Ceftolozane-Tazobactam Treatment of Hypervirulent Multidrug Resistant Pseudomonas aeruginosa Infections in Neutropenic Patients

 , , ,
, , ,
Abstract
:1. Introduction
2. Case Descriptions
2.1. Case #1—Index Case
2.2. Case #2
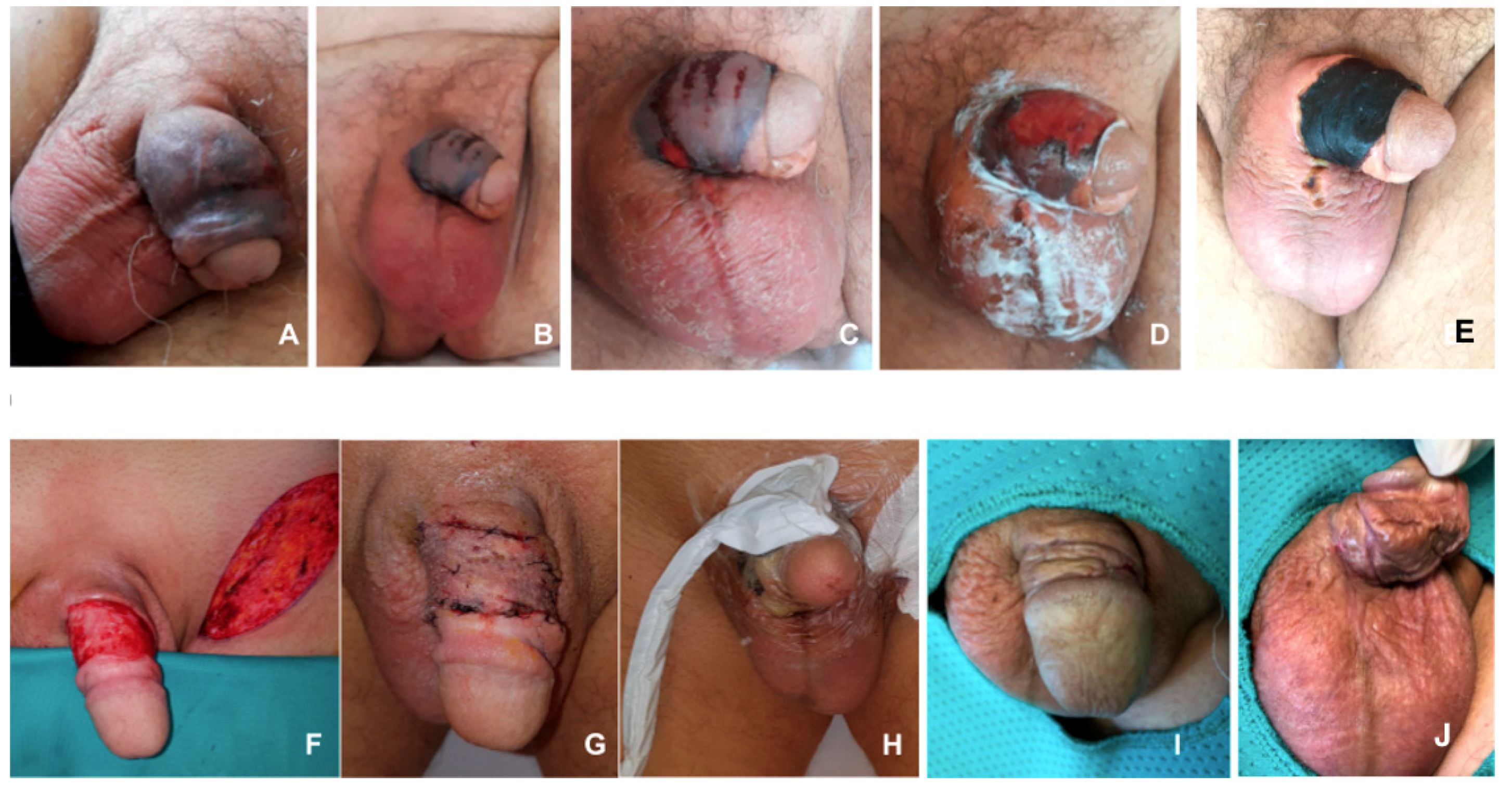
2.3. Case #3
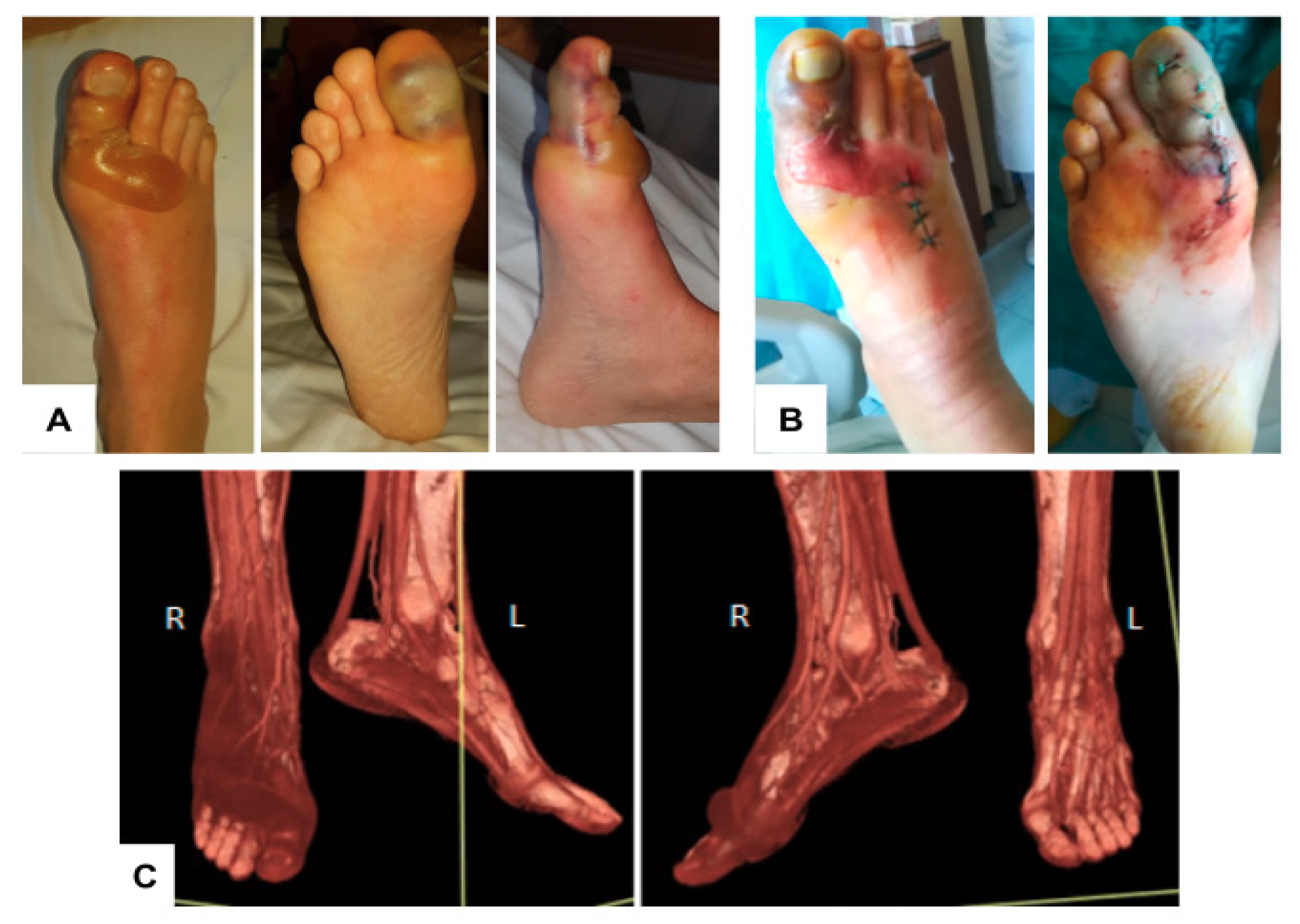
2.4. Case #4
2.5. Cases #5–7
3. Microbiology
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Smibert, O.; Satlin, M.J.; Nellore, A.; Peleg, A.Y. Carbapenem-Resistant Enterobacteriaceae in Solid Organ Transplantation: Management Principles. Curr. Infect. Dis. Rep. 2019, 21, 26. [Google Scholar] [CrossRef] [PubMed]
- Emmett, C.D.; Kane, G. Necrotising fasciitis caused by P aeruginosa in a male patient with chronic lymphocytic leukaemia. BMJ Case Rep. 2013, 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinelli, G.; Alessandrino, E.; Bernasconi, P.; Caldera, D.; Colombo, A.A.; Malcovati, L.; Gaviglio; Vignoli, G.; Borroni, G.; Bernasconi, C. Fournier’s gangrene: A clinical presentation of necrotizing fasciitis after bone marrow transplantation. Bone Marrow Transplant. 1998, 22, 1023–1026. [Google Scholar] [CrossRef] [Green Version]
- Verweij, P.E.; Bijl, D.; Melchers, W.J.; De Pauw, B.E.; Meis, J.F.; Hoogkamp-Korstanje, J.A.; Voss, A. Pseudo-outbreak of multiresistant Pseudomonas aeruginosa in a hematology unit. Infect. Control Hosp. Epidemiol. 1997, 18, 128–131. [Google Scholar] [CrossRef] [PubMed]
- Breathnach, A.; Cubbon, M.; Karunaharan, R.; Pope, C.; Planche, T. Multidrug-resistant Pseudomonas aeruginosa outbreaks in two hospitals: Association with contaminated hospital waste-water systems. J. Hosp. Infect. 2012, 82, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Kossow, A.; Kampmeier, S.; Willems, S.; Burckhardt, B.; Groth, C.; Kipp, F.; Mellmann, A.; Stelljes, M.; Berdel, W.E.; Groll, A.; et al. Control of Multidrug-Resistant Pseudomonas aeruginosa in Allogeneic Hematopoietic Stem Cell Transplant Recipients by a Novel Bundle Including Remodeling of Sanitary and Water Supply Systems. Clin. Infect. Dis. 2017, 65, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Rodríguez-Baño, J. The Use of Noncarbapenem β-Lactams for the Treatment of Extended-Spectrum β-Lactamase Infections. Clin. Infect. Dis. 2017, 64, 972–980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treepong, P.; Kos, V.; Guyeux, C.; Blanc, D.; Bertrand, X.; Valot, B.; Hocquet, D. Global emergence of the widespread Pseudomonas aeruginosa ST235 clone. Clin. Microbiol. Infect. 2018, 24, 258–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabot, G.; López-Causapé, C.; Ocampo-Sosa, A.A.; Sommer, L.M.; Domínguez, M.Á.; Zamorano, L.; Juan, C.; Tubau, F.; Rodríguez, C.; Moyà, B.; et al. Deciphering the Resistome of the Widespread Pseudomonas aeruginosa Sequence Type 175 International High-Risk Clone through Whole-Genome Sequencing. Antimicrob. Agents Chemother. 2016, 60, 7415–7423. [Google Scholar] [PubMed] [Green Version]
- Peña, C.; Cabot, G.; Gómez-Zorrilla, S.; Zamorano, L.; A Ocampososa, A.; Murillas, J.; Almirante, B.; Pomar, V.; Aguilar, M.; Granados, A.; et al. Influence of Virulence Genotype and Resistance Profile in the Mortality of Pseudomonas aeruginosa Bloodstream Infections. Clin. Infect. Dis. 2015, 60, 539–548. [Google Scholar] [CrossRef]
- Engel, J.N.; Balachandran, P. Role of Pseudomonas aeruginosa type III effectors in disease. Curr. Opin. Microbiol. 2009, 12, 61–66. [Google Scholar] [CrossRef]
- Van Duin, D.; Bonomo, R.A. Ceftazidime/Avibactam and Ceftolozane/Tazobactam: Second-generation β-Lactam/β-Lactamase Inhibitor Combinations. Clin. Infect. Dis. 2016, 63, 234–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhanel, G.G.; Chung, P.; Adam, H.; Zelenitsky, S.; Denisuik, A.; Schweizer, F.; Lagacé-Wiens, P.R.S.; Rubinstein, E.; Gin, A.S.; Walkty, A.; et al. Ceftolozane/Tazobactam: A Novel Cephalosporin/β-Lactamase Inhibitor Combination with Activity Against Multidrug-Resistant Gram-Negative Bacilli. Drugs 2013, 74, 31–51. [Google Scholar] [CrossRef] [PubMed]
- Cluck, D.; Lewis, P.; Stayer, B.; Spivey, J.; Moorman, J. Ceftolozane–tazobactam: A new-generation cephalosporin. Am. J. Heal. Pharm. 2015, 72, 2135–2146. [Google Scholar] [CrossRef] [PubMed]
- Goodlet, K.J.; Nicolau, D.P.; Nailor, M.D. In Vitro Comparison of Ceftolozane-Tazobactam to Traditional Beta-Lactams and Ceftolozane-Tazobactam as an Alternative to Combination Antimicrobial Therapy for Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 2017, 61, e01350-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solomkin, J.; Hershberger, E.; Miller, B.; Popejoy, M.; Friedland, I.; Steenbergen, J.; Yoon, M.; Collins, S.; Yuan, G.; Barie, P.S.; et al. Ceftolozane/Tazobactam Plus Metronidazole for Complicated Intra-abdominal Infections in an Era of Multidrug Resistance: Results From a Randomized, Double-Blind, Phase 3 Trial (ASPECT-cIAI). Clin. Infect. Dis. 2015, 60, 1462–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, L.J. Ceftolozane/Tazobactam: A Review in Complicated Intra-Abdominal and Urinary Tract Infections. Drugs 2016, 76, 231–242. [Google Scholar] [CrossRef] [PubMed]
- Haidar, G.; Philips, N.J.; Shields, R.K.; Snyder, D.; Cheng, S.; A Potoski, B.; Doi, Y.; Hao, B.; Press, E.G.; Cooper, V.S.; et al. Ceftolozane-Tazobactam for the Treatment of Multidrug-Resistant Pseudomonas aeruginosa Infections: Clinical Effectiveness and Evolution of Resistance. Clin. Infect. Dis. 2017, 65, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Aitken, S.L.; A Bonomo, R.; Mathers, A.J.; Van Duin, D.; Clancy, C.J. OUP accepted manuscript. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Fermández-Cruz, A.; Alba, N.; Semiglia-Chong, M.A.; Padilla, B.; Rodríguez-Macías, G.; Kwon, M.; Cercenado, E.; Chamorro-De-Vega, E.; Machado, M.; Pérez-Lago, L.; et al. A Case-Control Study of Real-Life Experience with Ceftolozane-Tazobactam in Patients with Hematologic Malignancy and Pseudomonas aeruginosa Infection. Antimicrob. Agents Chemother. 2018, 63, e02340-18. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
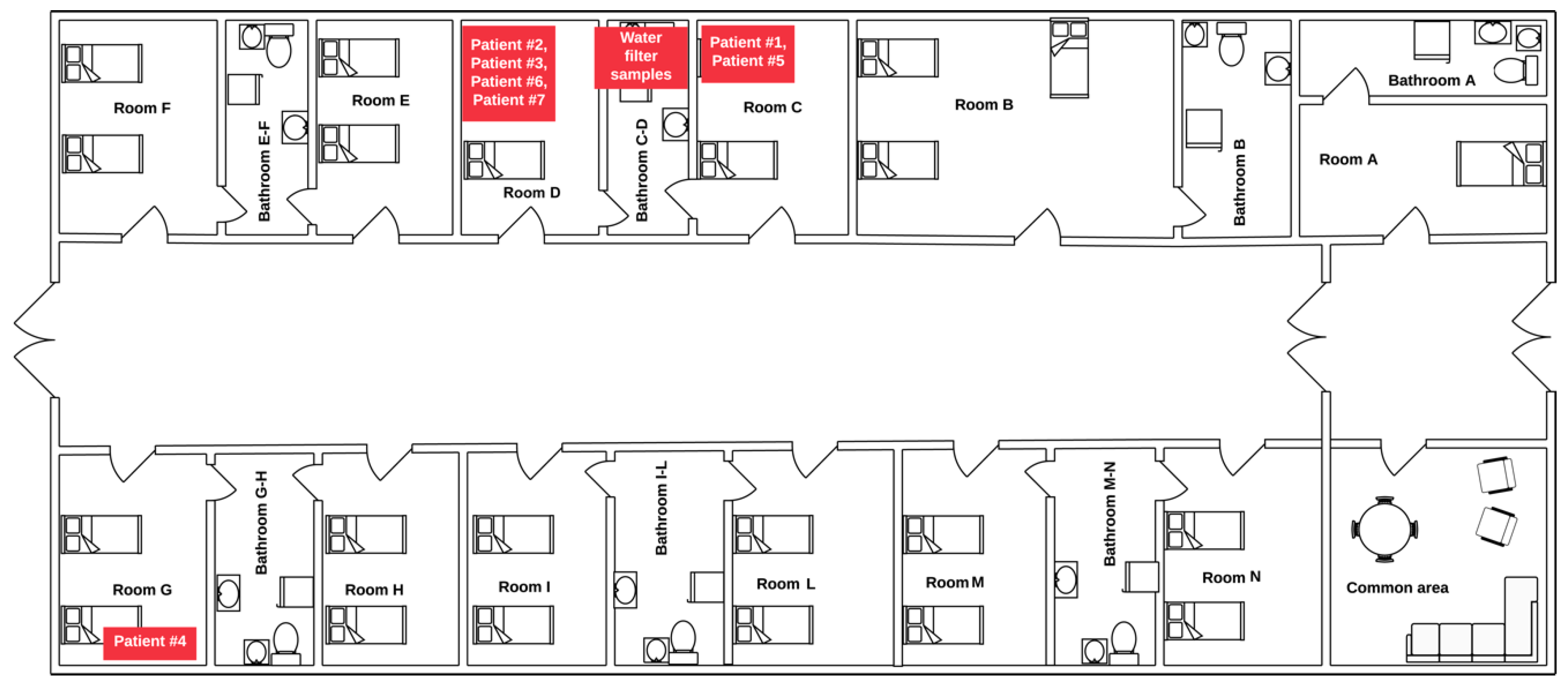
| ID | Case 1 | Case 2 | Case 3 | Case 4 |
|---|---|---|---|---|
| Room | C | D | D | G |
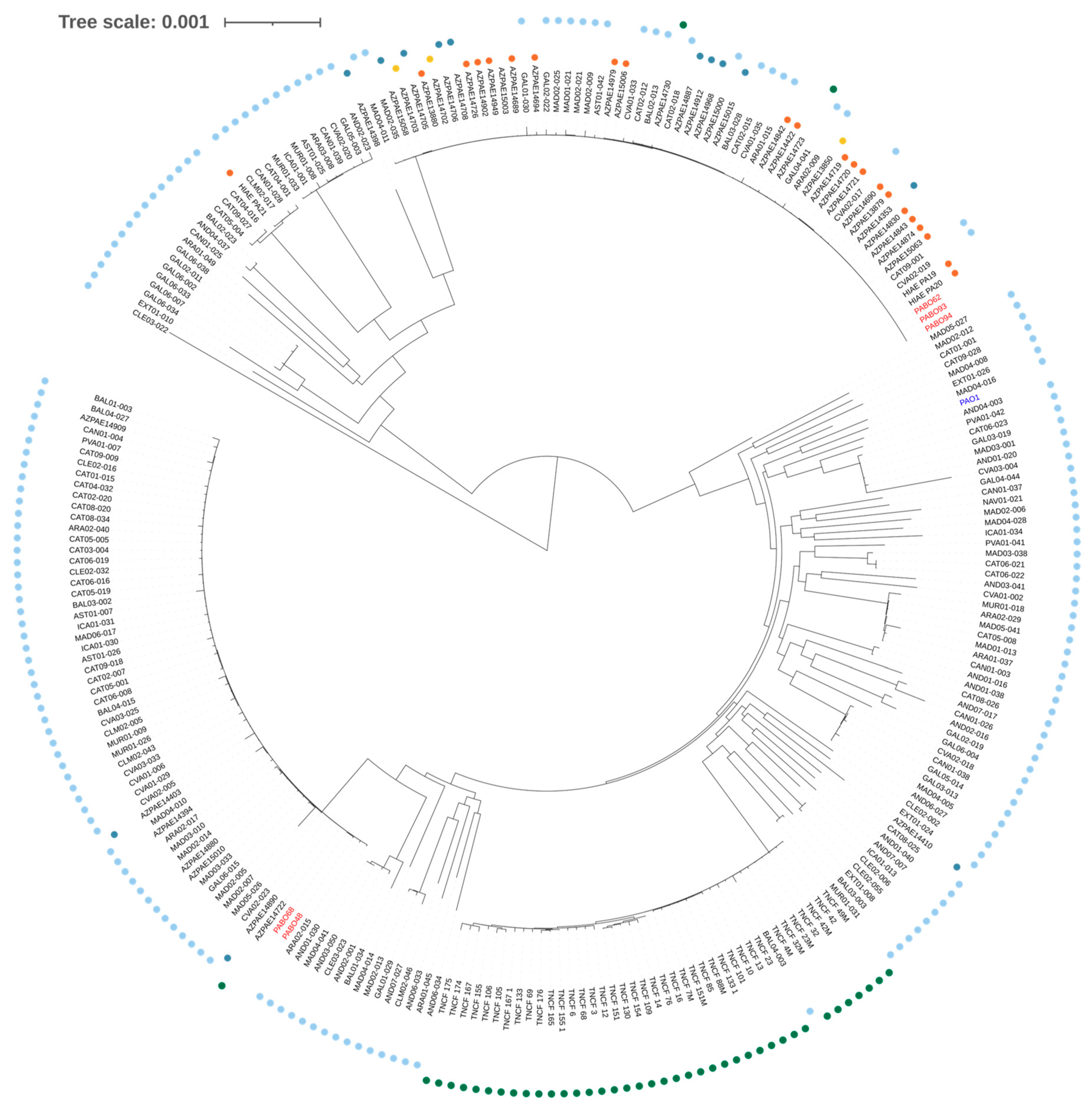
| Isolate (MLST type) | N/A | N/A | PABO62 (ST235) | PABO48 (ST175) |
| Date of onset | Feb 8 | Feb 19 | April 7 | May 4 |
| Hematological disease | ALL | AML | AML | LY |
| Age | 43 | 44 | 60 | 64 |
| Disease status | CR | Onset | Onset | Relapse |
| Chemotherapy | Consol. | Induction | Induction | Relapse |
| Neutropenia | Yes | Yes | Yes | Yes |
| Antimicrobial prophylaxis | TMP-SMX | TMP-SMX, levofloxacin | TMP-SMX | TMP-SMX, levofloxacin |
| Site of infection | Blood | Blood, skin, muscle | Blood, genitals | Blood, CVC |
| Culture site | Peripheral blood | Peripheral blood | Peripheral blood | CVC |
| Clinical presentation | Severe sepsis | Necrotizing fasciitis | Fournier’s gangrene | Septic shock |
| Treatment | MER | C/T + COL + AMK + MER; surgery | C/T + COL + AMK + CLI; Surgery | C/T |
| Outcome | Alive | Alive (leg amputation) | Alive (plastic surgery) | Alive |
| MIC (µg/mL) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Strain (Source) | Sample | CAZ | FEP | IPM | MEM | TZP | CAZ/AVI | C/T | CST | GEN | AMK |
| B062 (Case #3) | Blood | 32 | >8 | <1 | 1 | >16 | 4 | <1 | 0.5 | >4 | 16 |
| BO48 (Case #4) | Blood | 16 | >8 | >8 | 16 | >16 | 4 | <1 | 0.5 | >4 | 16 |
| BO68 (Case #6) | Blood | 32 | >8 | >8 | 8 | >16 | 4 | <1 | 0.5 | >4 | <8 |
| BO93 (bidet) | Bidet filter | 32 | >8 | 8 | 16 | >16 | >8 | >16 | 0.5 | >4 | >16 |
| BO94 (bidet) | Bidet water | 32 | >8 | >8 | 16 | >16 | >8 | >16 | 0.5 | >4 | >16 |
| Strain (Source) | ST | Carbapenemase | Beta-Lactams | Amino-Glycosides | Fluoro-Quinolones | Sulfon-Amide | No. PhageRegions |
|---|---|---|---|---|---|---|---|
| B062 (Case #3) | 235 | blaOXA-488, blaPAO | aac(6′)-Ib3, aadA11, ant(2′′)-Ia, aph(3′)-IIb | aac(6′)-Ib-cr | sul1 | 9 | |
| BO48 (Case #4) | 175 | blaOXA-50, blaPAO, | ant(2′′)-Ia, aph(3’)-IIb | crpP | sul1 | 11 | |
| BO68 (Case #6) | 175 | blaOXA-50, blaPAO, | ant(2′′)-Ia, aph(3′)-Iib | crpP | sul1 | 11 | |
| BO93 (bidet) | 235 | blaVIM-1 | blaOXA-488, blaPAO | aac(6′)-Ib3, aadA1, aadA11, ant(2′′)-Ia, aph(3′)-IIb | aac(6′)-Ib-cr | sul1 | 12 |
| BO94 (bidet) | 235 | blaVIM-1 | blaOXA-488, blaPAO | Ib3, aadA1, aadA11, ant(2′′)-Ia, aph(3′)-IIb | aac(6′)-Ib-cr | sul1 | 12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coppola, P.E.; Gaibani, P.; Sartor, C.; Ambretti, S.; Lewis, R.E.; Sassi, C.; Pignatti, M.; Paolini, S.; Curti, A.; Castagnetti, F.; et al. Ceftolozane-Tazobactam Treatment of Hypervirulent Multidrug Resistant Pseudomonas aeruginosa Infections in Neutropenic Patients. Microorganisms 2020, 8, 2055. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8122055
Coppola PE, Gaibani P, Sartor C, Ambretti S, Lewis RE, Sassi C, Pignatti M, Paolini S, Curti A, Castagnetti F, et al. Ceftolozane-Tazobactam Treatment of Hypervirulent Multidrug Resistant Pseudomonas aeruginosa Infections in Neutropenic Patients. Microorganisms. 2020; 8(12):2055. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8122055
Chicago/Turabian StyleCoppola, Paolo E., Paolo Gaibani, Chiara Sartor, Simone Ambretti, Russell E. Lewis, Claudia Sassi, Marco Pignatti, Stefania Paolini, Antonio Curti, Fausto Castagnetti, and et al. 2020. "Ceftolozane-Tazobactam Treatment of Hypervirulent Multidrug Resistant Pseudomonas aeruginosa Infections in Neutropenic Patients" Microorganisms 8, no. 12: 2055. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8122055