
Unraveling the Diversity of Co-Colonization by CPE
by
 ,
,
Gabrielle Levi
1, 
Mor Lurie-Weinberger
1,
Alona Keren-Paz
1,
Antoine O. Andremont
2,
David Schwartz
1 and
Yehuda Carmeli
1,3,* 1
National Institute for Antibiotic Resistance and Infection Control, Ministry of Health, Tel Aviv 6423906, Israel
2
Microbiology Department, Université Paris Diderot, Sorbonne Paris Cité, 75018 Paris, France
3
Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv 6997801, Israel
*
Author to whom correspondence should be addressed.
Microorganisms 2022, 10(7), 1292; https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms10071292
Submission received: 31 May 2022
/
Revised: 16 June 2022
/
Accepted: 20 June 2022
/
Published: 25 June 2022
(This article belongs to the Special Issue Bacterial Enzymes and Antibiotic Resistance)
Abstract
:Antibiotic-resistant bacteria, and more specifically, carbapenem-producing Enterobacterales (CPE) strains, are increasing worldwide. Despite their growing prevalence, in most high-income countries, the detection of CPE is still considered a low-frequency event. Sporadically, patients co-colonized with distinct CPE strains and/or different carbapenemase enzymes are detected. In this paper, we present three cases that illustrate the underlying mechanisms of co-colonization, focusing on horizontal gene transfer (HGT) and patient-to-patient transmission. We also demonstrate the diversity of CPE species and discuss the potential consequences of co-colonization.
1. Introduction
The emergence and spread of bacteria with multi-drug resistance (MDR) is a major public health concern worldwide, declared by the World Health Organization (WHO) as one of the top 10 global public health threats [1]. In 2019, more than 1.2 million deaths were directly attributable to bacterial MDR, with the overall death toll estimated at 4.95 million deaths [2]. Of the resistant bacteria listed as “critical” [3], carbapenem-resistant Enterobacteriaceae (CRE) are considered an urgent threat [4].
While some bacteria are naturally resistant to carbapenems, the rapid spread of CRE across the globe is mainly driven by acquired resistance, with susceptible bacteria gaining resistance by acquiring genes that encode for a variety of carbapenem-hydrolyzing enzymes [5], thus becoming carbapenem-producing Enterobacterales (CPE). This horizontal gene transfer (HGT) is mediated by various genetic elements, including plasmids, transposons [6], and integrons [7,8], and can occur between clones of a single species or between different species [9,10] within the human body. The gastrointestinal tract of hospitalized patients, with its diverse microbiota, is an ideal setting for HGT [11,12] promoting the spread of carbapenem resistance. Patients treated with carbapenems are particularly prone to becoming colonized by CRE, even if exposure is short [13,14]. Mobile genetic elements carrying resistance genes have been implicated in the patient-to-patient spread of resistant isolates and have been identified as the cause of many outbreaks [15,16]. Patient mobility has also been highlighted as a risk factor for CRE acquisition and spread [17], and the transfer of patients to different countries has been shown to introduce novel CRE variants into healthcare systems [18,19].
Typically, a single strain of CPE, carrying a single carbapenemase gene, is identified in a colonized patient. Occasionally, the co-carriage of two carbapenamases in the same strain is detected. However, as there is potential to acquire multiple CPEs exogenously (patient to patient), and for HGT to then occur across different species within the gastrointestinal tract, patients may have a substantial risk of becoming colonized with more than one CRE species. Whilst this phenomenon is now beginning to be investigated [20,21,22], these types of cases remain under-reported in the literature. Here, we describe in detail several such co-colonization cases with Klebsiella pneumoniae carbapenemase (KPC) and New Delhi metallo-beta-lactamase (NDM), focusing on the variety of the underlying genetic, microbiological, and epidemiological mechanisms.
2. Epidemiological Background from the National Center for Infection Control, Israel
Over the last 3 years, 95.6% of the total cases of CPE carriers reported to the National Registry of the National Centre for Infection Control (NCIC), Israel, had a single carbapenemase gene, while 4.4% of the CPE carriers had more than one type of carbapenemase. In 62% of those cases, the two carbapenemases were present in the same isolate, while in the remaining 38%, the different carbapenemases were present in different bacterial species.
3. Case Studies
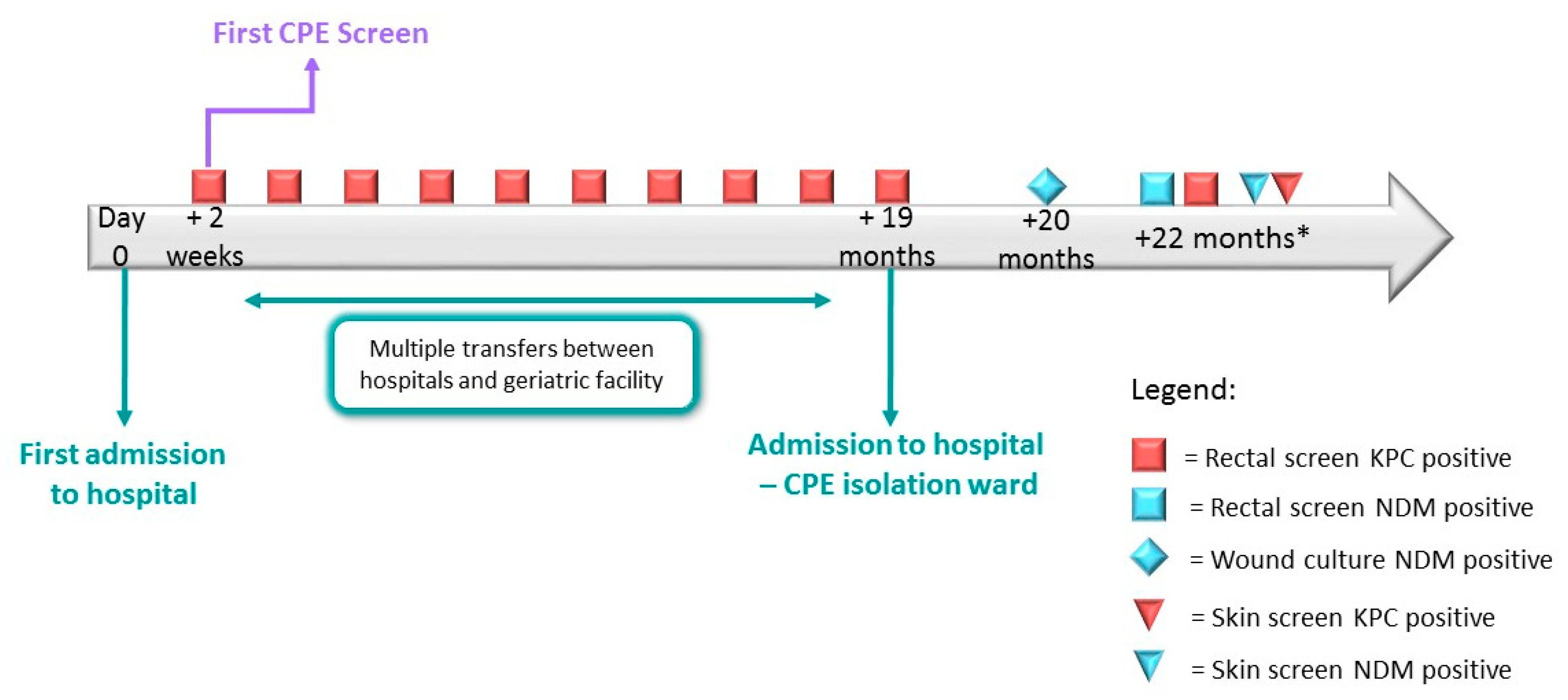
In Case 1, a sixty-seven-year-old male was admitted to a hospital. In accordance with screening protocols, he was not screened on admission for CPE carriage as he had no risk factors. Two weeks after admission, routine screening revealed him to be CPE-positive, carrying Klebsiella pneumoniae carbapenemase (KPC)-producing Enterobacter cloacae. Subsequently, the patient had multiple hospitalizations and was transferred between different geriatric centers, and repeated CPE screening samples returned results positive for KPC-producing Enterobacter cloacae until the date of his next hospitalization, nearly two years later. The patient was hospitalized in a CPE cohort ward. The following month, a second CPE acquisition was identified—the patient’s wound culture was positive for New Delhi metallo-beta-lactamase (NDM)-producing K. pneumoniae. Two months later, whilst hospitalized in a geriatric medical center, he was screened for the presence of MDR bacteria, as part of a point prevalence study carried out by the NCIC. He was found to be positive for both KPC- and NDM-producing Enterobacterales. The rectal sample was found to contain NDM-producing K. pneumoniae and KPC-producing K. pneumoniae, whilst the skin sample contained NDM-producing E. coli and KPC-producing K. pneumoniae (Figure 1 and Table 1). Further WGS conducted by the NCIC laboratory confirmed that the patient was infected with two distinct K. pneumoniae isolates, carrying two different carbapenemase genes (Table 1).
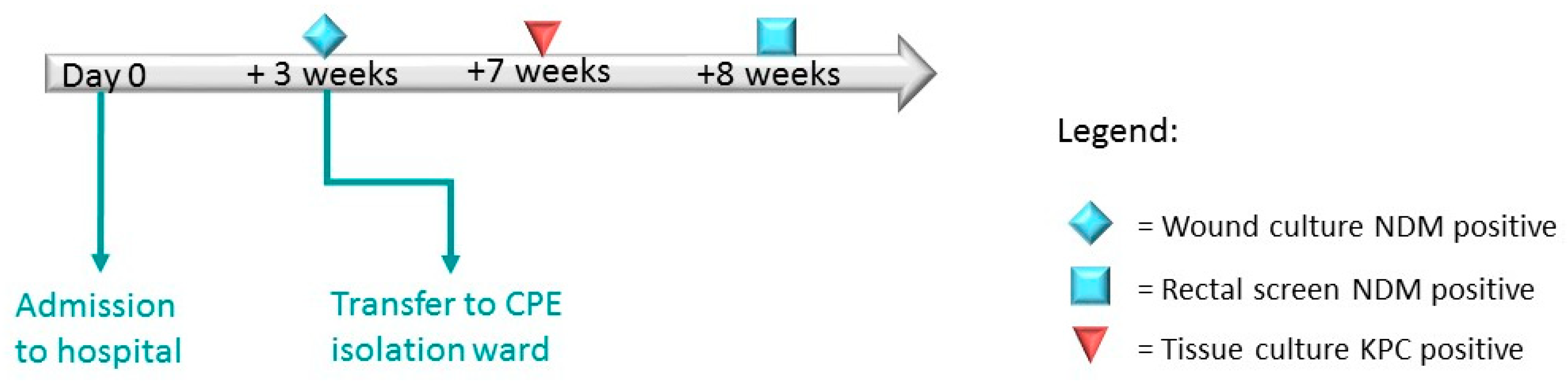
In Case 2, a 48-year-old man was admitted to an orthopedic department. Due to having no risk factors, this patient was not screened for CPE upon admission. Three weeks after admission, his surgical wound culture was identified as positive for NDM-producing K. oxytoca, and he was subsequently transferred to a CPE cohort ward. One month after his transfer, a tissue sample culture was identified as positive for KPC-producing E. cloacae. Concurrently, a rectal screening sample returned a positive result for NDM-producing E. cloacae (Figure 2 and Table 2). WGS analysis proved that the two E. cloacae isolates were distinct from one another (Table 2). Further analysis revealed that the K. oxytoca and the secondary E. cloacae carried the same variant of blaNDM. Strikingly, plasmid content analysis detected the presence of an IncX3 plasmid within both isolates (Table 2).
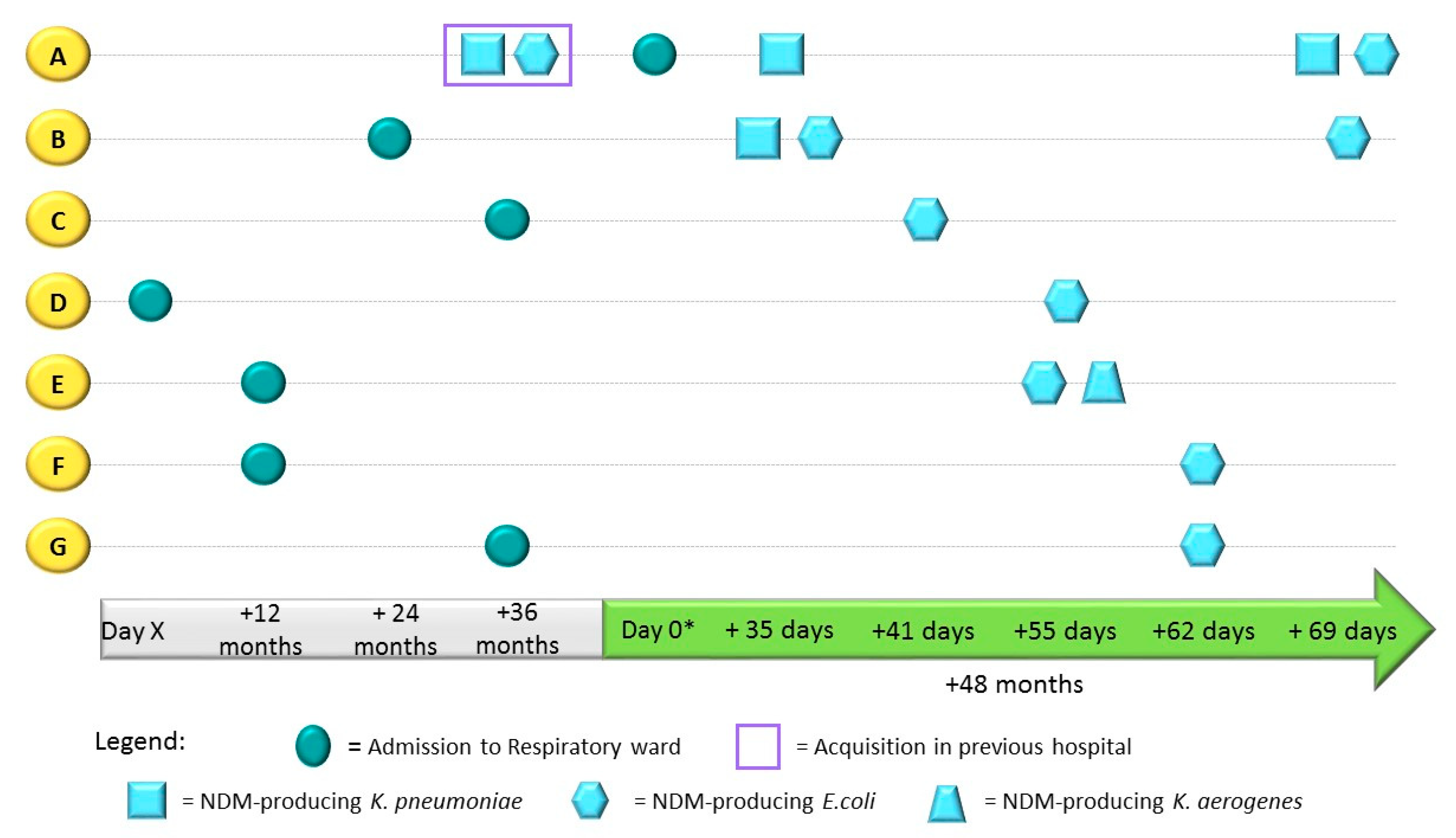
In Case 3, an outbreak of NDM-producing CPE in a ward of a post-acute care facility was detected. According to surveillance data reported to the NCIC, this was the first documentation of CPE transmission on this ward in 10 years. When patient A was admitted to the ward, he was known to have been previously colonized by NDM-producing E. coli and K. pneumoniae. Despite his CPE status, he was housed in a room with patient B. Shortly after patient A’s admission to the ward, patient B, who had been hospitalized for two years previous, was tested for CPE during routine screening and was found to be positive (Figure 3). Nursing staff at the NCIC were alerted, and point prevalence screening was then carried out weekly in the department in order to detect colonization and aid in the epidemiological investigation. Five additional patients (C–G) on the respiratory ward, some of whom shared a room with patient B, were subsequently found to be positive. For all these patients, this was the first positive result for CPE after one to four years of hospitalization (Figure 3). All positive screening samples were analyzed at the NCIC Reference Laboratory. Patient A’s initial rectal screen on admission was found to be positive for NDM-producing K. pneumoniae. Screening conducted one month later detected both NDM-producing E. coli and K. pneumoniae. Patient B’s rectal screen sample was found to be positive for NDM-producing E. coli and K. pneumoniae. Patients C–G were all found to be positive for NDM-producing E. coli, and patient E’s rectal screen showed NDM-producing K. aerogenes (Table 3, Figure 3). WGS analysis of the E. coli and K. pneumoniae from patient B showed that the two strains carried different blaNDM variants (blaNDM-7 and blaNDM-5, respectfully). In addition, the E. coli strain contained an IncX3 plasmid. Further Sanger sequencing of the NDM-producing E. coli and K. aerogenes from patients C–G detected the presence of the blaNDM7 variant (Table 3) and showed that they had an IncX3 plasmid sharing a high degree of sequence identity with a previously reported plasmid, pC158-NDM7-IncX3 (Gen Bank accession: MN175471.1)
4. Methods
Case Study 1: Point prevalence study. Rectal and skin samples were used to inoculate liquid brain heart infusion (BHI) broth. After overnight incubation at 37 °C, the broth was sub-cultured on selective agar media for CPE (CHROMagar mSuperCARBA, Hy Laboratories Ltd., Rehovot, Israel). Both the BHI broth and suspect CPE colonies (when present) were tested for the presence of carbapenemase genes (including blaKPC, blaNDM, blaIMI, blaVIM, and blaOXA-48-like) by multiplex polymerase chain reaction (PCR) based on Israeli National Policy for CPE Screening [23,24,25,26]. The presence of a carbapenemase was confirmed using a commercial ‘β-Carba Test’ kit (Biorad, Marnes-la-Coquette, France). Species identification and antibiotic susceptibility testing was performed using VITEK™ 2 (Biomerieux SA, Marcy I’Etoile, France). Whole genome sequencing (WGS) was performed on the NDM- and KPC-producing K. pneumoniae.
Case Studies 2 and 3: Upon receipt at the Reference Laboratory for Antibiotic Resistance (National Institute for Antibiotic Resistance, Ministry of Health), isolates were sub-cultured on CPE-selective media, and suspect CPE colonies were tested as outlined for Case Study 1. In Case 2, an additional immunochromatographic assay was performed, which was able to detect and differentiate between KPC, OXA-48-like, VIM, IMP, and NDM carbapenemases (NG-Test CARBA 5, NG Biotech, Guipry-Messac, France).
Whole genome sequencing (WGS): Sequencing was performed by the Sequencing Core at RUSH University, Chicago, IL, USA. Libraries were prepared using the Nextera XT (Illumina Inc., San Diego, CA, USA) kit, followed by sequencing on the Illumina NovaSeq (Illumina Inc.) using the high-output 2 × 150 bp kit (Illumina Inc.). De novo assembly was achieved using CLC Genomics Workbench protocol with default parameters. Strain MLST typing was determined with MLST software (https://github.com/tseemann/mlst (accessed on 5 May 2022)). The capsular polysaccharide (KL) and lipooligosaccharide outer core (OCL) synthesis was determined using Kaptive [27]. Antibiotic resistance genes were tested using the Center of Genomic Epidemiology ResFinder (https://cge.cbs.dtu.dk/services/ResFinder/ (accessed on 5 May 2022)). Plasmids were detected using PlasmidFinder (https://cge.food.dtu.dk/services/PlasmidFinder/ (accessed on 5 May 2022)). Sanger sequencing of blaNDM PCR products was performed by Hy laboratories, Israel.
Institutional review board approval was not required for this study.
5. Discussion
The most important finding of this study demonstrates that co-colonization with different CPEs may occasionally occur and is often detected by screening patients in cohort wards or patients who have a high risk of CPE carriage. It involves a high diversity of species, thus increasing the potential for further transmission and spread of the carbapenemase genes into bacterial species previously susceptible to carbapenems. This is because one patient can acquire multiple CPEs through patient-to-patient transmission, or a patient can acquire a CPE and subsequently experience HGT across different species within the gastrointestinal tract.
In Cases 1 and 2, the two patients had no previously known or documented risk factors for CPE upon hospitalization, but were likely colonized (Case 1) or infected (Case 2) with CPE during their stay in the hospital. The combination of the documented screening results in Case 1 and the positive CPE results from both patients obtained by the NCIC Reference Laboratory allows us to conclude with high certainty that both secondary CPE acquisitions of a different carbapenemase gene occurred on the CPE isolation ward. This demonstrates that the inappropriate cohorting of patients with different carbapenemases is a risk factor for co-colonization with CPE and can lead to the acquisition of additional resistance mechanisms by previously resistant or susceptible bacteria.
Another example of the results of failure to isolate a CPE carrier was reported in Case Study 3. In this case, an outbreak was caused by a clonally related blaNDM7-producing E. coli strain, transmitted between six patients and leading to their colonization. Most noteworthy in Case Study 3, however, is the clear evidence of HGT, which occurred in patient E. The rapid global spread of blaNDM in different bacterial species is extensively reported in the literature, because this gene is carried on a broad host range of conjugative plasmids [28,29]. Here, we discuss two cases of HGT occurring between distinct bacterial species that were very likely mediated by a plasmid: (1) blaNDM-7 was transferred between IncX3-carrying E. coli and K. aerogenes (Case 3) and (2) blaNDM-1 was transferred between K. oxytoca and E. cloacae (Case 2), both carrying IncX3. Despite the lack of detailed data on all CPE-positive isolates in Case Study 1, it is possible that HGT occurred twice in this patient: (1) blaKPC-3 was transferred between E. cloacae and K. pneumoniae ST512, and (2) blaNDM-1 was transferred between K. pneumoniae ST417 and E. coli. The repetition of this event in our results suggests that cross-species transmission occurs more frequently than is currently believed, especially during co-colonization events [20].
One reason for the underestimation of the frequency of co-colonization events is the in-depth WGS analysis needed for its detection. The WGS analysis performed by NCIC Reference Laboratory identified two distinct NDM variants (blaNDM-7 and blaNDM-5) within three different bacterial species in Case 3. Additionally, the WGS analysis of isolates from Case 1 and 2 identified two distinct K. pneumoniae and two different E. cloacae strains, belonging to different ST types. In each case, the different strains carried different carbapenemase genes. Without sequencing to determine the exact ST type and the specific allele within each species, the complex picture of co-colonization would have remained unclear.
The diversity of co-colonization described here highlights the importance of sub-classifying patients according to the carbapenemase genes carried by their CPE strains, rather than just according to the detection of CPE. Previous studies have suggested that multiple colonization with CPE may increase the risk of further infection with these organisms [21]. This could drastically lower patient outcomes, increasing morbidity and mortality due to complicated infections with very limited treatment options. The variety of species, carrying different carbapenemase genes, present in the same crowded niche (the GI tract), may carry a substantial risk of simultaneous colonization with more than one CPE species. The increasing prevalence of CPE worldwide [30,31,32] further increases this risk.
The inappropriate isolation and cohorting of patients with different resistance mechanisms increases the likelihood of co-colonization. Therefore, to improve patient outcomes, patients should be separated whenever feasible. Not detecting the presence of CPE allows transmission to occur, increasing the risk of co-colonization. The screening of patients with CPE or those who are at risk of CPE is essential for detecting changes in colonization status and allows fast action to prevent transmission or acquisition.
There are several limitations to this study. Not all isolates were available for WGS and plasmid extraction, and therefore the genetic analysis was not complete. In addition, the identification of all potential CPE species from screening swabs is subject to microbiological and technical limitations, and therefore the CPE detection results may have been underestimated.
6. Conclusions
We demonstrate here that there is no single CPE status: multiple different CPE strains may be present in a single CPE-positive patient. The diversity of resistance genes and the presence of natural HGT mechanisms increases the potential of the spread of multiple carbapenemases between different currently susceptible bacterial species, allowing the possible combinations of CPE to become infinite. It is therefore of vital importance to continue global efforts to control the spread of these MDR organisms through appropriate cohorting, increased screening, and performing real-time in-depth genetic analysis in clinical settings.
Supplementary Materials
The following supporting information can be downloaded at: https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/microorganisms10071292/s1. Table S1. sequence data information.
Author Contributions
Conceptualization, G.L. and Y.C.; methodology, G.L.; validation, D.S. and A.K.-P.; formal analysis, M.L.-W.; investigation, G.L. and M.L.-W.; data curation, M.L.-W.; writing—original draft preparation, G.L.; writing—review and editing, A.K.-P. and A.O.A.; visualization, G.L.; supervision, Y.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
All sequence data were deposited at the NCBI repository under BioProject PRJNA843363 (see Supplementary Materials for sequence data information).
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO. World Health Organisation Antimicrobial Resistance. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 1 May 2022).
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Tacconelli, E.; Magrini, N.; Kahlmeter, G.; Singh, N. Global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics. World Health Organ. 2017, 27, 318–327. [Google Scholar]
- Antibiotic Resistance Threats in the United States; U.S. Centers for Disease Control and Prevention CDC: Atlanta, GA, USA, 2019.
- Nordmann, P.; Poirel, L. Epidemiology and Diagnostics of Carbapenem Resistance in Gram-negative Bacteria. Clin. Infect. Dis. 2019, 69, S521–S528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuzon, G.; Naas, T.; Nordmann, P. Functional characterization of Tn4401, a Tn3-based transposon involved in bla KPC gene mobilization. Antimicrob. Agents Chemother. 2011, 55, 5370–5373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yelin, I.; Kishony, R. Antibiotic Resistance. Cell 2018, 172, 1136.e1. [Google Scholar] [CrossRef] [PubMed]
- Nikaido, H. Multidrug resistance in bacteria. Annu. Rev. Biochem. 2009, 78, 119–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Chen, G.; Wu, X.; Wang, L.; Cai, J.; Chan, E.W.; Chen, S.; Zhang, R. Increased prevalence of carbapenem resistant Enterobacteriaceae in hospital setting due to cross-species transmission of the blaNDM-1 element and clonal spread of progenitor resistant strains. Front. Microbiol. 2015, 6, 595. [Google Scholar] [CrossRef] [Green Version]
- Thomas, C.M.; Nielsen, K.M. Mechanisms of, and barriers to, horizontal gene transfer between bacteria. Nat. Rev. Microbiol. 2005, 3, 711–721. [Google Scholar] [CrossRef]
- Munita, J.M.; Arias, C.A. Mechanisms of antibiotic resistance. In Virulence Mechanisms of Bacterial Pathogens; Wiley: Hoboken, NJ, USA, 2016; pp. 481–511. [Google Scholar] [CrossRef] [Green Version]
- Goodman, K.E.; Simner, P.J.; Tamma, P.D.; Milstone, A.M. Infection control implications of heterogeneous resistance mechanisms in carbapenem-resistant Enterobacteriaceae (CRE). Expert Rev. Anti. Infect. Ther. 2016, 14, 95–108. [Google Scholar] [CrossRef]
- Ventola, C.L. The Antibiotic Resistance Crisis Part 1: Causes and Threats. Pharm. Ther. 2015, 40, 277–283. [Google Scholar] [CrossRef]
- Armand-Lefèvre, L.; Angebault, C.; Barbier, F.; Hamelet, E.; Defrance, G.; Ruppé, E.; Bronchard, R.; Lepeule, R.; Lucet, J.C.; Mniai, A.E.; et al. Emergence of imipenem-resistant gram-negative bacilli in intestinal flora of intensive care patients. Antimicrob. Agents Chemother. 2013, 57, 1488–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navon-Venezia, S.; Leavitt, A.; Schwaber, M.J.; Rasheed, J.K.; Srinivasan, A.; Patel, J.B.; Carmeli, Y.; Rubinovitch, B.; Muskovitch, I.; Schwartz-Harari, O.; et al. First report on a hyperepidemic clone of KPC-3-producing Klebsiella pneumoniae in Israel genetically related to a strain causing outbreaks in the United States. Antimicrob. Agents Chemother. 2009, 53, 818–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwaber, M.J.; Lev, B.; Israeli, A.; Solter, E.; Smollan, G.; Rubinovitch, B.; Shalit, I.; Carmeli, Y. Containment of a country-wide outbreak of carbapenem-resistant klebsiella pneumoniae in israeli hospitals via a nationally implemented intervention. Clin. Infect. Dis. 2011, 52, 848–855. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control Risk Assessment on the Spread of Carbapenemase-Producing Enterobacteriaceae (CPE) through Patient Transfer between Healthcare Facilities, with Special Emphasis on Cross-Border Transfer; ECDC: Stockholm, Sweden, 2011; ISBN 9789291933174.
- Dortet, L.; Poirel, L.; Nordmann, P. Worldwide dissemination of the NDM-Type carbapenemases in Gram-negative bacteria. BioMed Res. Int. 2014, 2014, 249856. [Google Scholar] [CrossRef] [Green Version]
- Woodford, N.; Zhang, J.; Warner, M.; Kaufmann, M.E.; Matos, J.; MacDonald, A.; Brudney, D.; Sompolinsky, D.; Navon-Venezia, S.; Livermore, D.M. Arrival of Klebsiella pneumoniae producing KPC carbapenemase in the United Kingdom. J. Antimicrob. Chemother. 2008, 62, 1261–1264. [Google Scholar] [CrossRef]
- Adediran, T.; Harris, A.D.; Kristie Johnson, J.; Calfee, D.P.; Miller, L.G.; Hong Nguyen, M.; Morgan, D.J.; Goodman, K.E.; Hitchcock, S.; Pineles, L.; et al. Epidemiologic and microbiologic characteristics of hospitalized patients co-colonized with multiple species of carbapenem-resistant enterobacteriaceae in the United States. Open Forum Infect. Dis. 2020, 7, ofaa386. [Google Scholar] [CrossRef]
- Hernández-García, M.; Pérez-Viso, B.; Navarro-San Francisco, C.; Baquero, F.; Morosini, M.I.; Ruiz-Garbajosa, P.; Cantón, R. Intestinal co-colonization with different carbapenemase-producing Enterobacterales isolates is not a rare event in an OXA-48 endemic area. EClinicalMedicine 2019, 15, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Snyder, G.M.; O’Fallon, E.; D’Agata, E.M.C. Co-colonization with multiple different species of multidrug-resistant gram-negative bacteria. Am. J. Infect. Control 2011, 39, 506–510. [Google Scholar] [CrossRef] [Green Version]
- Solter, E.; Adler, A.; Rubinovitch, B.; Temkin, E.; Schwartz, D.; Ben-David, D.; Masarwa, S.; Carmeli, Y.; Schwaber, M.J. Israeli national policy for carbapenem-resistant enterobacteriaceae screening, carrier isolation and discontinuation of isolation. Infect. Control Hosp. Epidemiol. 2018, 39, 85–89. [Google Scholar] [CrossRef] [Green Version]
- Adler, A.; Solter, E.; Masarwa, S.; Miller-Roll, T.; Abu-Libdeh, B.; Khammash, H.; Najem, K.; Dekadek, S.; Stein-Zamir, C.; Nubani, N.; et al. Epidemiological and microbiological characteristics of an outbreak caused by OXA-48-producing Enterobacteriaceae in a neonatal intensive care unit in Jerusalem, Israel. J. Clin. Microbiol. 2013, 51, 2926–2930. [Google Scholar] [CrossRef] [Green Version]
- Ellington, M.J.; Kistler, J.; Livermore, D.M.; Woodford, N. Multiplex PCR for rapid detection of genes encoding acquired metallo-β-lactamases. J. Antimicrob. Chemother. 2007, 59, 321–322. [Google Scholar] [CrossRef] [Green Version]
- Schechner, V.; Straus-Robinson, K.; Schwartz, D.; Pfeffer, I.; Tarabeia, J.; Moskovich, R.; Chmelnitsky, I.; Schwaber, M.J.; Carmeli, Y.; Navon-Venezia, S. Evaluation of PCR-based testing for surveillance of KPC-producing carbapenem-resistant members of the Enterobacteriaceae family. J. Clin. Microbiol. 2009, 47, 3261–3265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyres, K.L.; Cahill, S.M.; Holt, K.E.; Hall, R.M.; Kenyon, J.J. Identification of acinetobacter baumannii loci for capsular polysaccharide (KL) and lipooligosaccharide outer core (OCL) synthesis in genome assemblies using curated reference databases compatible with kaptive. Microb. Genom. 2020, 6, e000339. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Tong, M.K.; Chow, K.H.; Cheng, V.C.C.; Tse, C.W.S.; Wu, A.K.L.; Lai, R.W.M.; Luk, W.K.; Tsang, D.N.C.; Ho, P.L. Occurrence of highly conjugative IncX3 epidemic plasmid carrying blaNDM in enterobacteriaceaeisolates in geographically widespread areas. Front. Microbiol. 2018, 9, 2272. [Google Scholar] [CrossRef] [PubMed]
- Bilal, H.; Zhang, G.; Rehman, T.; Han, J.; Khan, S.; Shafiq, M.; Yang, X.; Yan, Z.; Yang, X. First report of blandm-1 bearing incx3 plasmid in clinically isolated st11 klebsiella pneumoniae from pakistan. Microorganisms 2021, 9, 951. [Google Scholar] [CrossRef]
- Gijón, D.; Curiao, T.; Baquero, F.; Coque, T.M.; Cantóna, R. Fecal carriage of carbapenemase-producing Enterobacteriaceae: A hidden reservoir in hospitalized and nonhospitalized patients. J. Clin. Microbiol. 2012, 50, 1558–1563. [Google Scholar] [CrossRef] [Green Version]
- Trepanier, P.; Mallard, K.; Meunier, D.; Pike, R.; Brown, D.; Ashby, J.P.; Donaldson, H.; Awad-El-Kariem, F.M.; Balakrishnan, I.; Cubbon, M.; et al. Carbapenemase-producing Enterobacteriaceae in the UK: A national study (EuSCAPE-UK) on prevalence, incidence, laboratory detection methods and infection control measures. J. Antimicrob. Chemother. 2017, 72, 596–603. [Google Scholar] [CrossRef] [Green Version]
- Grundmann, H.; Glasner, C.; Albiger, B.; Aanensen, D.M.; Tomlinson, C.T.; Andrasević, A.T.; Cantón, R.; Carmeli, Y.; Friedrich, A.W.; Giske, C.G.; et al. Occurrence of carbapenemase-producing Klebsiella pneumoniae and Escherichia coli in the European survey of carbapenemase-producing Enterobacteriaceae (EuSCAPE): A prospective, multinational study. Lancet Infect. Dis. 2017, 17, 153–163. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Epidemiological timeline of Case Study 1: patient’s previous known carbapenemase-producing Enterobacteriales (CPE) acquisitions and screening history, plus CPE results from point prevalence study in August 2021. * CPE detection performed by NCIC laboratory. Abbreviations: Klebsiella pneumoniae carbapenemase (KPC), New Delhi metallo-beta-lactamase (NDM).
Figure 1.
Epidemiological timeline of Case Study 1: patient’s previous known carbapenemase-producing Enterobacteriales (CPE) acquisitions and screening history, plus CPE results from point prevalence study in August 2021. * CPE detection performed by NCIC laboratory. Abbreviations: Klebsiella pneumoniae carbapenemase (KPC), New Delhi metallo-beta-lactamase (NDM).

Figure 2.
Epidemiological timeline of Case Study 2: patient’s CPE acquisition and screening results from period of hospitalization. All CPE detection performed by NCIC laboratory.
Figure 2.
Epidemiological timeline of Case Study 2: patient’s CPE acquisition and screening results from period of hospitalization. All CPE detection performed by NCIC laboratory.

Figure 3.
Epidemiological timeline of Case Study 3: patients A–G’s admission to hospital ward, CPE acquisition, and screening results spanning 5-year period. * From day 0 (start of outbreak), all patients were screened for CPE on a weekly basis, until receipt of a positive sample.
Figure 3.
Epidemiological timeline of Case Study 3: patients A–G’s admission to hospital ward, CPE acquisition, and screening results spanning 5-year period. * From day 0 (start of outbreak), all patients were screened for CPE on a weekly basis, until receipt of a positive sample.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Summary of results for patient in Case Study 1—CPE positive bacteria, isolated in the point prevalence study performed by the National Centre for Infection Control (NCIC).
Table 1.
Summary of results for patient in Case Study 1—CPE positive bacteria, isolated in the point prevalence study performed by the National Centre for Infection Control (NCIC).
| Sample Type | Carbapenemase Detected | Bacterial Identification | ‘β-Carba Test’ | ST Type | KL Type | O Type |
|---|---|---|---|---|---|---|
| Rectal swab | blaNDM-1 | K. pneumoniae | Positive | 417 | 64 | O1/O2v1 |
| blaKPC-3 | K. pneumoniae | Positive | 512 | 107 | O1/O2v2 | |
| Skin culture | NDM | E. coli | Positive | Unknown | Unknown | Unknown |
| blaKPC-3 | K. pneumoniae | Positive | 512 | 107 | O1/O2v2 |
Table 2.
Summary of results of CPE-positive bacteria isolated during routine CPE screening in Case Study 2.
Table 2.
Summary of results of CPE-positive bacteria isolated during routine CPE screening in Case Study 2.
| Sample Type | Carbapenemase Detected | Bacterial Identification | ‘β-Carba Test’ | NG-Test CARBA 5 | ST Type (Pasteur) | Presence of IncX3 Plasmid |
|---|---|---|---|---|---|---|
| Surgical wound | blaNDM-1 | K. oxytoca | Positive | NDM | 202 | + |
| Tissue culture | blaKPC-2 | E. cloacae | Positive | KPC | 88 | − |
| Rectal swab | blaNDM-1 | E. cloacae | Positive | NDM | 145 | + |
Table 3.
Summary of results of CPE-positive bacteria isolated during CPE screening in Case Study 3.
| Patient | Date of Screen | Carbapenemase Detected | Bacterial Identification | ‘β-Carba Test’ | NDM Variant | Presence of IncX3 Plasmid |
|---|---|---|---|---|---|---|
| A | 4 April 2022 | NDM | K. pneumoniae | Positive | blaNDM-5 | − |
| 8 May 2022 | NDM | E. coli | Positive | blaNDM-7 | + | |
| NDM | K. pneumoniae | Positive | blaNDM-5 | - | ||
| B | 4 April 2022 | NDM | E. coli | Positive | blaNDM-7 | + |
| NDM | K. pneumoniae | Positive | blaNDM-5 | - | ||
| 8 May 2022 | NDM | E. coli | Positive | blaNDM-7 | + | |
| C | 10 April 2022 | NDM | E. coli | Positive | blaNDM-7 | + |
| D | 24 April 2022 | NDM | E. coli | Positive | blaNDM-7 | + |
| E | 24 April 2022 | NDM | E. coli | Positive | blaNDM-7 | + |
| NDM | K. aerogenes | Positive | blaNDM-7 | + | ||
| F | 1 May 2022 | NDM | E. coli | Positive | blaNDM-7 | + |
| G | 1 May 2022 | NDM | E. coli | Positive | blaNDM-7 | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Levi, G.; Lurie-Weinberger, M.; Keren-Paz, A.; Andremont, A.O.; Schwartz, D.; Carmeli, Y. Unraveling the Diversity of Co-Colonization by CPE. Microorganisms 2022, 10, 1292. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms10071292
AMA Style
Levi G, Lurie-Weinberger M, Keren-Paz A, Andremont AO, Schwartz D, Carmeli Y. Unraveling the Diversity of Co-Colonization by CPE. Microorganisms. 2022; 10(7):1292. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms10071292
Chicago/Turabian StyleLevi, Gabrielle, Mor Lurie-Weinberger, Alona Keren-Paz, Antoine O. Andremont, David Schwartz, and Yehuda Carmeli. 2022. "Unraveling the Diversity of Co-Colonization by CPE" Microorganisms 10, no. 7: 1292. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms10071292
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.