
Post-COVID-19 Syndrome: Nine Months after SARS-CoV-2 Infection in a Cohort of 354 Patients: Data from the First Wave of COVID-19 in Nord Franche-Comté Hospital, France

 , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
3. Results
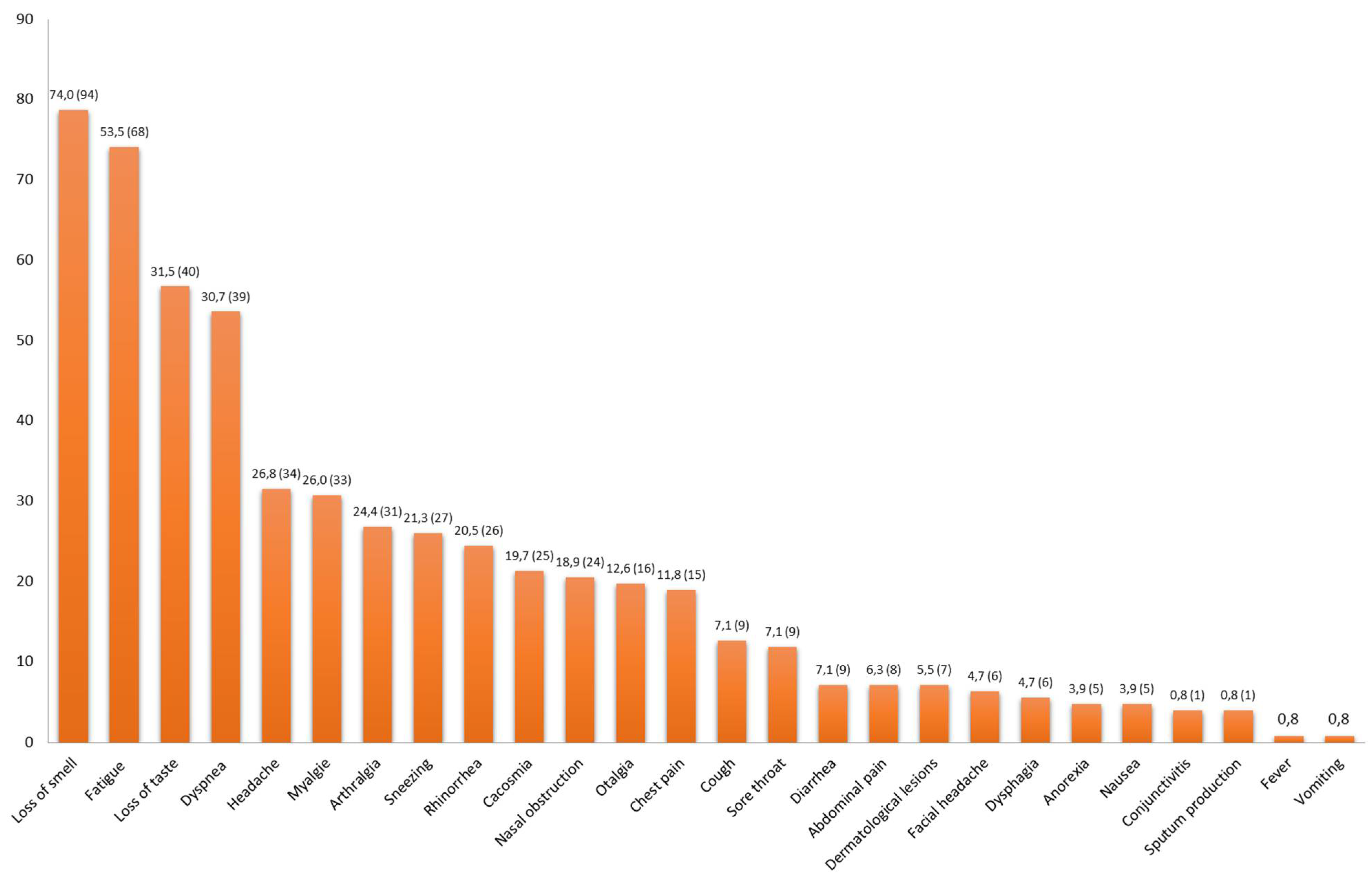
3.1. Description of Patients with Persistent Symptoms of COVID-19
3.2. Comparison of Two Groups (Table 2)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Armange, L.; Bénézit, F.; Picard, L.; Pronier, C.; Guillot, S.; Lentz, P.-A.; Carré, F.; Tattevin, P.; Revest, M. Prevalence and characteristics of persistent symptoms after non-severe COVID-19: A prospective cohort study. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2021, 1–5. [Google Scholar] [CrossRef]
- Petersen, M.S.; Kristiansen, M.F.; Hanusson, K.D.; Danielsen, M.E.; Steig, B.Á.; Gaini, S.; Strøm, M.; Weihe, P. Long COVID in the Faroe Islands: A Longitudinal Study among Nonhospitalized Patients. Clin. Infect. Dis. 2020, ciaa1792. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Osikomaiya, B.; Erinoso, O.; Wright, K.O.; Odusola, A.O.; Thomas, B.; Adeyemi, O.; Bowale, A.; Adejumo, O.; Falana, A.; Abdus-salam, I.; et al. “Long COVID”: Persistent COVID-19 symptoms in survivors managed in Lagos State, Nigeria. BMC Infect. Dis. 2021, 21, 304. [Google Scholar] [CrossRef]
- The Lancet Neurology. Long COVID: Understanding the neurological effects. Lancet Neurol. 2021, 20, 247. [Google Scholar] [CrossRef]
- Norton, A.; Olliaro, P.; Sigfrid, L.; Carson, G.; Paparella, G.; Hastie, C.; Kaushic, C.; Boily-Larouche, G.; Suett, J.C.; O’Hara, M. Long COVID: Tackling a multifaceted condition requires a multidisciplinary approach. Lancet Infect. Dis. 2021, 21, 601–602. [Google Scholar] [CrossRef]
- Coronavirus. National Guidance for Post-COVID Syndrome Assessment Clinics. Available online: https://www.england.nhs.uk/coronavirus/publication/national-guidance-for-post-covid-syndrome-assessment-clinics/ (accessed on 27 April 2021).
- Dennis, A.; Wamil, M.; Alberts, J.; Oben, J.; Cuthbertson, D.J.; Wootton, D.; Crooks, M.; Gabbay, M.; Brady, M.; Hishmeh, L.; et al. Multiorgan impairment in low-risk individuals with post-COVID-19 syndrome: A prospective, community-based study. BMJ Open 2021, 11, e048391. [Google Scholar]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute covid-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Pérez, O.; Merino, E.; Leon-Ramirez, J.-M.; Andres, M.; Ramos, J.M.; Arenas-Jiménez, J.; Asensio, S.; Sanchez, R.; Ruiz-Torregrosa, P.; Galan, I.; et al. Post-acute COVID-19 syndrome. Incidence and risk factors: A Mediterranean cohort study. J. Infect. 2021, 82, 378–383. [Google Scholar] [CrossRef]
- Peluso, M.J.; Kelly, J.D.; Lu, S.; Goldberg, S.A.; Davidson, M.C.; Mathur, S.; Durstenfeld, M.S.; Spinelli, M.A.; Hoh, R.; Tai, V.; et al. Rapid implementation of a cohort for the study of post-acute sequelae of SARS-CoV-2 infection/COVID-19. MedRxiv Prepr. Serv. Health Sci. 2021. [CrossRef]
- Leth, S.; Gunst, J.D.; Mathiasen, V.; Hansen, K.; Søgaard, O.; Østergaard, L.; Jensen-Fangel, S.; Storgaard, M.; Agergaard, J. Persistent Symptoms in Patients Recovering From COVID-19 in Denmark. Open Forum Infect. Dis. 2021, 8, ofab042. [Google Scholar] [CrossRef] [PubMed]
- Riestra-Ayora, J.; Yanes-Diaz, J.; Esteban-Sanchez, J.; Vaduva, C.; Molina-Quiros, C.; Larran-Jimenez, A.; Martin-Sanz, E. Long-term follow-up of olfactory and gustatory dysfunction in COVID-19: 6 months case-control study of health workers. Eur. Arch. Oto-Rhino-Laryngol. 2021, 1–7. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet Lond. Engl. 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Biguenet, A.; Bouiller, K.; Marty-Quinternet, S.; Brunel, A.-S.; Chirouze, C.; Lepiller, Q. SARS-CoV-2 respiratory viral loads and association with clinical and biological features. J. Med. Virol. 2021, 93, 1761–1765. [Google Scholar] [CrossRef] [PubMed]
- Meije, Y.; Duarte-Borges, A.; Sanz, X.; Clemente, M.; Ribera, A.; Ortega, L.; González-Pérez, R.; Cid, R.; Pareja, J.; Cantero, I.; et al. Long-term outcomes of patients following hospitalization for COVID-19: A prospective observational study. Clin. Microbiol. Infect. 2021, 27, 1151–1157. [Google Scholar] [CrossRef]
- Poenaru, S.; Abdallah, S.J.; Corrales-Medina, V.; Cowan, J. COVID-19 and post-infectious myalgic encephalomyelitis/chronic fatigue syndrome: A narrative review. Ther. Adv. Infect. Dis. 2021, 8. [Google Scholar] [CrossRef]
- McGroder, C.F.; Zhang, D.; Choudhury, M.A.; Salvatore, M.M.; D’Souza, B.M.; Hoffman, E.A.; Wei, Y.; Baldwin, M.R.; Garcia, C.K. Pulmonary fibrosis 4 months after COVID-19 is associated with severity of illness and blood leucocyte telomere length. Thorax 2021. [CrossRef]
- Fang, Y.; Zhou, J.; Ding, X.; Ling, G.; Yu, S. Pulmonary fibrosis in critical ill patients recovered from COVID-19 pneumonia: Preliminary experience. Am. J. Emerg. Med. 2020, 38, 2134–2138. [Google Scholar] [CrossRef]
- Czuba, C. Nouveaux tableaux de maladie professionnelle de la COVID-19: Vers une reconnaissance plus facilitée? Arch. Mal. Prof. Environ. 2021, 82, 45–49. [Google Scholar]
- Havervall, S.; Rosell, A.; Phillipson, M.; Mangsbo, S.M.; Nilsson, P.; Hober, S.; Thålin, C. Symptoms and Functional Impairment Assessed 8 Months After Mild COVID-19 among Health Care Workers. JAMA 2021, 325, 2015–2016. [Google Scholar] [CrossRef] [PubMed]
- Zayet, S.; Royer, P.-Y.; Toko, L.; Pierron, A.; Gendrin, V.; Klopfenstein, T. Recurrence of COVID-19 after recovery ? A case series in health care workers, France. Microbes Infect. 2021, 23, 104803. [Google Scholar] [CrossRef]
- Zayet, S.; Royer, P.-Y.; Toko, L.; Pierron, A.; Gendrin, V.; Klopfenstein, T. Prolonged COVID 19 Outbreak and Psychological Response of Nurses in Italian Healthcare System: Cross-Sectional Study. Front. Psychol. 2021, 12, 608413. [Google Scholar]
- Klopfenstein, T.; Kadiane-Oussou, N.; Toko, L.; Royer, P.-Y.; Lepiller, Q.; Gendrin, V.; Zayet, S. Features of anosmia in COVID-19. Med. Mal. Infect. 2020, 50, 436–439. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Bangash, M.N.; Owen, A.; Alderman, J.E.; Chotalia, M.; Patel, J.M.; Parekh, D. COVID-19 recovery: Potential treatments for post-intensive care syndrome. Lancet Respir. Med. 2020, 8, 1071–1073. [Google Scholar] [CrossRef]
- Martillo, M.A.; Dangayach, N.S.; Tabacof, L.; Spielman, L.A.; Dams-O’Connor, K.; Chan, C.C.; Kohli-Seth, R.; Cortes, M.; Escalon, M.X. Postintensive Care Syndrome in Survivors of Critical Illness Related to Coronavirus Disease 2019: Cohort Study From a New York City Critical Care Recovery Clinic. Crit. Care Med. 2021. [CrossRef]
- Sehgal, K.; Fadel, H.J.; Tande, A.J.; Pardi, D.S.; Khanna, S. Outcomes in Patients with SARS-CoV-2 and Clostridioides difficile Coinfection. Infect. Drug Resist. 2021, 14, 1645–1648. [Google Scholar] [CrossRef] [PubMed]
- Chotpitayasunondh, T.; Fischer, T.K.; Heraud, J.-M.; Hurt, A.C.; Monto, A.S.; Osterhaus, A.; Shu, Y.; Tam, J.S. Influenza and COVID-19: What does co-existence mean? Influenza Other Respir. Viruses 2021, 15, 407–412. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No-PS Group (n = 227) | PS Group (n = 127) | Total (n = 354) | p-Value | |||
|---|---|---|---|---|---|---|
| (64.1%) | (35.9%) | (100%) | ||||
| Demographic and baseline characteristics | ||||||
| Age, years (mean, extremes, SD) | 50.1 (19–98) ± 18.4 | 48.6 (19–93) ± 19.4 | 49.6 (19–98) ± 18.7 | 0.472 | ||
| (18–30) | 41 (18.1) | 30 (23.6) | 71 (20.1) | 0.210 | ||
| (31–40) | 32 (14.1) | 18 (14.2) | 50 (14.1) | 0.984 | ||
| (41–50) | 50 (22) | 23 (18.1) | 73 (20.6) | 0.382 | ||
| (51–60) | 46 (20.3) | 19 (15) | 65 (18.4) | 0.216 | ||
| (61–70) | 20 (8.8) | 20 (15.7) | 40 (11.3) | 0.048 | ||
| (71–80) | 22 (9.7) | 8 (6.3) | 30 (8.5) | 0.272 | ||
| (81–90) | 12 (5.3) | 8 (6.3) | 20 (5.6) | 0.692 | ||
| >90 | 4 (1.8) | 1 (0.8) | 5 (1.4) | 0.411 | ||
| Sex (Number, %) | Male | 85 (37.4) | 46 (36.2) | 131 (37.0) | 0.819 | |
| Female | 142 (62.6) | 81 (63.8) | 223 (63.0) | 0.819 | ||
| HCWs (Number, %) | Total | 112 (49.3) | 73 (57.5) | 185 (52.3) | 0.141 | |
| Inpatients | 3/76 (3.9) | 2/45 (4.4) | 5/121 (4.1) | 0.617 | ||
| Outpatients | 109/151 (72.2) | 71/82 (86.6) | 180/233 (77.3) | 0.012 | ||
| BMI (kg/m2) | Total (mean, extremes, SD) | 26.7 (15.9–43.2) ± 5.3 | 26.3 (16.6–47) ± 5.4 | 26.5. (15.9–47) ± 5.3 | 0.472 | |
| <18.5 | 6 (2.7) | 6 (4.7) | 12(3.4) | 0.234 | ||
| (18.5–25) | 92 (40.9) | 52 (40.9) | 144 (40.9) | 0.992 | ||
| (25–30) | 74 (32.9) | 40 (31.5) | 114 (32.4) | 0.780 | ||
| >30 | 53 (23.6) | 29 (22.8) | 82 (23.3) | 0.878 | ||
| Pregnancy (Number, %) | 1 (0.4) | 3 (2.4) | 4 (1.1) | 0.101 | ||
| Current smoking (Number, %) | 29 (12.8) | 12 (9.4) | 41 (11.6) | 0.348 | ||
| Comorbidities (Number, %) | No | 93 (41) | 49 (38.6) | 142 (40.1) | 0.660 | |
| Cardio-vascular diseases (Number, %) | Total | 71 (31.3) | 28 (22) | 99 (28) | 0.060 | |
| Arterial hypertension | 48 (21.1) | 21 (16.5) | 69 (19.5) | 0.294 | ||
| Heart failure | 12 (5.3) | 2 (1.6) | 14 (4) | 0.086 | ||
| Others 1 | 18 (7.9) | 7 (5.5) | 25 (7.1) | 0.394 | ||
| Diabetes mellitus | 18 (7.9) | 6 (4.7) | 24 (6.8) | 0.250 | ||
| Chronic kidney failure (Number, %) | 6 (2.6) | 3 (2.4) | 9 (2.9) | 0.872 | ||
| Neurologic diseases (Number, %) | 15 (6.6) | 6 (4.7) | 21 (5.9) | 0.472 | ||
| Psychiatric disorders (Number, %) | Depressive disorders | 10 (4.4) | 8 (6.3) | 18 (5.1) | 0.437 | |
| Others 2 | 2 (0.9) | 0 (0) | 2 (0.6) | 0.411 | ||
| Malignancy (Number, %) | Past history of malignancy | 20 (8.8) | 10 (7.9) | 30 (8.5) | 0.762 | |
| Treated actually | 2 (0.9) | 2 (1.6) | 4 (1.1) | 0.453 | ||
| Respiratory diseases (Number, %) | Total | 38 (16.5) | 27 (21.3) | 66 (18.6) | 0.345 | |
| COPD | 7 (3.1) | 2 (1.6) | 9 (2.5) | 0.314 | ||
| Asthma | 26 (11.5) | 19 (15) | 45 (12.7) | 0.342 | ||
| Others 3 | 5 (2.2) | 5 (3.9) | 10 (2.8) | 0.266 | ||
| ENT diseases (Number, %) | Total | 48 (21.1) | 32 (25.2) | 80 (22.6) | 0.382 | |
| Rhinosinusitis nasal polyps | 2 (0.9) | 3 (2.4) | 5 (1.4) | 0.248 | ||
| Surgical rhinoplasty | 5 (2.2) | 4 (3.1) | 9 (2.9) | 0.413 | ||
| Allergic rhinitis | 40 (17.6) | 19 (15) | 59 (16.7) | 0.519 | ||
| Chronic rhinosinusitis | 3 (1.3) | 11 (8.7) | 14 (4) | <0.001 | ||
| Clinical characteristics and outcome, laboratory and imaging findings | ||||||
| Duration of symptoms of SARS-CoV-2 infection (days) (mean, extremes, SD) | 29.7 (1–283) ± 42.1 | 57.1 (0–335) ± 82.1 | 39.1 (0–335) ± 60.2 | <0.001 | ||
| Crackling Sounds heard on pulmonary auscultation (Number, %) | 56/76 (73.7) | 33/45 (73.3) | 89/121 (73.6) | 0.966 | ||
| Hospitalization (Number, %) | 76 (33.5) | 45 (35.4) | 121 (34.2) | 0.710 | ||
| Duration of hospitalization (days) (mean, extremes, SD) | 14.2 (1–128) ± 20.6 | 11.5 (1–45) ± 10.5 | 13.2 (1–128) ± 17.6 | 0.415 | ||
| Transferred to ICU (Number, %) | 13/76 (17.1) | 5/45 (11.1) | 18/121 (14.9) | 0.371 | ||
| Mechanical ventilation (Number, %) | 13/76 (17.1) | 5/45 (11.1) | 18/121 14.9) | 0.371 | ||
| Laboratory data on admission (mean, extremes, DS) in hospitalized patients | White-cell count/mm3 (4000–10,000/mm3) | 7795 (2660–23,950) ± 3.4 | 7161 (2790–13,340) ± 2.5 | 7561 (2660–23,950) ± 3.5 | 0.344 | |
| Lymphocytes/mm3 (1500–4000/mm3) | 0.889 (0.210–2.380) ± 0.4 | 0.950 (0.150–2.700) ± 0.5 | 0.911 (0.150–2700) ± 0.5 | 0.485 | ||
| Hemoglobin, g/dL (13.5–17.5 g/dL) | 13.9 (10.9–18.2) ± 1.5 | 13.5 (10.4–19.1) ± 1.8 | 13.8 (10.4–19.1) ± 1.6 | 0.208 | ||
| Creatinine, μmol/L (65–120 μmol/L) | 83.2 (46–403) ± 48.5 | 77.2 (43–139) ± 20.9 | 81.0 (43–403) ± 40.5 | 0.434 | ||
| Alanine aminotransferase, U/L (8–45 U/L) | 53.0 (12–230) ± 43.7 | 53.5 (12–175) ± 46.6 | 53.2 (12–230) ± 44.5 | 0.964 | ||
| Aspartate aminotransferase, U/L (10–40 U/L) | 56.5 (11–292) ± 45.0 | 53.9 (11–193) ± 41.5 | 55.6 (11–292) ± 43.6 | 0.767 | ||
| D-dimer, ng/mL (<500 ng/mL) | 1695 (<500–34905) | 2169 (<500–58190) | 1871 (<500–58190] | 0.719 | ||
| C-reactive protein (CRP), mg/L | 121.1 (1–478) ± 94.2 | 117.2 (1–490) ± 96.6 | 119.6 (1–490) ± 94.7 | 0.828 | ||
| CRP >100mg/L (Number, %) | 37/76 (48.7) | 23/45 (51.1) | 60/121 (49.6) | 0.769 | ||
| RT-PCR SARS-CoV-2 CT (mean, extremes, SD) | 27.0 (16.4–37.6) ± 5.4 | 27.2 (17.3–34.2) ± 5.3 | 27.1 (16.4–37.6) ± 5.3 | 0.901 | ||
| Radiologic data | Thoracic imaging features | GGO | 58/60 (96.7) | 30/32 (93.8) | 88/92 (95.7) | 0.434 |
| Consolidation opacities | 45/60 (75) | 22/32 (68.8) | 67/92 (72.8) | 0.521 | ||
| Crazy-paving sign | 28/60 (46.7) | 13/32 (40.6) | 41/92 (44.6) | 0.579 | ||
| Extension < 25% | 30/60 (50.0) | 14/32 (43.8) | 44/92 (47.8) | 0.568 | ||
| Extension >50% | 8/60 (13.3) | 3/32 (9.4) | 11/92 (12.0) | 0.424 | ||
| Treatment received | ||||||
| Antibiotics * | 64/76 (84.2) | 35/45 (77.8) | 99/121 (81.8) | 0.375 | ||
| Hydroxychloroquine | 51/76 (67.1) | 26/45 (57.8) | 77/121 (63.6) | 0.303 | ||
| Lopinavir/Ritonavir | 5/76 (6.6) | 2/45 (4.4) | 7/121 (5.8) | 0.480 | ||
| Steroids (Dexamethasone) | 11/76 (14.5) | 6/45 (13.3) | 17/121 (14.0) | 0.862 | ||
| Anti-IL-6 (Tocilizumab) | 3/76 (3.9) | 3/45 (6.7) | 6/121 (5.0) | 0.396 | ||
| Persistent Symptoms (Number) | Number of Patients with Persistent Symptoms (%) | Duration of SARS-CoV-2 Acute Infection (Mean, Extremes, SD), Days |
|---|---|---|
| 1 | 7 (5.5) | 13.5 (7–19) ± 5 |
| 2 | 16 (12.6) | 59.9 (8–279) ± 86.3 |
| 3 | 36 (28.3) | 55.5 (7–303) ± 85.4 |
| 4 | 24 (18.9) | 37.4 (10–119) ± 25.8 |
| >5 | 44 (34.6) | 90.3 (9–335) ± 103.0 |
| Total | 127 (100) | 43.8 (7–335) ± 62.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zayet, S.; Zahra, H.; Royer, P.-Y.; Tipirdamaz, C.; Mercier, J.; Gendrin, V.; Lepiller, Q.; Marty-Quinternet, S.; Osman, M.; Belfeki, N.; et al. Post-COVID-19 Syndrome: Nine Months after SARS-CoV-2 Infection in a Cohort of 354 Patients: Data from the First Wave of COVID-19 in Nord Franche-Comté Hospital, France. Microorganisms 2021, 9, 1719. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9081719
Zayet S, Zahra H, Royer P-Y, Tipirdamaz C, Mercier J, Gendrin V, Lepiller Q, Marty-Quinternet S, Osman M, Belfeki N, et al. Post-COVID-19 Syndrome: Nine Months after SARS-CoV-2 Infection in a Cohort of 354 Patients: Data from the First Wave of COVID-19 in Nord Franche-Comté Hospital, France. Microorganisms. 2021; 9(8):1719. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9081719
Chicago/Turabian StyleZayet, Souheil, Hajer Zahra, Pierre-Yves Royer, Can Tipirdamaz, Julien Mercier, Vincent Gendrin, Quentin Lepiller, Solène Marty-Quinternet, Molka Osman, Nabil Belfeki, and et al. 2021. "Post-COVID-19 Syndrome: Nine Months after SARS-CoV-2 Infection in a Cohort of 354 Patients: Data from the First Wave of COVID-19 in Nord Franche-Comté Hospital, France" Microorganisms 9, no. 8: 1719. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9081719