Diagnosis of Osteoarticular Tuberculosis: Perceptions, Protocols, Practices, and Priorities in the Endemic and Non-Endemic Areas of the World—A WAIOT View

 ,
,  ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
1.1. Epidemiology with India as an Example of the Endemic World
1.2. Epidemiology in the Non-Endemic World
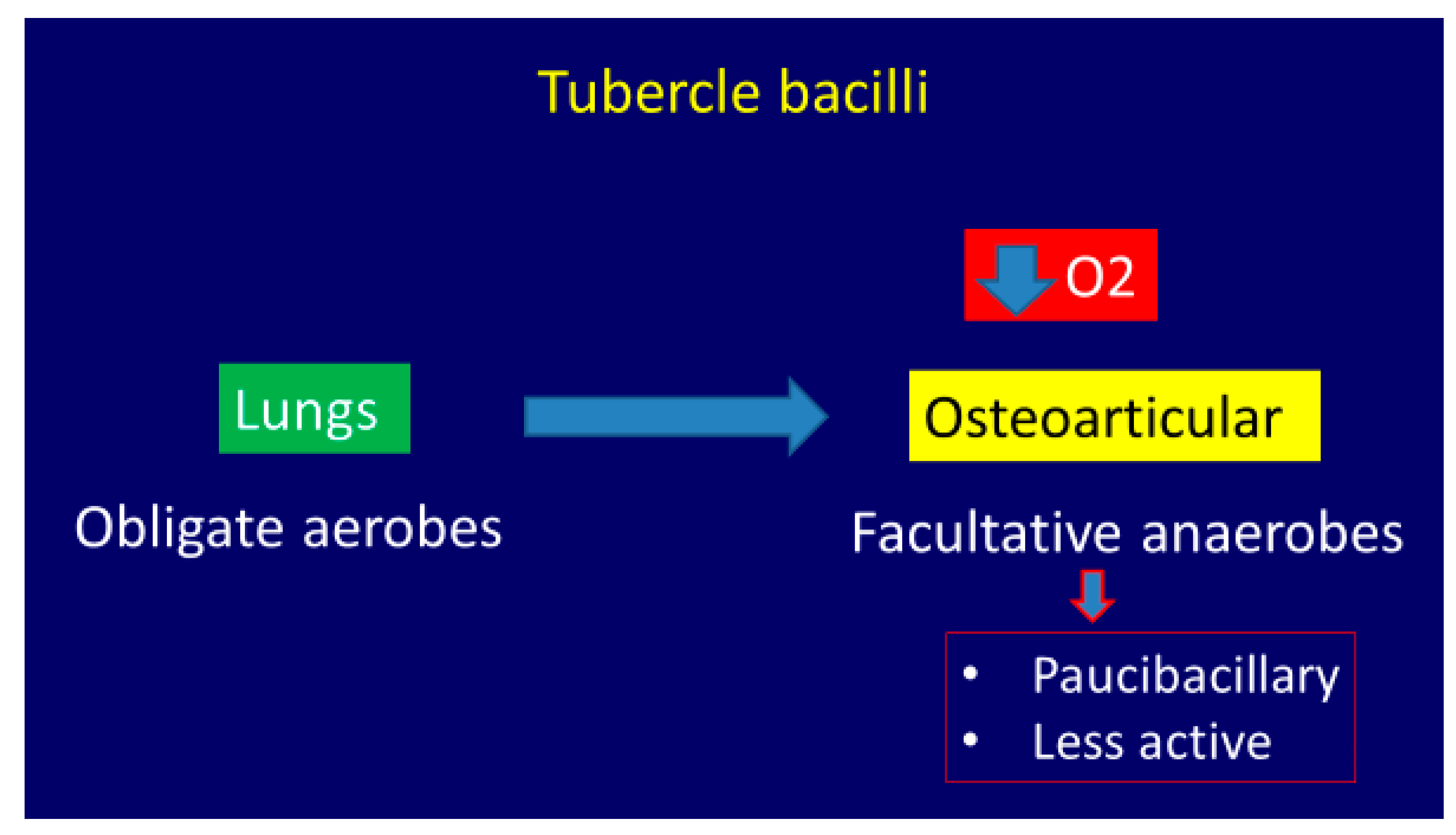
2. Etiopathogenesis
2.1. Clinical Features
- 1.
- Stage of synovitis. Patient presents with night pain and spasm of the affected group of muscles. Affected joint has >75% of the joint movement preserved. X-ray shows rarefaction and haziness of the articular regions. This stage has excellent prognosis.
- 2.
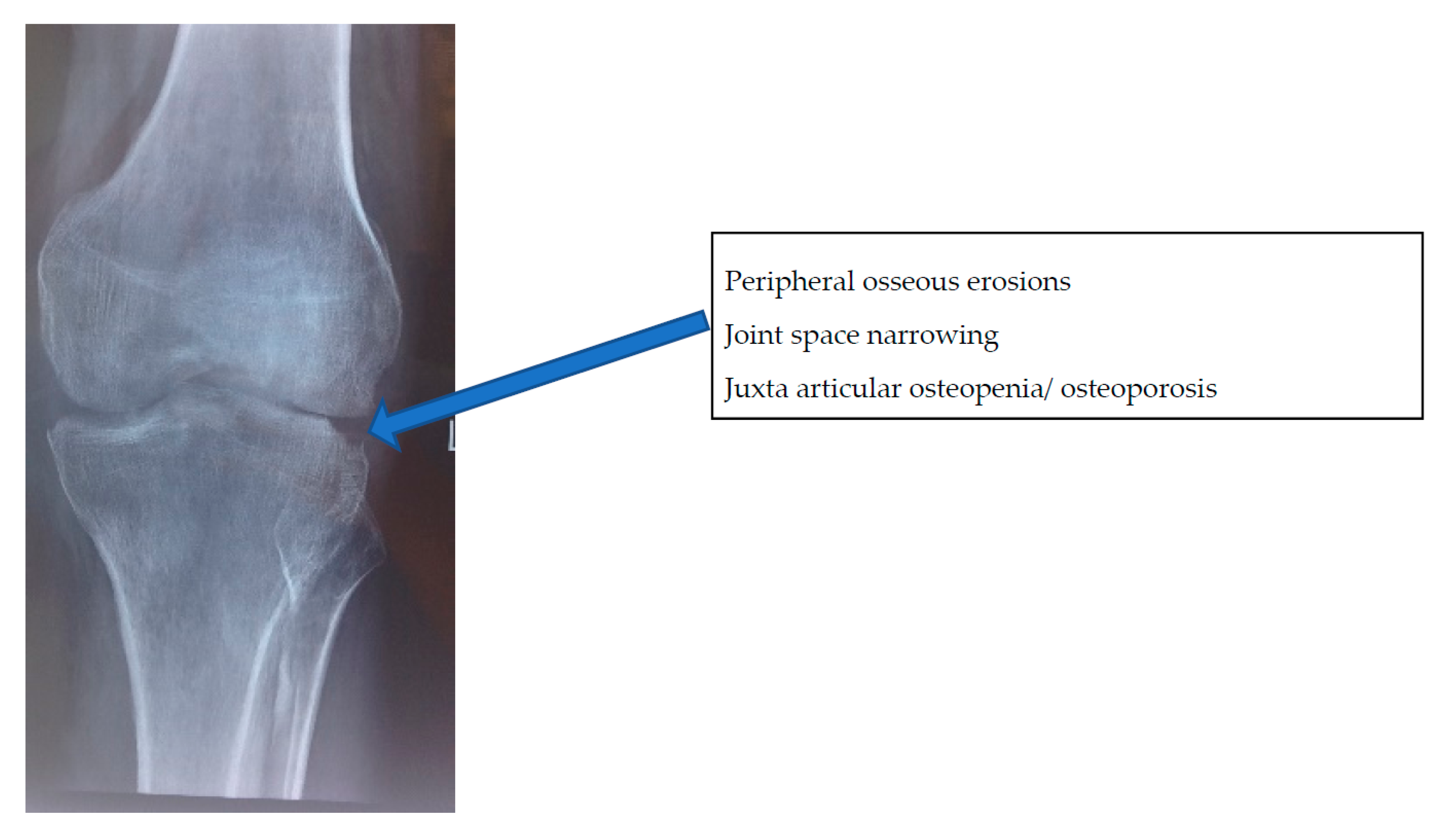
- Stage of early arthritis. Patient presents with joint pain, spasm of the surrounding muscle, and difficulty in doing some activities of daily living. Affected joint has 50–75% of the joint movement preserved. X-ray shows classical Phemister’s triad of juxta-articular osteopenia, mild joint space reduction, and peripheral osseous erosions. This stage has good prognosis with mild stiffness.
- 3.
- Stage of late arthritis. Patient presents with joint pain, spasm, and difficulty in activities of daily living. Affected joint has >75% loss of range of movement of the joint. X-ray shows marked joint space reduction and joint destruction. This stage has fair prognosis with severe loss of motion.
- 4.
- Stage of advanced arthritis with subluxation and dislocation. Patient presents with deformity of the involved joint. Affected joint has gross restriction of all movements. X-ray shows pathological dislocation with wandering acetabulum in the hip. This stage has poor prognosis.
- 5.
- Terminal or sequelae of arthritis. Fibrous ankylosis of the joint is seen.
2.2. Imaging Features
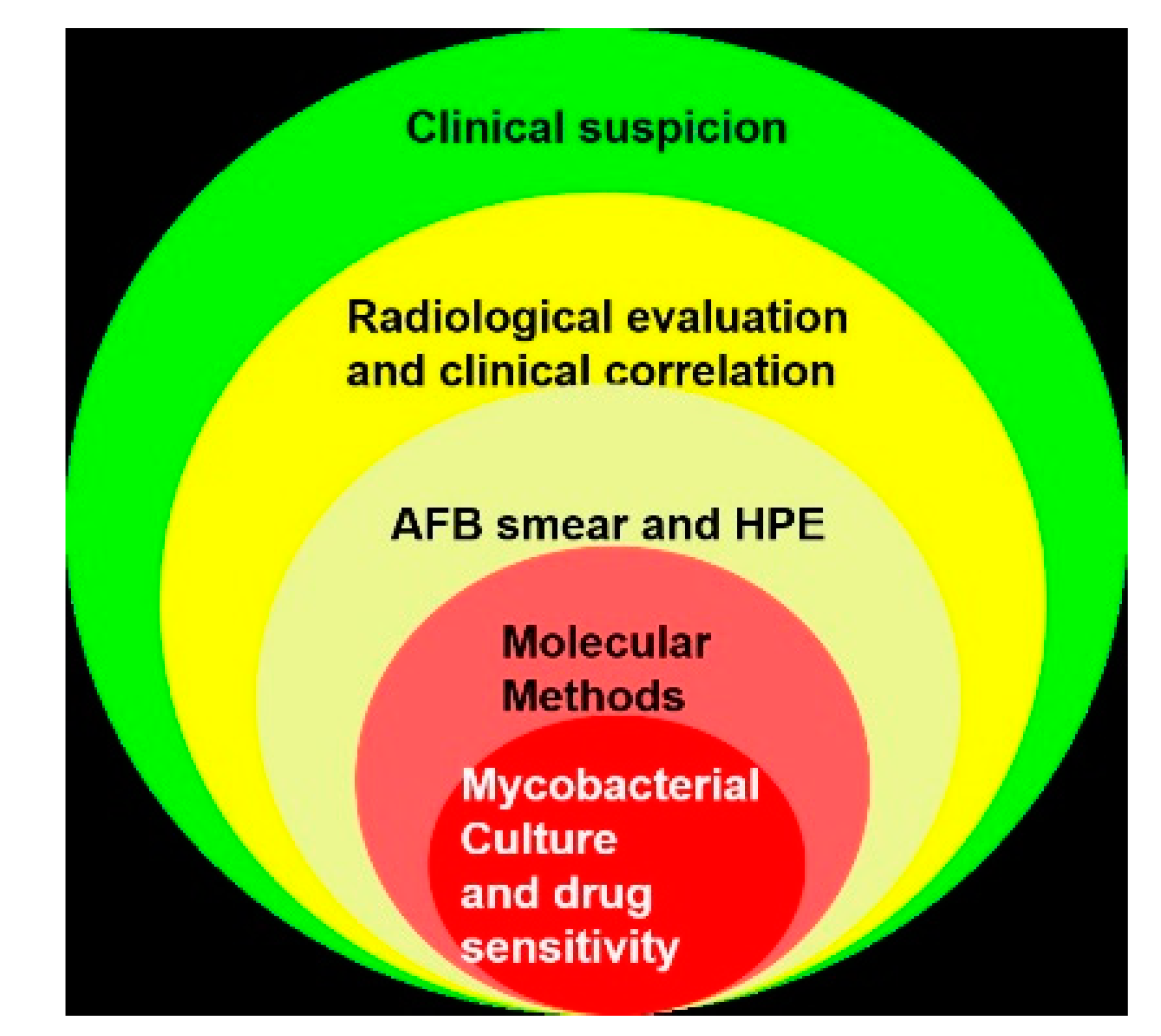
3. Diagnosis of Osteoarticular Tuberculosis
3.1. Obtaining an Appropriate Sample for Laboratory Studies
3.2. Culture, Genotype Diagnosis, and Drug Susceptibility
3.3. Smear and Histopathology
3.4. Indirect Diagnosis—Serological Tests
3.5. Clinico-Radiological Diagnosis
3.6. Differential Diagnosis
- 1.
- Non-tuberculous mycobacteria (NTM). Initiating ATT would not yield desirable results in cases of NTM [71].
- 2.
- Pyogenic arthritis
- 3.
- Rheumatoid arthritis (RA). In RA, the disease is usually polyarticular, the synovium tends to be thicker and irregular, and erosions are smaller as compared to OA TB [76].
- 4.
- Pyogenic spondylodiscitis. Presents as single segment involvement with poor soft tissue mass and early disc changes on MRI [77].
- 5.
- Seronegative spondyloarthropathy, especially while dealing with sacroiliac lesions.


4. Discussion
- 1)
- Ruling out false-positive and false-negative cases and achieving probable diagnosis of TB.
- a)
- Confirming that other conditions are not treated as tuberculosis (Ruling out false positive);
- b)
- Establishing that TB is not treated as other conditions (Ruling out false negative).
- 2)
- Achieving accurate diagnosis of TB and establishing sensitivity pattern, ideally in every patient of OA tuberculosis.
- 3)
- Performing diagnostics in patients who were treated with empirical ATT and not responding to ATT.
- a)
- Ruling out false-positive cases: Empirical ATT is often erroneously initiated in NTM infections and pyogenic infections, among many others.NTM infections are often not even considered and ATT is instituted when histopathology reveals granulomatous infections. Some details of history like infection following open fractures or invasive procedures like arthroscopy or intra-articular injections would point to NTM infection [71]. It is best to inform the microbiologist about the suspicion so that appropriate tests are carried out. Another important feature in NTM infections that helps in early diagnosis is a positive smear for acid-fast bacilli and negative GeneXpert [75,76,77,78,79,80]. The incidence of these infections is sizeable. In an Indian study of 1295 extrapulmonary TB suspects, NTM was grown in 72 specimens, while M. tb was cultured in 189 specimens [51].Pyogenic infections are to be ruled out in every case of suspected OA TB by smear and culture for pyogenic organisms. In a study of 93 patients referred from city public hospitals and private healthcare facilities across Mumbai on the threshold of receiving ATT for suspected OA TB, 7 out of 93 were diagnosed to be suffering from pyogenic infections [41]. Other conditions such as rheumatoid arthritis and ankylosing spondylitis can be differentiated from OA TB by a good clinical and radiological examination and an appropriate referral to a rheumatologist.
- b)
- Ruling out false negative: Confirming that TB is not treated as other conditions. Several studies from non-endemic areas or developed countries have reported a delay in diagnosis and treatment for OA TB, mainly because the condition is not high on the clinician’s differential diagnosis list. The medical community should bear in mind that immigration from disease-endemic regions has reintroduced the relatively rare tuberculosis infection.In a paper entitled “Delays in the diagnosis and treatment of bone and joint tuberculosis in the United Kingdom”, Broderick et al. described a median delay of seven months between the onset of symptoms and the referral to an appropriate center in 30 patients who were finally diagnosed as OA TB; 89% of their patients were migrants. They also noted that in 23% of the patients the initial sample was not sent for mycobacterial culture at the time of index surgery at the tertiary center, needing a second surgery [86].Arrabal et al. described a three-year delay in diagnosis of TB of the hip joint in a 54-year-old patient in Spain, even though he had multiple discharging sinuses around the hip. Based on a culture from the sinus that grew coagulase-negative Staphylococcus aureus, he was initially treated with targeted antibiotics [87].
- 4)
- Establishing a sensitivity pattern ideally in every patient of OA tuberculosis: The importance of establishing a sensitivity pattern can be judged by a recent publication on prevalence and patterns of drug-resistant pulmonary tuberculosis in India by Lohiya et al. [58]. They found the incidence of any one drug resistance at 24.9%, MDR at 3.5%, and XDR at 0.6% in new cases. INH (isoniazid) resistance was highest at 16% while rifampicin was at 4.7%, suggesting that rifampicin sensitivity cannot be considered as a surrogate marker of INH sensitivity. In re-treatment cases, the incidence of MDR was 26.7% and any one drug resistance was 58.4%.Since OA TB is likely to follow the same trend, targeted ATT is essential to addressing the challenge of drug-resistant OA TB infection. Prerequisite to this is improving the yield of the M. tb culture. Appropriate sample and container, early transfer to a laboratory with experience to tackle extrapulmonary specimens, and availability of liquid culture medium play an important role in improving the yield of the sample.
- 5)
- Diagnosing and Addressing Non-Respondents: After the initiation of empirical ATT based on either clinico-radiological or histopathological findings, the patients must be closely observed.If a satisfactory response is not determined in about three months, a close review is needed to find the reason for poor response. The poor response can be judged by persistent or increased swelling, development of new swelling or new lesion, persistent discharging sinus, development of new sinus, development of non-healing ulcer, neurological deterioration, or development of new neurological deficit. Agashe et al. under the aegis of the Bombay Orthopaedic Society studied 89 patients not responding to ATT at a mean duration of 9.32 months (3 months to 60 months). Surprisingly, 80.9% patients were initiated on ATT without tissue diagnosis. Of the 89 patients, 33 had resistance to at least one drug, 24 were MDR, and 3 were XDR. Noteworthy findings were varying resistance pattern, primary resistance to second-line drugs, and high number of resistant patients in the pediatric age group. On comparing the resistance pattern with another Bombay Orthopaedic Society project conducted between 2004 and 2007, the authors noted significant deterioration in the resistance pattern [41]. Another concerning observation was that 16/89 patients were suffering from TB mimics. The authors urged for a drastic change in mindset in diagnosing and managing OA TB in India and have stressed that it is not adequate to only diagnose OA TB but establishing a drug sensitivity pattern is important [38].
- 1.
- “Complete diagnosis of OA TB”—i.e., culture-positive cases with drug sensitivity known and in whom targeted chemotherapy can be initiated.
- 2.
- “Qualify for ATT”—i.e., ATT is initiated based only on clinical and imaging findings or on results of tests that do not establish a sensitivity pattern. This is an acceptable practice but only after attempts at establishing a “complete diagnosis” have failed and the surgeon strongly suspects OA TB.
- 3.
- The term “clinico-radiological diagnosis” should be replaced by clinico-radiological impression as there is no consensus on clinical and/or radiological criteria for diagnosing OA TB.
5. Conclusions
- 1.
- TB is a tenacious disease having bounced back from the brink of defeat to a position of infecting 10 million people annually.
- 2.
- The incidence of TB is disproportionately high in India, China, and some African countries.
- 3.
- Drug resistance is increasing in endemic areas and, at present, at least a quarter of new TB cases are resistant to at least one drug and about 3% have MDR. Resistance to fluroquinolones, aminoglycosides, ethionamide, and PAS are also noted in new cases.
- 4.
- OA TB is paucibacterial, often slowly progressive, accompanied by constitutional symptoms in about one-third to one-half of cases. Spinal TB is the most common presentation of OA TB.
- 5.
- OA TB constitutes between 1% and 3% of the TB population and, hence, surgeons in endemic areas are exposed to a greater patient load of OA TB cases as compared to surgeons in non-endemic areas.
- 6.
- Surgeons in endemic areas tend to “over-diagnose” TB as tissue diagnosis is hardly obtained due to the lack of infrastructure, a reportedly poor culture yield, the confidence in clinical acumen, and a belief in MRI. The initiation of empirical ATT is almost a norm in most parts of India.
- 7.
- While surgeons in non-endemic areas often “under-diagnose” OA TB because pyogenic infections are always high on the list and investigations are directed accordingly, this often leads to a delay in diagnosis.
- 8.
- The initiation of ATT is a fateful decision; the practice of empirical ATT, although reasonably successful in previous years, is certainly not advisable in view of rising drug resistance. Every attempt must be made to establish a drug sensitivity pattern before the initiation of ATT.
- 9.
- Due to the paucibacterial nature and moderate culture yield at best, empirical ATT must be started in a proportion of cases even if the culture yield is negative, if OA TB is strongly suspected. These patients must be observed very carefully and, if a good response is not obtained after three to four months, the cause for the poor response must be investigated and addressed.
- 10.
- Infrastructure development on a priority basis is the need of the hour in endemic regions and an improved perception is required in non-endemic regions.
Author Contributions
Funding
Conflicts of Interest
References
- Romanò, C.L.; Drago, L.; Del Sel, H.; Johari, A.; Lob, G.; Mavrogenis, A.F.; Benzakour, T. World Association against Infection in Orthopedics and Trauma (WAIOT) Study Group On Bone and Joint Infection Definitions. Loud and silent epidemics in the third millennium: Tuning-up the volume. Int. Orthop. 2020, 44, 1019–1022. [Google Scholar] [CrossRef] [PubMed]
- Holm, J. How Can Elimination of Tuberculosis as a Public Health Problem be Achieved? Am. Rev. Tuberc. Pulm. Dis. 1959, 79, 690–694. [Google Scholar] [CrossRef]
- Vankayalapati, R.; Barnes, P.F. Innate and adaptive immune responses to human Mycobacterium tuberculosis infection. Tuberculosis 2009, 89, S77–S80. [Google Scholar] [CrossRef]
- Maniar, J.K.; Kamath, R.R.; Mandalia, S.; Shah, K.; Maniar, A. HIV and tuberculosis: Partners in crime. Indian J. Dermatol. Venereol. Leprol. 2006, 72, 276. [Google Scholar] [CrossRef] [PubMed]
- Seung, K.J.; Keshavjee, S.; Rich, M.L. Multidrug-Resistant Tuberculosis and Extensively Drug-Resistant Tuberculosis. Cold Spring Harb. Perspect. Med. 2015, 5, a017863. [Google Scholar] [CrossRef] [Green Version]
- Annabel, B.; Anna, D.; Hannah, M. WHO Global Tuberculosis Report; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Cummings, K.J. Tuberculosis control: Challenges of an ancient and ongoing epidemic. Public Health Rep. 2007, 122, 683–692. [Google Scholar] [CrossRef]
- Magnussen, A.; Dinneen, A.; Ramesh, P. Osteoarticular tuberculosis: Increasing incidence of a difficult clinical diagnosis. Br. J. Gen. Pr. 2013, 63, 385–386. [Google Scholar] [CrossRef] [Green Version]
- Central TB Division, Ministry of Health & Family Welfare, GoI. Report on National Workshop on Drug Susceptibility Testing (DST) Guided Treatment for Drug Resistant Tuberculosis Patients in India. Available online: https://tbcindia.gov.in/WriteReadData/l892s/713587265Report_ITR%20workshop.pdf (accessed on 1 July 2020).
- Ministry of Health and Family Welfare GoI. Report of the first national anti-tuberculosis drug resistance survey: India 2014–16. Available online: https://tbcindia.gov.in/showfile.php?lid=3315 (accessed on 9 April 2018).
- Mohan, K.; Rawall, S.; Pawar, U.M.; Sadani, M.; Nagad, P.; Nene, A.; Nene, A.M. Drug resistance patterns in 111 cases of drug-resistant tuberculosis spine. Eur. Spine J. 2012, 22, 647–652. [Google Scholar] [CrossRef] [Green Version]
- Garg, R.K.; Somvanshi, D.S. Spinal tuberculosis: A review. J. Spinal Cord Med. 2011, 34, 440–454. [Google Scholar] [CrossRef] [Green Version]
- Fitoz, S.; Atasoy, C.; Yagmurlu, A.; Akyar, S. Psoas abscess secondary to tuberculous lymphadenopathy: Case report. Abdom. Imaging 2001, 26, 323–324. [Google Scholar] [CrossRef]
- Boudville, D.; Joshi, R.; Rijkers, G.T. Migration and tuberculosis in Europe. J. Clin. Tuberc. Other Mycobact. Dis. 2020, 18, 100143. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control/WHO Regional Office for Europe. Tuberculosis Surveillance and Monitoring in Europe 2020: 2018 Data. Available online: https://www.ecdc.europa.eu/en/publications-data/tuberculosis-surveillance-and-monitoring-europe-2020-2018-data (accessed on 1 July 2020).
- Centers for Disease Control and Prevention. Trends in Tuberculosis, 2018. Available online: https://www.cdc.gov/tb/publications/factsheets/statistics/tbtrends.htm (accessed on 1 July 2020).
- Pigrau, C.; Rodríguez-Pardo, D. Bone and joint tuberculosis. Eur. Spine J. 2012, 22 (Suppl. 4), 556–566. [Google Scholar] [CrossRef]
- Moon, M.-S.; Kim, S.-S.; Moon, H.-L.; Kim, D.-H. Mycobacterium tuberculosis in spinal tuberculosis. Asian Spine J. 2017, 11, 138–149. [Google Scholar] [CrossRef] [Green Version]
- Procopie, I.; Popescu, E.L.; Huplea, V.; Pleșea, R.; Ghelase, Ș.M.; Stoica, G.; Mureșan, R.; Onțică, V.; Pleșea, I.; Anușca, D. Osteoraticular tuberculosis-brief review of clinical morphological and therapeutic profiles. Curr. Health Sci. J. 2017, 43, 171–190. [Google Scholar] [CrossRef]
- Tuli, S.M. General principles of osteoarticular tuberculosis. Clin. Orthop. Relat. Res. 2002, 398, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, V.; Prasad, S.; Wakhlu, A.; Misra, R.; Aggarwal, A.; Lawrence, A.; Gupta, R.K.; Krishnani, N.; Agrawal, V. Features of extra-spinal musculoskeletal tuberculosis: A retrospective study from an North Indian Tertiary Care Institute. Indian J. Rheumatol. 2017, 12, 146. [Google Scholar] [CrossRef]
- Somen, D. A Manual on Clinical Surgery, 13th ed.; S Das Publication: Kolkata, India, 2015. [Google Scholar]
- Tuli, S. Tuberculosis of the Skeletal System; JP Medical Ltd.: New Delhi, India, 2016; p. 57. [Google Scholar]
- Griffith, J.F.; Kumta, S.M.; Leung, P.C.; Cheng, J.; Chow, L.T.; Metreweli, C. Imaging of musculoskeletal tuberculosis: A new look at an old disease. Clin. Orthop. Relat. Res. 2002, 398, 32–39. [Google Scholar] [CrossRef]
- Jain, A.K. Tuberculosis of spine: Research evidence to treatment guidelines. Indian J. Orthop. 2016, 50, 3–9. [Google Scholar] [CrossRef]
- Jain, A.K. Spinal TB: Impact of research evidence on clinical practice. Ann. Natl. Acad. Med Sci. 2018, 54, 33–42. [Google Scholar] [CrossRef]
- Vanhoenacker, F.M.; Sanghvi, D.A.; De Backer, A.I. Imaging features of extraaxial musculoskeletal tuberculosis. Indian J. Radiol. Imaging 2009, 19, 176–186. [Google Scholar] [CrossRef]
- Jain, R.; Sawhney, S.; Berry, M. Computer tomography of vertebral tuberculosis: Patterns of bone destruction. Clin. Radiol. 1993, 47, 196–199. [Google Scholar] [CrossRef]
- Sharif, H.S.; Morgan, J.L.; Al Shahed, M.S.; Al Thagafi, M.Y. Role of CT and MR imaging in the management of tuberculous spondylitis. Radiol. Clin. N. Am. 1995, 33, 787–804. [Google Scholar] [PubMed]
- Buxi, T.B.S.; Sud, S.; Vohra, R. CT and MRI in the diagnosis of tuberculosis. Indian J. Pediatr. 2002, 69, 965–972. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Papadopoulos, N.; Chen, Y.; Zhao, Y. Osteoarticular tuberculosis in children. A fast reappearing disease diagnosed by 18F-FDG PET/CT and other modalities. The cover page of Nicholas Andry booklet L’ Orthopedie. Hell. J. Nucl. Med. 2018, 21, 205–212. [Google Scholar]
- Jain, A.K.; Mittal, S.; Chakraborti, K.L.; Aggarwal, A.N.; Upreti, L.; Bhayana, H. Evaluation of healed status in tuberculosis of spine by fluorodeoxyglucose-positron emission tomography/computed tomography and contrast magnetic resonance imaging. Indian J. Orthop. 2019, 53, 160–168. [Google Scholar] [CrossRef]
- Cho, Y.S.; Chung, D.R.; Lee, E.J.; Kim, B.-T.; Lee, K.-H. 18F-FDG PET/CT in a case of multifocal skeletal tuberculosis without pulmonary disease and potential role for monitoring treatment response. Clin. Nucl. Med. 2014, 39, 980–983. [Google Scholar] [CrossRef] [PubMed]
- Mousa, H.A.-L. Evaluation of sinus-track cultures in chronic bone infection. J. Bone Jt. Surg. 1997, 79, 567–569. [Google Scholar] [CrossRef]
- Evanchick, C.C.; E Davis, D.; Harrington, T.M. Tuberculosis of peripheral joints: An often missed diagnosis. J. Rheumatol. 1986, 13, 187–189. [Google Scholar]
- Jacobs, J.C.; Li, S.C.; Ruzal-Shapiro, C.; Kiernan, H.; Parisien, M.; Shapiro, A. Tuberculous arthritis in children. Clin. Pediatr. 1994, 33, 344–348. [Google Scholar] [CrossRef]
- Dhillon, M.S.; Agashe, V.; Patil, S.D. Role of surgery in management of osteo-articular tuberculosis of the foot and ankle. Open Orthop. J. 2017, 11, 633–650. [Google Scholar] [CrossRef] [Green Version]
- Agashe, V.M.; Rodrigues, C.; Soman, R.; Shetty, A.; Deshpande, R.B.; Ajbani, K.; Pingle, J.; Agashe, M.; Patil, H.; Raghuwanshi, S.; et al. Diagnosis and management of osteoarticular tuberculosis: A drastic change in mind set needed—It is not enough to simply diagnose TB. Indian J. Orthop. 2020. [Google Scholar] [CrossRef]
- Sahoo, M.M.; Mahapatra, S.K.; Sethi, G.C.; Sahoo, A.; Kar, B.K.; Sahoo, M.M. Role of percutaneous transpedicular biopsy in diagnosis of spinal tuberculosis and its correlation with the clinico-radiological features. Indian J. Tuberc. 2018, 66, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Chakravorty, S.; Sen, M.K.; Tyagi, J.S. Diagnosis of extrapulmonary tuberculosis by smear, culture, and PCR using universal sample processing technology. J. Clin. Microbiol. 2005, 43, 4357–4362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agashe, V.; Shenai, S.; Mohrir, G.; Deshmukh, M.; Bhaduri, A.; Deshpande, R.; Mehta, A.; Rodrigues, C. Osteoarticular tuberculosis—Diagnostic solutions in a disease endemic region. J. Infect. Dev. Ctries. 2009, 3, 511–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonio, M.; Otu, J.; Cheung, Y.B.; Donkor, S.; De Jong, B.C.; Corrah, T.; Adegbola, R.A. Comparative evaluation of BACTEC MGIT 960 with BACTEC 9000 MB and LJ for isolation of mycobacteria in The Gambia. J. Infect. Dev. Ctries. 2008, 2, 200–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malhotra, B.; Pal, N.; Rishi, S.; Sinha, P. A comparative study for the detection of Mycobacteria by BACTEC MGIT 960, Lowenstein Jensen media and direct AFB smear examination. Indian J. Med Microbiol. 2007, 25, 383. [Google Scholar] [CrossRef] [PubMed]
- Chien, H.P.; Yu, M.C.; Wu, M.H.; Lin, T.P.; Luh, K.T. Comparison of the BACTEC MGIT 960 with Löwenstein-Jensen medium for recovery of mycobacteria from clinical specimens. Int. J. Tuberc. Lung Dis. 2000, 4, 866–870. [Google Scholar] [PubMed]
- Nambiar, R.; Chatellier, S.; Bereksi, N.; Van Belkum, A.; Singh, N.; Barua, B.; Shetty, A.; Rodrigues, C. Evaluation of mycotube, a modified version of Lowenstein–Jensen (LJ) medium, for efficient recovery of mycobacterium tuberculosis (MTB). Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 1981–1988. [Google Scholar] [CrossRef]
- Shenai, S. WHO recommended tools to improve diagnosis of active and drug resistant tuberculosis. Acta Med. Int. 2015, 2, 118–129. [Google Scholar] [CrossRef]
- Rageade, F.; Picot, N.; Blanc-Michaud, A.; Chatellier, S.; Mirande, C.; Fortin, E.; Van Belkum, A. Performance of solid and liquid culture media for the detection of mycobacterium tuberculosis in clinical materials: Meta-analysis of recent studies. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 867–870. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Zhang, Z.; Luo, F.; Xu, J.-Z.; Cheng, P.; Wu, Z.; Zhou, Q.; He, Q.; Dai, F.; Wang, J.; et al. Management of drug-resistant spinal tuberculosis with a combination of surgery and individualised chemotherapy: A retrospective analysis of thirty-five patients. Int. Orthop. 2011, 36, 277–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, J.; Jian-Zhong, X.; Xue-Mei, L.; Bao-Feng, G. Drug susceptibility testing guided treatment for drug-resistant spinal tuberculosis: A retrospective analysis of 19 patients. Int. Surg. 2013, 98, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Lakhanpal, V.P.; Tuli, S.M.; Singh, H.; Sen, P.C. The Value of Histology, Culture and Guinea Pig Inoculation Examination in Osteo-Articular Tuberculosis. Acta Orthop. Scand. 1974, 45, 36–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swaminathan, S.; Dusthackeer, A.; Sekar, G.; Chidambaram, S.; Kumar, V.; Mehta, P. Drug resistance among extrapulmonary TB patients: Six years experience from a supranational reference laboratory. Indian J. Med. Res. 2015, 142, 568–574. [Google Scholar] [CrossRef]
- Vardhan, V.; Yanamandra, U. Diagnosis of osteoarticular tuberculosis. Indian J. Rheumatol. 2011, 6 (Suppl. 1), 87–94. [Google Scholar] [CrossRef]
- Sekyere, J.O.; Maphalala, N.; Malinga, L.A.; Mbelle, N.M.; Maningi, N.E. A comparative evaluation of the new genexpert MTB/RIF ultra and other rapid diagnostic assays for detecting tuberculosis in pulmonary and extra pulmonary specimens. Sci. Rep. 2019, 9, 16587. [Google Scholar] [CrossRef] [Green Version]
- E Dorman, S.; Schumacher, S.G.; Alland, D.; Nabeta, P.; Armstrong, D.T.; King, B.; Hall, S.L.; Chakravorty, S.; Cirillo, D.M.; Tukvadze, N.; et al. Xpert MTB/RIF ultra for detection of mycobacterium tuberculosis and rifampicin resistance: A prospective multicentre diagnostic accuracy study. Lancet Infect. Dis. 2017, 18, 76–84. [Google Scholar] [CrossRef] [Green Version]
- Menichini, M.; Lari, N.; Lupetti, A.; Rindi, L. Evaluation of Xpert MTB/RIF Ultra assay for rapid diagnosis of pulmonary and extra-pulmonary tuberculosis in an Italian center. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1597–1600. [Google Scholar] [CrossRef]
- Huh, H.J.; Song, D.J.; Ki, C.-S.; Lee, N.Y. Is cross-reactivity with nontuberculous mycobacteria a systematic problem in the xpert MTB/RIF assay? Tuberc. Respir. Dis. 2019, 82, 88–89. [Google Scholar] [CrossRef]
- Zheng, R.; Zhu, C.-T.; Guo, Q.; Qin, L.; Wang, J.; Lü, J.; Cui, H.; Cui, Z.; Ge, B.; Liu, J.-M.; et al. Pyrosequencing for rapid detection of Tuberculosis resistance in clinical isolates and Sputum samples from re-treatment pulmonary tuberculosis patients. BMC Infect. Dis. 2014, 14, 200. [Google Scholar] [CrossRef] [Green Version]
- Lohiya, A.; Suliankatchi, R.A.; Rath, R.S.; Jacob, O.; Chinnakali, P.; Goel, A.D.; Agrawal, S. National and sub-national level prevalence and patterns of drug resistant pulmonary tuberculosis—A systematic review and meta-analysis of Indian studies. J. Glob. Antimicrob. Resist. 2020, 22, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Shi, M.; Feng, G.-D.; Liu, J.-Y.; Wang, B.-J.; Shi, X.-D.; Ma, L.; Liu, X.-D.; Yang, Y.-N.; Dai, W.; et al. A highly efficient Ziehl-Neelsen stain: Identifying de novo intracellular mycobacterium tuberculosis and improving detection of extracellular M. tuberculosis in cerebrospinal fluid. J. Clin. Microbiol. 2012, 50, 1166–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooja, S.; Pal, N.; Malhotra, B.; Goyal, S.; Kumar, V.; Vyas, L. Comparison of Ziehl Neelsen & Auramine O staining methods on direct and concentrated smears in clinical specimens. Indian J. Tuberc. 2011, 58, 72–76. [Google Scholar] [PubMed]
- Hazra, A.; Laha, B. Chemotherapy of osteoarticular tuberculosis. Indian J. Pharmacol. 2005, 37, 5. [Google Scholar] [CrossRef]
- Ahmad, N.A.F.; Huda, N. Osteoarticular tuberculosis—A three years’ retrospective study. J. Clin. Diagn. Res. 2013, 7, 2189–2192. [Google Scholar] [CrossRef]
- Barik, S.; Choudhury, A.K.; Singh, V.; Bali, S. Extra-spinal osteoarticular tuberculosis: A retrospective analysis of 103 cases. Curr. Health Sci. J. 2019, 45, 142–147. [Google Scholar]
- Aggarwal, A.N.; Dhammi, I.K.; Jain, A.K. Multifocal skeletal tuberculosis. Trop. Dr. 2001, 31, 219–220. [Google Scholar] [CrossRef]
- Dhammi, I.K.; Jain, A.K.; Singh, S.; Aggarwal, A.; Kumar, S. Multifocal skeletal tuberculosis in children: A retrospective study of 18 cases. Scand. J. Infect. Dis. 2003, 35, 797–799. [Google Scholar] [CrossRef]
- Harries, A. Applying advances to the developing world for TB and HIV control. Int. J. Tuberc. Lung Dis. 2000, 4, S65–S70. [Google Scholar]
- Fan, L.; Chen, Z.; Hao, X.-H.; Hu, Z.-Y.; Xiao, H. Interferon-gamma release assays for the diagnosis of extrapulmonary tuberculosis: A systematic review and meta-analysis. FEMS Immunol. Med. Microbiol. 2012, 65, 456–466. [Google Scholar] [CrossRef]
- Rangaka, M.X.; A Wilkinson, K.; Glynn, J.R.; Ling, D.; Menzies, D.; Mwansa-Kambafwile, J.; Fielding, K.; Wilkinson, R.J.; Pai, M. Predictive value of interferon-γ release assays for incident active tuberculosis: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 45–55. [Google Scholar] [CrossRef] [Green Version]
- World Health Orgnaization (WHO). Commercial Serodiagnostic Tests for Diagnosis of Tuberculosis: Policy Statement; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Mariconda, M.; Cozzolino, A.; Attingenti, P.; Cozzolino, F.; Milano, C. Osteoarticular tuberculosis in a developed country. J. Infect. 2007, 54, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Gundavda, M.; Patil, H.G.; Agashe, V.M.; Soman, R.; Rodriques, C.; Deshpande, R.B. Nontuberculous mycobacterial infection of the musculoskeletal system in immunocompetent hosts. Indian J. Orthop. 2017, 51, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Bacha, J.M.; Ngo, K.; Clowes, P.; Draper, H.R.; Ntinginya, E.N.; Dinardo, A.; Mangu, C.; Sabi, I.; Mtafya, B.; Mandalakas, A.M. Why being an expert—Despite Xpert -remains crucial for children in high TB burden settings. BMC Infect. Dis. 2017, 17, 123. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, S.; Poonawala, H.; Jain, Y. Drug-resistant tuberculosis: Is India ready for the challenge? BMJ Glob. Health 2018, 3, e000971. [Google Scholar] [CrossRef]
- Durán, M.J.P.; Sanz-Gadea, B.M.; Raves, T.D.R.; Peña, M.J.M.; Baquero-Artigao, F. Osteoarticular tuberculosis in paediatrics: A review of 20 years of cases in a tertiary hospital. An. Pediatría (English Edition) 2017, 87, 291–292. [Google Scholar] [CrossRef]
- Lombardi, G.; Di Gregori, V.; Girometti, N.; Tadolini, M.; Bisognin, F.; Monte, P.D. Diagnosis of smear-negative tuberculosis is greatly improved by Xpert MTB/RIF. PLoS ONE 2017, 12, e0176186. [Google Scholar] [CrossRef]
- Choi, J.-A.; Koh, S.H.; Hong, S.-H.; Koh, Y.H.; Choi, J.-Y.; Kang, H.S. Rheumatoid arthritis and tuberculous arthritis: Differentiating MRI features. Am. J. Roentgenol. 2009, 193, 1347–1353. [Google Scholar] [CrossRef]
- De Souza, C.G.; Gasparetto, E.L.; Marchiori, E.; Bahia, P.R.V. Pyogenic and tuberculous discitis: Magnetic resonance imaging findings for differential diagnosis. Radiol. Bras. 2013, 46, 173–177. [Google Scholar] [CrossRef] [Green Version]
- Tsantes, A.G.; Papadopoulos, D.V.; Vrioni, G.; Sioutis, S.; Sapkas, G.; Benzakour, A.; Benzakour, T.; Angelini, A.; Ruggieri, P.; Mavrogenis, A.F.; et al. Spinal infections: An update. Microorganisms 2020, 8, 476. [Google Scholar] [CrossRef] [Green Version]
- Wagh, Y.; Reddy, R.; Gundavda, M.; Agarwal, M.; Agashe, V.M.; Bajwa, S. Tuberculosis (T.B.) masquerading as tumor. An 8-year study on 25 cases of long bone tuberculosis presenting as tumors. SICOT-J 2020, 6, 14. [Google Scholar] [CrossRef] [PubMed]
- Mnyambwa, N.; Ngadaya, E.S.; Kimaro, G.; Kim, N.-J.; Kazwala, R.; Petrucka, P.; Mfinanga, S.G. Assessment of sputum smear-positive but culture-negative results among newly diagnosed pulmonary tuberculosis patients in Tanzania. Int. J. Gen. Med. 2017, 10, 199–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukopadhaya, B. The role of excisional surgery in the treatment of bone and joint tuberculosis. Ann. R. Coll. Surg. Engl. 1956, 18, 288–313. [Google Scholar] [PubMed]
- Velayati, A.A.; Masjedi, M.R.; Farnia, P.; Tabarsi, P.; Ghanavi, J.; ZiaZarifi, A.H.; Hoffner, S.E. Emergence of new forms of totally drug-resistant tuberculosis bacilli. Chest 2009, 136, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Udwadia, Z.F.; Amale, R.A.; Ajbani, K.K.; Rodrigues, C. Totally drug-resistant tuberculosis in India. Clin. Infect. Dis. 2011, 54, 579–581. [Google Scholar] [CrossRef] [Green Version]
- Mistry, N.; Tolani, M.; Osrin, D. Drug-resistant tuberculosis in Mumbai, India: An agenda for operations research. Oper. Res. Health Care 2012, 1, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Udwadia, Z.F.; Pinto, L.; Uplekar, M.W. Tuberculosis Management by Private Practitioners in Mumbai, India: Has anything changed in two decades? PLoS ONE 2010, 5, e12023. [Google Scholar] [CrossRef] [Green Version]
- Broderick, C.; Hopkins, S.; Mack, D.J.F.; Aston, W.; Pollock, R.; Skinner, J.A.; Warren, S. Delays in the diagnosis and treatment of bone and joint tuberculosis in the United Kingdom. Bone Jt. J. 2018, 100, 119–124. [Google Scholar] [CrossRef]
- Arrabal, E.G.; Sola, M.J.P.; Ruiz-Cabello, M.M.; Granger, J.R.; Egea, G. Osteoarticular tuberculosis of the hip and soft tissues: Images of a diagnostic delay. Rev. Esp. Quimioter. 2018, 31, 383–385. [Google Scholar]
- Law, S.; Piatek, A.; Vincent, C.; Oxlade, O.; Menzies, D. Emergence of drug resistance in patients with tuberculosis cared for by the Indian health-care system: A dynamic modelling study. Lancet Public Health 2017, 2, e47–e55. [Google Scholar] [CrossRef] [Green Version]
- Central Bureau of Health intelligence, Government of India. National Health Profile; 14th Issue; Central Bureau of Health intelligence, Government of India: New Delhi, India, 2019.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Country, Year | Culture-Positive TB | Number of TB-Resistant Cases (MDR, Multidrug Resistance; XDR, Extensive Drug Resistance) |
|---|---|---|
| Li L et al., 2012 [48] | 127/249 | Any one drug resistance—39 (30.7%); Of these, MDR—12/127 (9.5%) |
| Xu L et al., 2013 [49] | 76/152 | Any one drug resistance—23/76 (30.1%); MDR—16/76 (21%) |
| Agashe et al., 2009 [41] | 47/74 | Any one drug resistance—5/47 (32%) MDR—12/47 (25.5%); XDR—2/47 (4.3%) |
| Mohan K et al., 2013 [11] | 686 | Any one drug resistance—111/686 (16.2%); MDR—87/686 (12.7%); XDR—3/686 (0.4%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agashe, V.M.; Johari, A.N.; Shah, M.; Anjum, R.; Romano, C.; Drago, L.; Sharma, H.K.; Benzakour, T. Diagnosis of Osteoarticular Tuberculosis: Perceptions, Protocols, Practices, and Priorities in the Endemic and Non-Endemic Areas of the World—A WAIOT View. Microorganisms 2020, 8, 1312. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8091312
Agashe VM, Johari AN, Shah M, Anjum R, Romano C, Drago L, Sharma HK, Benzakour T. Diagnosis of Osteoarticular Tuberculosis: Perceptions, Protocols, Practices, and Priorities in the Endemic and Non-Endemic Areas of the World—A WAIOT View. Microorganisms. 2020; 8(9):1312. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8091312
Chicago/Turabian StyleAgashe, Vikas M., Ashok N. Johari, Mudit Shah, Rashid Anjum, Carlo Romano, Lorenzo Drago, Hemant K. Sharma, and Thami Benzakour. 2020. "Diagnosis of Osteoarticular Tuberculosis: Perceptions, Protocols, Practices, and Priorities in the Endemic and Non-Endemic Areas of the World—A WAIOT View" Microorganisms 8, no. 9: 1312. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8091312