
Silent Pauses and Speech Indices as Biomarkers for Primary Progressive Aphasia

 , , , ,
, , , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Language Assessment
2.3. Speech Analysis
2.4. Statistical Analysis
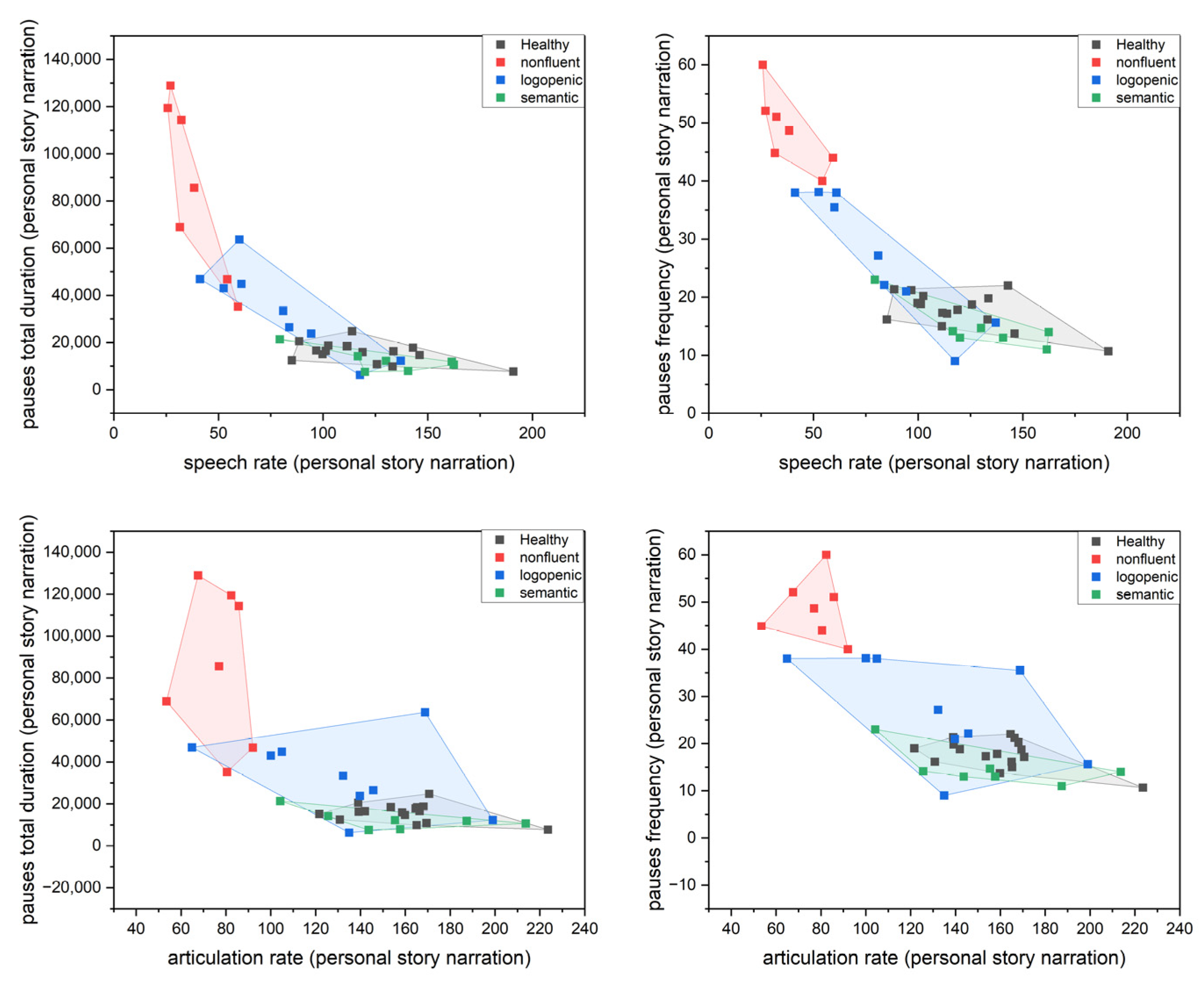
3. Results
3.1. One-Way ANOVA
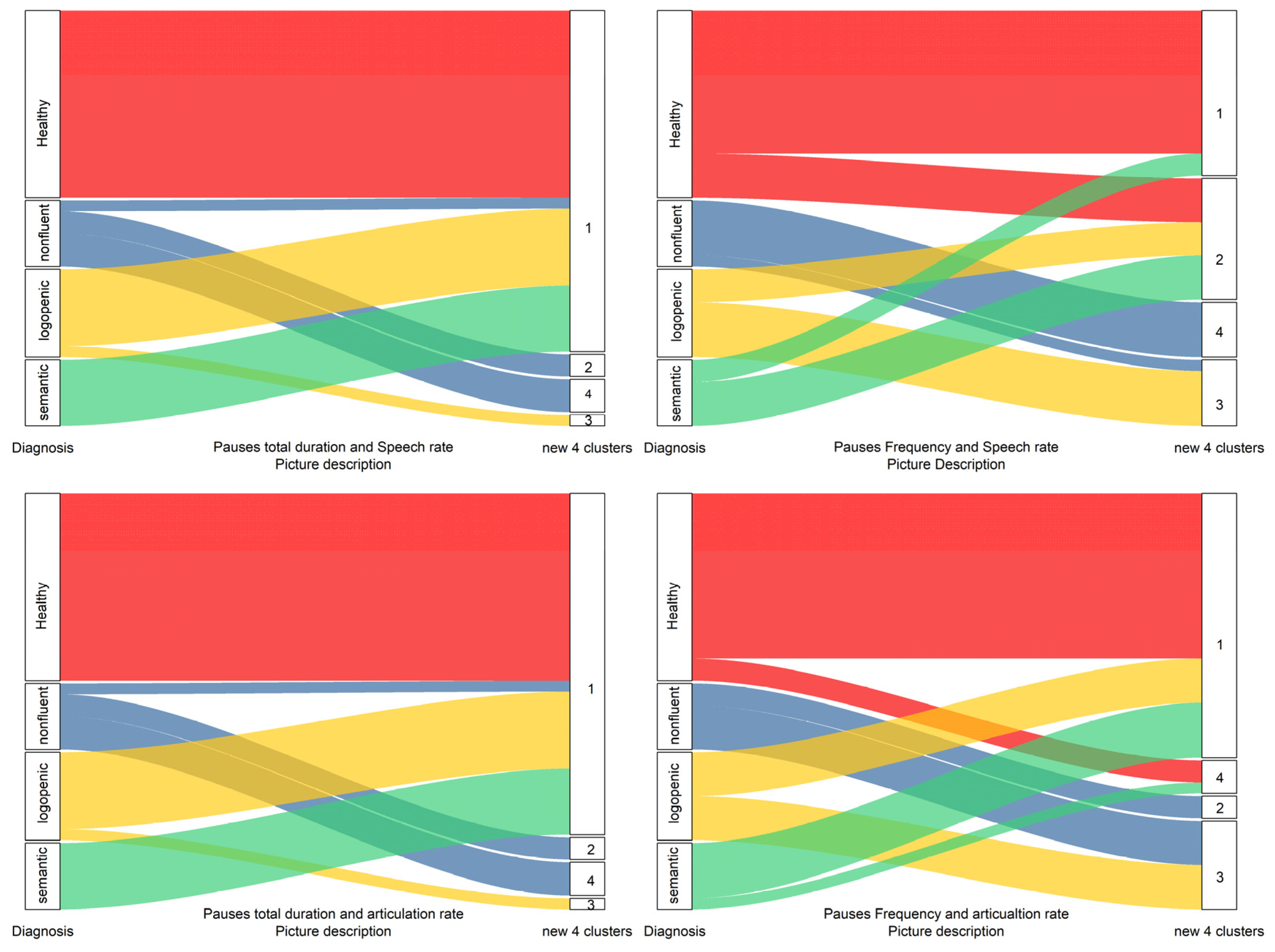
3.2. Hierarchical Cluster Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mesulam, M.M. Primary progressive aphasia. Ann. Neurol. 2001, 49, 425–432. [Google Scholar] [CrossRef]
- Hodges, J.R.; Davies, R.R.; Xuereb, J.H.; Casey, B.; Broe, M.; Bak, T.H.; Kril, J.J.; Halliday, G.M. Clinicopathological correlates in frontotemporal dementia. Ann. Neurol. 2004, 56, 399–406. [Google Scholar] [CrossRef]
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of primary progressive aphasia and its variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef]
- Mesulam, M.M.; Weintraub, S.; Rogalski, E.J.; Wieneke, C.; Geula, C.; Bigio, E.H. Asymmetry and heterogeneity of Alzheimer’s and frontotemporal pathology in primary progressive aphasia. Brain 2014, 137, 1176–1192. [Google Scholar] [CrossRef] [PubMed]
- Mesulam, M.M.; Rogalski, E.J.; Wieneke, C.; Hurley, R.S.; Geula, C.; Bigio, E.H.; Thompson, C.K.; Weintraub, S. Primary progressive aphasia and the evolving neurology of the language network. Nat. Rev. Neurol. 2014, 10, 554–569. [Google Scholar] [CrossRef]
- Grossman, M. The non-fluent/agrammatic variant of primary progressive aphasia. Lancet Neurol. 2012, 11, 545–555. [Google Scholar] [CrossRef]
- Gorno-Tempini, M.L.; Brambati, S.M.; Ginex, V.; Ogar, J.; Dronkers, N.F.; Marcone, A.; Perani, D.; Garibotto, V.; Cappa, S.F.; Miller, B.L. The logopenic/phonological variant of primary progressive aphasia. Neurology 2008, 71, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Henry, M.L.; Gorno-Tempini, M.L. The logopenic variant of primary progressive aphasia. Curr. Opin. Neurol. 2010, 23, 633. [Google Scholar] [CrossRef] [PubMed]
- Teichmann, M.; Kas, A.; Boutet, C.; Ferrieux, S.; Nogues, M.; Samri, D.; Rogan, C.; Dormont, D.; Dubois, B.; Migliaccio, R. Deciphering logopenic primary progressive aphasia: A clinical, imaging and biomarker investigation. Brain 2013, 136, 3474–3488. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, D.; Gorno-Tempini, M.L.; Rabinovici, G.D.; Santos-Santos, M.A.; Seeley, W.; Miller, B.L.; Pijnenburg, Y.; Keulen, M.A.; Groot, C.; van Berckel, B.N.; et al. Prevalence of amyloid-β pathology in distinct variants of primary progressive aphasia. Ann. Neurol. 2018, 84, 729–740. [Google Scholar] [CrossRef] [Green Version]
- Snowden, J.; Goulding, P.J.; David, N. Semantic dementia: A form of circumscribed cerebral atrophy. Behav. Neurol. 1989, 2, 167–182. [Google Scholar] [CrossRef]
- Hodges, J.R.; Patterson, K.; Oxbury, S.; Funnell, E. Semantic dementia: Progressive fluent aphasia with temporal lobe atrophy. Brain 1992, 115, 1783–1806. [Google Scholar] [CrossRef] [PubMed]
- Mesulam, M.; Rogalski, E.; Wieneke, C.; Cobia, D.; Rademaker, A.; Thompson, C.; Weintraub, S. Neurology of anomia in the semantic variant of primary progressive aphasia. Brain 2009, 132, 2553–2565. [Google Scholar] [CrossRef] [PubMed]
- Suárez-González, A.; Savage, S.A.; Bier, N.; Henry, M.L.; Jokel, R.; Nickels, L.; Taylor-Rubin, C. Semantic variant primary progressive aphasia: Practical recommendations for treatment from 20 years of behavioural research. Brain Sci. 2021, 11, 1552. [Google Scholar] [CrossRef]
- Collins, J.A.; Montal, V.; Hochberg, D.; Quimby, M.; Mandelli, M.L.; Makris, N.; Seeley, W.W.; Gorno-Tempini, M.L.; Dickerson, B.C. Focal temporal pole atrophy and network degeneration in semantic variant primary progressive aphasia. Brain 2017, 140, 457–471. [Google Scholar] [CrossRef]
- Iaccarino, L.; Crespi, C.; Della Rosa, P.A.; Catricala, E.; Guidi, L.; Marcone, A.; Tagliavini, F.; Magnani, G.; Cappa, S.F.; Perani, D. The semantic variant of primary progressive aphasia: Clinical and neuroimaging evidence in single subjects. PLoS ONE 2015, 10, e0120197. [Google Scholar] [CrossRef]
- Agosta, F.; Galantucci, S.; Canu, E.; Cappa, S.F.; Magnani, G.; Franceschi, M.; Falini, A.; Comi, G.; Filippi, M. Disruption of structural connectivity along the dorsal and ventral language pathways in patients with nonfluent and semantic variant primary progressive aphasia: A DT MRI study and a literature review. Brain Lang. 2013, 127, 157–166. [Google Scholar] [CrossRef]
- Mesulam, M.M.; Weintraub, S. Is it time to revisit the classification guidelines for primary progressive aphasia? Neurology 2014, 82, 1108–1109. [Google Scholar] [CrossRef]
- Wicklund, M.R.; Duffy, J.R.; Strand, E.A.; Machulda, M.M.; Whitwell, J.L.; Josephs, K.A. Quantitative application of the primary progressive aphasia consensus criteria. Neurology 2014, 82, 1119–1126. [Google Scholar] [CrossRef]
- Botha, H.; Duffy, J.R.; Whitwell, J.L.; Strand, E.A.; Machulda, M.M.; Schwarz, C.G.; Reid, R.I.; Spychalla, A.J.; Senjem, M.L.; Jones, D.T.; et al. Classification and clinicoradiologic features of primary progressive aphasia (PPA) and apraxia of speech. Cortex 2015, 69, 220–236. [Google Scholar] [CrossRef] [Green Version]
- Flanagan, E.P.; Duffy, J.R.; Whitwell, J.L.; Vemuri, P.; Dickson, D.W.; Josephs, K.A. Mixed tau and TDP-43 pathology in a patient with unclassifiable primary progressive aphasia. Neurocase 2016, 22, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, H.; Hikida, S.; Ikeda, M.; Mori, E. Unclassified fluent variants of primary progressive aphasia: Distinction from semantic and logopenic variants. Brain Commun. 2022, 4, fcac015. [Google Scholar] [CrossRef]
- Clark, H.M.; Utianski, R.L.; Duffy, J.R.; Strand, E.A.; Botha, H.; Josephs, K.A.; Whitwell, J.L. Western Aphasia Battery–Revised profiles in primary progressive aphasia and primary progressive apraxia of speech. Am. J. Speech-Lang. Pathol. 2020, 29 (Suppl. S1), 498–510. [Google Scholar] [CrossRef] [PubMed]
- Utianski, R.L.; Botha, H.; Martin, P.R.; Schwarz, C.G.; Duffy, J.R.; Clark, H.M.; Machulda, M.M.; Butts, A.M.; Lowe, V.J.; Jack, C.R., Jr.; et al. Clinical and neuroimaging characteristics of clinically unclassifiable primary progressive aphasia. Brain Lang. 2019, 197, 104676. [Google Scholar] [CrossRef]
- De la Sablonnière, J.; Tastevin, M.; Lavoie, M.; Laforce, R., Jr. Longitudinal changes in cognition, behaviours, and functional abilities in the three main variants of primary progressive aphasia: A literature review. Brain Sci. 2021, 11, 1209. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.M.; Henry, M.L.; Besbris, M.; Ogar, J.M.; Dronkers, N.F.; Jarrold, W.; Miller, B.L.; Gorno-Tempini, M.L. Connected speech production in three variants of primary progressive aphasia. Brain 2010, 133, 2069–2088. [Google Scholar] [CrossRef] [PubMed]
- Ash, S.; Evans, E.; O’Shea, J.; Powers, J.; Boller, A.; Weinberg, D.; Haley, J.; McMillan, C.; Irwin, D.J.; Rascovsky, K.; et al. Differentiating primary progressive aphasias in a brief sample of connected speech. Neurology 2013, 81, 329–336. [Google Scholar] [CrossRef]
- Fraser, K.C.; Meltzer, J.A.; Graham, N.L.; Leonard, C.; Hirst, G.; Black, S.E.; Rochon, E. Automated classification of primary progressive aphasia subtypes from narrative speech transcripts. Cortex 2014, 55, 43–60. [Google Scholar] [CrossRef]
- Themistocleous, C.; Webster, K.; Afthinos, A.; Tsapkini, K. Part of speech production in patients with primary progressive aphasia: An analysis based on natural language processing. Am. J. Speech-Lang. Pathol. 2021, 30 (Suppl. S1), 466–480. [Google Scholar] [CrossRef]
- Nevler, N.; Ash, S.; Irwin, D.J.; Liberman, M.; Grossman, M. Validated automatic speech biomarkers in primary progressive aphasia. Ann. Clin. Transl. Neurol. 2019, 6, 4–14. [Google Scholar] [CrossRef]
- Dalton, S.G.; Shultz, C.; Henry, M.L.; Hillis, A.E.; Richardson, J.D. Describing phonological paraphasias in three variants of primary progressive aphasia. Am. J. Speech-Lang. Pathol. 2018, 27 (Suppl. S1), 336–349. [Google Scholar] [CrossRef] [PubMed]
- Goldman-Eisler, F. Pauses, clauses, sentences. Lang. Speech 1972, 15, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Butterworth, B. Hesitation and semantic planning in speech. J. Psycholinguist. Res. 1975, 4, 75–87. [Google Scholar] [CrossRef]
- Beattie, G.W.; Butterworth, B.L. Contextual probability and word frequency as determinants of pauses and errors in spontaneous speech. Lang. Speech 1979, 22, 201–211. [Google Scholar] [CrossRef]
- Angelopoulou, G.; Kasselimis, D.; Makrydakis, G.; Varkanitsa, M.; Roussos, P.; Goutsos, D.; Evdokimidis, I.; Potagas, C. Silent pauses in aphasia. Neuropsychologia 2018, 114, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Pistono, A.; Jucla, M.; Barbeau, E.J.; Saint-Aubert, L.; Lemesle, B.; Calvet, B.; Köpke, B.; Puel, M.; Pariente, J. Pauses during autobiographical discourse reflect episodic memory processes in early Alzheimer’s disease. J. Alzheimers Dis. 2016, 50, 687–698. [Google Scholar] [CrossRef]
- DeDe, G.; Salis, C. Temporal and episodic analyses of the story of Cinderella in latent aphasia. Am. J. Speech-Lang. Pathol. 2020, 29 (Suppl. S1), 449–462. [Google Scholar] [CrossRef]
- Hird, K.; Kirsner, K. Objective measurement of fluency in natural language production: A dynamic systems approach. J. Neurolinguistics 2010, 23, 518–530. [Google Scholar] [CrossRef]
- Pistono, A.; Pariente, J.; Bézy, C.; Lemesle, B.; Le Men, J.; Jucla, M. What happens when nothing happens? An investigation of pauses as a compensatory mechanism in early Alzheimer’s disease. Neuropsychologia 2019, 124, 133–143. [Google Scholar] [CrossRef]
- Çokal, D.; Zimmerer, V.; Turkington, D.; Ferrier, N.; Varley, R.; Watson, S.; Hinzen, W. Disturbing the rhythm of thought: Speech pausing patterns in schizophrenia, with and without formal thought disorder. PLoS ONE 2019, 14, e0217404. [Google Scholar] [CrossRef]
- Mack, J.E.; Chandler, S.D.; Meltzer-Asscher, A.; Rogalski, E.; Weintraub, S.; Mesulam, M.M.; Thompson, C.K. What do pauses in narrative production reveal about the nature of word retrieval deficits in PPA? Neuropsychologia 2015, 77, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Nevler, N.; Ash, S.; Cho, S.; Shellikeri, S.; Parjane, N.; Irwin, D.J.; Liberman, M.Y.; Grossman, M. A longitudinal study of automated analysis of acoustic speech markers in FTD and PPA: Biomarkers (non-neuroimaging)/Longitudinal change over time. Alzheimers Dement. 2020, 16, e045315. [Google Scholar] [CrossRef]
- Da Cunha, E.; Plonka, A.; Arslan, S.; Mouton, A.; Meyer, T.; Robert, P.; Meunier, F.; Manera, V.; Gros, A. Logogenic Primary Progressive Aphasia or Alzheimer Disease: Contribution of Acoustic Markers in Early Differential Diagnosis. Life 2022, 12, 933. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, E. Aphasic discourse analysis: The story so far. Aphasiology 2000, 14, 875–892. [Google Scholar] [CrossRef]
- Bliss, L.S.; McCabe, A. Comparison of discourse genres: Clinical implications. Contemp. Issues Commun. Sci. Disord. 2006, 33, 126–167. [Google Scholar] [CrossRef]
- Fergadiotis, G.; Wright, H.H. Lexical diversity for adults with and without aphasia across discourse elicitation tasks. Aphasiology 2011, 25, 1414–1430. [Google Scholar] [CrossRef] [PubMed]
- Ulatowska, H.K.; North, A.J.; Macaluso-Haynes, S. Production of narrative and procedural discourse in aphasia. Brain Lang. 1981, 13, 345–371. [Google Scholar] [CrossRef]
- Li, E.C.; Ritterman, S.; Della Volpe, A.; Williams, S. Variation in grammatic complexity across three types of discourse. J. Speech-Lang. Pathol. Audiol. 1996, 20, 180–186. [Google Scholar]
- Lavoie, M.; Black, S.E.; Tang-Wai, D.F.; Graham, N.L.; Stewart, S.; Leonard, C.; Rochon, E. Description of connected speech across different elicitation tasks in the logopenic variant of primary progressive aphasia. Int. J. Lang. Commun. Disord. 2021, 56, 1074–1085. [Google Scholar] [CrossRef]
- Haley, K.L.; Jacks, A.; Jarrett, J.; Ray, T.; Cunningham, K.T.; Gorno-Tempini, M.L.; Henry, M.L. Speech metrics and samples that differentiate between nonfluent/agrammatic and logopenic variants of primary progressive aphasia. J. Speech Lang. Hear. Res. 2021, 64, 754–775. [Google Scholar] [CrossRef]
- Boschi, V.; Catricala, E.; Consonni, M.; Chesi, C.; Moro, A.; Cappa, S.F. Connected speech in neurodegenerative language disorders: A review. Front. Psychol. 2017, 8, 269. [Google Scholar] [CrossRef] [Green Version]
- Paraskevas, G.P.; Kasselimis, D.; Kourtidou, E.; Constantinides, V.; Bougea, A.; Potagas, C.; Evdokimidis, I.; Kapaki, E. Cerebrospinal fluid biomarkers as a diagnostic tool of the underlying pathology of primary progressive aphasia. J. Alzheimers Dis. 2017, 55, 1453–1461. [Google Scholar] [CrossRef] [PubMed]
- Goodglass, H.; Kaplan, E. The Assessment of Aphasia and Related Disorders; Lea & Febiger: Philadelphia, PA, USA, 1972. [Google Scholar]
- Tsapkini, K.; Vlahou, C.H.; Potagas, C. Adaptation and validation of standardized aphasia tests in different languages: Lessons from the Boston Diagnostic Aphasia Examination–Short Form in Greek. Behav. Neurol. 2009, 22, 111–119. [Google Scholar] [CrossRef]
- Efthymiopoulou, E.; Kasselimis, D.S.; Ghika, A.; Kyrozis, A.; Peppas, C.; Evdokimidis, I.; Petrides, M.; Potagas, C. The effect of cortical and subcortical lesions on spontaneous expression of memory-encoded and emotionally infused information: Evidence for a role of the ventral stream. Neuropsychologia 2017, 101, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Angelopoulou, G.; Meier, E.L.; Kasselimis, D.; Pan, Y.; Tsolakopoulos, D.; Velonakis, G.; Karavasilis, E.; Kelekis, N.L.; Goutsos, D.; Potagas, C.; et al. Investigating gray and white matter structural substrates of sex differences in the narrative abilities of healthy adults. Front. Neurosci. 2020, 13, 1424. [Google Scholar] [CrossRef]
- García, A.M.; Welch, A.E.; Mandelli, M.L.; Henry, M.L.; Lukic, S.; Prioris, M.J.; Deleon, J.; Ratnasiri, B.M.; Puls, D.L.; Miller, B.L.; et al. Automated detection of speech timing alterations in autopsy-confirmed non-fluent/agrammatic variant primary progressive aphasia. Neurology 2022, 99, e500–e511. [Google Scholar] [CrossRef]
- Slegers, A.; Filiou, R.P.; Montembeault, M.; Brambati, S.M. Connected speech features from picture description in Alzheimer’s disease: A systematic review. J. Alzheimers Dis. 2018, 65, 519–542. [Google Scholar] [CrossRef]
- Cordella, C.; Dickerson, B.C.; Quimby, M.; Yunusova, Y.; Green, J.R. Slowed articulation rate is a sensitive diagnostic marker for identifying non-fluent primary progressive aphasia. Aphasiology 2017, 31, 241–260. [Google Scholar] [CrossRef]
- Cordella, C.; Quimby, M.; Touroutoglou, A.; Brickhouse, M.; Dickerson, B.C.; Green, J.R. Quantification of motor speech impairment and its anatomic basis in primary progressive aphasia. Neurology 2019, 92, e1992–e2004. [Google Scholar] [CrossRef]
- Miller, J.L.; Grosjean, F.; Lomanto, C. Articulation rate and its variability in spontaneous speech: A reanalysis and some implications. Phonetica 1984, 41, 215–225. [Google Scholar] [CrossRef]
- Bislick, L.; Hula, W.D. Perceptual characteristics of consonant production in apraxia of speech and aphasia. Am. J. Speech-Lang. Pathol. 2019, 28, 1411–1431. [Google Scholar] [CrossRef]
- Schenk, T. Apraxia and the representation of knowledge: Where is the boundary between the cognitive and the motor domain? Cortex A J. Devoted Study Nerv. Syst. Behav. 2014, 57, 290–308. [Google Scholar] [CrossRef]
- Goldman-Eisler, F. The determinants of the rate of speech output and their mutual relations. J. Psychosom. Res. 1956, 1, 137–143. [Google Scholar] [CrossRef]
- Goldman-Eisler, F. The significance of changes in the rate of articulation. Lang. Speech 1961, 4, 171–174. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PPA Patients | Healthy Speakers | |||
|---|---|---|---|---|
| Range | Mean (SD) | Range | Mean (SD) | |
| Age (years) | 52–84 | 66.13 (8.8) | 53–65 | 58.76 (4.1) |
| Education (years) | 2–18 | 13.40 (4.5) | 6–20 | 14.58 (4.0) |
| Patient No. | Age | Sex | Education (Years) | Hand Preference | TPO in Months | PPA Variant | BNT | BDAE—Oral Expression | BDAE—Auditory Comprehension | Speech Rate (CTP) |
|---|---|---|---|---|---|---|---|---|---|---|
| P001 | 84 | M | 16 | Right | 21 | non-fluent | - | 23 | 29.5 | 33.70 |
| P002 | 74 | M | 12 | Right | 7 | non-fluent | 4 | 20 | 23 | 27.84 |
| P008 | 65 | M | 14 | Right | 15 | non-fluent | ΝA | 19 | 24 | 25.70 |
| P010 | 74 | M | 2 | Right | 8 | non-fluent | 5 | - | - | 23.50 |
| P018 | 74 | F | 18 | Right | 16 | non-fluent | - | 23 | 30.5 | 52.40 |
| P021 | 67 | M | 18 | Right | 24 | non-fluent | 10 | 18 | 25 | 31.90 |
| P005 | 57 | M | 16 | Right | 44 | semantic | 1 | 28 | 21.5 | 68.40 |
| P006 | 76 | M | 16 | Right | 36 | semantic | 1 | 18 | 20.5 | 74.70 |
| P009 | 70 | M | 17 | Right | 36 | semantic | 0 | 26 | 23.5 | 144.70 |
| P011 | 57 | M | 14 | Right | 36 | semantic | 0 | 21 | 15 | 77.70 |
| P012 | 66 | F | 16 | Right | 36 | semantic | 1 | 23 | 24.5 | 94.70 |
| P014 | 74 | F | 17 | Ambidextrous | 24 | semantic | 1 | 23 | 26 | 148.70 |
| P007 | 67 | M | 12 | Right | 24 | logopenic | 11 | 23 | 26 | 92.10 |
| P003 | 64 | M | 6 | Right | 20 | logopenic | 0 | 22 | 22 | 53.40 |
| P004 | 76 | M | 12 | Right | 12 | logopenic | 4 | 23 | 31 | 55.71 |
| P013 | 59 | F | 16 | Right | 46 | logopenic | 6 | 21 | 28 | 87.30 |
| P016 | 54 | F | 6 | Right | 4 | logopenic | 1 | 22 | 31 | 74.70 |
| P017 | 61 | F | 16 | Right | 10 | logopenic | 2 | 23 | 31 | 53.90 |
| P020 | 66 | M | 17 | Right | ΝA | logopenic | 14 | 28 | 29 | 47.50 |
| P022 | 58 | M | 14 | Right | 18 | logopenic | 15 | 18 | 27 | 55.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Potagas, C.; Nikitopoulou, Z.; Angelopoulou, G.; Kasselimis, D.; Laskaris, N.; Kourtidou, E.; Constantinides, V.C.; Bougea, A.; Paraskevas, G.P.; Papageorgiou, G.; et al. Silent Pauses and Speech Indices as Biomarkers for Primary Progressive Aphasia. Medicina 2022, 58, 1352. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58101352
Potagas C, Nikitopoulou Z, Angelopoulou G, Kasselimis D, Laskaris N, Kourtidou E, Constantinides VC, Bougea A, Paraskevas GP, Papageorgiou G, et al. Silent Pauses and Speech Indices as Biomarkers for Primary Progressive Aphasia. Medicina. 2022; 58(10):1352. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58101352
Chicago/Turabian StylePotagas, Constantin, Zoi Nikitopoulou, Georgia Angelopoulou, Dimitrios Kasselimis, Nikolaos Laskaris, Evie Kourtidou, Vasilios C. Constantinides, Anastasia Bougea, George P. Paraskevas, Georgios Papageorgiou, and et al. 2022. "Silent Pauses and Speech Indices as Biomarkers for Primary Progressive Aphasia" Medicina 58, no. 10: 1352. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58101352