


Exploring the Potential Use of Wearable Devices as a Prognostic Tool among Patients in Hospice Care
 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Recruitment
2.3. Wrist Actigraphy
2.4. Data Collection and Acquisition
2.5. Clinical Information
2.6. Data Analysis
3. Results
3.1. Demographics of Study Population
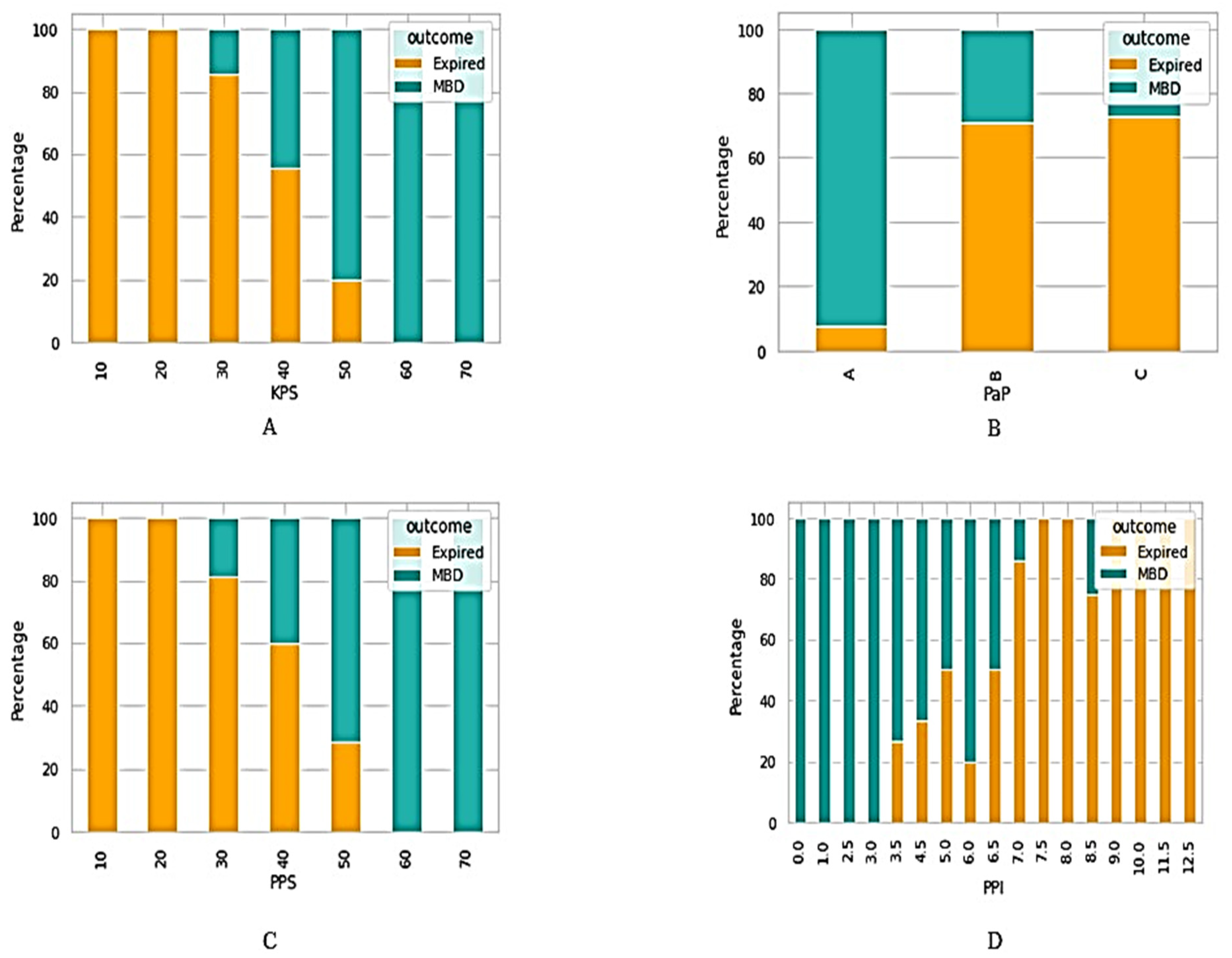
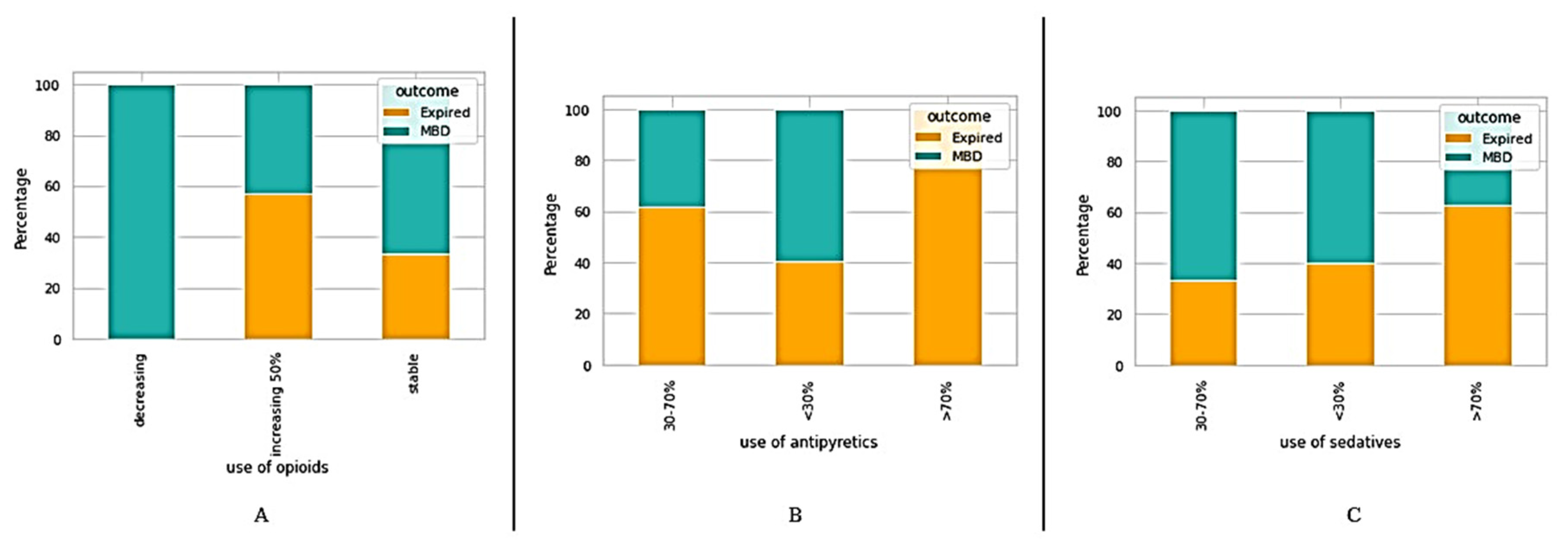
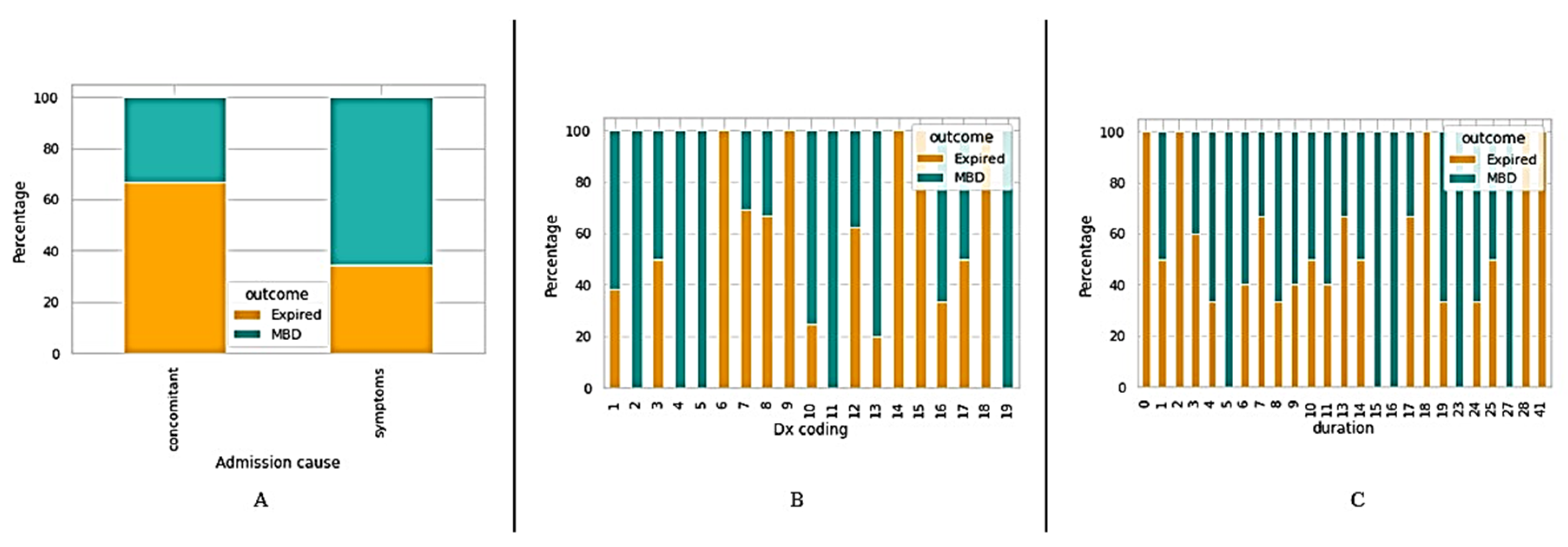
3.2. Description of Clinical Data
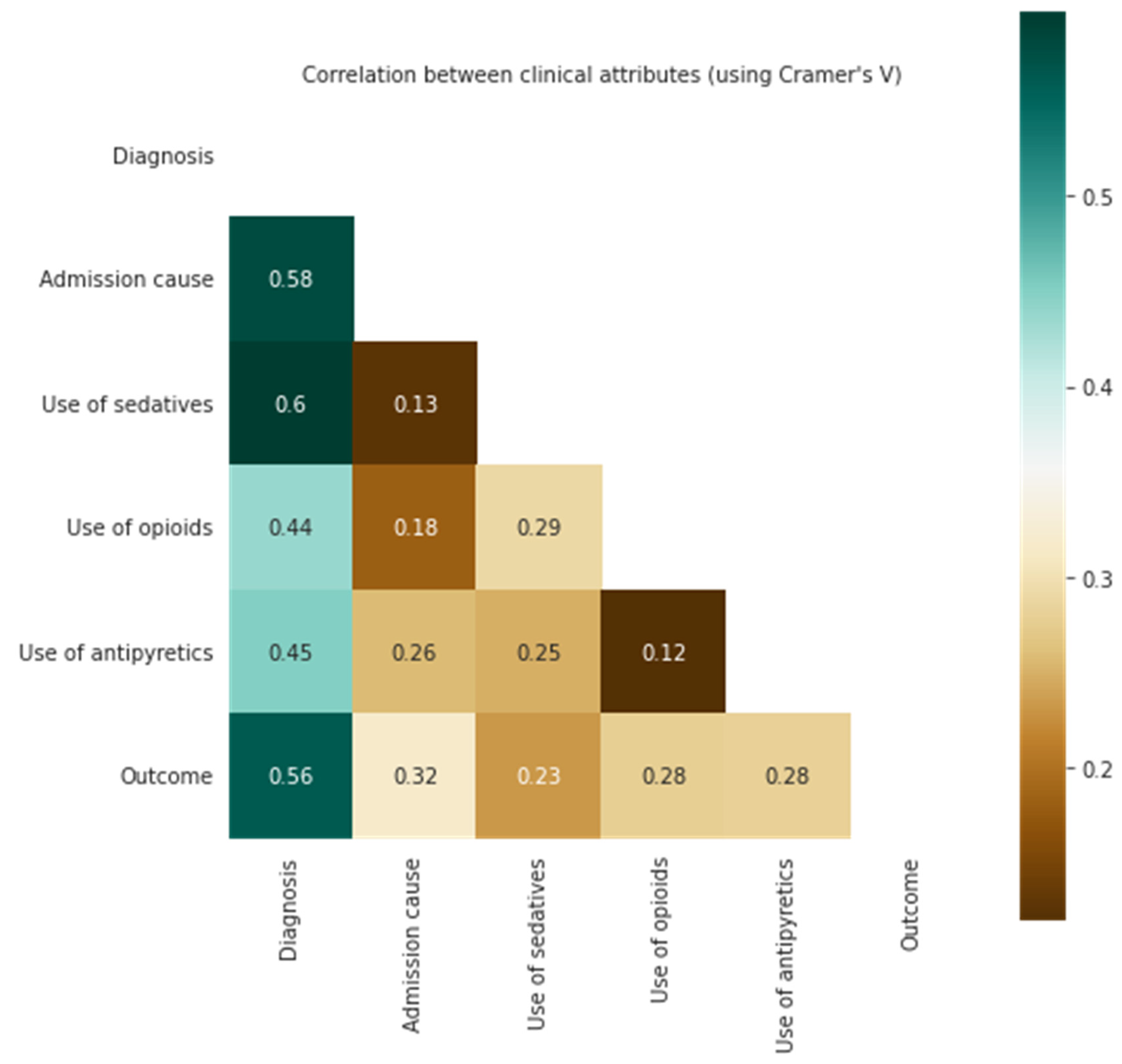
3.3. Correlation of Clinical Information with Survival Outcomes
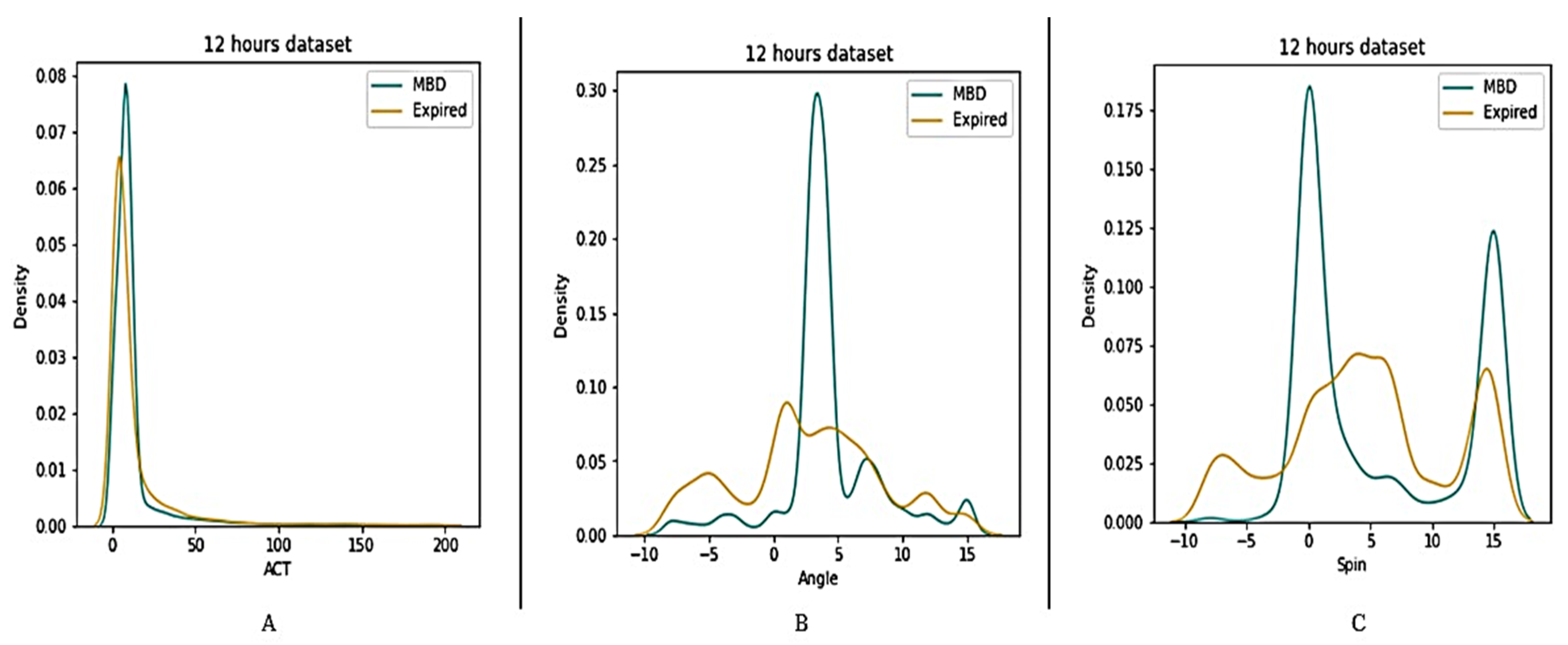
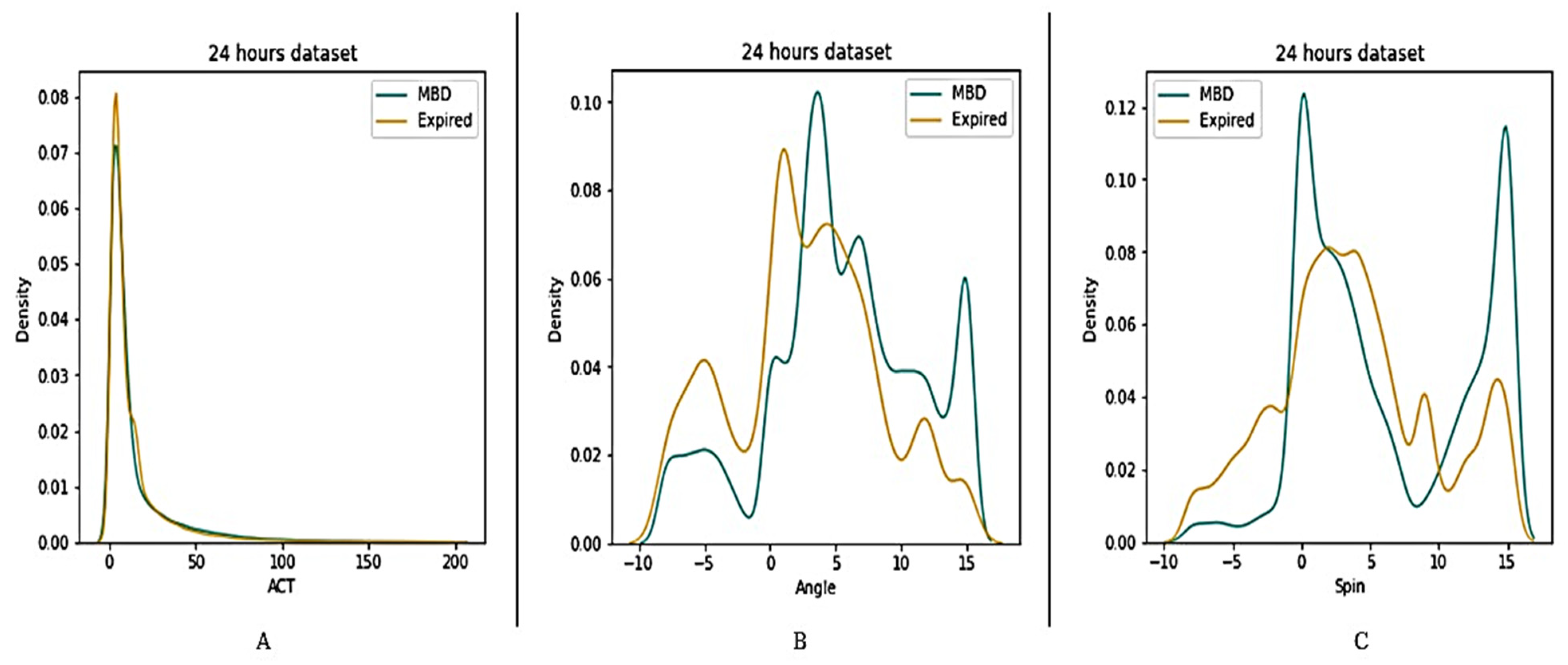
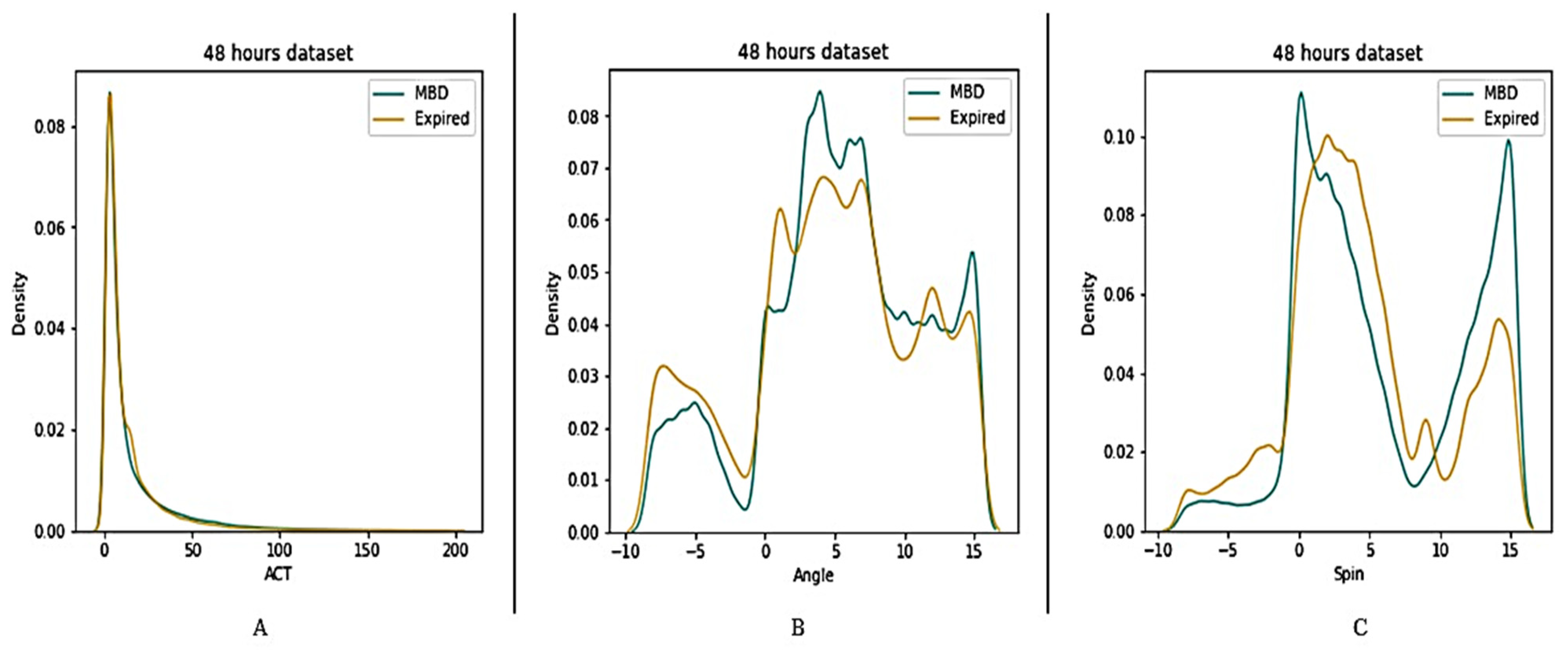
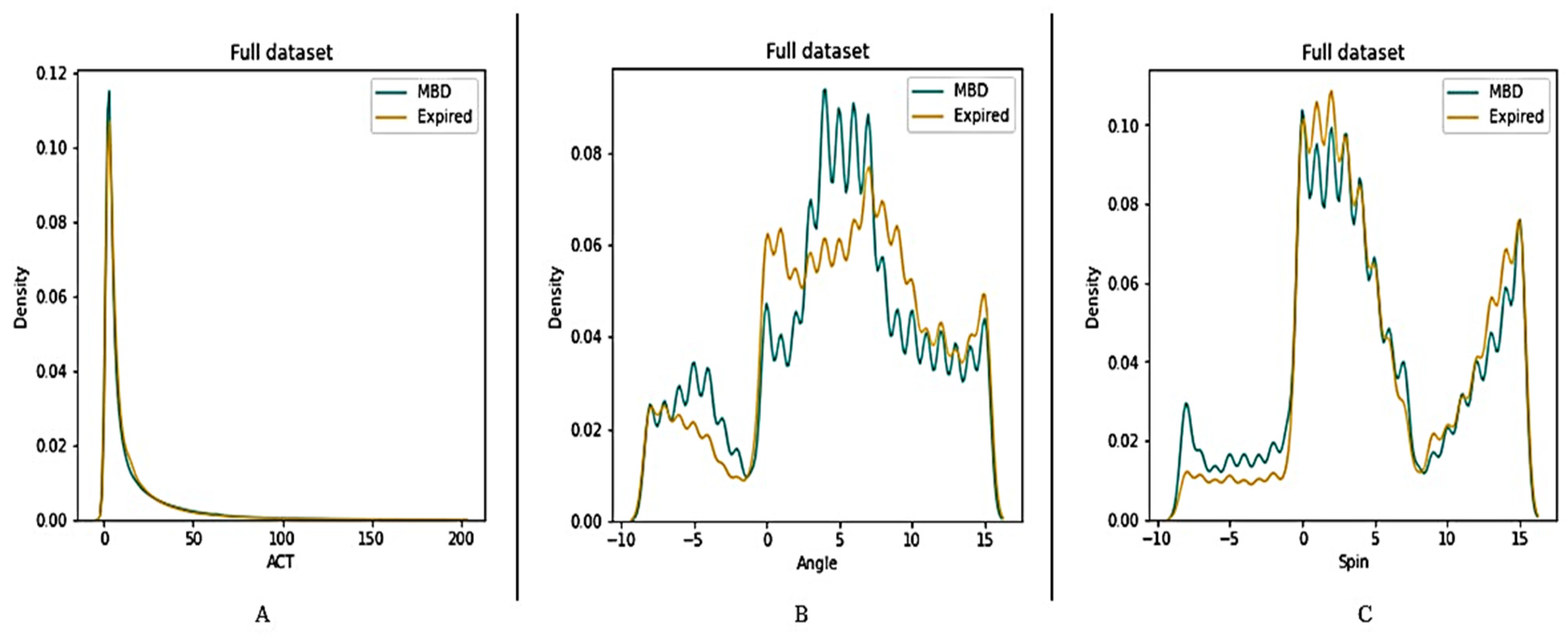
3.4. Description of Wearable Dataset
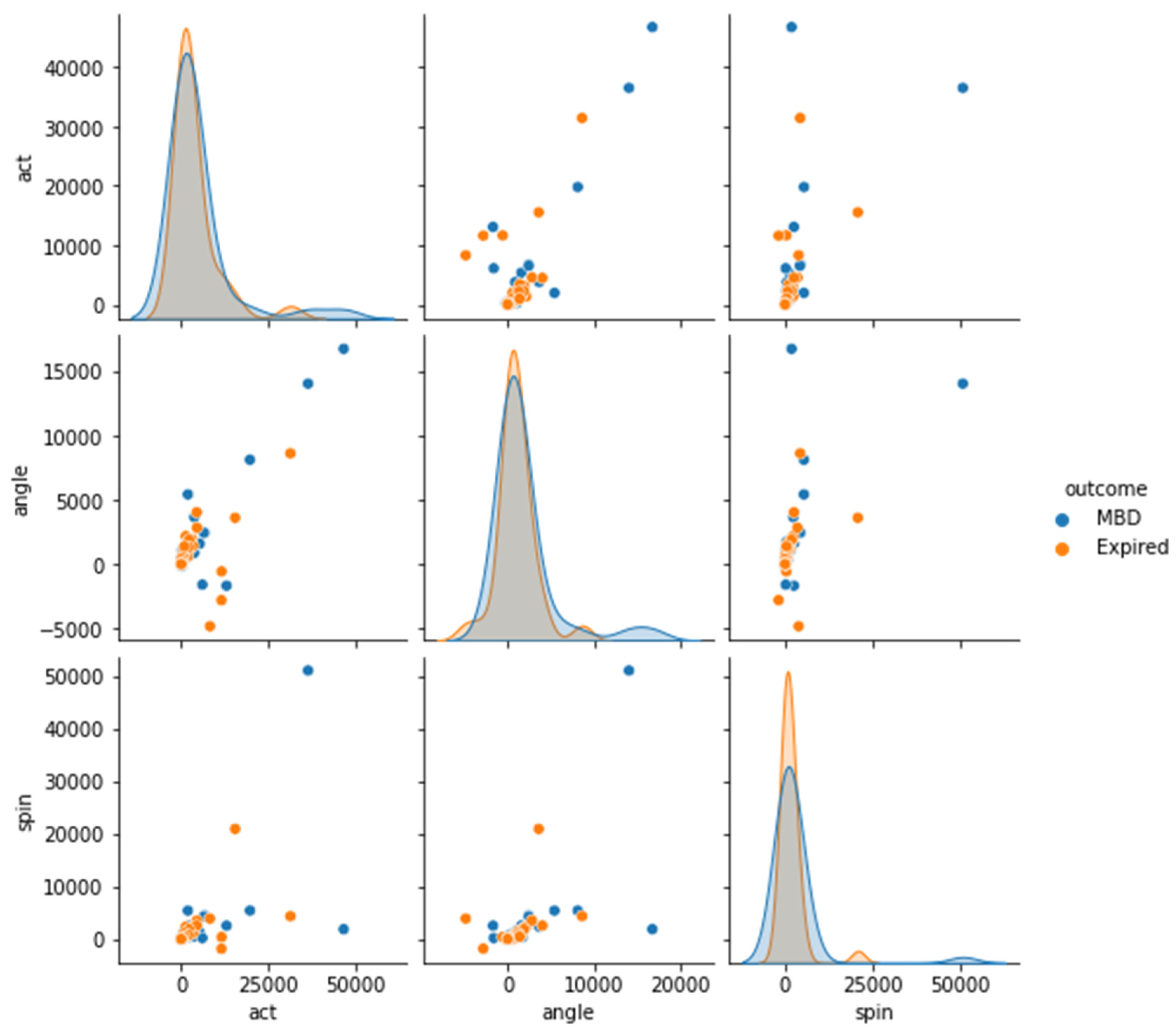
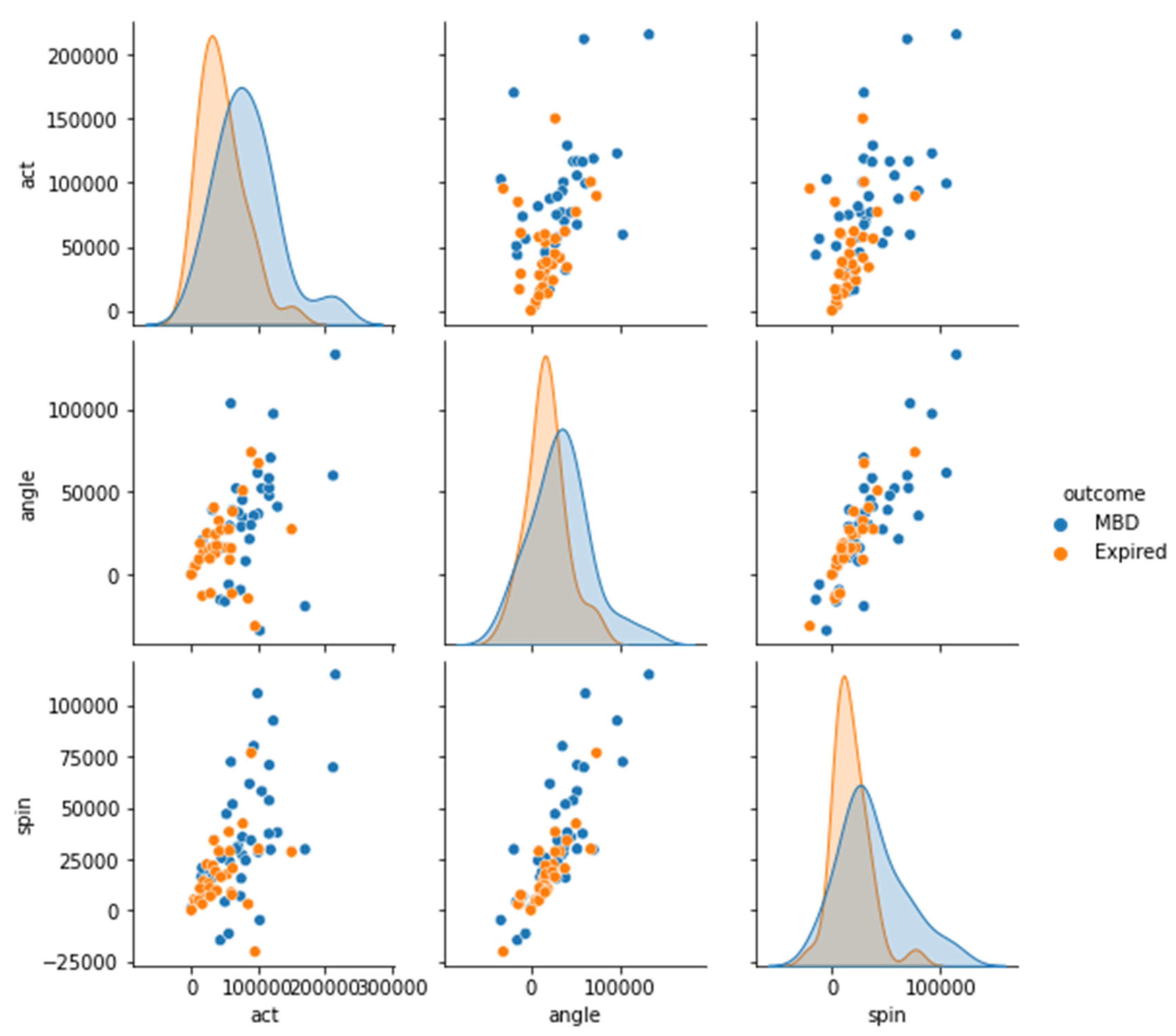
3.5. Significance of Cumulative Sensor Data to Differentiate between MBD and Expired
4. Discussion
4.1. Mobile Technology in Palliative Care
4.2. Need for Objective Prediction of Survival
4.3. WD for Short-Term Survival
4.4. Risks of using Wearable Devices in Palliative Care
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hui, D.; Bruera, E. Integrating palliative care into the trajectory of cancer care. Nat. Rev. Clin. Oncol. 2016, 13, 159–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neeman, E.; Gresham, G.; Ovasapians, N.; Hendifar, A.; Tuli, R.; Figlin, R.; Shinde, A. Comparing Physician and Nurse Eastern Cooperative Oncology Group Performance Status (ECOG-PS) Ratings as Predictors of Clinical Outcomes in Patients with Cancer. Oncologist 2019, 24, e1460–e1466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tatum, P.E.; Mills, S.S. Hospice and palliative care: An overview. Med. Clin. 2020, 104, 359–373. [Google Scholar]
- Li, S.; Zhang, Z.; Zhang, X. A qualitative study exploring nursing students’ perspectives on and attitudes towards hospice care in China. Nurse Educ. Today 2022, 119, 105384. [Google Scholar] [CrossRef] [PubMed]
- Hom, J.; Nikowitz, J.; Ottesen, R.; Niland, J.C. Facilitating clinical research through automation: Combining optical character recognition with natural language processing. Clin. Trials 2022, 19, 17407745221093621. [Google Scholar] [CrossRef] [PubMed]
- Jang, R.W.; Caraiscos, V.B.; Swami, N.; Banerjee, S.; Mak, E.; Kaya, E.; Rodin, G.; Bryson, J.; Ridley, J.Z.; Le, L.W. Simple prognostic model for patients with advanced cancer based on performance status. J. Oncol. Pract. 2014, 10, e335–e341. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-H.; Chou, W.-C.; Yang, H.-Y.; Chen, C.-C.; Chang, H.; Wang, P.-N.; Kuo, M.-C.; Kao, Y.-F.; Ho, L.-H.; Hsueh, S.-W. Utility of palliative prognostic index in predicting survival outcomes in patients with hematological malignancies in the acute ward setting. Am. J. Hosp. Palliat. Med. 2022, 39, 548–554. [Google Scholar] [CrossRef]
- Baba, M.; Maeda, I.; Morita, T.; Inoue, S.; Ikenaga, M.; Matsumoto, Y.; Sekine, R.; Yamaguchi, T.; Hirohashi, T.; Tajima, T. Survival prediction for advanced cancer patients in the real world: A comparison of the Palliative Prognostic Score, Delirium-Palliative Prognostic Score, Palliative Prognostic Index and modified Prognosis in Palliative Care Study predictor model. Eur. J. Cancer 2015, 51, 1618–1629. [Google Scholar] [CrossRef]
- Hui, D.; Ross, J.; Park, M.; Dev, R.; Vidal, M.; Liu, D.; Paiva, C.E.; Bruera, E. Predicting survival in patients with advanced cancer in the last weeks of life: How accurate are prognostic models compared to clinicians’ estimates? Palliat. Med. 2020, 34, 126–133. [Google Scholar] [CrossRef]
- Allende-Pérez, S.; Rodríguez-Mayoral, O.; Peña-Nieves, A.; Bruera, E. Performance status and survival in cancer patients undergoing palliative care: Retrospective study. BMJ Support. Palliat. Care, 2022; in press. [Google Scholar]
- Glare, P.; Virik, K.; Jones, M.; Hudson, M.; Eychmuller, S.; Simes, J.; Christakis, N. A systematic review of physicians’ survival predictions in terminally ill cancer patients. BMJ 2003, 327, 195. [Google Scholar] [CrossRef] [Green Version]
- Colloca, G. Performance status as prognostic factor in phase III trials of first-line chemotherapy of unresectable or metastatic pancreatic cancer: A trial-level meta-analysis. Asia-Pac. J. Clin. Oncol. 2022, 18, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Laranjeira, C.; Dixe, M.A.; Martinho, R.; Rijo, R.; Querido, A. Building Bridges for” Palliative Care-in-Place”: Development of a mHealth Intervention for Informal Home Care. Front. Psychol. 2022, 13, 862347. [Google Scholar] [CrossRef] [PubMed]
- Finucane, A.M.; O’Donnell, H.; Lugton, J.; Gibson-Watt, T.; Swenson, C.; Pagliari, C. Digital health interventions in palliative care: A systematic meta-review. NPJ Digit. Med. 2021, 4, 64. [Google Scholar] [CrossRef] [PubMed]
- Pavic, M.; Klaas, V.; Theile, G.; Kraft, J.; Tröster, G.; Blum, D.; Guckenberger, M. Mobile health technologies for continuous monitoring of cancer patients in palliative care aiming to predict health status deterioration: A feasibility study. J. Palliat. Med. 2020, 23, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, S.; Mahgoub, I.; Du, E.; Leavitt, M.A.; Asghar, W. Advances in healthcare wearable devices. NPJ Flex. Electron. 2021, 5, 9. [Google Scholar] [CrossRef]
- Ashur, C.; Cascino, T.; Lewis, C.; Richardson, C.; Jackson, E. Wearable technology as an intervention for patients with coronary heart disease in an exercise-based rehabilitation program: A systematic review. J. Am. Coll. Cardiol. 2019, 73, 1827. [Google Scholar] [CrossRef]
- Baig, M.M.; GholamHosseini, H.; Moqeem, A.A.; Mirza, F.; Lindén, M. A Systematic Review of Wearable Patient Monitoring Systems—Current Challenges and Opportunities for Clinical Adoption. J. Med. Syst. 2017, 41, 115. [Google Scholar] [CrossRef]
- Hawthorne, G.; Greening, N.; Esliger, D.; Briggs-Price, S.; Richardson, M.; Chaplin, E.; Clinch, L.; Steiner, M.C.; Singh, S.J.; Orme, M.W. Usability of wearable multiparameter technology to continuously monitor free-living vital signs in people living with chronic obstructive pulmonary disease: Prospective observational study. JMIR Hum. Factors 2022, 9, e30091. [Google Scholar] [CrossRef]
- Silva de Lima, A.L.; Smits, T.; Darweesh, S.K.; Valenti, G.; Milosevic, M.; Pijl, M.; Baldus, H.; de Vries, N.M.; Meinders, M.J.; Bloem, B.R. Home-based monitoring of falls using wearable sensors in Parkinson’s disease. Mov. Disord. 2020, 35, 109–115. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Upadhyay, U.; Dhar, E.; Kuo, L.-J.; Syed-Abdul, S. A Scoping Review to Assess Adherence to and Clinical Outcomes of Wearable Devices in the Cancer Population. Cancers 2022, 14, 4437. [Google Scholar] [CrossRef]
- Sano, A.; Taylor, S.; McHill, A.W.; Phillips, A.J.; Barger, L.K.; Klerman, E.; Picard, R. Identifying objective physiological markers and modifiable behaviors for self-reported stress and mental health status using wearable sensors and mobile phones: Observational study. J. Med. Internet Res. 2018, 20, e9410. [Google Scholar] [CrossRef] [PubMed]
- Phongtankuel, V.; Adelman, R.D.; Reid, M. Mobile health technology and home hospice care: Promise and pitfalls. Prog. Palliat. Care 2018, 26, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.; Schuchert, A.; Krieg, T.; Oeff, M. Home telemonitoring in patients with chronic heart failure: A chance to improve patient care? Dtsch. Arztebl. Int. 2010, 107, 131. [Google Scholar] [PubMed]
- Gensini, G.F.; Alderighi, C.; Rasoini, R.; Mazzanti, M.; Casolo, G. Value of telemonitoring and telemedicine in heart failure management. Card. Fail. Rev. 2017, 3, 116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Payne, C.; Kondylakis, H.; Koumakis, L. Digital Health for Palliative Care. Front. Digit. Health 2022, 57, 888419. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, D.; Jacobs, J.; Eusebio, J.; Traeger, L.; El-Jawahri, A.; Greer, J.; Temel, J. Actigraphy as an objective measure of performance status in patients with advanced cancer. J. Clin. Oncol. 2015, 33, 62. [Google Scholar] [CrossRef]
- Yang, T.Y.; Kuo, P.Y.; Huang, Y.; Lin, H.W.; Malwade, S.; Lu, L.S.; Tsai, L.W.; Syed-Abdul, S.; Sun, C.W.; Chiou, J.F. Deep-Learning Approach to Predict Survival Outcomes Using Wearable Actigraphy Device Among End-Stage Cancer Patients. Front. Public Health 2021, 9, 730150. [Google Scholar] [CrossRef]
- Kuo, T.B.J.; Li, J.-Y.; Chen, C.-Y.; Lin, Y.-C.; Tsai, M.-W.; Lin, S.-P.; Yang, C.C.H. Influence of Accelerometer Placement and/or Heart Rate on Energy Expenditure Prediction during Uphill Exercise. J. Mot. Behav. 2018, 50, 127–133. [Google Scholar] [CrossRef]
- Kelly, C.M.; Shahrokni, A. Moving beyond Karnofsky and ECOG performance status assessments with new technologies. J. Oncol. 2016, 2016, 6186543. [Google Scholar] [CrossRef] [Green Version]
- Kos, M.; Pijnappel, E.N.; Buffart, L.M.; Balvers, B.R.; Kampshoff, C.S.; Wilmink, J.W.; van Laarhoven, H.W.; van Oijen, M.G. The association between wearable activity monitor metrics and performance status in oncology: A systematic review. Support. Care Cancer 2021, 29, 7085–7099. [Google Scholar] [CrossRef]
- To, T.H.; Currow, D.C.; Swetenham, K.; Morgan, D.D.; Tieman, J. How Can Activity Monitors Be Used in Palliative Care Patients? J. Palliat. Med. 2019, 22, 830–832. [Google Scholar] [CrossRef] [PubMed]
- Pavic, M.; Klaas, V.; Theile, G.; Kraft, J.; Tröster, G.; Guckenberger, M. Feasibility and usability aspects of continuous remote monitoring of health status in palliative cancer patients using wearables. Oncology 2020, 98, 386–395. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.; Anderson, R.; White, N.; Stone, P. Prognosticating for adult patients with advanced incurable cancer: A needed oncologist skill. Curr. Treat. Options Oncol. 2020, 21, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, P.; Vickerstaff, V.; Kalpakidou, A.; Todd, C.; Griffiths, J.; Keeley, V.; Spencer, K.; Buckle, P.; Finlay, D.; Omar, R. Prognostic tools or clinical predictions: Which are better in palliative care? PLoS ONE 2021, 16, e0249763. [Google Scholar] [CrossRef]
- Stone, P.C.; Chu, C.; Todd, C.; Griffiths, J.; Kalpakidou, A.; Keeley, V.; Omar, R.Z.; Vickerstaff, V. The accuracy of clinician predictions of survival in the Prognosis in Palliative care Study II (PiPS2): A prospective observational study. PLoS ONE 2022, 17, e0267050. [Google Scholar] [CrossRef]
- Tedesco, S.; Andrulli, M.; Larsson, M.Å.; Kelly, D.; Timmons, S.; Alamäki, A.; Barton, J.; Condell, J.; O’Flynn, B.; Nordström, A. Investigation of the analysis of wearable data for cancer-specific mortality prediction in older adults. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, 1–5 November 2021; pp. 1848–1851. [Google Scholar]
- Ghiasi, S.; Zhu, T.; Lu, P.; Hagenah, J.; Khanh, P.N.Q.; Hao, N.V.; Thwaites, L.; Clifton, D.A.; Consortium, V. Sepsis Mortality Prediction Using Wearable Monitoring in Low–Middle Income Countries. Sensors 2022, 22, 3866. [Google Scholar] [CrossRef]
- Gresham, G.; Hendifar, A.E.; Spiegel, B.; Neeman, E.; Tuli, R.; Rimel, B.; Figlin, R.A.; Meinert, C.L.; Piantadosi, S.; Shinde, A.M. Wearable activity monitors to assess performance status and predict clinical outcomes in advanced cancer patients. NPJ Digit. Med. 2018, 1, 27. [Google Scholar] [CrossRef] [Green Version]
- Low, C.A. Harnessing consumer smartphone and wearable sensors for clinical cancer research. Npj Digit. Med. 2020, 3, 140. [Google Scholar] [CrossRef]
- Amin, T.; Mobbs, R.J.; Mostafa, N.; Sy, L.W.; Choy, W.J. Wearable devices for patient monitoring in the early postoperative period: A literature review. Mhealth 2021, 7, 50. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients; n = | 78 |
| Age (years); mean (range) | 72.1 (39–92) |
| Gender; n = (%) | |
| Male | 46 (58.97%) |
| Female | 32 (41.03%) |
| Primary Site of Cancer; n = | |
| Bladder cancer | 1 |
| Brain cancer | 2 |
| Breast cancer | 4 * |
| Cervical cancer | 2 |
| Cholangiocarcinoma | 1 |
| Colorectal cancer | 19 * |
| Duodenal cancer | 1 |
| Endometrial cancer | 1 |
| Esophageal cancer | 4 |
| Gastric cancer | 8 |
| Hepatocellular carcinoma | 3 |
| Head and neck cancer | 3 |
| Lung cancer (non-small cell) | 14 |
| Small cell lung cancer | 2 |
| Ovarian cancer | 2 |
| Pancreatic cancer | 2 |
| Prostate cancer | 9 |
| Vaginal cancer | 1 |
| Admission Cause; n = (%) | |
| Concomitant diseases | 34 (45.59%) |
| Cancer-related symptoms | 44 (56.41%) |
| Duration (days); median (range) | 10 (0–41) |
| Outcome; n = (%) | |
| Discharge | 40 (51.28%) |
| Death | 38 (48.72%) |
| KPS score; n = | |
| 10 | 6 |
| 20 | 5 |
| 30 | 15 |
| 40 | 15 |
| 50 | 27 |
| 60 | 9 |
| 70 | 1 |
| PaP score group; n = | |
| A | 26 |
| B | 37 |
| C | 15 |
| PPS score; n = | |
| 10 | 1 |
| 20 | 7 |
| 30 | 17 |
| 40 | 16 |
| 50 | 23 |
| 60 | 11 |
| 70 | 3 |
| PPI score; n = | |
| A | 27 |
| B | 21 |
| C | 30 |
| Use of sedatives (time of study days); n = | |
| <30% | 39 |
| 30–70% | 11 |
| >70% | 28 |
| Status of using opioids; n = | |
| decreasing use | 2 |
| stable | 29 |
| increasing use | 47 |
| Use of antipyretics (time of study days); n = | |
| <30% | 60 |
| 30–70% | 14 |
| >70% | 4 |
| Group Statistics | Independent Sample Test | ||||||
|---|---|---|---|---|---|---|---|
| Outcome | N | Mean | Std. Deviation | Std. Error Mean | t | p | |
| ACT | MBD | 37 | 4609.9086 | 9892.71842 | 1626.35289 | 0.497 | 0.621 |
| Expired | 31 | 3578.8661 | 6493.51718 | 1166.27011 | |||
| angle | MBD | 37 | 1779.49 | 3745.058 | 615.684 | 1.171 | 0.246 |
| Expired | 31 | 885.90 | 2185.059 | 392.448 | |||
| spin | MBD | 37 | 2466.19 | 8344.602 | 1371.844 | 0.569 | 0.571 |
| Expired | 31 | 1539.81 | 3830.535 | 687.984 | |||
| Group Statistics | Independent Sample Test | ||||||
|---|---|---|---|---|---|---|---|
| Outcome | N | Mean | Std. Deviation | Std. Error Mean | t | p | |
| ACT | MBD | 37 | 27,819.4646 | 18,034.62067 | 2964.87338 | 1.024 | 0.310 |
| Expired | 31 | 22,762.5619 | 22,696.78910 | 4076.46366 | |||
| angle | MBD | 37 | 11,304.95 | 14,008.048 | 2302.909 | 2.063 | 0.043 * |
| Expired | 31 | 4921.42 | 10,943.677 | 1965.542 | |||
| spin | MBD | 37 | 12,946.70 | 14,883.926 | 2446.902 | 1.929 | 0.058 |
| Expired | 31 | 7149.94 | 8318.599 | 1494.065 | |||
| Group Statistics | Independent Sample Test | ||||||
|---|---|---|---|---|---|---|---|
| Outcome | N | Mean | Std. Deviation | Std. Error Mean | t | p | |
| ACT | MBD | 37 | 83,090.4759 | 48,290.05494 | 7938.83613 | 3.659 | <0.001 * |
| Expired | 31 | 45,445.1471 | 33,616.47689 | 6037.69748 | |||
| angle | MBD | 37 | 32,920.30 | 34,666.121 | 5699.075 | 2.197 | 0.032 * |
| Expired | 31 | 16,984.23 | 22,592.679 | 4057.765 | |||
| spin | MBD | 37 | 36,702.27 | 30,719.356 | 5050.231 | 3.197 | 0.002 * |
| Expired | 31 | 16,919.39 | 16,983.133 | 3050.261 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.; Kabir, M.A.; Upadhyay, U.; Dhar, E.; Uddin, M.; Syed-Abdul, S. Exploring the Potential Use of Wearable Devices as a Prognostic Tool among Patients in Hospice Care. Medicina 2022, 58, 1824. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58121824
Huang Y, Kabir MA, Upadhyay U, Dhar E, Uddin M, Syed-Abdul S. Exploring the Potential Use of Wearable Devices as a Prognostic Tool among Patients in Hospice Care. Medicina. 2022; 58(12):1824. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58121824
Chicago/Turabian StyleHuang, Yaoru, Muhammad Ashad Kabir, Umashankar Upadhyay, Eshita Dhar, Mohy Uddin, and Shabbir Syed-Abdul. 2022. "Exploring the Potential Use of Wearable Devices as a Prognostic Tool among Patients in Hospice Care" Medicina 58, no. 12: 1824. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58121824