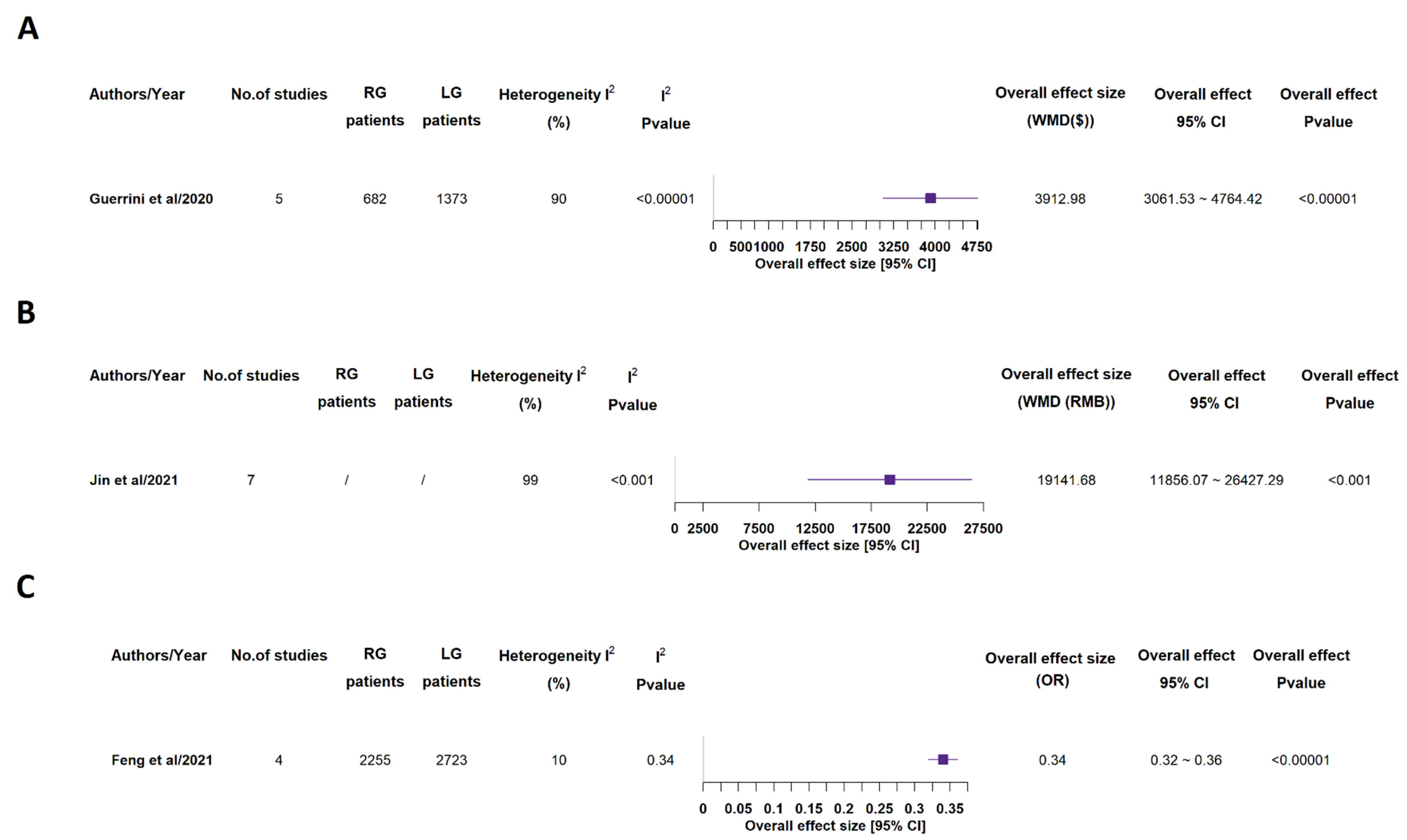
3.5. Long-Term Outcomes and Costs
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smyth, E.C.; Nilsson, M.; Grabsch, H.I.; van Grieken, N.C.; Lordick, F. Gastric cancer. Lancet 2020, 396, 635–648. [Google Scholar] [CrossRef]
- Smyth, E.C.; Verheij, M.; Allum, W.; Cunningham, D.; Cervantes, A.; Arnold, D.; ESMO Guidelines Committee. Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27 (Suppl. S5), v38–v49. [Google Scholar] [CrossRef] [PubMed]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer 2021, 24, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guideline Committee of the Korean Gastric Cancer Association (KGCA); Development Working Group & Review Panel. Korean Practice Guideline for Gastric Cancer 2018: An Evidence-based, Multi-disciplinary Approach. J. Gastric Cancer 2019, 19, 1–48. [Google Scholar] [CrossRef]
- Wang, F.H.; Zhang, X.T.; Li, Y.F.; Tang, L.; Qu, X.J.; Ying, J.E.; Zhang, J.; Sun, L.Y.; Lin, R.B.; Qiu, H.; et al. The Chinese Society of Clinical Oncology (CSCO): Clinical guidelines for the diagnosis and treatment of gastric cancer, 2021. Cancer Commun. 2021, 41, 747–795. [Google Scholar] [CrossRef] [PubMed]
- De Manzoni, G.; Marrelli, D.; Baiocchi, G.L.; Morgagni, P.; Saragoni, L.; Degiuli, M.; Donini, A.; Fumagalli, U.; Mazzei, M.A.; Pacelli, F.; et al. The Italian Research Group for Gastric Cancer (GIRCG) guidelines for gastric cancer staging and treatment: 2015. Gastric Cancer 2017, 20, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Zizzo, M.; Ugoletti, L.; Manzini, L.; Castro Ruiz, C.; Nita, G.E.; Zanelli, M.; De Marco, L.; Besutti, G.; Scalzone, R.; Sassatelli, R.; et al. Management of duodenal stump fistula after gastrectomy for malignant disease: A systematic review of the literature. BMC Surg. 2019, 19, 55. [Google Scholar]
- Marano, L.; Fusario, D.; Savelli, V.; Marrelli, D.; Roviello, F. Robotic versus laparoscopic gastrectomy for gastric cancer: An umbrella review of systematic reviews and meta-analyses. Updates Surg. 2021, 73, 1673–1689. [Google Scholar] [CrossRef]
- Mocan, L. Surgical Management of Gastric Cancer: A Systematic Review. J. Clin. Med. 2021, 10, 2557. [Google Scholar] [CrossRef]
- Agnes, A.; Biondi, A.; Laurino, A.; Persiani, R.; D’Ugo, D. Global updates in the treatment of gastric cancer: A systematic review. Part 1: Staging, classification and surgical treatment. Updates Surg. 2020, 72, 341–353. [Google Scholar] [CrossRef]
- Caruso, S.; Scatizzi, M. Laparoscopic gastrectomy for gastric cancer: Has the time come for considered it a standard procedure? Surg. Oncol. 2022, 40, 101699. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, J.; Li, X.; Zhao, S.; Zhang, R.; Yang, D. Robotic versus laparoscopic gastrectomy for gastric cancer: A systematic review and meta-analysis. World J. Surg. Oncol. 2020, 18, 306. [Google Scholar] [CrossRef] [PubMed]
- Guerrini, G.P.; Esposito, G.; Magistri, P.; Serra, V.; Guidetti, C.; Olivieri, T.; Catellani, B.; Assirati, G.; Ballarin, R.; Di Sandro, S.; et al. Robotic versus laparoscopic gastrectomy for gastric cancer: The largest meta-analysis. Int. J. Surg. 2020, 82, 210–228. [Google Scholar] [CrossRef] [PubMed]
- Jin, T.; Liu, H.D.; Yang, K.; Chen, Z.H.; Zhang, Y.X.; Hu, J.K. Effectiveness and safety of robotic gastrectomy versus laparoscopic gastrectomy for gastric cancer: A meta-analysis of 12,401 gastric cancer patients. Updates Surg. 2022, 74, 267–281. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhang, X.; Liu, Y.; Li, Y.; Zhao, Q.; Fan, L.; Zhang, Z.; Wang, D.; Zhao, X.; Tan, B. Meta-analysis of the efficacy of Da Vinci robotic or laparoscopic distal subtotal gastrectomy in patients with gastric cancer. Medicine 2021, 100, e27012. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, W.; Feng, Z.; Sun, Z.; Zhang, Q.; Ren, S. Comparison of short-term outcomes of robotic-assisted and laparoscopic-assisted D2 gastrectomy for gastric cancer: A meta-analysis. Videosurg. Other Miniinvasive Tech. 2021, 16, 443–454. [Google Scholar] [CrossRef]
- Feng, Q.; Ma, H.; Qiu, J.; Du, Y.; Zhang, G.; Li, P.; Wen, K.; Xie, M. Comparison of Long-Term and Perioperative Outcomes of Robotic Versus Conventional Laparoscopic Gastrectomy for Gastric Cancer: A Systematic Review and Meta-Analysis of PSM and RCT Studies. Front. Oncol. 2021, 11, 759509. [Google Scholar] [CrossRef]
- Gong, S.; Li, X.; Tian, H.; Song, S.; Lu, T.; Jing, W.; Huang, X.; Xu, Y.; Wang, X.; Zhao, K.; et al. Clinical efficacy and safety of robotic distal gastrectomy for gastric cancer: A systematic review and meta-analysis. Surg. Endosc. 2022, 36, 2734–2748. [Google Scholar] [CrossRef]
- Chen, L.; Wang, Q.; Liu, Y.; Wang, Y.; Li, Y.; Dan, J.; Wang, J. A meta-analysis of robotic gastrectomy versus open gastrectomy in gastric cancer treatment. Asian J. Surg. 2022, 45, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Vining, C.C.; Skowron, K.B.; Hogg, M.E. Robotic gastrointestinal surgery: Learning curve, educational programs and outcomes. Updates Surg. 2021, 73, 799–814. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Tanigawa, N. Learning curve of laparoscopic surgery for gastric cancer, a laparoscopic distal gastrectomy-based analysis. Surg. Endosc. 2009, 23, 1259–1264. [Google Scholar] [CrossRef]
- Jung, D.H.; Son, S.Y.; Park, Y.S.; Shin, D.J.; Ahn, H.S.; Ahn, S.H.; Park, D.J.; Kim, H.H. The learning curve associated with laparoscopic total gastrectomy. Gastric Cancer 2016, 19, 264–272. [Google Scholar] [CrossRef]
- Song, J.; Kang, W.H.; Oh, S.J.; Hyung, W.J.; Choi, S.H.; Noh, S.H. Role of robotic gastrectomy using da Vinci system compared with laparoscopic gastrectomy: Initial experience of 20 consecutive cases. Surg. Endosc. 2009, 23, 1204–1211. [Google Scholar] [CrossRef] [PubMed]
- Park, S.S.; Kim, M.C.; Park, M.S.; Hyung, W.J. Rapid adaptation of robotic gastrectomy for gastric cancer by experienced laparoscopic surgeons. Surg. Endosc. 2012, 26, 60–67. [Google Scholar] [CrossRef]
- Kim, M.S.; Kim, W.J.; Hyung, W.J.; Kim, H.I.; Han, S.U.; Kim, Y.W.; Ryu, K.W.; Park, S. Comprehensive Learning Curve of Robotic Surgery: Discovery From a Multicenter Prospective Trial of Robotic Gastrectomy. Ann. Surg. 2021, 273, 949–956. [Google Scholar] [CrossRef]
- Yang, J.; Wang, Z.; Dong, K.; Zhang, R.; Xiao, K.; Shang, L.; Li, L. Safety and efficacy of indocyanine green fluorescence imaging-guided radical gastrectomy: A systematic review and meta-analysis. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 1319–1328. [Google Scholar] [CrossRef]
- Pang, H.Y.; Liang, X.W.; Chen, X.L.; Zhou, Q.; Zhao, L.Y.; Liu, K.; Zhang, W.H.; Yang, K.; Chen, X.Z.; Hu, J.K. Assessment of indocyanine green fluorescence lymphography on lymphadenectomy during minimally invasive gastric cancer surgery: A systematic review and meta-analysis. Surg. Endosc. 2022, 36, 1726–1738. [Google Scholar] [CrossRef]
- Alhossaini, R.M.; Altamran, A.A.; Choi, S.; Roh, C.K.; Seo, W.J.; Cho, M.; Son, T.; Kim, H.I.; Hyung, W.J. Similar Operative Outcomes between the da Vinci Xi® and da Vinci Si® Systems in Robotic Gastrectomy for Gastric Cancer. J. Gastric Cancer 2019, 19, 165–172. [Google Scholar] [CrossRef] [Green Version]
- Ojima, T.; Nakamura, M.; Hayata, K.; Kitadani, J.; Takeuchi, A.; Yamaue, H. Comparison of short-term surgical outcomes using da Vinci S, Si and Xi Surgical System for robotic gastric cancer surgery. Sci. Rep. 2021, 11, 11063. [Google Scholar] [CrossRef] [PubMed]
- Abdel Raheem, A.; Sheikh, A.; Kim, D.K.; Alatawi, A.; Alabdulaali, I.; Han, W.K.; Choi, Y.D.; Rha, K.H. Da Vinci Xi and Si platforms have equivalent perioperative outcomes during robot-assisted partial nephrectomy: Preliminary experience. J. Robot. Surg. 2017, 11, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Kim, H.; Kwak, S.; Baek, K.; Na, G.; Kim, J.H.; Kim, S.H. The Settings, Pros and Cons of the New Surgical Robot da Vinci Xi System for Transoral Robotic Surgery (TORS): A Comparison with the Popular da Vinci Si System. Surg. Laparosc. Endosc. Percutan. Tech. 2016, 26, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Morelli, L.; Guadagni, S.; Di Franco, G.; Palmeri, M.; Caprili, G.; D’Isidoro, C.; Cobuccio, L.; Marciano, E.; Di Candio, G.; Mosca, F. Use of the new da Vinci Xi® during robotic rectal resection for cancer: A pilot matched-case comparison with the da Vinci Si®. Int. J. Med. Robot. 2017, 13, e1728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibasaki, S.; Suda, K.; Obama, K.; Yoshida, M.; Uyama, I. Should robotic gastrectomy become a standard surgical treatment option for gastric cancer? Surg. Today 2020, 50, 955–965. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.M.; Hyung, W.J. Current status of robotic gastrectomy for gastric cancer: Comparison with laparoscopic gastrectomy. Updates Surg. 2021, 73, 853–863. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, G.; Guerra, F.; De Franco, L.; Salvischiani, L.; Benigni, R.; Coratti, A. Review on Perioperative and Oncological Outcomes of Robotic Gastrectomy for Cancer. J. Pers. Med. 2021, 11, 638. [Google Scholar] [CrossRef]
- Chen, Q.Y.; Zhong, Q.; Liu, Z.Y.; Li, P.; Wang, J.B.; Lin, J.X.; Lu, J.; Cao, L.L.; Lin, M.; Tu, R.H.; et al. Surgical Outcomes, Technical Performance and Surgery Burden of Robotic Total Gastrectomy for Locally Advanced Gastric Cancer: A Prospective Study. Ann. Surg. 2021, 11, 638. [Google Scholar] [CrossRef]
- Li, Z.; Qian, F.; Zhao, Y.; Chen, J.; Zhang, F.; Li, Z.; Wang, X.; Li, P.; Liu, J.; Wen, Y.; et al. A comparative study on perioperative outcomes between robotic versus laparoscopic D2 total gastrectomy. Int. J. Surg. 2022, 102, 106636. [Google Scholar] [CrossRef]
- Regione Emilia-Romagna. Available online: https://www.regione.emilia-romagna.it/notizie/2021/marzo/covid-il-grazie-a-tutto-il-personale-sanitario-della-nazionale-di-calcio-all-ospedale-maggiore-di-parma/chirurgia-robotica-in-emilia-romagna.pdf (accessed on 1 April 2022).
- Gkegkes, I.D.; Mamais, I.A.; Iavazzo, C. Robotics in general surgery: A systematic cost assessment. J. Minimal Access Surg. 2017, 13, 243–255. [Google Scholar] [CrossRef]
- Van Dam, P.; Hauspy, J.; Verkinderen, L.; Trinh, B.; Looy, L.V.; Dirix, L. Do Costs of Robotic Surgery Matter? In Advanced Gynecologic Endoscopy; Darwish, A., Ed.; IntechOpen: London, UK, 2011; Available online: https://www.intechopen.com/chapters/18360 (accessed on 1 April 2022). [CrossRef] [Green Version]
- Van Dam, P.; Hauspy, J.; Verkinderen, L.; Trinh, X.B.; van Dam, P.J.; Van Looy, L.; Dirix, L. Are costs of robot-assisted surgery warranted for gynecological procedures? Obstet. Gynecol. Int. 2011, 2011, 973830. [Google Scholar] [CrossRef] [PubMed] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors/Year | Database | Studies Included | Surgical Extension | Patient Population | AMSTAR-2 | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number | Type | Period | Country | Language | P | D | T | PPG | Not Described | Overall | RG | LG | ||||||||||
| Restrospective | Prospective | RCT | China | Japan | Korea | Taiwan | Italy | USA | ||||||||||||||
| Ma et al./2020 [14] | Pubmed, Cochrane Library, WanFang, CNKI, VIP | 19 | 19 | 0 | 0 | 2003–2019 | 13 | 2 | 4 | 0 | 0 | 0 | English, Chinese | 7 | 17 | 14 | 1 | 0 | 7275 | 2677 | 4598 | Low |
| Guerrini et al./2020 [15] | Pubmed, MEDLINE, Cochrane Library | 40 | 11 | 29 | 0 | 2003–2019 | 8 | 7 | 21 | 1 | 3 | 0 | English | 5 | 36 | 28 | 2 | 0 | 17,712 | 5402 | 12,310 | Low |
| Jin et al./2021 [16] | Pubmed, Embase, Cochrane Library | 31 | 30 | 0 | 1 | / | 13 | 3 | 12 | 0 | 2 | 1 | English | / | 6 | 3 | / | 22 | 12,401 | 4274 | 8127 | Low |
| Zhang Z et al./2021 [17] | Pubmed, Embase, Cochrane Library, Web of Science | 15 | 15 | 0 | 0 | 2003–2018 | 9 | 1 | 5 | 0 | 1 | 0 | English, Chinese | 0 | 15 | 0 | 0 | 0 | 3293 | 1193 | 2100 | Low |
| Zhang X et al./2021 [18] | Pubmed, Embase Cochrane Library, WanFang, CNKI, VIP | 12 | 12 | 0 | 0 | 2000–2019 | 10 | 0 | 1 | 0 | 1 | 0 | All | 1 | 9 | 4 | / | 2 | 3176 | 1339 | 1837 | Low |
| Feng et al./2021 [19] | Pubmed, Embase, Cochrane Library, Web of Science | 20 | 19 | 1 | 2005–2020 | 11 | 2 | 5 | 0 | 1 | 1 | English | / | / | / | / | 20 | 13,446 | 6173 | 7273 | High | |
| Gong et al./2022 [20] | Pubmed, Embase, Cochrane Library, Web of Science | 22 | 22 | 0 | 0 | 2000–2020 | 5 | 5 | 9 | 0 | 3 | 0 | English | 0 | 22 | 0 | 0 | 0 | 5386 | 2148 | 3238 | High |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zizzo, M.; Zanelli, M.; Sanguedolce, F.; Torricelli, F.; Morini, A.; Tumiati, D.; Mereu, F.; Zuliani, A.L.; Palicelli, A.; Ascani, S.; et al. Robotic versus Laparoscopic Gastrectomy for Gastric Cancer: An Updated Systematic Review. Medicina 2022, 58, 834. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060834
Zizzo M, Zanelli M, Sanguedolce F, Torricelli F, Morini A, Tumiati D, Mereu F, Zuliani AL, Palicelli A, Ascani S, et al. Robotic versus Laparoscopic Gastrectomy for Gastric Cancer: An Updated Systematic Review. Medicina. 2022; 58(6):834. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060834
Chicago/Turabian StyleZizzo, Maurizio, Magda Zanelli, Francesca Sanguedolce, Federica Torricelli, Andrea Morini, David Tumiati, Federica Mereu, Antonia Lavinia Zuliani, Andrea Palicelli, Stefano Ascani, and et al. 2022. "Robotic versus Laparoscopic Gastrectomy for Gastric Cancer: An Updated Systematic Review" Medicina 58, no. 6: 834. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060834