RhoA, Claudin 18, and c-MET in Gastric Cancer: Clinicopathological Characteristics and Prognostic Significance in Curative Resected Patients

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Tissue Microarray Construction (TMA)
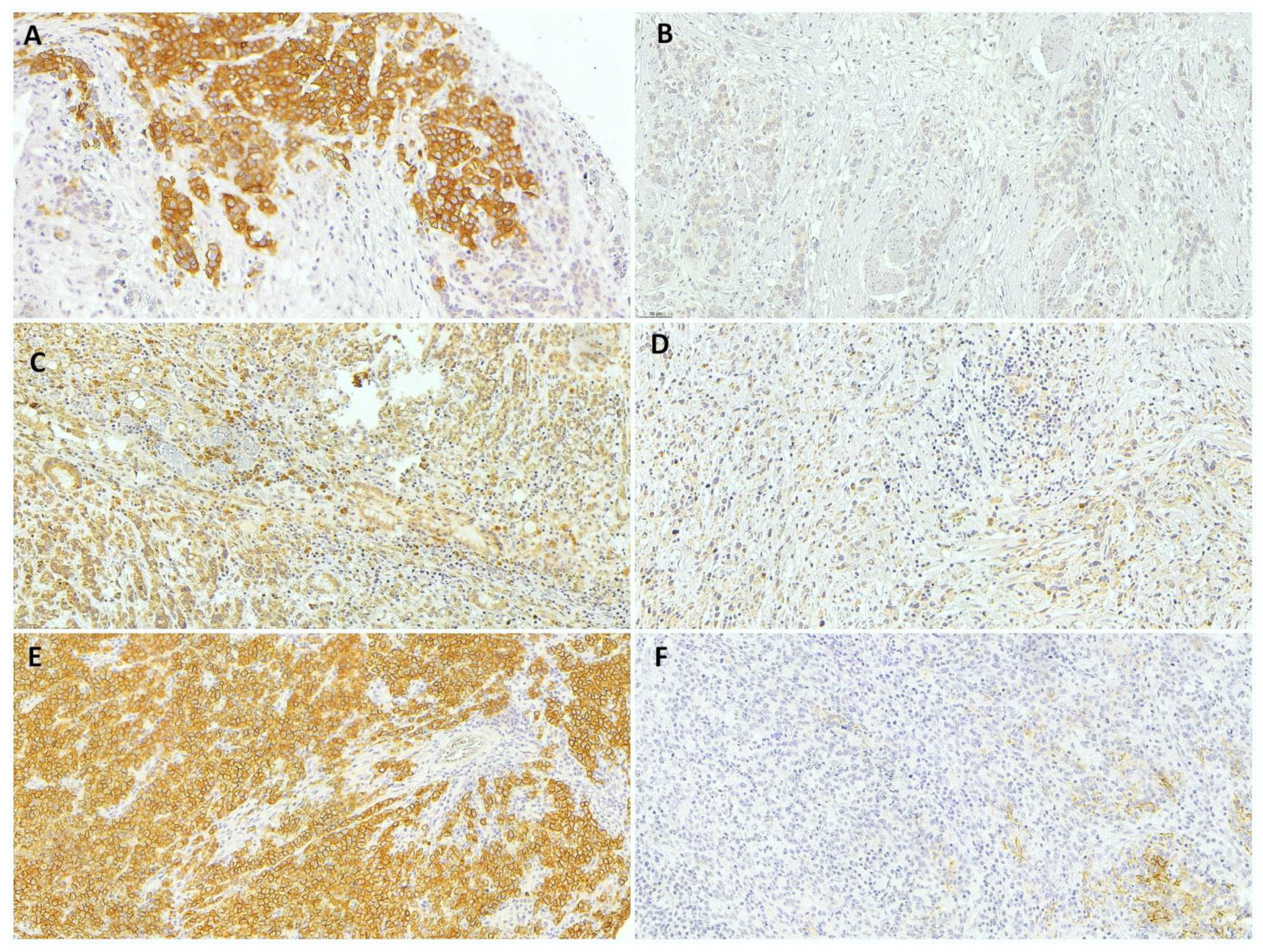
2.3. Immunohistochemistry
2.4. Statistical Analysis
3. Results
3.1. C-MET and Clinicopathological Characteristics
3.2. RhoA and Clinicopathological Characteristics
3.3. CLDN18 and Clinicopathological Characteristics
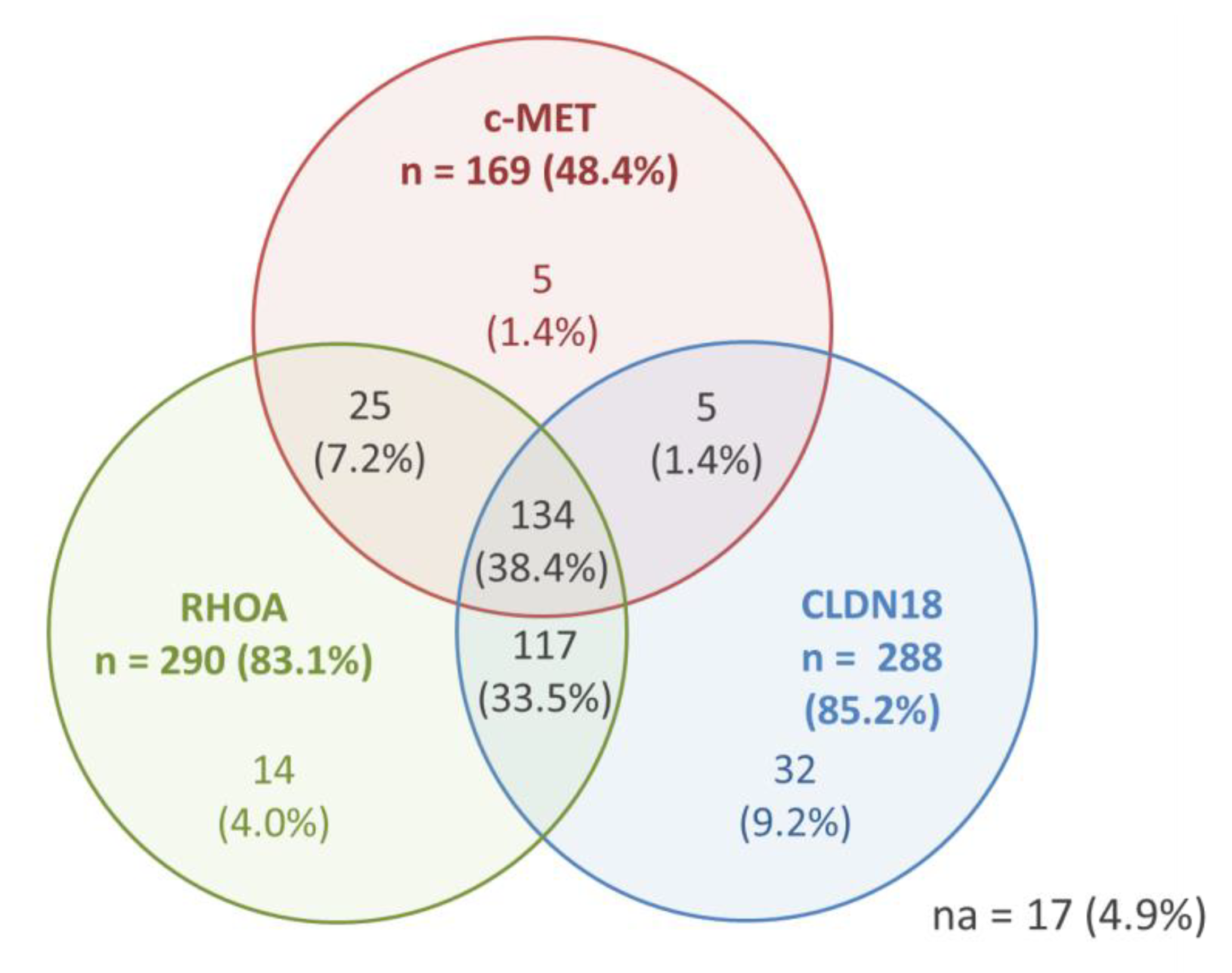
3.4. Immunohistochemical Analysis and Correlation between c-MET, RhoA, and CLDN18
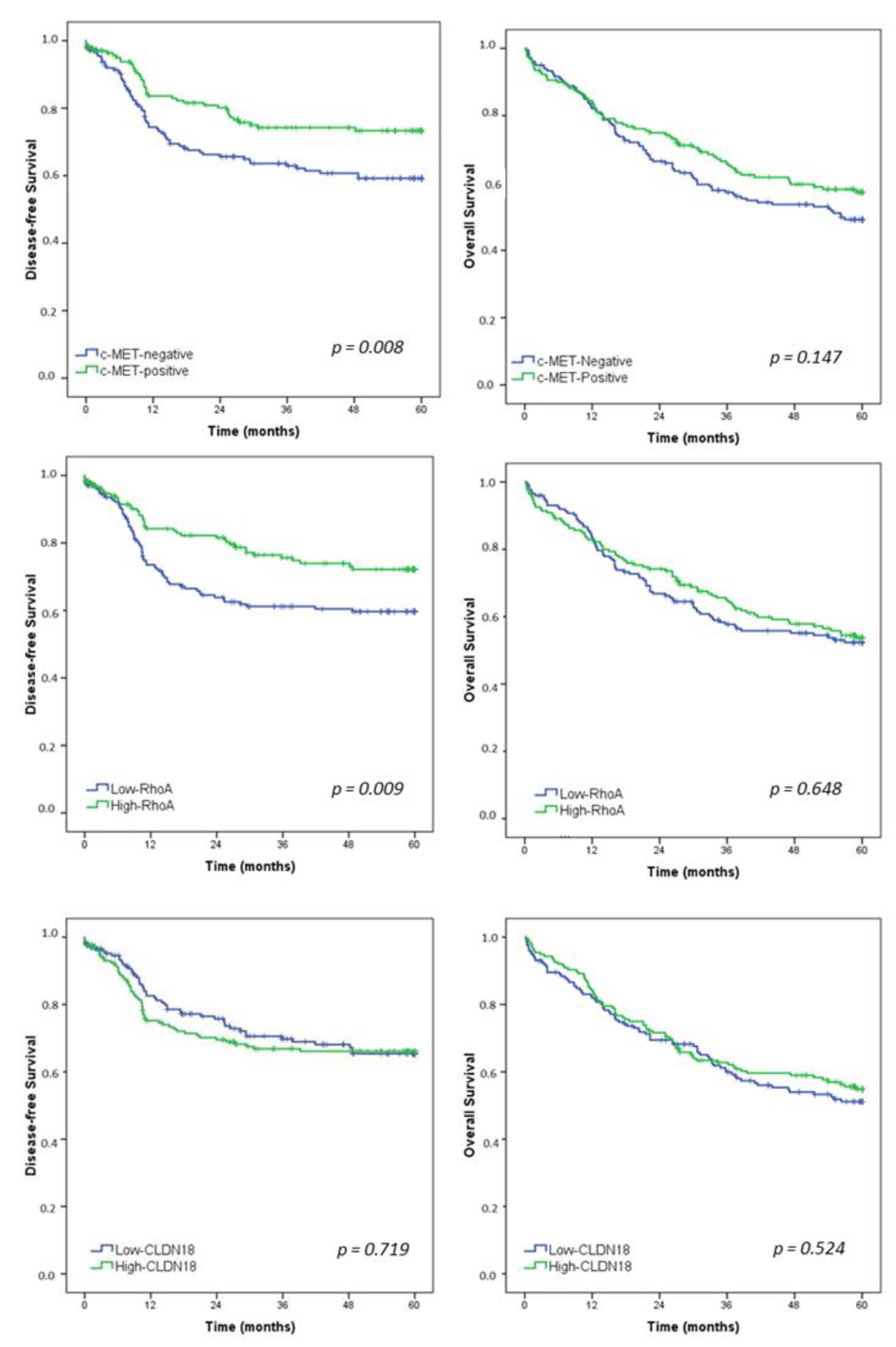
3.5. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2017, 20, 1–19. [Google Scholar] [CrossRef]
- Barchi, L.C.; Ramos, M.F.K.P.; Dias, A.R.; Andreollo, N.A.; Weston, A.C.; Lourenço, L.G.; Malheiros, C.A.; Kassab, P.; Zilberstein, B.; Ferraz, Á.A.B.; et al. II brazilian consensus on gastric cancer by the brazilian gastric cancer association. ABCD Arq. Bras. De Cir. Dig. 2020, 33, e1535. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef]
- Pereira, M.A.; Ramos, M.; Dias, A.R.; Faraj, S.F.; Ribeiro, R.R.E.; de Castria, T.B.; Zilberstein, B.; Alves, V.A.F.; Ribeiro, U.; de Mello, E.S., Jr. Expression profile of markers for targeted therapy in gastric cancer patients: HER2, microsatellite instability and PD-L1. Mol. Diagn. Ther. 2019, 23, 761–771. [Google Scholar] [CrossRef]
- Ramos, M.; Pereira, M.A.; de Mello, E.S.; Cirqueira, C.D.S.; Zilberstein, B.; Alves, V.A.F.; Ribeiro-Junior, U.; Cecconello, I. Gastric cancer molecular classification based on immunohistochemistry and in situ hybridization: Analysis in western patients after cura-tive-intent surgery. World J. Clin. Oncol. 2021, 12, 688–701. [Google Scholar] [CrossRef]
- Pereira, M.A.; Ramos, M.; Dias, A.R.; Ribeiro, R.; Cardili, L.; Zilberstein, B.; Cecconello, I.; Ribeiro, U.; de Mello, E.S., Jr.; de Castria, T.B. Scoring systems for PD-L1 expression and their prognostic impact in patients with resectable gastric cancer. Virchows Arch. Int. J. Pathol. 2021, 478, 1039–1048. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R. AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: New York, NY, USA; American Joint Commission on Cancer: Chicago, IL, USA, 2017. [Google Scholar]
- Sunakawa, Y.; Lenz, H.J. Molecular classification of gastric adenocarcinoma: Translating new insights from the cancer genome atlas research network. Curr. Treat. Options Oncol. 2015, 16, 17. [Google Scholar] [CrossRef]
- Zhang, W. TCGA divides gastric cancer into four molecular subtypes: Implications for individualized therapeutics. Chin. J. Cancer 2014, 33, 469–470. [Google Scholar] [CrossRef] [PubMed]
- Hao, T.; Jiang, J.; Wu, W.; Li, M.; Li, L.; Zhang, C.; He, Y. RhoA mutations in diffuse-type gastric cancer. Dig. Med. Res. 2020, 3, 4. [Google Scholar] [CrossRef]
- Baek, J.H.; Park, D.J.; Kim, G.Y.; Cheon, J.; Kang, B.W.; Cha, H.J.; Kim, J.G. Clinical Implications of Claudin18.2 Expression in Patients with Gastric Cancer. Anticancer. Res. 2019, 39, 6973–6979. [Google Scholar] [CrossRef]
- Kawakami, H.; Okamoto, I. MET-targeted therapy for gastric cancer: The importance of a biomarker-based strategy. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2016, 19, 687–695. [Google Scholar] [CrossRef]
- Dottermusch, M.; Krüger, S.; Behrens, H.M.; Halske, C.; Röcken, C. Expression of the potential therapeutic target claudin-18.2 is frequently decreased in gastric cancer: Results from a large caucasian cohort study. Virchows Arch. Int. J. Pathol. 2019, 475, 563–571. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.R.; Nam, S.; Lee, J.; Kim, J.H.; Jung, H.R.; Park, H.S.; Park, S.; Ahn, Y.Z.; Huh, I.; Balch, C.; et al. Systematic approach identifies RHOA as a potential biomarker therapeutic target for Asian gastric cancer. Oncotarget 2016, 7, 81435–81451. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Bosman, T.F.; Carneiro, F.; Hruban, R.H.; Theise, N.D. WHO Classification of Tumours of the Digestive System, 4th ed.; International Agency for Research on Cancer (IARC), IARC Press: Lyon, France, 2010. [Google Scholar]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Pereira, M.A.; Ramos, M.; Dias, A.R.; Faraj, S.F.; Cirqueira, C.D.S.; de Mello, E.S.; Zilberstein, B.; Alves, V.A.F.; Ribeiro, U., Jr. Immunohistochemical expression of thymidylate synthase and prognosis in gastric cancer patients submitted to fluoropyrimi-dine-based chemotherapy. Chin. J. Cancer Res. 2018, 30, 526–536. [Google Scholar] [CrossRef]
- Rohde, C.; Yamaguchi, R.; Mukhina, S.; Sahin, U.; Itoh, K.; Türeci, Ö. Comparison of Claudin 18.2 expression in primary tumors and lymph node metastases in Japanese patients with gastric adenocarcinoma. Jpn. J. Clin. Oncol. 2019, 49, 870–876. [Google Scholar] [CrossRef]
- Huang, K.H.; Lan, Y.T.; Chen, M.H.; Chao, Y.; Lo, S.S.; Li, A.F.; Wu, C.W.; Chiou, S.H.; Yang, M.H.; Shyr, Y.M.; et al. The correlation between RhoA expression and clinicopathological characteristics in gastric cancer patients after curative surgery. World J. Surg. 2015, 39, 2289–2299. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, M.; Stoss, O.; Shi, D.; Buttner, R.; van de Vijver, M.; Kim, W.; Ochiai, A.; Ruschoff, J.; Henkel, T. Assessment of a HER2 scoring system for gastric cancer: Results from a validation study. Histopathology 2008, 52, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.C.; Koh, Y.W.; Chang, H.M.; Kim, T.H.; Yook, J.H.; Kim, B.S.; Jang, S.J.; Park, Y.S. Evaluation of HER2 protein expression in gastric carcinomas: Comparative analysis of 1414 cases of whole-tissue sections and 595 cases of tissue microarrays. Ann. Surg. Oncol. 2011, 18, 2833–2840. [Google Scholar] [CrossRef]
- Carpenter, P.M.; Al-Kuran, R.A.; Theuer, C.P. Paranuclear E-Cadherin in gastric adenocarcinoma. Am. J. Clin. Pathol. 2002, 118, 887–894. [Google Scholar] [CrossRef]
- Ahn, S.; Lee, S.J.; Kim, Y.; Kim, A.; Shin, N.; Choi, K.U.; Lee, C.H.; Huh, G.Y.; Kim, K.M.; Setia, N.; et al. High-throughput protein and mRNA expression-based classification of gastric cancers can identify clinically distinct subtypes, concordant with recent molecular classifications. Am. J. Surg. Pathol. 2017, 41, 106–115. [Google Scholar] [CrossRef]
- Setia, N.; Agoston, A.T.; Han, H.S.; Mullen, J.T.; Duda, D.G.; Clark, J.W.; Deshpande, V.; Mino-Kenudson, M.; Srivastava, A.; Lennerz, J.K.; et al. A protein and mRNA expression-based classification of gastric cancer. Mod. Pathol. Off. J. United States Can. Acad. Pathol. Inc. 2016, 29, 772–784. [Google Scholar] [CrossRef] [PubMed]
- Cristescu, R.; Lee, J.; Nebozhyn, M.; Kim, K.M.; Ting, J.C.; Wong, S.S.; Liu, J.; Yue, Y.G.; Wang, J. Molecular analysis of gastric cancer identifies subtypes associated with distinct clinical outcomes. Nat. Med. 2015, 21, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, R.S.; Messing, S.; Tu, X.; McMahon, L.A.; Whitney-Miller, C.L. Immunohistochemistry as a surrogate for molecular subtyping of gastric adenocarcinoma. Hum. Pathol. 2016, 56, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Garattini, S.K.; Basile, D.; Cattaneo, M.; Fanotto, V.; Ongaro, E.; Bonotto, M.; Negri, F.V.; Berenato, R.; Ermacora, P.; Cardellino, G.G.; et al. Molecular classifications of gastric cancers: Novel insights and possible future applications. World J. Gastrointest. Oncol. 2017, 9, 194–208. [Google Scholar] [CrossRef]
- Kuboki, Y.; Yamashita, S.; Niwa, T.; Ushijima, T.; Nagatsuma, A.; Kuwata, T.; Yoshino, T.; Doi, T.; Ochiai, A.; Ohtsu, A. Comprehensive analyses using next-generation sequencing and immunohistochemistry enable precise treatment in advanced gastric cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27, 127–133. [Google Scholar] [CrossRef]
- Kim, H.S.; Shin, S.J.; Beom, S.H.; Jung, M.; Choi, Y.Y.; Son, T.; Kim, H.I.; Cheong, J.H.; Hyung, W.J.; Noh, S.H.; et al. Comprehensive expression profiles of gastric cancer molecular subtypes by immunohistochemistry: Implications for individualized therapy. Oncotarget 2016, 7, 44608–44620. [Google Scholar] [CrossRef]
- Lee, H.E.; Kim, M.A.; Lee, H.S.; Jung, E.J.; Yang, H.K.; Lee, B.L.; Bang, Y.J.; Kim, W.H. MET in gastric carcinomas: Comparison between protein expression and gene copy number and impact on clinical outcome. Br. J. Cancer 2012, 107, 325–333. [Google Scholar] [CrossRef]
- Drebber, U.; Baldus, S.E.; Nolden, B.; Grass, G.; Bollschweiler, E.; Dienes, H.P.; Hölscher, A.H.; Mönig, S.P. The overexpression of c-met as a prognostic indicator for gastric carcinoma compared to p53 and p21 nuclear accumulation. Oncol. Rep. 2008, 19, 1477–1483. [Google Scholar]
- Nakajima, M.; Sawada, H.; Yamada, Y.; Watanabe, A.; Tatsumi, M.; Yamashita, J.; Matsuda, M.; Sakaguchi, T.; Hirao, T.; Nakano, H. The prognostic significance of amplification and overexpression of c-met and c-erb B-2 in human gastric carcinomas. Cancer 1999, 85, 1894–1902. [Google Scholar] [CrossRef]
- Retterspitz, M.F.; Mönig, S.P.; Schreckenberg, S.; Schneider, P.M.; Hölscher, A.H.; Dienes, H.P.; Baldus, S.E. Expression of {be-ta}-catenin, MUC1 and c-met in diffuse-type gastric carcinomas: Correlations with tumour progression and prognosis. Anticancer. Res. 2010, 30, 4635–4641. [Google Scholar]
- Kim, Y.N.; Koo, K.H.; Sung, J.Y.; Yun, U.J.; Kim, H. Anoikis resistance: An essential prerequisite for tumor metastasis. Int. J. Cell Biol. 2012, 2012, 306879. [Google Scholar] [CrossRef] [PubMed]
- Korourian, A.; Roudi, R.; Shariftabrizi, A.; Madjd, Z. MicroRNA-31 inhibits RhoA-mediated tumor invasion and chemotherapy resistance in MKN-45 gastric adenocarcinoma cells. Exp. Biol. Med. 2017, 242, 1842–1847. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.H.; Choi, W.S.; Kim, O.; Choi, B.J.; Nam, S.W.; Lee, J.Y.; Park, W.S. Gastrokine 1 inhibits gastric cancer cell migration and invasion by downregulating RhoA expression. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2017, 20, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, Y.; Semba, S.; Ueda, J.; Fuku, T.; Hasuo, T.; Chiba, H.; Sawada, N.; Kuroda, Y.; Yokozaki, H. Gastric and intestinal claudin expression at the invasive front of gastric carcinoma. Cancer Sci. 2007, 98, 1014–1019. [Google Scholar] [CrossRef]
- Fuse, N.; Kuboki, Y.; Kuwata, T.; Nishina, T.; Kadowaki, S.; Shinozaki, E.; Machida, N.; Yuki, S.; Ooki, A.; Kajiura, S.; et al. Prognostic impact of HER2, EGFR, and c-MET status on overall survival of advanced gastric cancer patients. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2016, 19, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Ushiku, T.; Ishikawa, S.; Kakiuchi, M.; Tanaka, A.; Katoh, H.; Aburatani, H.; Lauwers, G.Y.; Fukayama, M. RHOA mutation in diffuse-type gastric cancer: A comparative clinicopathology analysis of 87 cases. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2016, 19, 403–411. [Google Scholar] [CrossRef]
- Nam, S.; Kim, J.H.; Lee, D.H. RHOA in gastric cancer: Functional roles and therapeutic potential. Front. Genet. 2019, 10, 438. [Google Scholar] [CrossRef]
- Wang, K.; Yuen, S.T.; Xu, J.; Lee, S.P.; Yan, H.H.; Shi, S.T.; Siu, H.C.; Deng, S.; Chu, K.M.; Law, S.; et al. Whole-genome sequencing and comprehensive molecular profiling identify new driver mutations in gastric cancer. Nat. Genet. 2014, 46, 573–582. [Google Scholar] [CrossRef]
- O’Hayre, M.; Inoue, A.; Kufareva, I.; Wang, Z.; Mikelis, C.M.; Drummond, R.A.; Avino, S.; Finkel, K.; Kalim, K.W.; DiPasquale, G.; et al. Inactivating mutations in GNA13 and RHOA in Burkitt’s lymphoma and diffuse large B-cell lymphoma: A tumor suppressor function for the Gα13/RhoA axis in B cells. Oncogene 2016, 35, 3771–3780. [Google Scholar] [CrossRef]
- Kalpana, G.; Figy, C.; Yeung, M.; Yeung, K.C. Reduced RhoA expression enhances breast cancer metastasis with a concomitant increase in CCR5 and CXCR4 chemokines signaling. Sci. Rep. 2019, 9, 16351. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, P.; Macaya, I.; Bazzocco, S.; Mazzolini, R.; Andretta, E.; Dopeso, H.; Mateo-Lozano, S.; Bilić, J.; Cartón-García, F.; Nieto, R.; et al. RHOA inactivation enhances Wnt signalling and promotes colorectal cancer. Nat. Commun. 2014, 5, 5458. [Google Scholar] [CrossRef]
- Sanada, Y.; Oue, N.; Mitani, Y.; Yoshida, K.; Nakayama, H.; Yasui, W. Down-regulation of the claudin-18 gene, identified through serial analysis of gene expression data analysis, in gastric cancer with an intestinal phenotype. J. Pathol. 2006, 208, 633–642. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Schuler, M.; Al-Batran, S.E.; Zvirbule, Z.; Manikhas, G.; Lordick, F.; Rusyn, A.; Vinnyk, Y.; Vynnychenko, I.; Fadeeva, N.; Nechaeva, M.; et al. Final results of the FAST study, an international, multicenter, randomized, phase II trial of epirubicin, oxaliplatin, and capecitabine (EOX) with or without the an-ti-CLDN18.2 antibody IMAB362 as first-line therapy in patients with advanced CLDN18.2+ gastric and gastroesophageal junction (GEJ) adenocarcinoma. Ann. Oncol. 2016, 27, vi208. [Google Scholar] [CrossRef]
- Al-Batran, S.-E.; Schuler, M.H.; Zvirbule, Z.; Manikhas, G.; Lordick, F.; Rusyn, A.; Vynnyk, Y.; Vynnychenko, I.; Fadeeva, N.; Nechaeva, M.; et al. FAST: An international, multicenter, randomized, phase II trial of epirubicin, oxaliplatin, and capecitabine (EOX) with or without IMAB362, a first-in-class anti-CLDN18.2 antibody, as first-line therapy in patients with advanced CLDN18.2+ gastric and gastroesophageal junction (GEJ) adenocarcinoma. J. Clin. Oncol. 2016, 34 (Suppl. 18), LBA4001. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | c-MET-Negative n = 180 (%) | c-MET-Positive n = 169 (%) | p | |
|---|---|---|---|---|
| Sex | 0.358 | |||
| Female | 68 (37.8) | 72 (42.6) | ||
| Male | 112 (62.2) | 97 (57.4) | ||
| Age (years) | 0.173 | |||
| Mean (SD) | 63.1 (11.9) | 61.4 (11.6) | ||
| ASA classification | 0.686 | |||
| I/II | 155 (86.1) | 148 (87.6) | ||
| III/IV | 25 (13.9) | 21 (12.4) | ||
| Type of resection | 0.026 | |||
| Subtotal | 83 (46.1) | 98 (58) | ||
| Total | 97 (53.9) | 71 (42) | ||
| Tumor size (cm) | 0.143 | |||
| Mean (SD) | 5.3 (3.2) | 4.8 (3.3) | ||
| Lauren type | 0.619 | |||
| Intestinal | 90 (50) | 89 (52.7) | ||
| Diffuse/mixed | 90 (50) | 80 (47.3) | ||
| Grade of histological differentiation | 0.004 | |||
| Well/moderately differentiated | 68 (37.8) | 90(53.3) | ||
| Poorly differentiated | 112 (62.2) | 79 (46.7) | ||
| Peritumoral inflammatory infiltrate | 0.001 | |||
| Absent/mild | 104 (58.4) | 128 (75.7) | ||
| Moderate/intense | 74 (41.6) | 41 (24.3) | ||
| Lymphatic invasion | 0.097 | |||
| No | 82 (45.6) | 92 (54.4) | ||
| Yes | 98 (54.4) | 77 (45.6) | ||
| Venous invasion | 0.680 | |||
| No | 122 (67.8) | 118 (69.8) | ||
| Yes | 58 (32.2) | 51 (30.2) | ||
| Perineural Invasion | 0.879 | |||
| No | 88 (48.9) | 84 (49.7) | ||
| Yes | 91 (51.1) | 85 (50.3) | ||
| pT status | 0.058 | |||
| pT1/T2 | 59 (32.8) | 72 (42.6) | ||
| pT3/T4 | 121 (67.2) | 97 (57.4) | ||
| No of lymph nodes | 0.600 | |||
| Mean (SD) | 38.6 (18.4) | 39.6 (18.6) | ||
| pN status | 0.088 | |||
| pN0 | 70 (38.9) | 81 (47.9) | ||
| pN+ | 110 (61.1) | 88 (52.1) | ||
| pTNM status | 0.164 | |||
| I/II | 91 (50.6) | 98 (58) | ||
| III/IV | 89 (49.4) | 71 (42) | ||
| RhoA | <0.001 | |||
| Low-RhoA | 116 (64.4) | 58 (34.3) | ||
| High-RhoA | 64 (35.6) | 111 (65.7) | ||
| Claudin 18 | 0.122 | |||
| Low-CLDN18 | 82 (45.6) | 91 (53.8) | ||
| High-CLDN18 | 90 (54.4) | 78 (46.2) | ||
| HER2 * | 0.014 | |||
| HER2 (0/+1) | 151 (86.8) | 119 (76.3) | ||
| HER2 (+2/+3) | 23 (13.2) | 37 (23.7) | ||
| E-cadherin * | 0.013 | |||
| Normal | 150 (86.7) | 146 (94.8) | ||
| Loss of expression | 23 (13.3) | 8 (5.2) | ||
| Variables | Low-RhoA n = 174 (%) | High-RhoA n = 169 (%) | p | |
|---|---|---|---|---|
| Sex | 0.793 | |||
| Female | 71 (40.8) | 69 (39.4) | ||
| Male | 103 (59.2) | 106 (60.6) | ||
| Age (years) | 0.260 | |||
| Mean (SD) | 61.5 (12.8) | 63.0 (10.7) | ||
| ASA classification | 0.198 | |||
| I/II | 147 (84.5) | 156 (89.1) | ||
| III/IV | 27 (15.5) | 19 (10.9) | ||
| Type of resection | 0.871 | |||
| Subtotal | 91 (52.3) | 90 (51.4) | ||
| Total | 83 (47.7) | 85 (48.6) | ||
| Tumor size (cm) | 0.170 | |||
| Mean (SD) | 5.3 (3.3) | 4.8 (3.3) | ||
| Lauren type | <0.001 | |||
| Intestinal | 72 (41.4) | 107 (61.1) | ||
| Diffuse/mixed | 102 (58.6) | 68 (38.9) | ||
| Grade of histological differentiation | ||||
| Well/moderately differentiated | 62 (35.6) | 96 (54.9) | <0.001 | |
| Poorly differentiated | 112 (64.4) | 79 (45.1) | ||
| Peritumoral inflammatory infiltrate | 0.012 | |||
| Absent/mild | 104 (60.5) | 128 (73.1) | ||
| Moderate/intense | 68 (39.5) | 47 (26.9) | ||
| Lymphatic invasion | 0.097 | |||
| No | 79 (45.4) | 95 (54.3) | ||
| Yes | 95 (54.6) | 80 (45.7) | ||
| Venous invasion | 0.191 | |||
| No | 114 (65.5) | 126 (72) | ||
| Yes | 60 (34.5) | 49 (28) | ||
| Perineural Invasion | 0.872 | |||
| No | 85 (48.9) | 87 (49.7) | ||
| Yes | 89 (51.1) | 88 (50.3) | ||
| pT status | 0.023 | |||
| pT1/T2 | 55 (31.6) | 76 (43.4) | ||
| pT3/T4 | 119 (68.4) | 99 (56.6) | ||
| No of lymph nodes | 0.269 | |||
| Mean (SD) | 40.2 (18.1) | 38.0 (18.8) | ||
| pN status | 0.355 | |||
| pN0 | 71 (40.8) | 80 (45.7) | ||
| pN+ | 103 (59.2) | 95 (54.3) | ||
| pTNM status | 0.047 | |||
| I/II | 85 (48.9) | 104 (59.4) | ||
| III/IV | 89 (51.1) | 71 (40.6) | ||
| c-MET | <0.001 | |||
| c-MET-negative | 116 (66.7) | 64 (36.6) | ||
| c-MET-positive | 58 (33.3) | 111 (63.4) | ||
| Claudin 18 | 0.422 | |||
| Low-CLDN18 | 90 (51.7) | 83 (47.4) | ||
| High-CLDN18 | 84 (48.3) | 91 (52.6) | ||
| HER2 * | 0.533 | |||
| HER2 (0/+1) | 138 (83.1) | 132 (80.5) | ||
| HER2 (+2/+3) | 28 (16.9) | 32 (19.5) | ||
| E-cadherin * | 0.040 | |||
| Normal | 143 (87.2) | 153 (93.9) | ||
| Loss of expression | 21 (12.8) | 10 (6.1) | ||
| Variables | Low-CLDN18 n = 173 (%) | High-CLDN18 n = 176 (%) | p | |
|---|---|---|---|---|
| Sex | 0.931 | |||
| Female | 69 (39.3) | 71 (40.3) | ||
| Male | 104 (60.1) | 105 (59.7) | ||
| Age (years) | 0.407 | |||
| Mean (SD) | 62.8 (12.0) | 61.7 (11.6) | ||
| ASA classification | 0.705 | |||
| I/II | 149 (86.1) | 154 (87.5) | ||
| III/IV | 24 (13.9) | 22 (12.5) | ||
| Type of resection | 0.258 | |||
| Subtotal | 95 (54.9) | 86 (48.9) | ||
| Total | 78 (45.1) | 90 (51.1) | ||
| Tumor size (cm) | 0.145 | |||
| Mean (SD) | 5.3 (3.4) | 4.8 (3.1) | ||
| Lauren type | 0.627 | |||
| Intestinal | 91 (52.6) | 88 (50) | ||
| Diffuse/mixed | 82 (47.4) | 88 (50) | ||
| Grade of histological differentiation | 0.151 | |||
| Well/moderately differentiated | 85 (49.1) | 73 (41.5) | ||
| Poorly differentiated | 88 (50.9) | 103 (58.5) | ||
| Peritumoral inflammatory infiltrate | 0.080 | |||
| Absent/mild | 122 (71,3) | 110 (62.5) | ||
| Moderate/intense | 49 (28.7) | 66 (37.5) | ||
| Lymphatic invasion | 0.120 | |||
| No | 79 (45.7) | 95 (54) | ||
| Yes | 94 (54.3) | 81 (46) | ||
| Venous invasion | 0.038 | |||
| No | 110 (63.6) | 130 (73.9) | ||
| Yes | 63 (36.4) | 46 (26.1) | ||
| Perineural Invasion | 0.874 | |||
| No | 86 (49.7) | 86 (48.9) | ||
| Yes | 87 (50.3) | 90 (51.1) | ||
| pT status | 0.079 | |||
| pT1/T2 | 57 (32.9) | 74 (42) | ||
| pT3/T4 | 116 (67.1) | 102 (58) | ||
| No of lymph nodes | 0.562 | |||
| Mean (SD) | 39.7 (17.8) | 38.5 (19.1) | ||
| pN status | 0.854 | |||
| pN0 | 74 (42.8) | 77 (43.8) | ||
| pN+ | 99 (57.2) | 99 (56.2) | ||
| pTNM status | 0.883 | |||
| I/II | 93 (53.8) | 96 (54.5) | ||
| III/IV | 80 (46.2) | 80 (45.5) | ||
| c-MET | 0.122 | |||
| c-MET-negative | 82 (47.4) | 98 (55.7) | ||
| c-MET-positive | 91 (52.6) | 78 (44.3) | ||
| RhoA | 0.422 | |||
| Low-RhoA | 90 (52) | 84 (47.7) | ||
| High-RhoA | 83 (48) | 92 (52.3) | ||
| HER2 * | 0.046 | |||
| HER2 (0/+1) | 128 (77.6) | 142 (86.1) | ||
| HER2 (+2/+3) | 37 (22.4) | 23 (13.9) | ||
| E-cadherin * | 0.608 | |||
| Normal | 148 (91.4) | 148 (89.7) | ||
| Loss of expression | 14 (8.6) | 17 (10.3) | ||
| Disease-Free Survival | Univariate Analysis | Multivariate Analysis | ||||
| Variables | HR | 95% CI | p | HR | 95% CI | p |
| Male (vs female) | 1.12 | 0.75–1.66 | 0.579 | ― | ― | ― |
| Age > 65 (vs <65 years) | 0.84 | 0.57–1.24 | 0.384 | ― | ― | ― |
| Total Gastrectomy (vs. subtotal) | 2.52 | 1.69–3.76 | <0.001 | 2.05 | 1.37–3.09 | 0.001 |
| Diffuse/mixed Lauren type (vs. others) | 1.65 | 0.12–2.44 | 0.011 | 1.11 | 0.74–1.65 | 0.620 |
| pT3/T4 status (vs. pT1/T2) | 7.68 | 4.00–14.75 | <0.001 | 3.83 | 1.92–7.64 | <0.001 |
| pN+ (vs. pN0) | 5.92 | 3.42–10.24 | <0.001 | 3.32 | 1.86–5.92 | <0.001 |
| c-MET-negative (vs. c-MET-positive) | 1.70 | 1.14–2.52 | 0.009 | 1.26 | 0.84–1.90 | 0.258 |
| Low-RhoA (vs. High-RhoA) | 1.67 | 1.13–2.47 | 0.010 | 1.35 | 0.90–2.02 | 0.152 |
| Low-CLDN18 (vs. High-CLDN18) | 0.93 | 0.64–1.37 | 0.719 | ― | ― | ― |
| non-CMT (vs. CMT) | 0.72 | 0.48–1.07 | 0.099 | ― | ― | ― |
| Overall Survival | Univariate Analysis | Multivariate Analysis | ||||
| Variables | HR | 95% CI | p | HR | 95% CI | p |
| Male (vs. female) | 1.21 | 0.87–1.67 | 0.253 | ― | ― | ― |
| Age > 65 (vs <65 years) | 1.22 | 0.89–1.67 | 0.218 | ― | ― | ― |
| Total Gastrectomy (vs. subtotal) | 2.08 | 1.51–2.86 | <0.001 | 1.87 | 1.35–2.58 | <0.001 |
| Diffuse/mixed Lauren type (vs. others) | 1.25 | 0.91–1.71 | 0.162 | ― | ― | ― |
| pT3/T4 status (vs. pT1/T2) | 3.07 | 2.08–4.54 | <0.001 | 2.21 | 1.44–3.39 | <0.001 |
| pN+ (vs. pN0) | 2.55 | 1.79–3.62 | <0.001 | 1.74 | 1.18–2.56 | 0.005 |
| c-MET-negative (vs. c-MET-positive) | 1.26 | 0.92–1.73 | 0.149 | ― | ― | ― |
| Low-RhoA (vs. High-RhoA) | 1.08 | 0.79–1.47 | 0.648 | ― | ― | ― |
| Low-CLDN18 (vs. High-CLDN18) | 1.11 | 0.81–1.51 | 0.525 | ― | ― | ― |
| non-CMT (vs. CMT) | 1.01 | 0.74–1.39 | 0.932 | ― | ― | ― |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, M.A.; Ramos, M.F.K.P.; Dias, A.R.; Cardili, L.; Ribeiro, R.R.e.; de Castria, T.B.; Zilberstein, B.; Nahas, S.C.; Ribeiro, U., Jr.; de Mello, E.S. RhoA, Claudin 18, and c-MET in Gastric Cancer: Clinicopathological Characteristics and Prognostic Significance in Curative Resected Patients. Med. Sci. 2022, 10, 4. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010004
Pereira MA, Ramos MFKP, Dias AR, Cardili L, Ribeiro RRe, de Castria TB, Zilberstein B, Nahas SC, Ribeiro U Jr., de Mello ES. RhoA, Claudin 18, and c-MET in Gastric Cancer: Clinicopathological Characteristics and Prognostic Significance in Curative Resected Patients. Medical Sciences. 2022; 10(1):4. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010004
Chicago/Turabian StylePereira, Marina Alessandra, Marcus Fernando Kodama Pertille Ramos, Andre Roncon Dias, Leonardo Cardili, Renan Ribeiro e Ribeiro, Tiago Biachi de Castria, Bruno Zilberstein, Sergio Carlos Nahas, Ulysses Ribeiro, Jr., and Evandro Sobroza de Mello. 2022. "RhoA, Claudin 18, and c-MET in Gastric Cancer: Clinicopathological Characteristics and Prognostic Significance in Curative Resected Patients" Medical Sciences 10, no. 1: 4. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010004