
Human Granulocytic Anaplasmosis—A Systematic Review of Published Cases

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
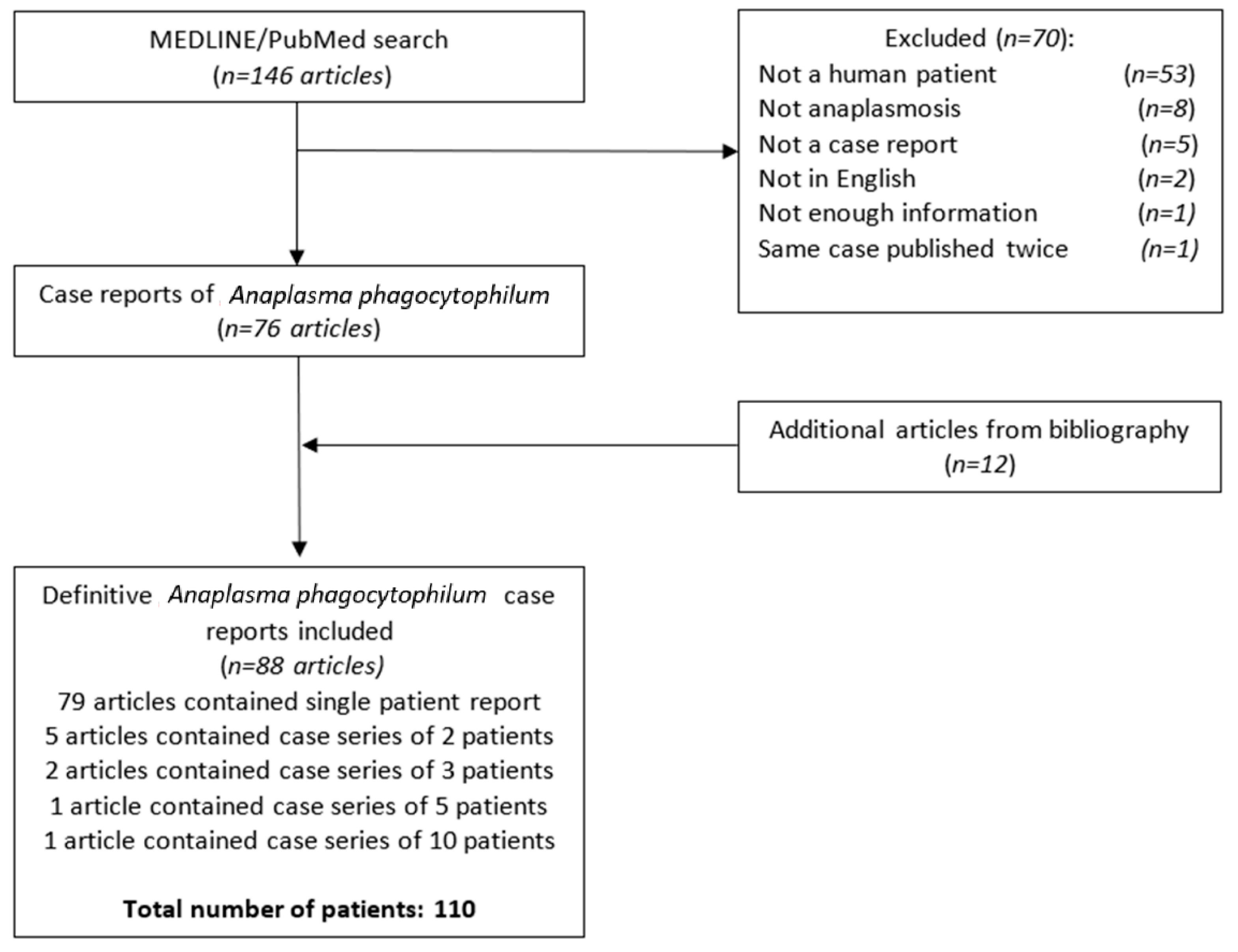
2. Materials and Methods
3. Results
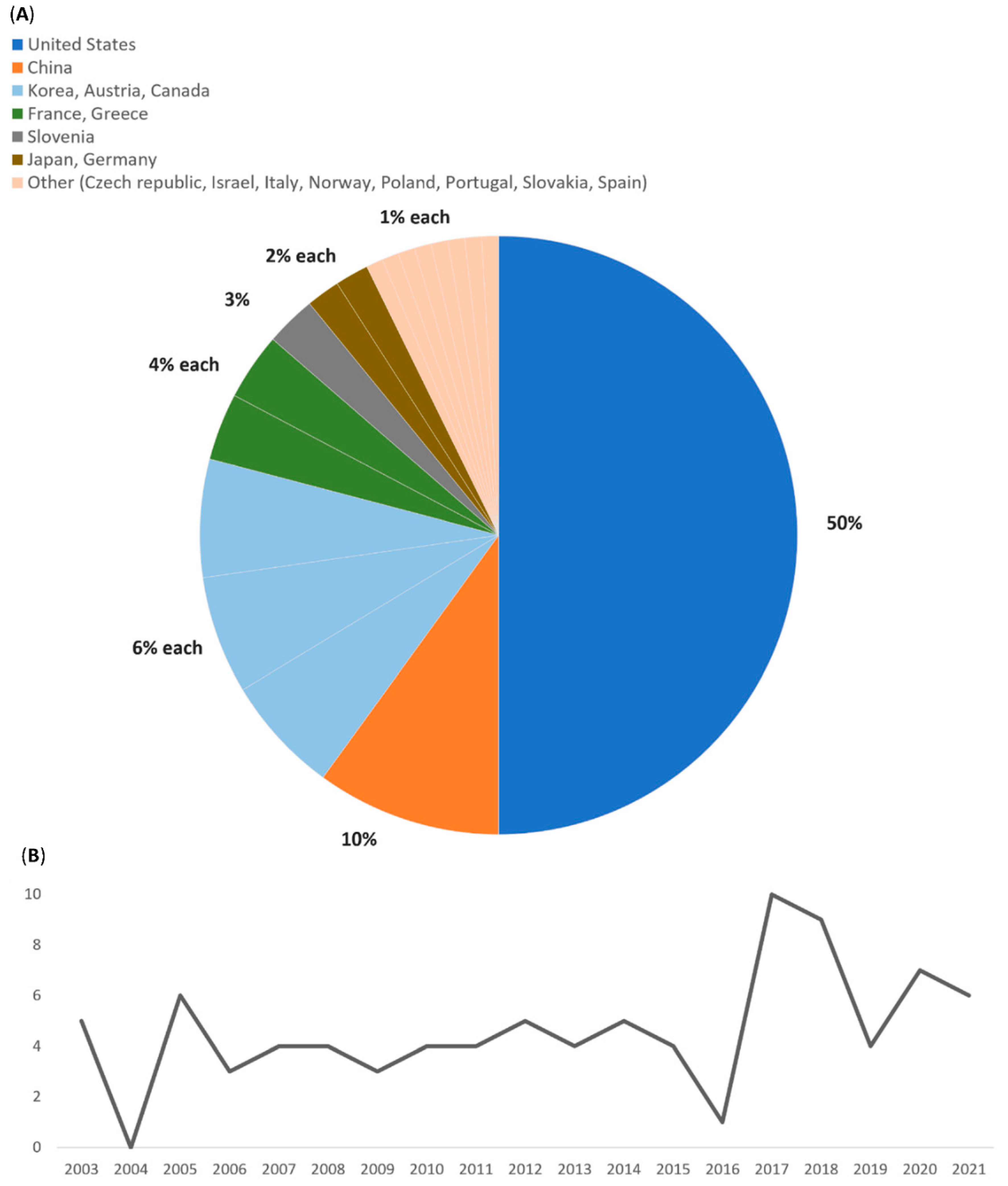
3.1. Demographic Characteristics
3.2. Exposure and Clinical Presentation
3.3. Investigations (Laboratory, Pathogen Identification)
3.4. Therapy
3.5. Outcome
4. Discussion
4.1. Epidemiology and Pathophysiology
4.2. Clinical Presentation
4.3. Coinfection
4.4. Diagnosis and Differential Diagnosis
4.5. Treatment and Outcome
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Chen, S.M.; Dumler, J.S.; Bakken, J.S.; Walker, D.H. Identification of a granulocytotropic Ehrlichia species as the etiologic agent of human disease. J. Clin. Microbiol. 1994, 32, 589–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakken, J.S.; Dumler, J.S.; Chen, S.M.; Eckman, M.R.; Van Etta, L.L.; Walker, D.H. Human granulocytic ehrlichiosis in the upper Midwest United States. A new species emerging? JAMA 1994, 272, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Dumler, J.S.; Choi, K.-S.; Garcia-Garcia, J.C.; Barat, N.S.; Scorpio, D.G.; Garyu, J.W.; Grab, D.J.; Bakken, J.S. Human granulocytic anaplasmosis and Anaplasma phagocytophilum. Emerg. Infect. Dis. 2005, 11, 1828–1834. [Google Scholar] [CrossRef] [PubMed]
- Dumler, J.S.; Barbet, A.F.; Bekker, C.P.J.; Dasch, G.A.; Palmer, G.H.; Ray, S.; Rikihisa, Y.; Rurangirwa, F.R. Reorganization of genera in the families Rickettsiaceae and Anaplasmataceae in the order Rickettsiales: Unification of some species of Ehrlichia with Anaplasma, Cowdria with Ehrlichia and Ehrlichia with Neorickettsia, descriptions of six new species combi. Int. J. Syst. Evol. Microbiol. 2001, 51 Pt 6, 2145–2165. [Google Scholar] [CrossRef] [Green Version]
- Bakken, J.S.; Dumler, J.S. Human granulocytic anaplasmosis. Infect. Dis. Clin. N. Am. 2015, 29, 341–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhand, A.; Nadelman, R.B.; Aguero-Rosenfeld, M.; Haddad, F.A.; Stokes, D.P.; Horowitz, H.W. Human granulocytic anaplasmosis during pregnancy: Case series and literature review. Clin. Infect. Dis. 2007, 45, 589–593. [Google Scholar] [CrossRef] [Green Version]
- Madison-Antenucci, S.; Kramer, L.D.; Gebhardt, L.L.; Kauffman, E. Emerging Tick-Borne Diseases. Clin. Microbiol. Rev. 2020, 33, e00083-18. [Google Scholar] [CrossRef]
- Ismail, N.; McBride, J.W. Tick-Borne Emerging Infections: Ehrlichiosis and Anaplasmosis. Clin. Lab. Med. 2017, 37, 317–340. [Google Scholar] [CrossRef]
- McFee, R.B. Tick borne illness—Anaplasmosis. Dis. Mon. 2018, 64, 181–184. [Google Scholar] [CrossRef]
- Sanchez, E.; Vannier, E.; Wormser, G.P.; Hu, L.T. Diagnosis, Treatment, and Prevention of Lyme Disease, Human Granulocytic Anaplasmosis, and Babesiosis: A Review. JAMA 2016, 315, 1767–1777. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Anaplasmosis. 2021. Available online: https://www.cdc.gov/anaplasmosis/index.html (accessed on 30 May 2022).
- Lagler, H.; Harrison, N.; Kussmann, M.; Obermüller, M.; Burgmann, H.; Makristathis, A.; Ramharter, M. Direct detection of Anaplasma phagocytophilum by polymerase chain reaction followed by electrospray ionization mass spectrometry from human blood. Int. J. Infect. Dis. 2017, 60, 61–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nováková, M.; Víchová, B.; Majláthová, V.; Lesňáková, A.; Pochybová, M.; Peťko, B. First case of human granulocytic anaplasmosis from Slovakia. Ann. Agric. Environ. Med. 2010, 17, 173–175. [Google Scholar] [PubMed]
- Sykes, D.B.; Zhang, E.W.; Karp Leaf, R.S.; Nardi, V.; Turbett, S.E. Case 10-2020: An 83-Year-Old Man with Pancytopenia and Acute Renal Failure. N. Engl. J. Med. 2020, 382, 1258–1266. [Google Scholar] [CrossRef]
- Fine, A.B.; Sweeney, J.D.; Nixon, C.P.; Knoll, B.M. Transfusion-transmitted anaplasmosis from a leukoreduced platelet pool. Transfusion 2016, 56, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Shields, K.; Cumming, M.; Rios, J.; Wong, M.T.; Zwicker, J.I.; Stramer, S.L.; Alonso, C.D. Transfusion-associated anaplasma phagocytophilum infection in a pregnant patient with thalassemia trait: A case report. Transfusion 2015, 55, 719–725. [Google Scholar] [CrossRef]
- Ohashi, N.; Gaowa Wuritu Kawamori, F.; Wu, D.; Yoshikawa, Y.; Chiya, S.; Fukunaga, K.; Funato, T.; Shiojiri, M.; Nakajima, H.; Hamauzu, Y.; et al. Human Granulocytic anaplasmosis, Japan. Emerg. Infect. Dis. 2013, 19, 289. [Google Scholar] [CrossRef]
- Koebel, C.; Kern, A.; Edouard, S.; Hoang, A.T.; Celestin, N.; Hansmann, Y.; Jaulhac, B.; Brouqui, P.; De Martino, S.J. Human granulocytic anaplasmosis in eastern France: Clinical presentation and laboratory diagnosis. Diagn. Microbiol. Infect. Dis. 2012, 72, 214–218. [Google Scholar] [CrossRef]
- Edginton, S.; Guan, T.H.; Evans, G.; Srivastava, S. Human granulocytic anaplasmosis acquired from a blacklegged tick in Ontario. CMAJ 2018, 190, E363–E366. [Google Scholar] [CrossRef] [Green Version]
- Ghera, P.; Kasirye, Y.; Choudhry, M.W.; Shaw, G.R.; Ejercito, V.S. Acute transient sensorineural hearing loss due to Anaplasma phagocytophilum. Wis. Med. J. 2011, 110, 288–290. [Google Scholar]
- Chochlakis, D.; Koliou, M.; Ioannou, I.; Tselentis, Y.; Psaroulaki, A. Kawasaki disease and Anaplasma sp. infection of an infant in Cyprus. Int. J. Infect. Dis. 2009, 13, 71–73. [Google Scholar] [CrossRef] [Green Version]
- Camacci, M.L.; Panganiban, R.P.; Pattison, Z.; Haghayeghi, K.; Daly, A.; Ojevwe, C.; Munyon, R.J. Severe Human Granulocytic anaplasmosis with Significantly Elevated Ferritin Levels in an Immunocompetent Host in Pennsylvania: A Case Report. J. Investig. Med. High Impact Case Rep. 2018, 6, 2324709618758350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markowicz, M.; Schötta, A.M.; Wijnveld, M.; Stanek, G. Human granulocytic anaplasmosis acquired in Connecticut, USA, diagnosed in Vienna, Austria, 2015. Diagn. Microbiol. Infect. Dis. 2016, 84, 347–349. [Google Scholar] [CrossRef] [PubMed]
- Tsiodras, S.; Spanakis, N.; Spanakos, G.; Pervanidou, D.; Georgakopoulou, T.; Campos, E.; Petra, T.; Kanellopoulos, P.; Georgiadis, G.; Antalis, E.; et al. Fatal human anaplasmosis associated with macrophage activation syndrome in Greece and the Public Health response. J. Infect. Public Health 2017, 10, 819–823. [Google Scholar] [CrossRef] [PubMed]
- Talsness, S.R.; Shukla, S.K.; Mazza, J.J.; Yale, S.H. Rhabdomyolysis-induced acute kidney injury secondary to Anaplasma phagocytophilum and concomitant statin use. Wis. Med. J. 2011, 110, 82–84. [Google Scholar]
- Epstein, R.; Ristau, J.; Ellner, J.J. An Unsuspected Zoonotic Infection Presenting as Sepsis. Am. J. Med. 2018, 131, e17–e18. [Google Scholar] [CrossRef]
- Moss, W.J.; Stephen Dumler, J. Simultaneous infection with Borrelia burgdorferi and human granulocytic ehrlichiosis. Pediatr. Infect. Dis. J. 2003, 22, 91–92. [Google Scholar] [CrossRef] [PubMed]
- Annen, K.; Friedman, K.; Eshoa, C.; Horowitz, M.; Gottschall, J.; Straus, T. Two cases of transfusion-transmitted Anaplasma phagocytophilum. Am. J. Clin. Pathol. 2012, 137, 562–565. [Google Scholar] [CrossRef] [Green Version]
- Heller, H.M.; Telford, S.R.; Branda, J.A. Case 10-2005: A 73-year-old man with weakness and pain in the legs. N. Engl. J. Med. 2005, 352, 1358–1364. [Google Scholar] [CrossRef]
- Wormser, G.P.; Filozov, A.; Telford, S.R., 3rd; Utpat, S.; Kamer, R.S.; Liveris, D.; Wang, G.; Zentmaier, L.; Schwartz, I.; Aguero-Rosenfeld, M.E. Dissociation between Inhibition and Killing by Levofloxacin in Human Granulocytic Anaplasmosis GARY. Vector-Borne Zoonotic Dis. 2006, 6, 388–394. [Google Scholar] [CrossRef]
- Parkins, M.D.; Church, D.L.; Xiu, Y.J.; Gregson, D.B. Human granulocytic anaplasmosis: First reported case in Canada. Can. J. Infect. Dis. Med. Microbiol. 2009, 20, 100–102. [Google Scholar] [CrossRef]
- Hoepler, W.; Markowicz, M.; Schoetta, A.M.; Zoufaly, A.; Stanek, G.; Wenisch, C. Molecular diagnosis of autochthonous human anaplasmosis in Austria—An infectious diseases case report. BMC Infect. Dis. 2020, 20, 288. [Google Scholar] [CrossRef] [PubMed]
- Marko, D.; Perry, A.M.; Ponnampalam, A.; Nasr, M.R. Cytopenias and clonal expansion of gamma/delta T-cells in a patient with anaplasmosis: A potential diagnostic pitfall. J. Clin. Exp Hematop. 2017, 56, 160–164. [Google Scholar] [CrossRef] [Green Version]
- Hsia, K.; Johnson, J.; Rice, D. Splenomegaly, Non-Traumatic Splenic Rupture, and Pancytopenia in Patient with Human Granulocytic Anaplasmosis. R. Isl. Med. J. 2021, 104, 60–62. [Google Scholar]
- Grant, L.; Mohamedy, I.; Loertscher, L. One man, three tick-borne illnesses. BMJ Case Rep. 2021, 14, e241004. [Google Scholar] [CrossRef] [PubMed]
- Kaphle, U.; Kheir, F.; Thammasitboon, S. A rare case of ARDS from human anaplasmosis. Respir. Care 2015, 60, e125–e127. [Google Scholar] [CrossRef] [Green Version]
- Goel, R.; Westblade, L.F.; Kessler, D.A.; Sfeir, M.; Slavinski, S.; Backenson, B.; Gebhardt, L.; Kane, K.; Laurence, J.; Scherr, D.; et al. Death from Transfusion-Transmitted Anaplasmosis, New York, USA, 2017. Emerg. Infect. Dis. 2018, 24, 1548–1550. [Google Scholar] [CrossRef]
- Halasz, C.L.G.; Niedt, G.W.; Kurtz, C.P.; Scorpio, D.G.; Bakken, J.S.; Dumler, J.S. A case of sweet syndrome associated with human granulocytic anaplasmosis. Arch. Dermatol. 2005, 141, 887–889. [Google Scholar] [CrossRef] [Green Version]
- Eldaour, Y.; Hariri, R.; Yassin, M. Severe Anaplasmosis presenting as possible CVA: Case report and 3-year Anaplasma infection diagnosis data is based on PCR testing and serology. IDCases 2021, 24, e01073. [Google Scholar] [CrossRef]
- Walder, G.; Falkensammer, B.; Aigner, J.; Tiwald, G.; Dierich, M.P.; Würzner, R.; Lechleitner, P. First documented case of human granulocytic ehrlichiosis in Austria. Wien. Klin. Wochenschr. 2003, 115, 263–266. [Google Scholar] [CrossRef]
- Bayard-Mc Neeley, M.; Bansal, A.; Chowdhury, I.; Girao, G.; Small, C.B.; Seiter, K.; Nelson, J.; Liveris, D.; Schwartz, I.; Mc Neeley, D.F.; et al. In vivo and in vitro studies on Anaplasma phagocytophilum infection of the myeloid cells of a patient with chronic myelogenous leukaemia and human granulocytic ehrlichiosis. J. Clin. Pathol. 2004, 57, 499–503. [Google Scholar] [CrossRef]
- Alhumaidan, H.; Westley, B.; Esteva, C.; Berardi, V.; Young, C.; Sweeney, J. Transfusion-transmitted anaplasmosis from leukoreduced red blood cells. Transfusion 2013, 53, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Jereb, M.; Pecaver, B.; Tomazic, J.; Muzlovic, I.; Avsic-Zupanc, T.; Premru-Srsen, T.; Levicnik-Stezinar, S.; Karner, P.; Strle, F. Severe human granulocytic anaplasmosis transmitted by blood transfusion. Emerg. Infect. Dis. 2012, 18, 1354–1357. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Uslan, D.Z.; Baddour, L.M. 70-Year-old man with fever, shaking chills, and weakness. Mayo Clin. Proc. 2005, 80, 1209–1212. [Google Scholar] [CrossRef] [Green Version]
- Tsibris, A.M.N.; Shepard, J.A.O.; Zukerberg, L.R. Case 6-2011: A 77-year-old man with dyspnea, weakness, and diaphoresis. N. Engl. J. Med. 2011, 364, 759–767. [Google Scholar] [CrossRef] [PubMed]
- Picco, P.; Naselli, A.; Pala, G.; Rizzo, F.; Damasio, B.; Buoncompagni, A.; Martini, A. Whole-body MRI as an unconventional diagnostic tool in a pediatric patient with systemic infection. Acta Radiol. Short Rep. 2014, 3, 204798161454957. [Google Scholar] [CrossRef] [PubMed]
- de la Fuente, J.; Torina, A.; Naranjo, V.; Caracappa, S.; Di Marco, V.; Alongi, A.; Russo, M.; Maggio, A.R.; Kocan, K.M. Infection with Anaplasma phagocytophilum in a seronegative patient in Sicily, Italy: Case report. Ann. Clin. Microbiol. Antimicrob. 2005, 4, 3–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krause, P.J.; Corrow, C.L.; Bakken, J.S. Successful treatment of human granulocytic ehrlichiosis in children using rifampin. Pediatrics 2003, 112, e252–e253. [Google Scholar] [CrossRef] [Green Version]
- George, S.; Sandal, S. A ticking time bomb. N. Engl. J. Med. 2013, 368, 1826. [Google Scholar] [CrossRef] [Green Version]
- Jawanda, J. Rare case of severe rhabdomyolysis secondary to human Granulocytic anaplasmosis. Am. J. Emerg. Med. 2020, 38, 1543.e1–1543.e2. [Google Scholar] [CrossRef]
- Anaplasma phagocytophilum Transmitted Through Blood Transfusion—Minnesota 2007. Ann. Emerg. Med. 2009, 53, 643–645. [CrossRef]
- Pozdnyakova, O.; Dorfman, D.M. Human granulocytic anaplasmosis. Blood 2012, 120, 4911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.H.; Yi, J.; Oh, W.S.; Kim, N.H.; Choi, S.J.; Choe, P.G.; Kim, N.J.; Lee, J.K.; Oh, M.D. Human Granulocytic Anaplasmosis, South Korea, 2013. Emerg. Infect. Dis. 2014, 20, 1708–1711. [Google Scholar] [CrossRef]
- Remy, V.; Hansmann, Y.; De Martino, S.; Christmann, D.; Brouqui, P. Human anaplasmosis presenting as atypical pneumonitis in France. Clin. Infect. Dis. 2003, 37, 846–848. [Google Scholar] [CrossRef]
- Townsend, R.L.; Moritz, E.D.; Fialkow, L.B.; Berardi, V.; Stramer, S.L. Probable transfusion-transmission of Anaplasma phagocytophilum by leukoreduced platelets. Transfusion 2014, 54, 2828–2832. [Google Scholar] [CrossRef] [PubMed]
- El Khoury, L.; Furie, R. Inflammatory arthritis: A unique presentation of human anaplasmosis. Clin. Rheumatol. 2019, 38, 257–259. [Google Scholar] [CrossRef] [PubMed]
- Hagedorn, P.; Imhoff, M.; Fischer, C.; Domingo, C.; Niedrig, M. Human granulocytic anaplasmosis acquired in Scotland, 2013. Emerg. Infect. Dis. 2014, 20, 1079–1081. [Google Scholar] [CrossRef]
- García, J.C.; Núñez, M.J.; Castro, B.; Fraile, F.J.; López, A.; Mella, M.C.; Blanco, A.; Sieira, C.; Loureiro, E.; Portillo, A.; et al. Human anaplasmosis: The first Spanish case confirmed by PCR. Ann. N. Y. Acad. Sci. 2006, 1078, 545–547. [Google Scholar] [CrossRef]
- Haschke-Becher, E.; Bernauer, R.; Walleczek, A.M.; Apfalter, P.; Afazel-Saeedi, S.; Kraus, J.; Ladurner, G.; Strasser, P. First detection of the Anaplasma phagocytophilum groEL-A genotype in man. J. Infect. 2010, 60, 300–305. [Google Scholar] [CrossRef]
- Psaroulaki, A.; Koliou, M.; Chochlakis, D.; Ioannou, I.; Mazeri, S.; Tselentis, Y. Anaplasma phacotytophilum infection in a child. Pediatr. Infect. Dis. J. 2008, 27, 664–666. [Google Scholar] [CrossRef]
- Lotric-Furlan, S.; Ruzic-Sabljic, E.; Strle, F. Concomitant human granulocytic anaplasmosis and Lyme neuroborreliosis. Clin. Microbiol. Infect. 2009, 15, 28–29. [Google Scholar] [CrossRef] [Green Version]
- Loebermann, M.; Fingerle, V.; Lademann, M.; Fritzsche, C.; Reisinger, E.C. Borrelia burgdorferi and Anaplasma phagocytophilum coinfection. Emerg. Infect. Dis. 2006, 12, 353–355. [Google Scholar] [CrossRef] [PubMed]
- Khatri, A.; Lloji, A.; Doobay, R.; Wang, G.; Knoll, B.; Dhand, A.; Nog, R. Anaplasma phagocytophilum presenting with orchitis in a renal transplant recipient. Transpl. Infect. Dis. 2019, 21, e13129. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Khankhanian, P.; Salama, C.; Brown, M.; Lieber, J. Pseudo-Pelger–Huët anomaly and granulocytic dysplasia associated with human Granulocytic anaplasmosis. Int. J. Hematol. 2015, 102, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Welc-Falęciak, R.; Kowalec, M.; Zajkowska, J.; Pancewicz, S.A.; Siński, E. Clinical and molecular features of one case of human infection with Anaplasma phagocytophilum from Podlaskie province in eastern Poland. Ann. Agric. Environ. Med. 2015, 22, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, M.; Calev, H.; Saunders, S.J.; Li, J.; Stillman, I.E.; Danziger, J. Acute Kidney Injury Associated With Human Granulocytic Anaplasmosis: A Case Report. Am. J. Kidney Dis. 2019, 74, 696–699. [Google Scholar] [CrossRef]
- Yoo, J.; Chung, J.H.; Kim, C.M.; Yun, N.R.; Kim, D.M. Asymptomatic-anaplasmosis confirmation using genetic and serological tests and possible coinfection with spotted fever group Rickettsia: A case report. BMC Infect. Dis. 2020, 20, 458. [Google Scholar] [CrossRef]
- Gaowa; Wulantuya; Yin, X.; Cao, M.; Guo, S.; Ding, C.; Lu, Y.; Luo, J.; Kawabata, H.; Ando, S.; et al. Case of human infection with Anaplasma phagocytophilum in inner Mongolia, China. Jpn. J. Infect. Dis. 2018, 71, 155–157. [Google Scholar] [CrossRef] [Green Version]
- Vikse, J.; Klos, J.; Berg, A. A travelling camper with a spiking fever, headache, myalgia, hepatitis, and intracellular inclusions. Lancet Infect. Dis. 2017, 17, 1318. [Google Scholar] [CrossRef]
- Varshney, A.; Barkoudah, E. The Simplest Explanation: Pancytopenia. Am. J. Med. 2018, 131, 1052–1054. [Google Scholar] [CrossRef]
- Uminski, K.; Kadkhoda, K.; Houston, B.L.; Lopez, A.; MacKenzie, L.J.; Lindsay, R.; Walkty, A.; Embil, J.; Zarychanski, R. Anaplasmosis: An emerging tick-borne disease of importance in Canada. IDCases 2018, 14, e00472. [Google Scholar] [CrossRef]
- Stokes, W.; Lisboa, L.F.; Lindsay, L.R.; Fonseca, K. Case report: Anaplasmosis in Canada: Locally acquired Anaplasma phagocytophilum infection in Alberta. Am. J. Trop. Med. Hyg. 2020, 103, 2478–2480. [Google Scholar] [CrossRef] [PubMed]
- Stice, M.J.; Bruen, C.A.; Grall, K.J.H. Anchoring on COVID-19: A case report of human granulocytic anaplasmosis masquerading as COVID-19. Clin. Pract. Cases Emerg. Med. 2021, 5, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Sigurjonsdottir, V.K.; Feder, H.M.; Wormser, G.P. Anaplasmosis in pediatric patients: Case report and review. Diagn. Microbiol. Infect. Dis. 2017, 89, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Shin, K.S.; Son, B.R.; Kim, D.M.; Kim, H.S.; Jeong, H.W. Human granulocytic anaplasmosis diagnosed based on a peripheral blood smear test in South Korea: A case report. Jpn. J. Infect. Dis. 2020, 73, 469–472. [Google Scholar] [CrossRef]
- Lotric-Furlan, S.; Petrovec, M.; Avsic-Zupanc, T.; Strle, F. Concomitant tickborne encephalitis and human granulocytic ehrlichiosis. Emerg. Infect. Dis. 2005, 11, 485–488. [Google Scholar] [CrossRef]
- Lee, S.H.; Shin, N.-R.; Kim, C.-M.; Park, S.; Yun, N.R.; Kim, D.-M.; Jung, D.S. First identification of Anaplasma phagocytophilum in both a biting tick Ixodes nipponensis and a patient in Korea: A case report. BMC Infect. Dis. 2020, 20, 826. [Google Scholar] [CrossRef]
- Lee, S.H.; Park, S.Y.; Jang, M.J.; Choi, K.J.; Lee, H.K.; Cho, Y.U.; Lee, Y.S.; Kim, S.H.; Hwang, S.D. Case Report: Clinical Isolation of Anaplasma phagocytophilum in South Korea. Am. J. Trop. Med. Hyg. 2017, 97, 1686–1690. [Google Scholar] [CrossRef] [Green Version]
- Ladzinski, A.T.; Baker, M.; Dunning, K.; Patel, P.P. Human Granulocytic Anaplasmosis presenting as Subacute Abdominal Pain and Hyponatremia. IDCases 2021, 25, e01183. [Google Scholar] [CrossRef]
- Kobayashi, K.J.; Weil, A.A.; Branda, J.A. Case 16-2018: A 45-Year-Old Man with Fever, Thrombocytopenia, and Elevated Aminotransferase Levels. N. Engl. J. Med. 2018, 378, 2023–2029. [Google Scholar] [CrossRef]
- Kim, S.W.; Kim, C.M.; Kim, D.M.; Yun, N.R. Manifestation of anaplasmosis as cerebral infarction: A case report. BMC Infect. Dis. 2018, 18, 409. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.-M.; Yoon, N.-R.; Lee, S.H.; Jha, P.; Kim, S.W.; Kim, D.-M.; Lee, Y.S.; Hwang, S.D.; Jang, S.J.; Ahn, Y.-J.; et al. Case report: Polymerase chain reaction testing of tick bite site samples for the diagnosis of human granulocytic anaplasmosis. Am. J. Trop. Med. Hyg. 2017, 97, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Khera, K.D.; Southerland, D.M.; Miller, N.E.; Garrison, G.M. A Case of Anaplasmosis during a Warm Minnesota Fall. J. Prim. Care Community Health 2021, 12, 21501327211005895. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.; de Sousa, R.; Alves, F.; Proença, P.; Núncio, M.; Dumler, J.; Bacellar, F. Isolation of Coxiella burnetii from the blood of a patient with positive Anaplasma phagocytophilum serological results. Clin. Microbiol. Infect. 2009, 15, 192–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, M.; Sharma, A.; Grover, P. Triple Tick Attack. Cureus 2019, 11, 3–7. [Google Scholar] [CrossRef] [Green Version]
- Young, N.P.; Klein, C.J. Encephalopathy with seizures having PCR-positive Anaplasma phagocytophilum and Ehrlichia chaffeensis. Eur. J. Neurol. 2007, 14, 2006–2007. [Google Scholar] [CrossRef]
- Chochlakis, D.; Ioannou, I.; Tselentis, Y.; Psaroulaki, A. Human Anaplasmosís and Anaplasma ovis Variant. Emerg. Infect. Dis. 2010, 16, 1031–1033. [Google Scholar] [CrossRef]
- Boateng, F.; Ohene-Adjei, R.; Amoateng-Adjepong, Y. Rhabdomyolysis and acute renal failure associated with human granulocytic amaplasmosis. Mayo Clin. Proc. 2007, 82, 250. [Google Scholar] [CrossRef] [Green Version]
- Qasba, N.; Shamshirsaz, A.A.; Feder, H.M.; Campbell, W.A.; Egan, J.F.; Shamshirsaz, A.A. A case report of human Granulocytic anaplasmosis (Ehrlichiosis) in pregnancy and a literature review of tick-borne diseases in the United States during pregnancy. Obstet. Gynecol. Surv. 2011, 66, 788–796. [Google Scholar] [CrossRef]
- Johnson, T.; Brown, M.; Rabbat, M.; Slim, J. Hemophagocytic Lymphohistiocytosis Associated with Anaplasmosis. J. Glob. Infect. Dis. 2017, 9, 76–78. [Google Scholar] [CrossRef]
- Malik, A.; Jameel, M.N.Q.; Ali, S.S.; Mir, S. Human granulocytic anaplasmosis affecting the myocardium. J. Gen. Intern. Med. 2005, 20, 958. [Google Scholar] [CrossRef]
- Joshi, M.; Suresh, S.; Shaikh, I.A.; Rana, Z.; Scholand, S.J. Tick-Borne Trauma: An Unusual Presentation of Anaplasmosis. Conneticut Med. 2013, 77, 417–420. [Google Scholar]
- Vogl, U.M.; Presterl, E.; Stanek, G.; Ramharter, M.; Gattringer, K.B.; Graninger, W. First described case of human granulocytic anaplasmosis in a patient in Eastern Austria. Wien. Med. Wochenschr. 2010, 160, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Herbst, J.; Crissinger, T.; Baldwin, K. Diffuse Ischemic Strokes and Sickle Cell Crisis Induced by Disseminated Anaplasmosis: A Case Report. Case Rep. Neurol. 2019, 11, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Nitzan, O.; Baneth, G.; Blum, A.; Tzadok, B.-S.; Marva, E.; Peretz, A.; Nachum-Biala, Y.; Katz, A. Case report: Infectious diseases in pilgrims visiting the holy land. Am. J. Trop. Med. Hyg. 2017, 97, 611–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanicek, J.; Stastnik, M.; Kianicka, B.; Bares, M.; Bulik, M. Rare neurological presentation of human granulocytic anaplasmosis. Eur. J. Neurol. 2013, 20, e70–e72. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Liu, Y.; Ni, D.; Li, Q.; Yu, Y.; Yu, X.J.; Wan, K.; Li, D.; Liang, G.; Jiang, X.; et al. Nosocomial transmission of human granulocytic anaplasmosis in China. JAMA 2008, 300, 2263–2270. [Google Scholar] [CrossRef]
- Assi, M.A.; Yao, J.D.C.; Walker, R.C. Lyme disease followed by human granulocytic anaplasmosis in a kidney transplant recipient. Transpl. Infect. Dis. 2007, 9, 66–72. [Google Scholar] [CrossRef]
- Dumic, I.; Severnini, E. “Ticking Bomb”: The Impact of Climate Change on the Incidence of Lyme Disease. Can. J. Infect. Dis. Med. Microbiol. 2018, 2018, 5719081. [Google Scholar] [CrossRef] [Green Version]
- Guzman, N.; Yarrarapu, S.N.S.; Beidas, S.O. Anaplasma Phagocytophilum. 2021. Available online: https://europepmc.org/article/NBK/nbk513341 (accessed on 1 May 2020).
- Camprubí-Ferrer, D.; Portillo, A.; Santibáñez, S.; Almuedo-Riera, A.; Rodriguez-Valero, N.; Subirà, C.; Martinez, M.J.; Navero-Castillejos, J.; Fernandez-Pardos, M.; Genton, B.; et al. Incidence of human granulocytic anaplasmosis in returning travellers with fever. J. Travel Med. 2021, 28, taab056. [Google Scholar] [CrossRef]
- Horowitz, H.W.; Kilchevsky, E.; Haber, S.; Aguero-Rosenfeld, M.; Kranwinkel, R.; James, E.K.; Wong, S.J.; Chu, F.; Liveris, D.; Schwartz, I. Perinatal transmission of the agent of human granulocytic ehrlichiosis. N. Engl. J. Med. 1998, 339, 375–378. [Google Scholar] [CrossRef]
- Bakken, J.S.; Krueth, J.K.; Lund, T.; Malkovitch, D.; Asanovich, K.; Dumler, J.S. Exposure to deer blood may be a cause of human granulocytic ehrlichiosis. Clin. Infect. Dis. 1996, 23, 198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mowla, S.J.; Drexler, N.A.; Cherry, C.C.; Annambholta, P.D.; Kracalik, I.T.; Basavaraju, S.V. Ehrlichiosis and Anaplasmosis among Transfusion and Transplant Recipients in the United States. Emerg. Infect. Dis. 2021, 27, 2768. [Google Scholar] [CrossRef] [PubMed]
- Dumler, J.S. The biological basis of severe outcomes in Anaplasma phagocytophilum infection. FEMS Immunol. Med. Microbiol. 2012, 64, 13–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matei, I.A.; Estrada-Peña, A.; Cutler, S.J.; Vayssier-Taussat, M.; Varela-Castro, L.; Potkonjak, A.; Zeller, H.; Mihalca, A.D. A review on the eco-epidemiology and clinical management of human granulocytic anaplasmosis and its agent in Europe. Parasites Vectors 2019, 12, 599. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Zheng, Y.-C.; Ma, L.; Jia, N.; Jiang, B.-G.; Jiang, R.-R.; Huo, Q.-B.; Wang, Y.-W.; Liu, H.-B.; Chu, Y.-L.; et al. Human infection with a novel tick-borne Anaplasma species in China: A surveillance study. Lancet Infect. Dis. 2015, 15, 663–670. [Google Scholar] [CrossRef]
- Moniuszko-Malinowska, A.; Dunaj, J.; Andersson, M.O.; Czupryna, P.; Zajkowska, J.; Guziejko, K.; Garkowski, A.; Grygorczuk, S.; Kondrusik, M.; Pancewicz, S. Assessment of Anaplasma phagocytophilum presence in early Lyme borreliosis manifested by erythema migrans skin lesions. Travel Med. Infect. Dis. 2020, 36, 101648. [Google Scholar] [CrossRef]
- Egenvall, A.; Lilliehöök, I.; Bjöersdorff, A.; Engvall, E.O.; Karlstam, E.; Artursson, K.; Heldtander, M.; Gunnarsson, A. Detection of granulocytic Ehrlichia species DNA by PCR in persistently infected dogs. Vet. Rec. 2000, 146, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Franzén, P.; Aspan, A.; Egenvall, A.; Gunnarsson, A.; Karlstam, E.; Pringle, J. Molecular evidence for persistence of Anaplasma phagocytophilum in the absence of clinical abnormalities in horses after recovery from acute experimental infection. J. Vet. Intern. Med. 2009, 23, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.J.; Birtles, R.J.; Radford, A.D.; Woldehiwet, Z. Recurrent bacteraemia in sheep infected persistently with Anaplasma phagocytophilum. J. Comp. Pathol. 2012, 147, 360–367. [Google Scholar] [CrossRef]
- Nelder, M.P.; Russell, C.B.; Sheehan, N.J.; Sander, B.; Moore, S.; Li, Y.; Johnson, S.; Patel, S.N.; Sider, D. Human pathogens associated with the blacklegged tick Ixodes scapularis: A systematic review. Parasit Vectors 2016, 9, 265. [Google Scholar] [CrossRef] [Green Version]
- Eisen, L. Pathogen transmission in relation to duration of attachment by Ixodes scapularis ticks. Ticks Tick Borne Dis. 2018, 9, 535–542. [Google Scholar] [CrossRef]
- Lehane, A.; Maes, S.E.; Graham, C.B.; Jones, E.; Delorey, M.; Eisen, R.J. Prevalence of single and coinfections of human pathogens in Ixodes ticks from five geographical regions in the United States, 2013–2019. Ticks Tick Borne Dis. 2021, 12, 101637. [Google Scholar] [CrossRef] [PubMed]
- Ben, I.; Lozynskyi, I. Prevalence of Anaplasma phagocytophilum in Ixodes ricinus and Dermacentor reticulatus and Coinfection with Borrelia burgdorferi and Tick-Borne Encephalitis Virus in Western Ukraine. Vector Borne Zoonotic Dis. 2019, 19, 793–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kjelland, V.; Paulsen, K.M.; Rollum, R.; Jenkins, A.; Stuen, S.; Soleng, A.; Edgar, K.S.; Lindstedt, H.H.; Vaino, K.; Gibory, M.; et al. Tick-borne encephalitis virus, Borrelia burgdorferi sensu lato, Borrelia miyamotoi, Anaplasma phagocytophilum and Candidatus Neoehrlichia mikurensis in Ixodes ricinus ticks collected from recreational islands in southern Norway. Ticks Tick Borne Dis. 2018, 9, 1098–1102. Available online: https://pubmed.ncbi.nlm.nih.gov/29678403/ (accessed on 6 February 2022).
- Horowitz, H.W.; Aguero-Rosenfeld, M.E.; Holmgren, D.; McKenna, D.; Schwartz, I.; Cox, M.E.; Wormser, G.P. Lyme Disease and Human Granulocytic Anaplasmosis Coinfection: Impact of Case Definition on Coinfection Rates and Illness Severity. Clin. Infect. Dis. 2013, 56, 93–99. [Google Scholar] [CrossRef]
- Belongia, E.; Reed, K.D.; Mitchell, P.D.; Chyou, P.-H.; Mueller-Rizner, N.; Finkel, M.F.; Schriefer, M.E. Clinical and epidemiological features of early Lyme disease and human granulocytic ehrlichiosis in Wisconsin. Clin. Infect. Dis. 1999, 29, 1472–1477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botelho-Nevers, E.; Socolovschi, C.; Raoult, D.; Parola, P. Treatment of Rickettsia spp. infections: A review. Expert Rev. Anti-Infect. Ther. 2012, 10, 1425–1437. [Google Scholar]
- Vannier, E.G.; Diuk-Wasser, M.A.; Ben Mamoun, C.; Krause, P.J. Babesiosis. Infect. Dis. Clin. N. Am. 2015, 29, 357. [Google Scholar] [CrossRef] [Green Version]
- Woldehiwet, Z. Immune evasion and immunosuppression by Anaplasma phagocytophilum, the causative agent of tick-borne fever of ruminants and human granulocytic anaplasmosis. Vet. J. 2008, 175, 37–44. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Comorbid Conditions of Immunocompetent Patients | Number of Patients (%) | Cause for Immunosuppression in Immunocompromised Patients | Number of Patients (%) |
|---|---|---|---|
| Hypertension | 9 (8.2) | Steroid use; DM | 5 (4.5) |
| Hypothyroidism; CAD | 6 (5.5) | CKD | 4 (3.6) |
| Joint disease | 5 (4.5) | Hematologic malignancies; Cytotoxic medication | 3 (2.7) |
| Smoking; HLP; Malignancy | 4 (3.6) | Asplenia | 1 (0.9) |
| BPH; COPD; Inherited hematologic abnormality | 3 (2.7) | ||
| Hematologic malignancy in remission; HF; Ischemic cardiomyopathy | 2 (1.8) | ||
| Other less common comorbidities (hydrocephalus, kidney transplant, A-fib, gynecomastia, depression, Chrons disease, valve replacement, aortic aneurysm, sleep apnea, ureter stones, diverticulosis, colectomy, gunshot wound, SVT, fungal sinusitis, gastritis, hip fracture, fibromyalgia, TIA, embolic stroke, carpal-tunnel syndrome, rhabdomyolysis, Stevens–Johnson syndrome, asthma) | 1 (0.9) | ||
| Symptom | Number of Cases (%) | |
|---|---|---|
| Fever | 99 (90) | |
| Constitutional symptoms | 65 (59.1) | |
| GI symptoms | Diarrhea | 20 (18.2) |
| Nausea | 16 (14.5) | |
| Abdominal pain | 10 (9.1) | |
| Anorexia | 8 (7.3) | |
| Emesis | 7 (6.4) | |
| Myalgia | 46 (41.8) | |
| Headache | 41 (37.3) | |
| Chills | 35 (31.8) | |
| Arthralgia | 25 (22.7) | |
| Rash | 19 (17.3) | |
| AKI | 17 (15.5) | |
| Cough | 10 (9.1) | |
| Splenic complications | Splenomegaly | 10 (9.1) |
| Splenic rupture | 1 (0.9) | |
| Splenic infarct | 1 (0.9) | |
| Confusion | 9 (8.2) | |
| Diaphoresis | 8 (7.3) | |
| SOB/Respiratory distress | 7 (6.4) | |
| Dizziness | 3 (2.7) | |
| Rigor | 2 (1.8) | |
| Parameter | Mean (SD) | Parameter | Number of Patients (%) | |
|---|---|---|---|---|
| Hb ** (g/dL) | 12.7 (1.8) | Anemia (<12 g/dL in women, <13 g/dL in men) | 33 (30) | |
| Platelets ** (×10 (9)/L) | 72 (6.6) | Thrombocytopenia (<150 × 10 (9)/L) | 79 (71.8) | |
| WBC ** (×10 (9)/L) | 4.8 (0.5) | Leukopenia (<4 × 10 (9)/L) | 51 (46.4) | |
| BUN * (mg/dL) | 50.1 (8.3) | |||
| Creatinine * (mg/dL) | 3.3 (0.4) | |||
| Bilirubin * (mg/dL) | 2.3 (0.5) | |||
| AST * (U/L) | 162.6 (19.7) | LFT abnormalities | AST (>40 U/L) | 63 (57.3) |
| ALT * (U/L) | 107.5 (11.1) | ALT (>50 U/L) | 53 (48.2) | |
| ALP * (U/L) | 148.4 (23.3) | ALP (>150 U/L) | 7 (6.4) | |
| Na ** (mmoL/L) | 132.4 (3.1) | |||
| LDH * (U/L) | 911.8 (198.5) | |||
| CRP * (mg/dL) | 148.1 (14.2) | Inflammation | ESR (>29 mm/h in women, >22 mm/h in men) | 13 (11.8) |
| ESR * (mm/hr) | 52.1 (7.4) | CRP (>10 mg/L) | 37 (33.6) | |
| Ferritin * (ng/mL) | 12,076 (6820) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dumic, I.; Jevtic, D.; Veselinovic, M.; Nordstrom, C.W.; Jovanovic, M.; Mogulla, V.; Veselinovic, E.M.; Hudson, A.; Simeunovic, G.; Petcu, E.; et al. Human Granulocytic Anaplasmosis—A Systematic Review of Published Cases. Microorganisms 2022, 10, 1433. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms10071433
Dumic I, Jevtic D, Veselinovic M, Nordstrom CW, Jovanovic M, Mogulla V, Veselinovic EM, Hudson A, Simeunovic G, Petcu E, et al. Human Granulocytic Anaplasmosis—A Systematic Review of Published Cases. Microorganisms. 2022; 10(7):1433. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms10071433
Chicago/Turabian StyleDumic, Igor, Dorde Jevtic, Mladjen Veselinovic, Charles W. Nordstrom, Milan Jovanovic, Vanajakshi Mogulla, Elmira Mofid Veselinovic, Ann Hudson, Gordana Simeunovic, Emilia Petcu, and et al. 2022. "Human Granulocytic Anaplasmosis—A Systematic Review of Published Cases" Microorganisms 10, no. 7: 1433. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms10071433