Classical Microbiological Diagnostics of Bacteremia: Are the Negative Results Really Negative? What is the Laboratory Result Telling Us About the “Gold Standard”?

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Samples
2.3. Blood Purification, Pellets Separation, and Direct Smear Preparation
2.4. Gram Staining
2.5. Fluorescence in-situ Hybridization (FISH).
2.6. Statistical Analysis
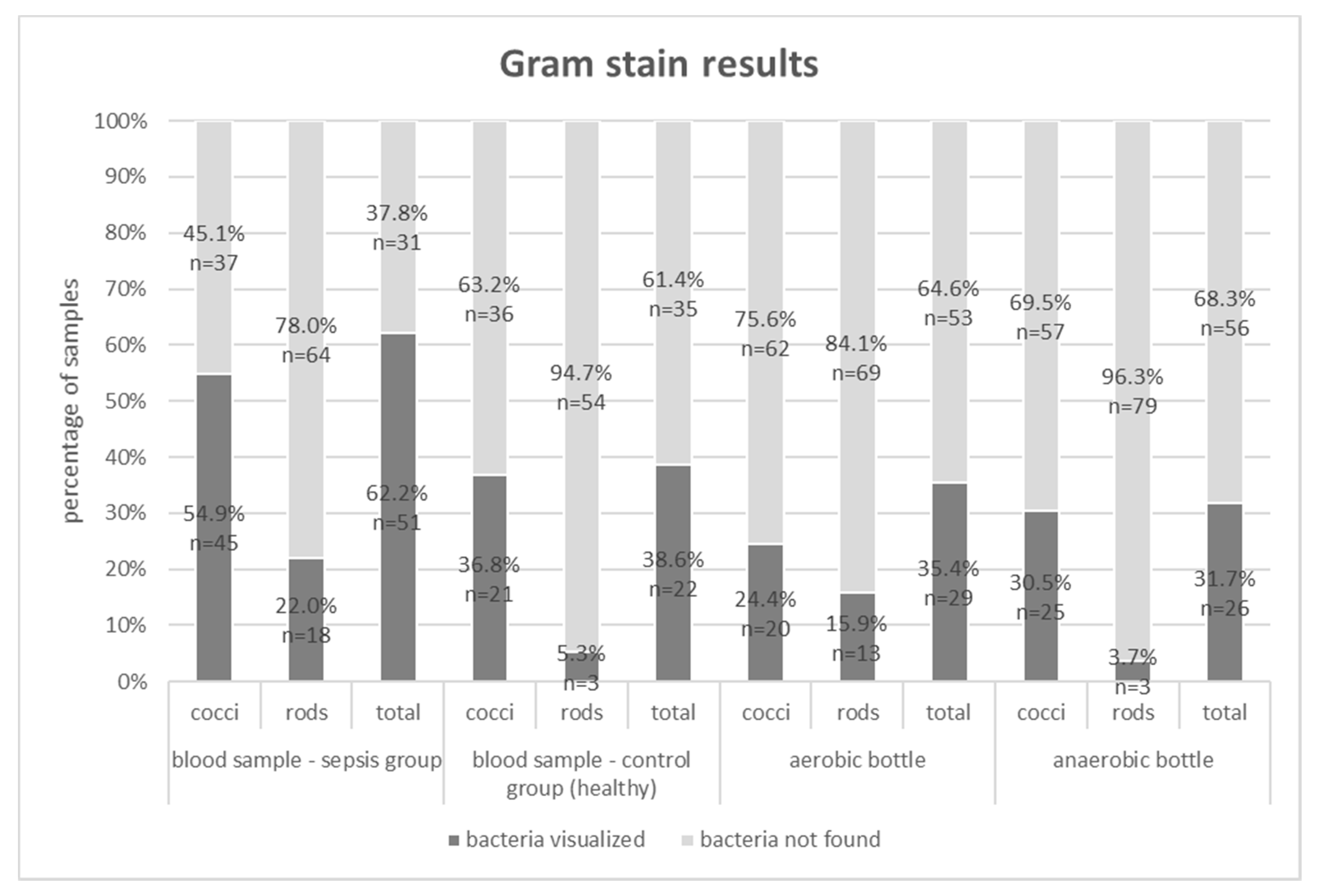
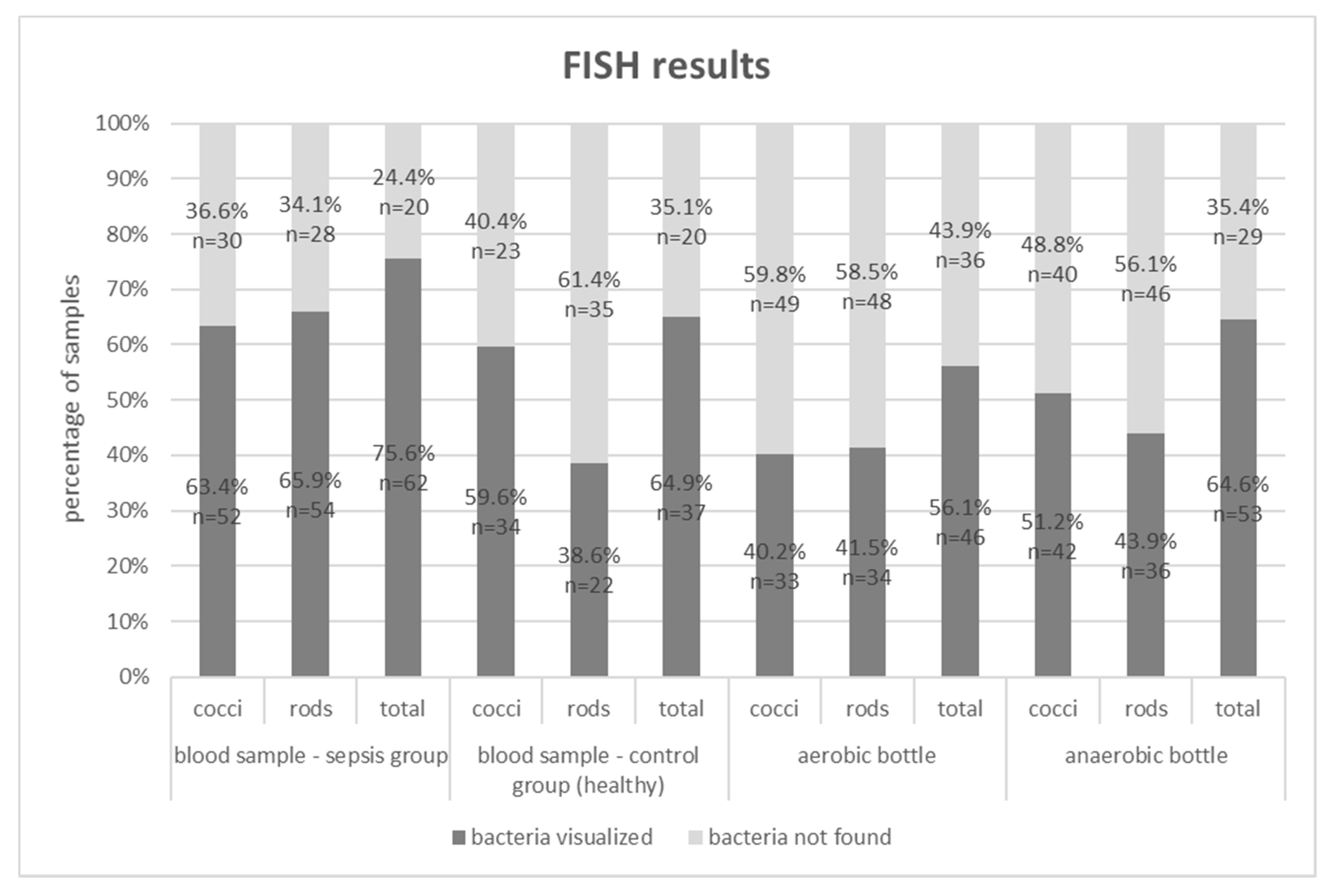
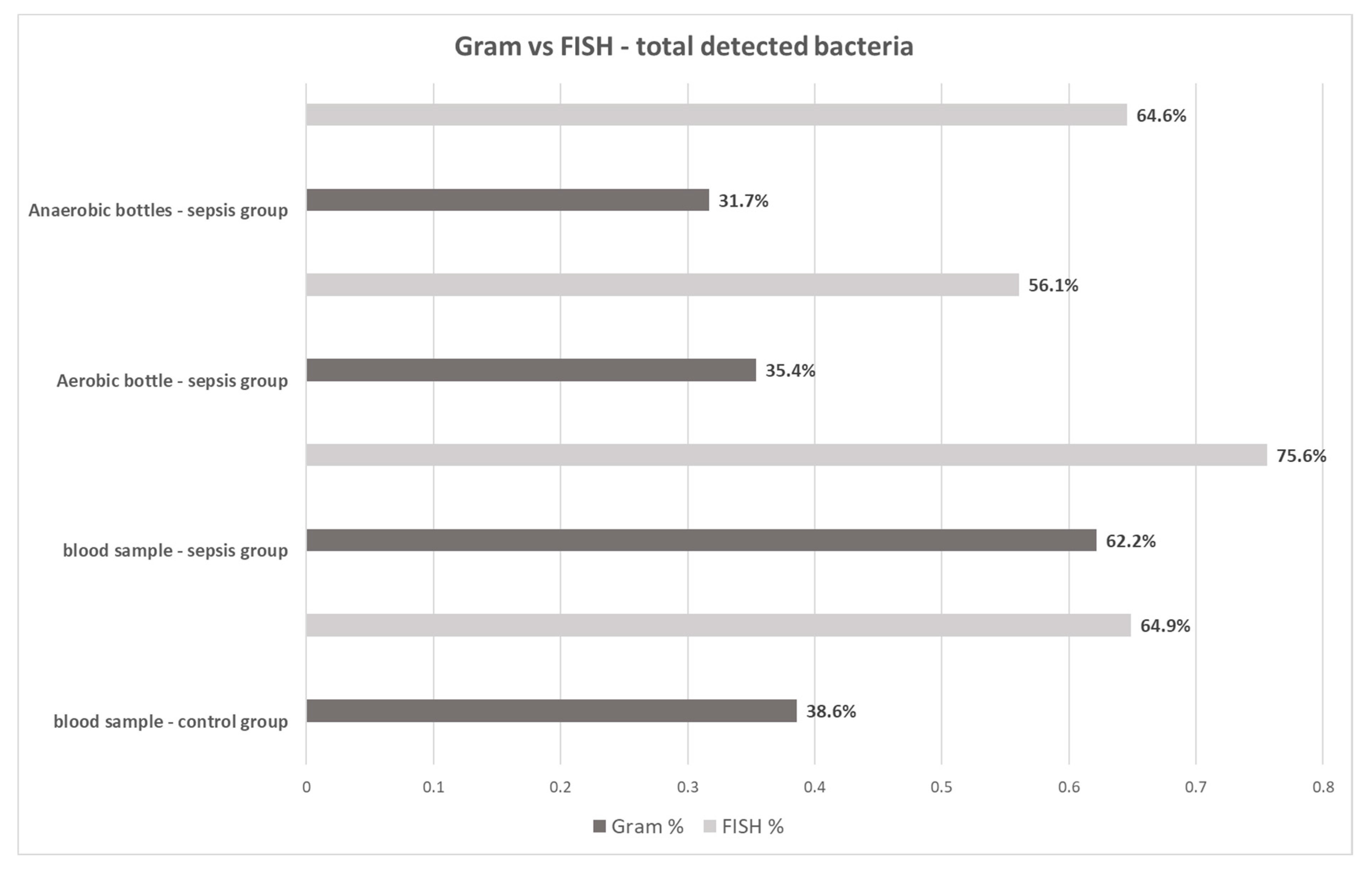
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hunfeld, K.-P.; Bingold, T.; Brade, V.; Wissing, H. Molecular biological detection of pathogens in patients with sepsis. Potentials, limitations and perspectives. Anaesthesist 2008, 57, 326–337. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.S.; Cheng, A.C.; McMillan, M.; Humphrey, A.B.; Stephens, D.P.; Anstey, N.M. Sepsis in the tropical Top End of Australia’s Northern Territory: Disease burden and impact on Indigenous Australians. Med. J. Aust. 2011, 194, 519–524. [Google Scholar] [CrossRef]
- Centers for Disease Control (CDC). Increase in National Hospital Discharge Survey Rates for Septicemia--United States. JAMA 1990, 263, 937–938.
- Fleischmann, C.; Scherag, A.; Adhikari, N.K.J.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K. Assessment of global incidence and mortality of hospital-treated sepsis current estimates and limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Sakhuja, A.; Kumar, G.; McGrath, E.; Nanchal, R.S.; Kashani, K.B. Culture-Negative Severe Sepsis. Chest 2016, 150, 1251–1259. [Google Scholar] [CrossRef] [PubMed]
- Jamal, W.; Tamaray, G.; Pazhoor, A.; Rotimi, V.O. Comparative evaluation of BacT/ALERT 3D and BACTEC systems for the recovery of pathogens causing bloodstream infections. Med. Princ. Pract. 2006, 15, 223–227. [Google Scholar] [CrossRef]
- Opal, S.M. Endotoxins and other sepsis triggers. Contrib. Nephrol. 2010, 167, 14–24. [Google Scholar]
- Dickson, K.; Lehmann, C. Inflammatory Response to Different Toxins in Experimental Sepsis Models. Int. J. Mol. Sci. 2019, 20, 4341. [Google Scholar] [CrossRef] [Green Version]
- Patterson, T.F.; Thompson, G.R.; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef]
- Gosiewski, T.; Flis, A.; Sroka, A.; Kedzierska, A.; Pietrzyk, A.; Kedzierska, J.; Drwila, R.; Bulanda, M. Comparison of nested, multiplex, qPCR; FISH; SeptiFast and blood culture methods in detection and identification of bacteria and fungi in blood of patients with sepsis. BMC Microbiol. 2014, 14, 2323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gosiewski, T.; Ludwig-Galezowska, A.H.H.; Huminska, K.; Sroka-Oleksiak, A.; Radkowski, P.; Salamon, D.; Wojciechowicz, J.; Kus-Slowinska, M.; Bulanda, M.; Wolkow, P.P.P. Comprehensive detection and identification of bacterial DNA in the blood of patients with sepsis and healthy volunteers using next-generation sequencing method - the observation of DNAemia. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 329–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Źródłowski, T.W.; Jurkiewicz-Badacz, D.; Sroka-Oleksiak, A.; Salamon, D.; Bulanda, M.; Gosiewski, T. Comparison of PCR, fluorescent in situ hybridization and blood cultures for detection of bacteremia in children and adolescents during antibiotic therapy. Polish J. Microbiol. 2018, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gosiewski, T.; Jurkiewicz-Badacz, D.; Sroka, A.; Brzychczy-Włoch, M.; Bulanda, M. A novel, nested, multiplex, real-time PCR for detection of bacteria and fungi in blood. BMC Microbiol. 2014, 14, 144. [Google Scholar] [CrossRef] [Green Version]
- Klouche, M.; Schröder, U. Rapid methods for diagnosis of bloodstream infections. Clin. Chem. Lab. Med. 2008, 46, 888–908. [Google Scholar] [CrossRef]
- Calderaro, A.; Martinelli, M.; Motta, F.; Larini, S.; Arcangeletti, M.C.; Medici, M.C.; Chezzi, C.; De Conto, F. Comparison of peptide nucleic acid fluorescence in situ hybridization assays with culture-based matrix-assisted laser desorption/ionization-time of flight mass spectrometry for the identification of bacteria and yeasts from blood cultures and cerebrospina. Clin. Microbiol. Infect. 2014, 8, O468–O475. [Google Scholar] [CrossRef] [Green Version]
- Farina, C.; Perin, S.; Andreoni, S.; Conte, M.; Fazii, P.; Lombardi, G.; Manso, E.; Morazzoni, C.; Sanna, S. Evaluation of the peptide nucleic acid fluorescence in situ hybridisation technology for yeast identification directly from positive blood cultures: An Italian experience. Mycoses 2012, 55, 388–392. [Google Scholar] [CrossRef]
- Parcell, B.J.; Orange, G. V PNA-FISH assays for early targeted bacteraemia treatment. J. Microbiol. Methods 2013, 95, 253–255. [Google Scholar] [CrossRef]
- Loonen, A.J.M.; Wolffs, P.F.G.; Bruggeman, C.A.; van den Brule, A.J.C. Developments for improved diagnosis of bacterial bloodstream infections. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1687–1702. [Google Scholar] [CrossRef]
- Źródłowski, T.W.; Flis, A.; Ziętkiewicz, M.; Drwiła, R.; Gosiewski, T. Fluorescent in situ hybridization and Gram-stained smears of whole blood as complementary screening tools in the diagnosis of sepsis. Polish Arch. Intern. Med. 2017, 127, 122–124. [Google Scholar] [CrossRef] [Green Version]
- Gosiewski, T.; Brzychczy, M. Gosiewski Method for efficient isolation of microbial dna from blood. United States Patent US9879311 (B2), 30 January 2018. [Google Scholar]
- Gosiewski, T.; Szała, L.; Pietrzyk, A.; Brzychczy-Włoch, M.; Heczko, P.B.; Bulanda, M. Comparison of Methods for Isolation of Bacterial and Fungal DNA from Human Blood. Curr. Microbiol. 2014, 68, 149–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amann, R.I.; Binder, B.J.; Olson, R.J.; Chisholm, S.W.; Devereux, R.; Stahl, D.A. Combination of 16S rRNA-targeted oligonucleotide probes with flow cytometry for analyzing mixed microbial populations. Appl. Environ. Microbiol. 1990, 56, 1919–1925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kempf, V.A.; Trebesius, K.; Autenrieth, I.B. Fluorescent In situ hybridization allows rapid identification of microorganisms in blood cultures. J. Clin. Microbiol. 2000, 38, 830–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedrich, U.; Van Langenhove, H.; Altendorf, K.; Lipski, A. Microbial community and physicochemical analysis of an industrial waste gas biofilter and design of 16S rRNA-targeting oligonucleotide probes. Environ. Microbiol. 2003, 5, 183–201. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, A.; Phillips, G.; Beale, R.; Cecconi, M.; Chiche, J.D.; De Backer, D.; Divatia, J.; Du, B.; Evans, L.; Ferrer, R.; et al. The Surviving Sepsis Campaign bundles and outcome: Results from the International Multicentre Prevalence Study on Sepsis (the IMPreSS study). Intensiv. Care Med. 2015, 41, 1620–1628. [Google Scholar] [CrossRef]
- Potgieter, M.; Bester, J.; Kell, D.B.; Pretorius, E. The dormant blood microbiome in chronic, inflammatory diseases. FEMS Microbiol. Rev. 2015, 39, 567–591. [Google Scholar] [CrossRef] [Green Version]
- Li, S.-K.; Leung, R.K.-K.; Guo, H.-X.; Wei, J.-F.; Wang, J.-H.; Kwong, K.-T.; Lee, S.-S.; Zhang, C.; Tsui, S.K.-W. Detection and identification of plasma bacterial and viral elements in HIV/AIDS patients in comparison to healthy adults. Clin. Microbiol. Infect. 2012, 18, 1126–1133. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Wang, C.; Tang, C.; Zhao, X.; He, Q.; Li, J. Identification and Characterization of Blood and Neutrophil-Associated Microbiomes in Patients with Severe Acute Pancreatitis Using Next-Generation Sequencing. Front. Cell. Infect. Microbiol. 2018, 8, 5. [Google Scholar] [CrossRef] [Green Version]
- Domingue, G.J.; Schlegel, J.U. Novel bacterial structures in human blood: Cultural isolation. Infect. Immun. 1977, 15, 621–627. [Google Scholar] [CrossRef] [Green Version]
- Tedeschi, G.G.; Bondi, A.; Paparelli, M.; Sprovieri, G. Electron microscopical evidence of the evolution of corynebacteria-like microorganisms within human erythrocytes. Experientia 1978, 34, 458–460. [Google Scholar] [CrossRef] [PubMed]
- Devine, K.M. Bacterial L-forms on tap: An improved methodology to generate Bacillus subtilis L-forms heralds a new era of research. Mol. Microbiol. 2012, 83, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Sinha, M.; Jupe, J.; Mack, H.; Coleman, T.P.; Lawrence, S.M.; Fraley, S.I. Emerging technologies for molecular diagnosis of sepsis. Clin. Microbiol. Rev. 2018, 31, e00089-17. [Google Scholar] [CrossRef] [Green Version]
- Delano, M.J.; Ward, P.A. Sepsis-induced immune dysfunction: Can immune therapies reduce mortality? J. Clin. Investig. 2016, 126, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Lissauer, M.E.; Leekha, S.; Preas, M.A.; Thom, K.A.; Johnson, S.B. Risk factors for central line-associated bloodstream infections in the era of best practice. J. Trauma Acute Care Surg. 2012, 72, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Wright, M.-O.; Decker, S.G.; Allen-Bridson, K.; Hebden, J.N.; Leaptrot, D. Healthcare-associated infections studies project: An American Journal of Infection Control and National Healthcare Safety Network data quality collaboration: Location mapping. Am. J. Infect. Control 2018, 46, 577–578. [Google Scholar] [CrossRef]
- Peretz, A.; Isakovich, N.; Pastukh, N.; Koifman, A.; Glyatman, T.; Brodsky, D. Performance of Gram staining on blood cultures flagged negative by an automated blood culture system. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 1539–1541. [Google Scholar] [CrossRef]
- Kocoglu, M.E.; Bayram, A.; Balci, I. Evaluation of negative results of BacT/Alert 3D automated blood culture system. J. Microbiol. 2005, 43, 257–259. [Google Scholar]
- Greene, M.T.; Saint, S.; Ratz, D.; Kuhn, L.; Davis, J.; Patel, P.K.; Rogers, M.A.M. Role of transfusions in the development of hospital-acquired urinary tract-related bloodstream infection among United States Veterans. Am. J. Infect. Control 2019, 47, 381–386. [Google Scholar] [CrossRef]
- Watanabe, N.; Kryukov, K.; Nakagawa, S.; Takeuchi, J.S.; Takeshita, M.; Kirimura, Y.; Mitsuhashi, S.; Ishihara, T.; Aoki, H.; Inokuchi, S.; et al. Detection of pathogenic bacteria in the blood from sepsis patients using 16S rRNA gene amplicon sequencing analysis. PLoS ONE 2018, 13, e0202049. [Google Scholar] [CrossRef]
- Rhodes, A.; Wort, S.J.; Thomas, H.; Collinson, P.; David, E.D. Plasma DNA concentration as a predictor of mortality and sepsis in critically ill patients. Crit. Care 2006, 10, R60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garnacho-Montero, J.; Huici-Moreno, M.J.; Gutiérrez-Pizarraya, A.; López, I.; Márquez-Vácaro, J.A.; Macher, H.; Guerrero, J.M.; Puppo-Moreno, A. Prognostic and diagnostic value of eosinopenia, C-reactive protein, procalcitonin, and circulating cell-free DNA in critically ill patients admitted with suspicion of sepsis. Crit. Care 2014, 18, R116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grumaz, S.; Stevens, P.; Grumaz, C.; Decker, S.O.; Weigand, M.A.; Hofer, S.; Brenner, T.; von Haeseler, A.; Sohn, K. Next-generation sequencing diagnostics of bacteremia in septic patients. Genome Med. 2016, 8, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Benítez-Páez, A.; Álvarez, M.; Belda-Ferre, P.; Rubido, S.; Mira, A.; Tomás, I. Detection of transient bacteraemia following dental extractions by 16S rDNA pyrosequencing: A pilot study. PLoS ONE 2013, 8, e57782. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sepsis Group – Blood Cultures | Control Group (n = 57) | ||
|---|---|---|---|
| Negative (n = 82) | Positive (n = 8) | ||
| Sex (male/female) | 0.64 (± 0.2) | 0.85 (± 0.4) | 0.31 (± 0.1) |
| Age (year) | 69.4 (± 11.2) | 58.8 (± 9.4) | 39.6 (± 7.9) |
| BMI (kg/m2) | 22.7 (± 4.8) | 23.5 (± 3.8) | 24.5 (± 1.9) |
| SOFA score | 7.9 (± 4.1) | 6.6 (± 4.7) | N/A |
| WBC (109/L) | 17.2 (± 10.9) | 18.1 (± 11.3) | 4.5 (± 0.8) |
| CRP (mg/L) | 194.1 (± 140.5) | 175.5 (± 150.8) | 1.4 (± 0.6) |
| PCT (ng/mL) | 5.9 (± 0.6) | 5.2 (± 0.7) | N/A |
| [%] | FISH | ||
|---|---|---|---|
| Gram stain | Blood Samples – Control Group | ||
| bacteria not found | bacteria visualized | ||
| bacteria not found | 35.1 | 26.3 | |
| bacteria visualized | 0.0 | 38.6 | |
| Blood Samples – Sepsis Group | |||
| bacteria not found | bacteria visualized | ||
| bacteria not found | 24.4 | 13.4 | |
| bacteria visualized | 0.0 | 62.2 | |
| Aerobic Bottles Samples – Sepsis Group | |||
| bacteria not found | bacteria visualized | ||
| bacteria not found | 43.9 | 20.7 | |
| bacteria visualized | 0.0 | 35.4 | |
| Anaerobic Bottles Samples – Sepsis Group | |||
| bacteria not found | bacteria visualized | ||
| bacteria not found | 24.4 | 45.3 | |
| bacteria visualized | 11.0 | 19.3 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Źródłowski, T.; Sobońska, J.; Salamon, D.; McFarlane, I.M.; Ziętkiewicz, M.; Gosiewski, T. Classical Microbiological Diagnostics of Bacteremia: Are the Negative Results Really Negative? What is the Laboratory Result Telling Us About the “Gold Standard”? Microorganisms 2020, 8, 346. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8030346
Źródłowski T, Sobońska J, Salamon D, McFarlane IM, Ziętkiewicz M, Gosiewski T. Classical Microbiological Diagnostics of Bacteremia: Are the Negative Results Really Negative? What is the Laboratory Result Telling Us About the “Gold Standard”? Microorganisms. 2020; 8(3):346. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8030346
Chicago/Turabian StyleŹródłowski, Tomasz, Joanna Sobońska, Dominika Salamon, Isabel M. McFarlane, Mirosław Ziętkiewicz, and Tomasz Gosiewski. 2020. "Classical Microbiological Diagnostics of Bacteremia: Are the Negative Results Really Negative? What is the Laboratory Result Telling Us About the “Gold Standard”?" Microorganisms 8, no. 3: 346. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8030346