Quantification of All-Trans Retinoic Acid by Liquid Chromatography–Tandem Mass Spectrometry and Association with Lipid Profile in Patients with Type 2 Diabetes

 ,
,
Abstract
:1. Introduction
2. Results
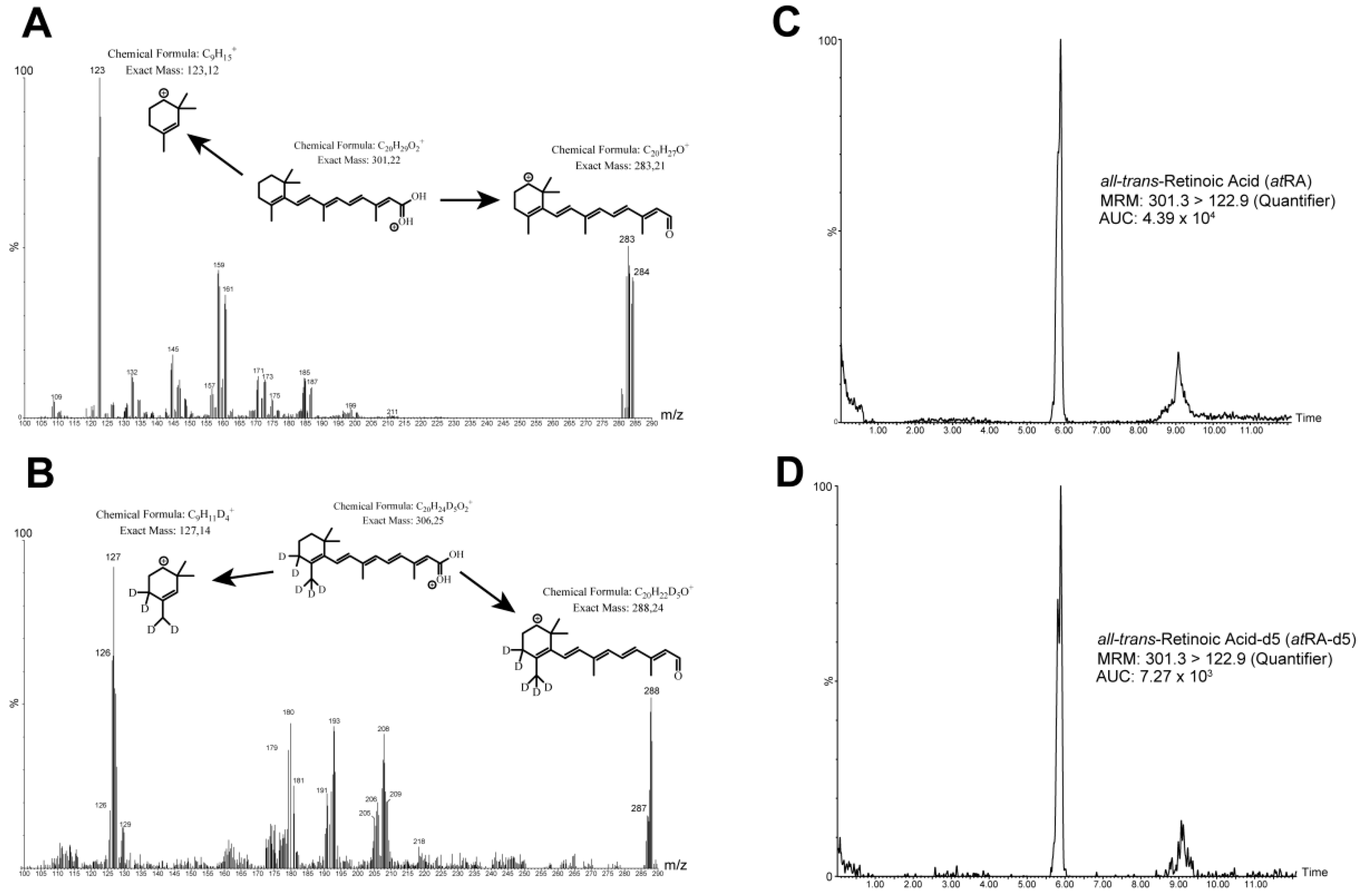
2.1. Fragmentation and Mass Transitions
2.2. Chromatography
2.3. Analytical Specificity
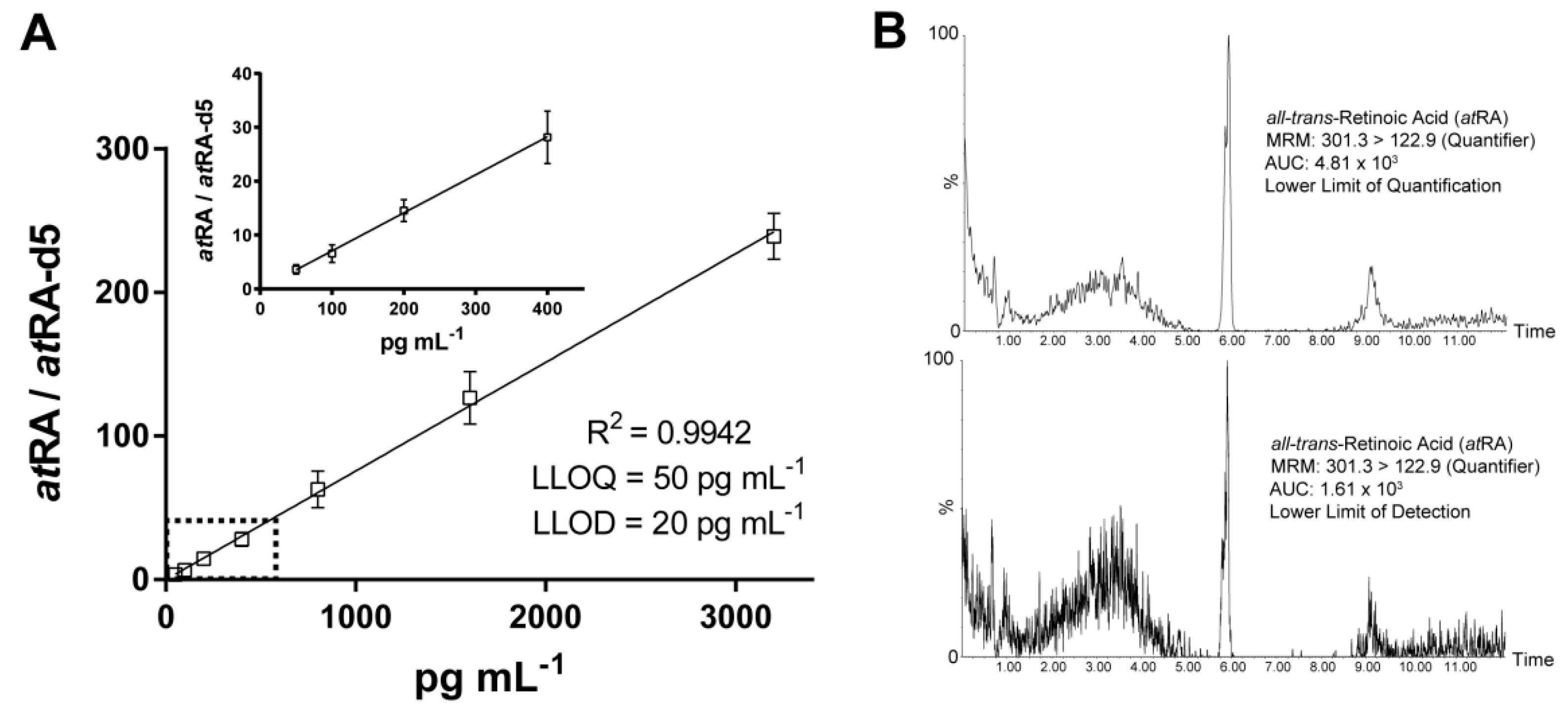
2.4. Linearity and Determination Limits
2.5. Recovery, Precision, and Accuracy
2.6. Stability
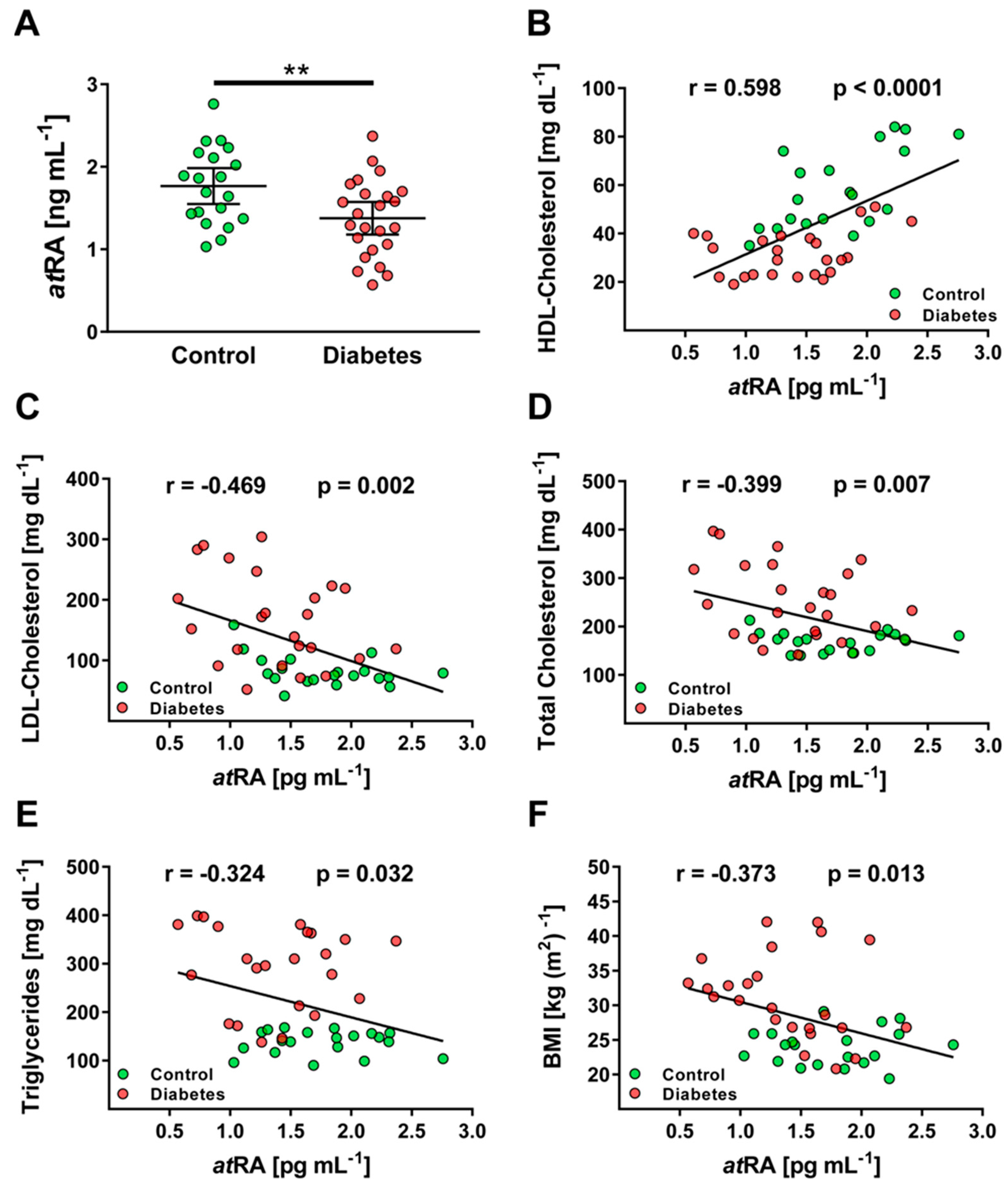
2.7. Clinical Application
3. Discussion
4. Materials and Methods
4.1. Chemicals and Reagents
4.2. Preparation of Calibration Standards
4.3. Sample Collection and Extraction
4.4. Chromatography
4.5. Mass Spectrometry
4.6. Validation Procedure
4.7. Clinical Chemistry
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marill, J.; Idres, N.; Capron, C.; Nguyen, E.; Chabot, G. Retinoic Acid Metabolism and Mechanism of Action: A Review. Curr. Drug Metab. 2003, 4, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Cifelli, C.J.; Ross, A.C. All-trans-retinoic acid distribution and metabolism in vitamin A-marginal rats. Am. J. Physiol. Gastrointest. Liver Physiol. 2006, 291, G195–G202. [Google Scholar] [CrossRef] [PubMed]
- Kedishvili, N.Y. Enzymology of retinoic acid biosynthesis and degradation: Thematic Review Series: Fat-Soluble Vitamins: Vitamin A. J. Lipid. Res. 2013, 54, 1744–1760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.A.; Parkinson, D.R.; Cheson, B.D.; Friedman, M.A. Retinoids in cancer therapy. J. Clin. Oncol. 1992, 10, 839–864. [Google Scholar] [CrossRef]
- Goldfarb, M.T.; Ellis, C.N.; Voorhees, J.J. Retinoids in Dermatology. Mayo Clin. Proc. 1987, 62, 1161–1164. [Google Scholar] [CrossRef] [Green Version]
- Obrochta, K.M.; Krois, C.R.; Campos, B.; Napoli, J.L. Insulin regulates retinol dehydrogenase expression and all-trans-retinoic acid biosynthesis through FoxO1. J. Biol. Chem. 2015, 290, 7259–7268. [Google Scholar] [CrossRef] [Green Version]
- Sierra-Modragon, E.; Molina-Jijon, E.; Namorado-Tonix, C.; Rodriguez-Munoz, R.; Pedraza-Chaverri, J.; Reyes, J.L. All-trans retinoic acid ameliorates inflammatory response mediated by TLR4/NF-κB during initiation of diabetic nephropathy. J. Nutr. Biochem. 2018, 60, 47–60. [Google Scholar] [CrossRef]
- Arnold, S.L.M.; Amory, J.K.; Walsh, T.J.; Isoherranen, N. A sensitive and specific method for measurement of multiple retinoids in human serum with UHPLC–MS/MS. J. Lipid. Res. 2012, 53, 587–598. [Google Scholar] [CrossRef] [Green Version]
- De Leenheer, A.P.; Lambert, W.E.; Claeys, I. All-trans-retinoic acid: Measurement of reference values in human serum by high performance liquid chromatography. J. Lipid. Res. 1982, 23, 1362–1367. [Google Scholar] [CrossRef]
- Gundersen, T.E.; Bastani, N.E.; Blomhoff, R. Quantitative high-throughput determination of endogenous retinoids in human plasma using triple-stage liquid chromatography/tandem mass spectrometry. Rapid. Commun. Mass. Spectrom. 2007, 21, 1176–1186. [Google Scholar] [CrossRef]
- Teerlink, T.; Copper, M.P.; Klaassen, I.; Braakhuis, B.J. Simultaneous analysis of retinol, all-trans- and 13-cis-retinoic acid and 13-cis-4-oxoretinoic acid in plasma by liquid chromatography using on-column concentration after single-phase fluid extraction. J. Chromatogr. B Biomed. Sci. Appl. 1997, 694, 83–92. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, H.; Wang, J.; Zhou, W.; Sun, R.; Xia, M. Association of serum retinoic acid with hepatic steatosis and liver injury in nonalcoholic fatty liver disease. Am. J. Clin. Nutr. 2015, 102, 130–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muindi, J.R.; Frankel, S.R.; Huselton, C.; DeGrazia, F.; Garland, W.A.; Young, C.W.; Warrell, R.P. Clinical pharmacology of oral all-trans retinoic acid in patients with acute promyelocytic leukemia. Cancer Res. 1992, 52, 2138–2142. [Google Scholar] [PubMed]
- Eckhoff, C.; Nau, H. Identification and quantitation of all-trans- and 13-cis-retinoic acid and 13-cis-4-oxoretinoic acid in human plasma. J. Lipid. Res. 1990, 31, 1445–1454. [Google Scholar] [CrossRef]
- De Ruyter, M.G.; Lambert, W.E.; De Leenheer, A.P. Retinoic acid: An endogenous compound of human blood. Unequivocal demonstration of endogenous retinoic acid in normal physiological conditions. Anal. Biochem. 1979, 98, 402–409. [Google Scholar] [CrossRef]
- Napoli, J.L.; Pramanik, B.C.; Williams, J.B.; Dawson, M.I.; Hobbs, P.D. Quantification of retinoic acid by gas–liquid chromatography–mass spectrometry: Total versus all-trans-retinoic acid in human plasma. J. Lipid. Res. 1985, 26, 387–392. [Google Scholar] [CrossRef]
- Nikolac, N. Lipemia: Causes, Interference Mechanisms, Detection and Management. Biochem. Med. 2014, 24, 57–67. [Google Scholar] [CrossRef] [Green Version]
- Jialal, I. A Practical Approach to the Laboratory Diagnosis of Dyslipidemia. Am. J. Clin. Pathol. 1996, 106, 128–138. [Google Scholar] [CrossRef] [Green Version]
- Morgenstern, J.; Fleming, T.; Kadiyska, I.; Brings, S.; Groener, J.B.; Nawroth, P.; Hecker, M.; Brune, M. Sensitive mass spectrometric assay for determination of 15-deoxy-Δ12,14-prostaglandin J2 and its application in human plasma samples of patients with diabetes. Anal. Bioanal. Chem. 2018, 410, 521–528. [Google Scholar] [CrossRef] [Green Version]
- Kane, M.A.; Chen, N.; Sparks, S.; Napoli, J.L. Quantification of endogenous retinoic acid in limited biological samples by LC/MS/MS. Biochem. J. 2005, 388, 363–369. [Google Scholar] [CrossRef] [Green Version]
- Peng, J.-B.; Luo, C.-H.; Wang, Y.-C.; Huang, W.H.; Chen, Y.; Zhou, H.H.; Tan, Z.R. Validation of a Liquid Chromatography–Electrospray Ionization-Tandem Mass Spectrometry Method for Determination of All-Trans Retinoic Acid in Human Plasma and Its Application to a Bioequivalence Study. Molecules 2014, 19, 1189–1200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Chen, H.; Mu, D.; Fan, J.; Song, J.; Zhong, Y.; Li, D.; Xia, M. Circulating Retinoic Acid Levels and the Development of Metabolic Syndrome. J. Clin. Endocrinol. Metab. 2016, 101, 1686–1692. [Google Scholar] [CrossRef] [PubMed]
- Rhee, E.-J.; Plutzky, J. Retinoid Metabolism and Diabetes Mellitus. Diabetes Metab. J. 2012, 36, 167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, J.; Guleria, R.; Zhu, S.; Baker, K. Molecular Mechanisms of Retinoid Receptors in Diabetes-Induced Cardiac Remodeling. J. Clin. Med. 2014, 3, 566–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maier, M.; Reinert, M.; Lehnert, M.; Bauer, C.; Marzi, I. Perioperative Application of a Serum Protein Solution (Biseko®) After Proximal Femur Fracture of Elder Patients. Eur. J. Trauma Emerg. S 2007, 33, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Nauck, M.; Gerdes, C.; Petersmann, A.; Müller-Wieland, D.; Müller, U.A.; Freckmann, G.; Heinemann, L.; Schleicher, E.; Landgraf, R. Definition, Klassifikation und Diagnostik des Diabetes mellitus: Update 2020. Diabetol. Und Stoffwechs. 2020, 15, S9–S17. [Google Scholar] [CrossRef]
- Knopfholz, J.; Disserol, C.C.D.; Pierin, A.J.; Schirr, F.L.; Streisky, L.; Takito, L.L.; Massucheto Ledesma, P.; Faria-Neto, J.R.; Olandoski, M.; da Cunha, C.L.P.; et al. Validation of the Friedewald Formula in Patients with Metabolic Syndrome. Cholesterol 2014, 1–5. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Analytes | Rt (min) | MRM Quantifier (m/z) | MRM Qualifier (m/z) | COV (V) | CE (V) |
|---|---|---|---|---|---|
| atRA | 5.90 | 301.3 > 122.9 | 301.1 > 283.1 | 23 | 16 |
| atRA-d5 | 5.89 | 306.3 > 126.8 | 306.3 > 288.1 | 26 | 16 |
| Parameter | Nominal Concentration (pg mL−1) | Recovery (%) | Measured Concentration (pg mL−1) | Accuracy (%) | Precision (% CV) | Precision of Retention Time (% CV) |
|---|---|---|---|---|---|---|
| Intraday | 50 600 2500 | 87.4 ± 8.2 90.0 ± 6.4 91.7 ± 12.9 | 46.8 ± 4.6 618.6 ± 41.7 2320.4 ± 263.2 | 93.6 103.1 92.8 | 9.8 6.7 11.3 | 5.5 |
| Interday | 50 600 2500 | 57.9 ± 8.3 519.4 ± 81.2 2549.6 ± 307.3 | 115.8 86.6 102.0 | 14.3 15.6 12.1 | ||
| Long-term | Various | 94.0 ± 14.2 | 17.8 |
| Conditions | Recovery | |
|---|---|---|
| Preprocessed | Postprocessed | |
| 1 h at 20 °C | 93 ± 12% | |
| 6 h at 20 °C | 84 ± 19% | |
| 1 h at 4 °C | 89 ± 17% | |
| 6 h at 4 °C | 81 ± 21% | 77 ± 18% |
| 1 week at 4 °C | 51 ± 31% | 44 ± 14% |
| 1 week at −20 °C | 91 ± 9% | |
| 1 month at −20 °C | 101 ± 15% | 93 ± 16% |
| F/T stability (6 cycles) | 82 ± 22% | |
| Parameter- | Controls (n = 20) | Type 2 Diabetes (n = 24) |
|---|---|---|
| Sex (% male) | 63.8 | 65.3 |
| Age (years) | 42.1 ± 12.3 | 49.6 ± 15.5 |
| Body-mass index (BMI; kg·m−2) | 24 ± 2.5 | 31.3 ± 6.1 *** |
| Blood glucose (mg·dL−1) | 97.1 ± 12.3 | 186.3 ± 84.3 *** |
| HbA1c (%) | 5.7 ± 0.8 | 11.2 ± 1.6 *** |
| C-reactive protein (CRP; mg·L−1) | 1.2 ± 1.1 | 12.9 ± 8.6 *** |
| Total cholesterol (mg dL−1) | 168.4 ± 19.9 | 256.1 ± 74.5 *** |
| Triglycerides (mg dL−1) | 137.7 ± 24.2 | 285.3 ± 86.4 *** |
| Low-density lipoprotein (LDL; mg·dL−1) | 82.7 ± 25.7 | 167.5 ± 73.4 *** |
| High-density lipoprotein (HDL; mg·dL−1) | 58.2 ± 15.9 | 31.5 ± 9.1 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morgenstern, J.; Fleming, T.; Kliemank, E.; Brune, M.; Nawroth, P.; Fischer, A. Quantification of All-Trans Retinoic Acid by Liquid Chromatography–Tandem Mass Spectrometry and Association with Lipid Profile in Patients with Type 2 Diabetes. Metabolites 2021, 11, 60. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11010060
Morgenstern J, Fleming T, Kliemank E, Brune M, Nawroth P, Fischer A. Quantification of All-Trans Retinoic Acid by Liquid Chromatography–Tandem Mass Spectrometry and Association with Lipid Profile in Patients with Type 2 Diabetes. Metabolites. 2021; 11(1):60. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11010060
Chicago/Turabian StyleMorgenstern, Jakob, Thomas Fleming, Elisabeth Kliemank, Maik Brune, Peter Nawroth, and Andreas Fischer. 2021. "Quantification of All-Trans Retinoic Acid by Liquid Chromatography–Tandem Mass Spectrometry and Association with Lipid Profile in Patients with Type 2 Diabetes" Metabolites 11, no. 1: 60. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11010060