

Arthroscopic Pan-Capsular and Transverse Humeral Ligament Release with Biceps Tenodesis for Patients with Refractory Frozen Shoulder
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Enrollment
2.2. Outcome Assessment
2.3. Surgical Technique
2.4. Intra-Articular Release
2.5. THL Release
2.6. Postoperative Care
2.7. Statistical Analysis
3. Results
3.1. Cohort Demographics
3.2. Range of Motion
3.3. Functional Assessment
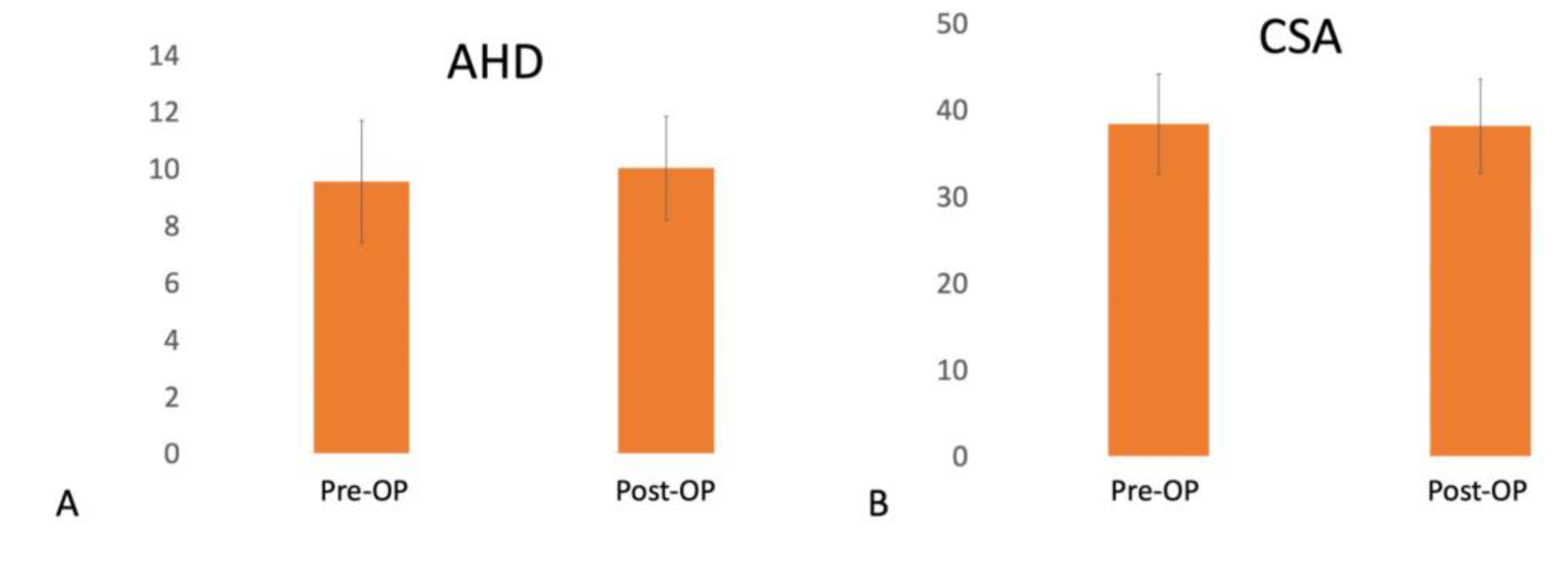
3.4. Image Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lewis, J. Frozen shoulder contracture syndrome—Aetiology, diagnosis and management. Man. Ther. 2015, 20, 2–9. [Google Scholar] [CrossRef]
- Hand, C.; Clipsham, K.; Rees, J.L.; Carr, A.J. Long-term outcome of frozen shoulder. J. Shoulder Elbow Surg. 2008, 17, 231–236. [Google Scholar] [CrossRef]
- Manske, R.C.; Prohaska, D. Diagnosis and management of adhesive capsulitis. Curr. Rev. Musculoskelet. Med. 2008, 1, 180–189. [Google Scholar] [CrossRef] [Green Version]
- Russell, S.; Jariwala, A.; Conlon, R.; Selfe, J.; Richards, J.; Walton, M. A blinded, randomized, controlled trial assessing conservative management strategies for frozen shoulder. J. Shoulder Elbow Surg. 2014, 23, 500–507. [Google Scholar] [CrossRef] [Green Version]
- Prestgaard, T.; Wormgoor, M.E.; Haugen, S.; Harstad, H.; Mowinckel, P.; Brox, J.I. Ultrasound-guided intra-articular and rotator interval corticosteroid injections in adhesive capsulitis of the shoulder: A double-blind, sham-controlled randomized study. Pain 2015, 156, 1683–1691. [Google Scholar] [CrossRef]
- Yoon, S.H.; Lee, H.Y.; Lee, H.J.; Kwack, K.S. Optimal dose of intra-articular corticosteroids for adhesive capsulitis: A randomized, triple-blind, placebo-controlled trial. Am. J. Sports Med. 2013, 41, 1133–1139. [Google Scholar] [CrossRef]
- Smith, C.D.; Hamer, P.; Bunker, T.D. Arthroscopic capsular release for idiopathic frozen shoulder with intra-articular injection and a controlled manipulation. Ann. R. Coll. Surg. Engl. 2014, 96, 55–60. [Google Scholar] [CrossRef]
- Le, H.V.; Lee, S.J.; Nazarian, A.; Rodriguez, E.K. Adhesive capsulitis of the shoulder: Review of pathophysiology and current clinical treatments. Shoulder Elbow 2017, 9, 75–84. [Google Scholar] [CrossRef] [Green Version]
- Gallacher, S.; Beazley, J.C.; Evans, J.; Anaspure, R.; Silver, D.; Redfern, A.; Thomas, W.; Kitson, J.; Smith, C. A randomized controlled trial of arthroscopic capsular release versus hydrodilatation in the treatment of primary frozen shoulder. J. Shoulder Elbow Surg. 2018, 27, 1401–1406. [Google Scholar] [CrossRef]
- Le Lievre, H.M.; Murrell, G.A. Long-term outcomes after arthroscopic capsular release for idiopathic adhesive capsulitis. J. Bone Joint Surg. Am. 2012, 94, 1208–1216. [Google Scholar] [CrossRef]
- Ogilvie-Harris, D.J.; Biggs, D.J.; Fitsialos, D.P.; MacKay, M. The resistant frozen shoulder. Manipulation versus arthroscopic release. Clin. Orthop. Relat. Res. 1995, 319, 238–248. [Google Scholar]
- Chen, J.; Chen, S.; Li, Y.; Hua, Y.; Li, H. Is the extended release of the inferior glenohumeral ligament necessary for frozen shoulder? Arthroscopy 2010, 26, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, Y.; Ando, A.; Kanazawa, K.; Koide, M.; Sekiguchi, T.; Hamada, J.; Itoi, E. Arthroscopic Coracohumeral Ligament Release for Patients with Frozen Shoulder. Arthrosc. Tech. 2018, 7, e1–e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanders, B.; Lavery, K.P.; Pennington, S.; Warner, J.J. Clinical success of biceps tenodesis with and without release of the transverse humeral ligament. J. Shoulder Elbow Surg. 2012, 21, 66–71. [Google Scholar] [CrossRef]
- Ozaki, J.; Nakagawa, Y.; Sakurai, G.; Tamai, S. Recalcitrant chronic adhesive capsulitis of the shoulder. Role of contracture of the coracohumeral ligament and rotator interval in pathogenesis and treatment. J. Bone Joint Surg. Am. 1989, 71, 1511–1515. [Google Scholar] [CrossRef] [PubMed]
- Alpantaki, K.; McLaughlin, D.; Karagogeos, D.; Hadjipavlou, A.; Kontakis, G. Sympathetic and sensory neural elements in the tendon of the long head of the biceps. J. Bone Joint Surg. Am. 2005, 87, 1580–1583. [Google Scholar] [CrossRef]
- Snow, B.J.; Narvy, S.J.; Omid, R.; Atkinson, R.D.; Vangsness, C.T., Jr. Anatomy and histology of the transverse humeral ligament. Orthopedics 2013, 36, e1295–e1298. [Google Scholar] [CrossRef] [Green Version]
- Boonstra, A.M.; Preuper, H.R.S.; Balk, G.A.; Stewart, R.E. Cut-off points for mild, moderate, and severe pain on the visual analogue scale for pain in patients with chronic musculoskeletal pain. Pain 2014, 155, 2545–2550. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, M.R. Arthroscopic treatment of refractory adhesive capsulitis of the shoulder. Rev. Col. Bras. Cir. 2014, 41, 30–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, J.H.; Kim, S.H.; Shin, S.H.; Chung, S.W.; Kim, J.Y.; Kim, S.H.; Kim, S.J. Outcome of rotator cuff repair in large-to-massive tear with pseudoparalysis: A comparative study with propensity score matching. Am. J. Sports Med. 2011, 39, 1413–1420. [Google Scholar] [CrossRef]
- American Institute of Ultrasound in Medicine. Official Statement: Training Guidelines for the Performance of Musculoskeletal Ultrasound Examinations. Available online: http://www.aium.org/officialStatements/61 (accessed on 11 February 2014).
- Rutten, M.J.; Maresch, B.J.; Jager, G.J.; Blickman, J.G.; van Holsbeeck, M.T. Ultrasound of the rotator cuff with MRI and anatomic correlation. Eur. J. Radiol. 2007, 62, 427–436. [Google Scholar] [CrossRef]
- Wakefield, R.J.; Balint, P.V.; Szkudlarek, M.; Filippucci, E.; Backhaus, M.; D’Agostino, M.-A.; Sanchez, E.N.; Iagnocco, A.; Schmidt, W.A.; Bruyn, G.A. Musculoskeletal ultrasound including definitions for ultrasonographic pathology. J. Rheumatol. 2005, 32, 2485–2487. [Google Scholar]
- Chen, H.-S.; Lin, S.-H.; Hsu, Y.-H.; Chen, S.-C.; Kang, J.-H. A comparison of physical examinations with musculoskeletal ultrasound in the diagnosis of biceps long head tendinitis. Ultrasound Med. Biol. 2011, 37, 1392–1398. [Google Scholar] [CrossRef]
- Constant, C.R.; Murley, A.H. A clinical method of functional assessment of the shoulder. Clin. Orthop. Relat. Res. 1987, 214, 160–164. [Google Scholar] [CrossRef]
- Gerber, C.; Fuchs, B.; Hodler, J. The results of repair of massive tears of the rotator cuff. J. Bone Joint Surg. Am. 2000, 82, 505–515. [Google Scholar] [CrossRef]
- Moor, B.; Bouaicha, S.; Rothenfluh, D.; Sukthankar, A.; Gerber, C. Is there an association between the individual anatomy of the scapula and the development of rotator cuff tears or osteoarthritis of the glenohumeral joint? A radiological study of the critical shoulder angle. Bone Jt. J. 2013, 95, 935–941. [Google Scholar] [CrossRef]
- Park, J.S.; Kim, S.H.; Jung, H.J.; Lee, Y.H.; Oh, J.H. A Prospective Randomized Study Comparing the Interference Screw and Suture Anchor Techniques for Biceps Tenodesis. Am. J. Sports Med. 2017, 45, 440–448. [Google Scholar] [CrossRef]
- Teefey, S.A.; Hasan, S.A.; Middleton, W.D.; Patel, M.; Wright, R.W.; Yamaguchi, K. Ultrasonography of the rotator cuff. A comparison of ultrasonographic and arthroscopic findings in one hundred consecutive cases. J. Bone Joint Surg. Am. 2000, 82, 498–504. [Google Scholar] [CrossRef]
- Chen, S.K.; Lin, S.Y.; Liao, J.S. [An orthopaedic study of frozen shoulder]. Gaoxiong Yi Xue Ke Xue Za Zhi 1988, 4, 1–9. [Google Scholar]
- Jacobs, L.G.; Smith, M.G.; Khan, S.A.; Smith, K.; Joshi, M. Manipulation or intra-articular steroids in the management of adhesive capsulitis of the shoulder? A prospective randomized trial. J. Shoulder Elbow Surg. 2009, 18, 348–353. [Google Scholar] [CrossRef]
- Yoo, J.C.; Kim, J.H.; Ahn, J.H.; Lee, S.H. Arthroscopic perspective of the axillary nerve in relation to the glenoid and arm position: A cadaveric study. Arthroscopy 2007, 23, 1271–1277. [Google Scholar] [CrossRef]
- Jerosch, J. 360 degrees arthroscopic capsular release in patients with adhesive capsulitis of the glenohumeral joint—Indication, surgical technique, results. Knee Surg. Sports Traumatol. Arthrosc. 2001, 9, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Cuff, D.J.; Pupello, D.R. Comparison of hemiarthroplasty and reverse shoulder arthroplasty for the treatment of proximal humeral fractures in elderly patients. JBJS 2013, 95, 2050–2055. [Google Scholar] [CrossRef]
- Griggs, S.M.; Ahn, A.; Green, A. Idiopathic adhesive capsulitis. A prospective functional outcome study of nonoperative treatment. J. Bone Joint Surg. Am. 2000, 82, 1398–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaffer, B.; Tibone, J.E.; Kerlan, R.K. Frozen shoulder. A long-term follow-up. J. Bone Joint Surg. Am. 1992, 74, 738–746. [Google Scholar] [CrossRef]
- Taylor, S.A.; Ramkumar, P.N.; Fabricant, P.D.; Dines, J.S.; Gausden, E.; White, A.; Conway, J.E.; O’Brien, S.J. The clinical impact of bicipital tunnel decompression during long head of the biceps tendon surgery: A systematic review and meta-analysis. Arthrosc. J. Arthrosc. Relat. Surg. 2016, 32, 1155–1164. [Google Scholar] [CrossRef]
- Soifer, T.B.; Levy, H.J.; Soifer, F.M.; Kleinbart, F.; Vigorita, V.; Bryk, E. Neurohistology of the subacromial space. Arthroscopy 1996, 12, 182–186. [Google Scholar] [CrossRef]
- Van Kleunen, J.P.; Tucker, S.A.; Field, L.D.; Savoie, F.H., 3rd. Return to high-level throwing after combination infraspinatus repair, SLAP repair, and release of glenohumeral internal rotation deficit. Am. J. Sports Med. 2012, 40, 2536–2541. [Google Scholar] [CrossRef]
- Ueda, Y.; Sugaya, H.; Takahashi, N.; Matsuki, K.; Kawai, N.; Tokai, M.; Onishi, K.; Hoshika, S. Rotator Cuff Lesions in Patients with Stiff Shoulders: A Prospective Analysis of 379 Shoulders. J. Bone Joint Surg. Am. 2015, 97, 1233–1237. [Google Scholar] [CrossRef] [Green Version]
- Lutton, D.M.; Gruson, K.I.; Harrison, A.K.; Gladstone, J.N.; Flatow, E.L. Where to tenodese the biceps: Proximal or distal? Clin Orthop. Relat. Res. 2011, 469, 1050–1055. [Google Scholar] [CrossRef] [Green Version]
- Rhee, P.C.; Spinner, R.J.; Bishop, A.T.; Shin, A.Y. Iatrogenic brachial plexus injuries associated with open subpectoral biceps tenodesis: A report of 4 cases. Am. J. Sports Med. 2013, 41, 2048–2053. [Google Scholar] [CrossRef] [PubMed]
- Dickens, J.F.; Kilcoyne, K.G.; Tintle, S.M.; Giuliani, J.; Schaefer, R.A.; Rue, J.P. Subpectoral biceps tenodesis: An anatomic study and evaluation of at-risk structures. Am. J. Sports Med. 2012, 40, 2337–2341. [Google Scholar] [CrossRef] [PubMed]
- Dein, E.J.; Huri, G.; Gordon, J.C.; McFarland, E.G. A humerus fracture in a baseball pitcher after biceps tenodesis. Am. J. Sports Med. 2014, 42, 877–879. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, Y.; Sugaya, H.; Takahashi, N.; Kawai, N.; Ando, A.; Hamada, J.; Itoi, E. Effects of intra-articular steroid injection before pan-capsular release in patients with refractory frozen shoulder. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 1536–1541. [Google Scholar] [CrossRef] [PubMed]
- D'Orsi, G.M.; Via, A.G.; Frizziero, A.; Oliva, F. Treatment of adhesive capsulitis: A review. Muscles Ligaments Tendons J. 2012, 2, 70–78. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. of Patients | 35 |
|---|---|
| Age, y | 53.1 ± 9 |
| Sex, male: female, n | 19:16 |
| Dominant hand, right: left | 30:5 |
| Surgical side, right: left | 15:20 |
| Duration of pain, month | 9.9 ± 2.3 |
| Number of previous injections | 5.2 ± 2.1 |
| Mean follow-up, month | 24 ± 1.5 |
| Underlined disease (%) | |
| Diabetes mellitus | 5 (14.3) |
| Cancer | 2 (5.7) |
| Thyroid dysfunction | 0 |
| Previous trauma | 4 (11.4) |
| Intra-operative finding other than frozen shoulder (%) | |
| PASTA lesion | 8 (22.9) |
| Biceps pulley tear | 2 (5.7) |
| SLAP tear | 1 (2.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, C.-H.; Sheu, H.; Chen, P.; Berco, D.; Chan, Y.-S.; Chen, A.C.-Y. Arthroscopic Pan-Capsular and Transverse Humeral Ligament Release with Biceps Tenodesis for Patients with Refractory Frozen Shoulder. Medicina 2022, 58, 1712. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58121712
Chiu C-H, Sheu H, Chen P, Berco D, Chan Y-S, Chen AC-Y. Arthroscopic Pan-Capsular and Transverse Humeral Ligament Release with Biceps Tenodesis for Patients with Refractory Frozen Shoulder. Medicina. 2022; 58(12):1712. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58121712
Chicago/Turabian StyleChiu, Chih-Hao, Huan Sheu, Poyu Chen, Dan Berco, Yi-Sheng Chan, and Alvin Chao-Yu Chen. 2022. "Arthroscopic Pan-Capsular and Transverse Humeral Ligament Release with Biceps Tenodesis for Patients with Refractory Frozen Shoulder" Medicina 58, no. 12: 1712. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58121712