Physicochemical Compatibility and Stability of Linezolid with Parenteral Nutrition

 ,
,  ,
,  ,
, 
Abstract
: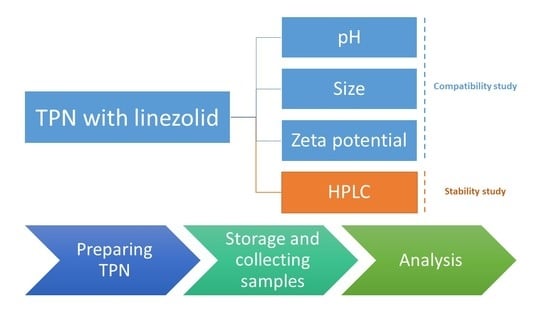
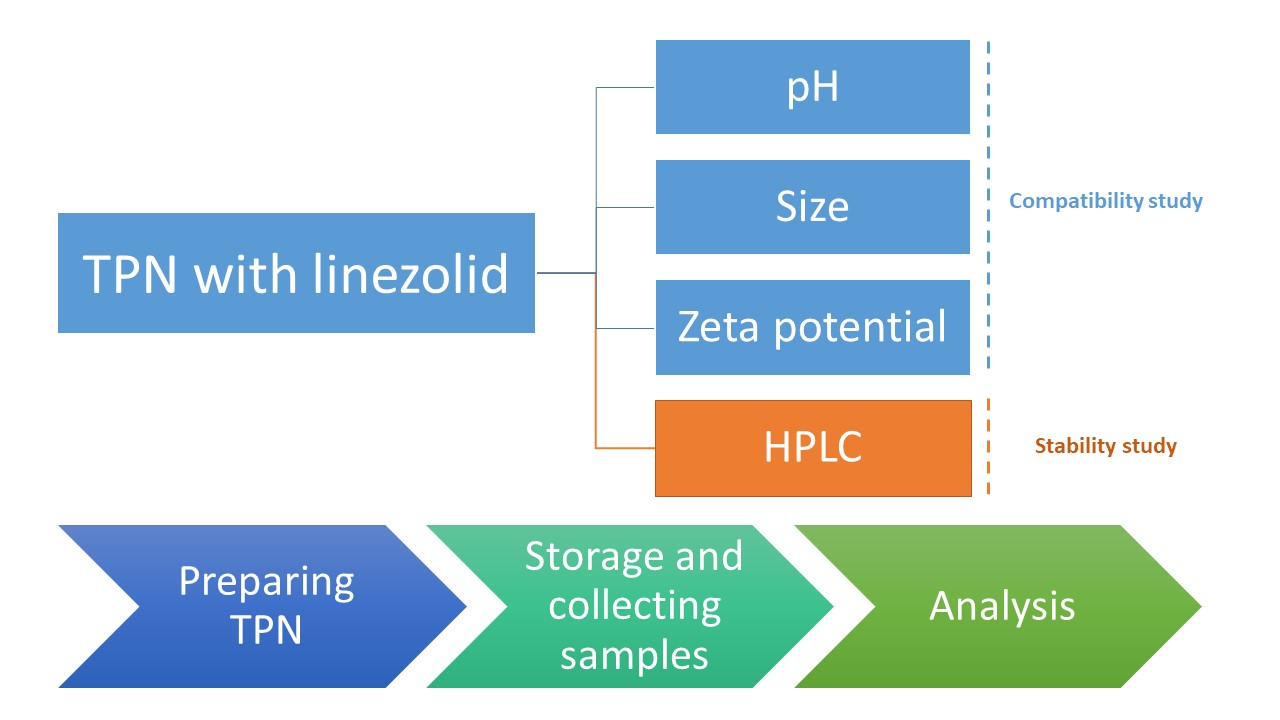
1. Introduction
2. Results and Discussion
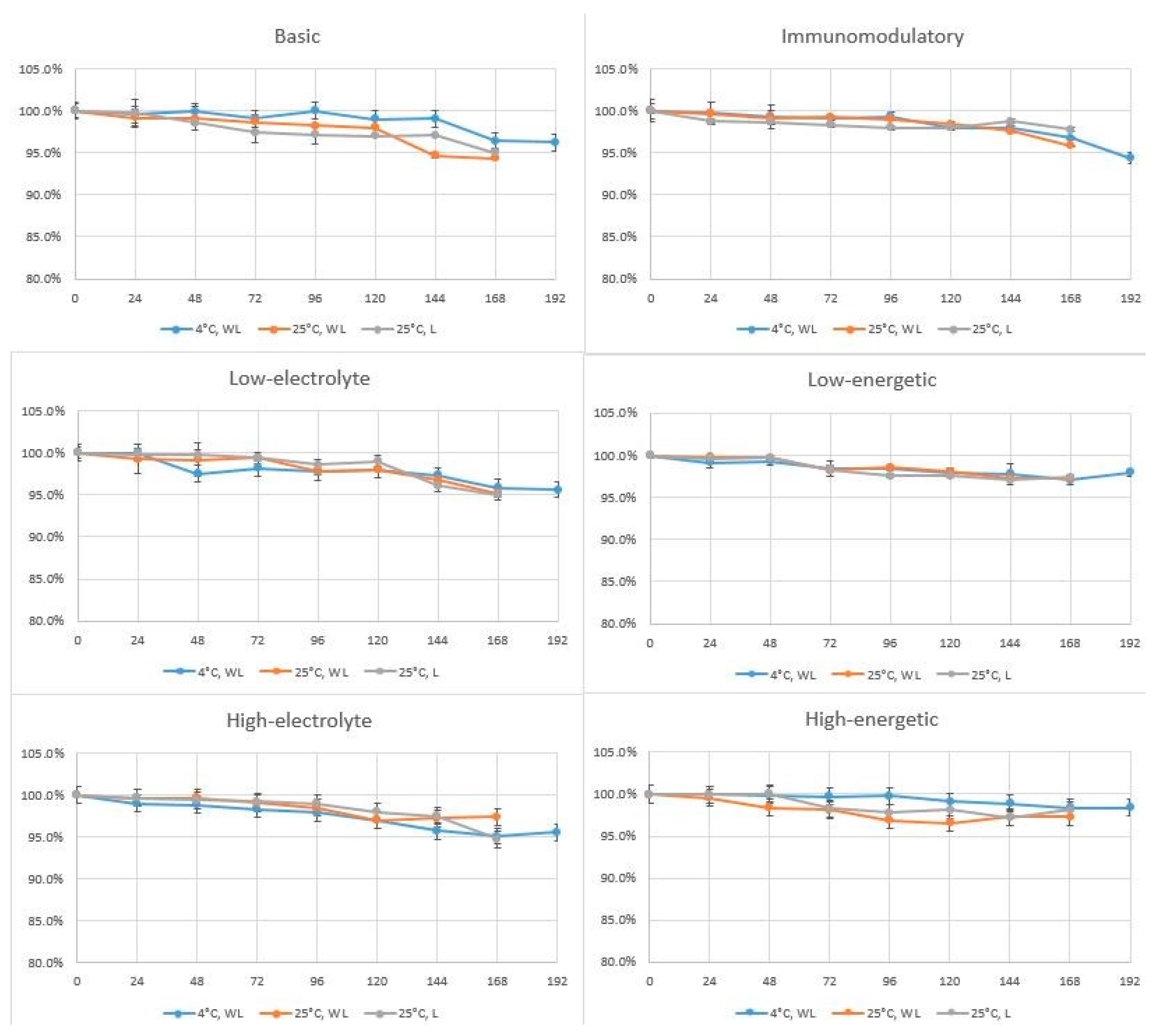
2.1. Linezolid Determination in TPN Mixtures
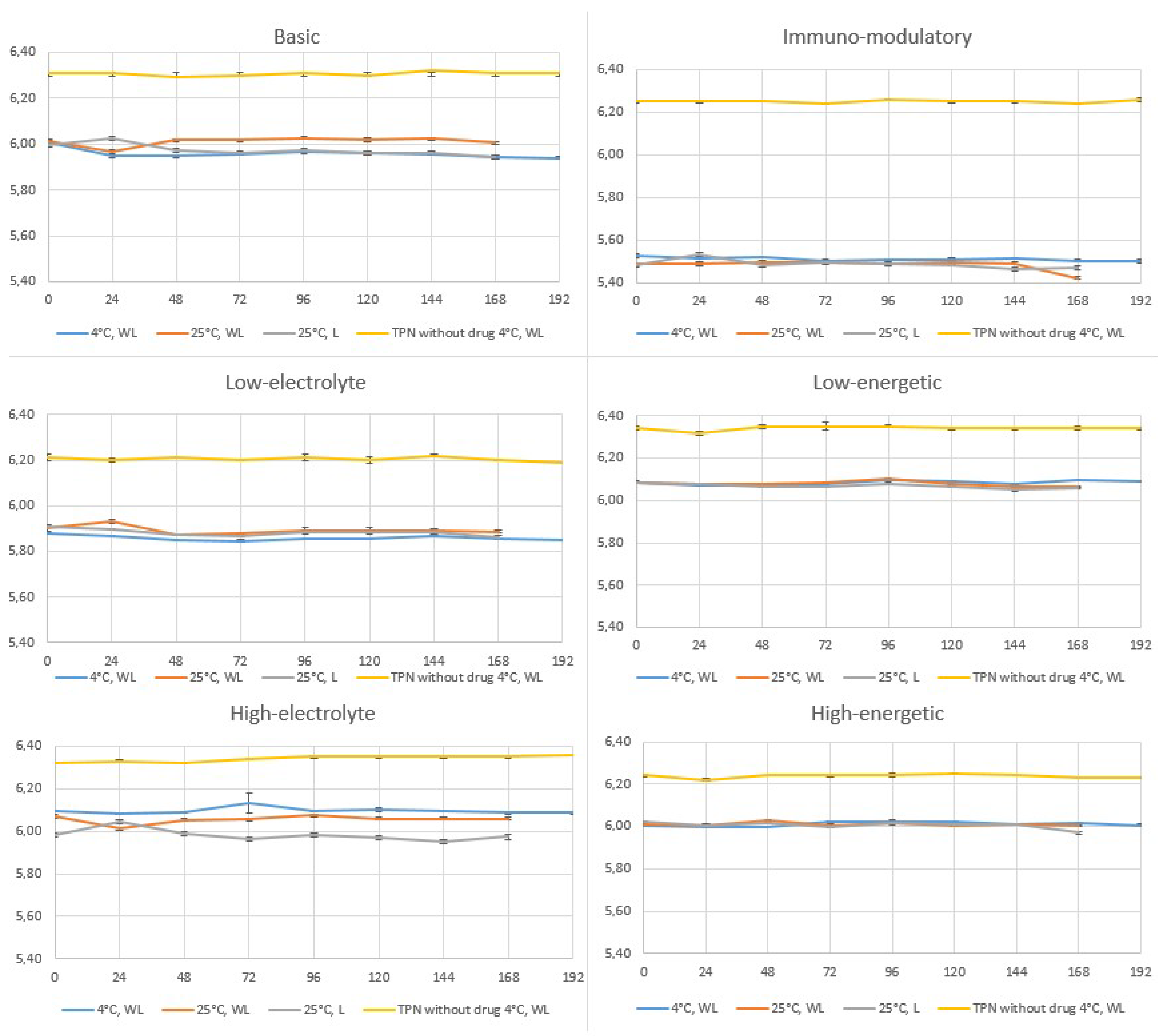
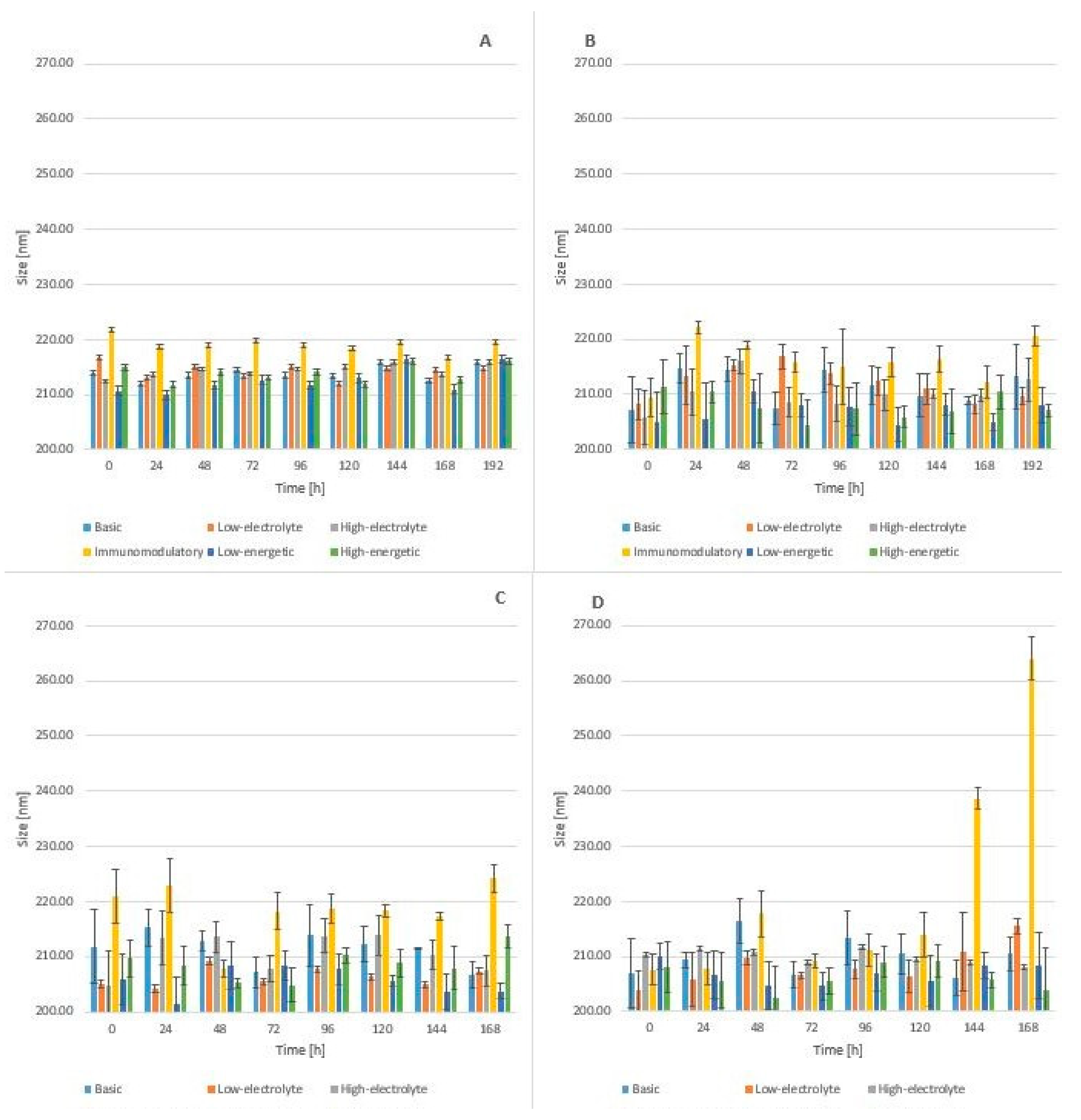
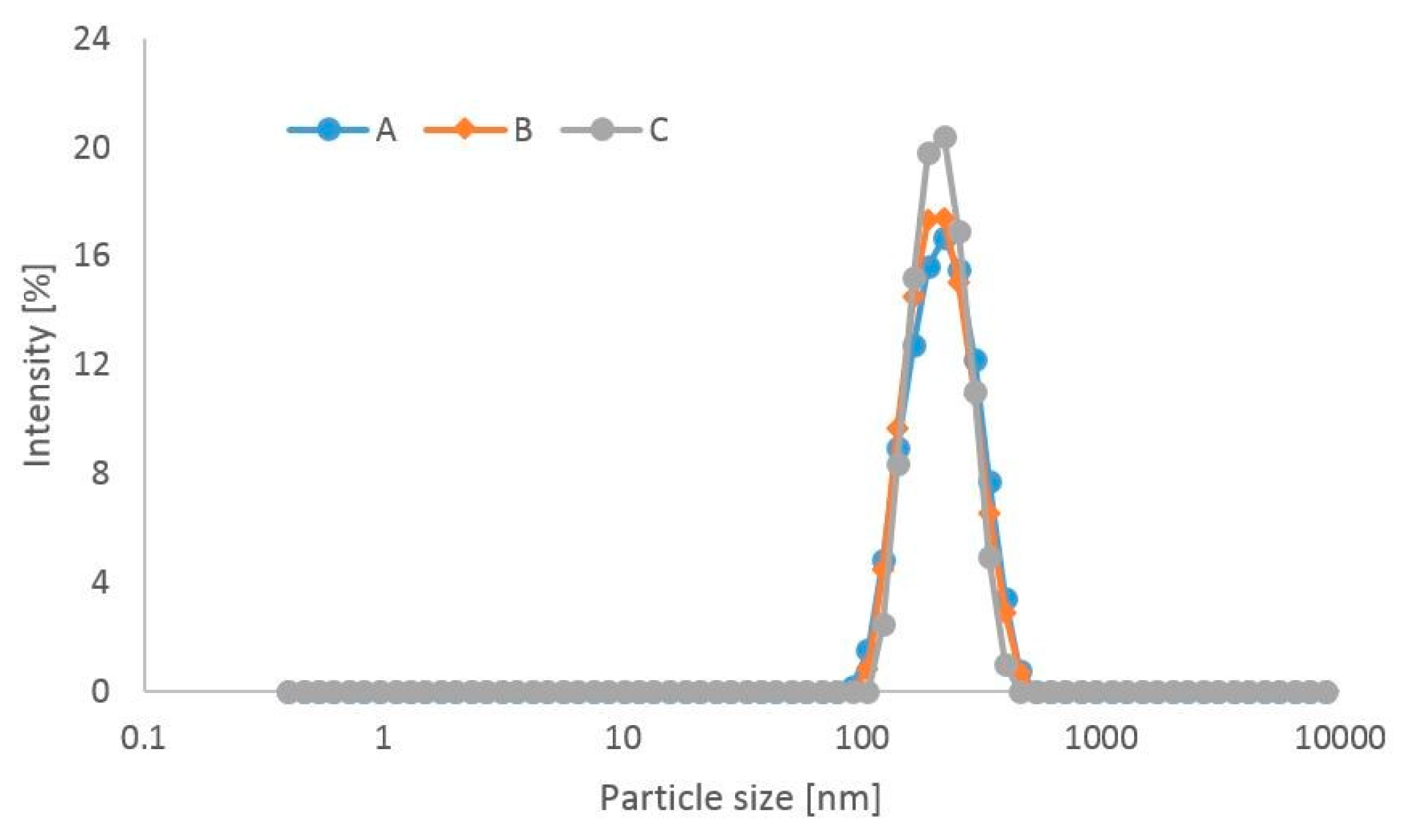
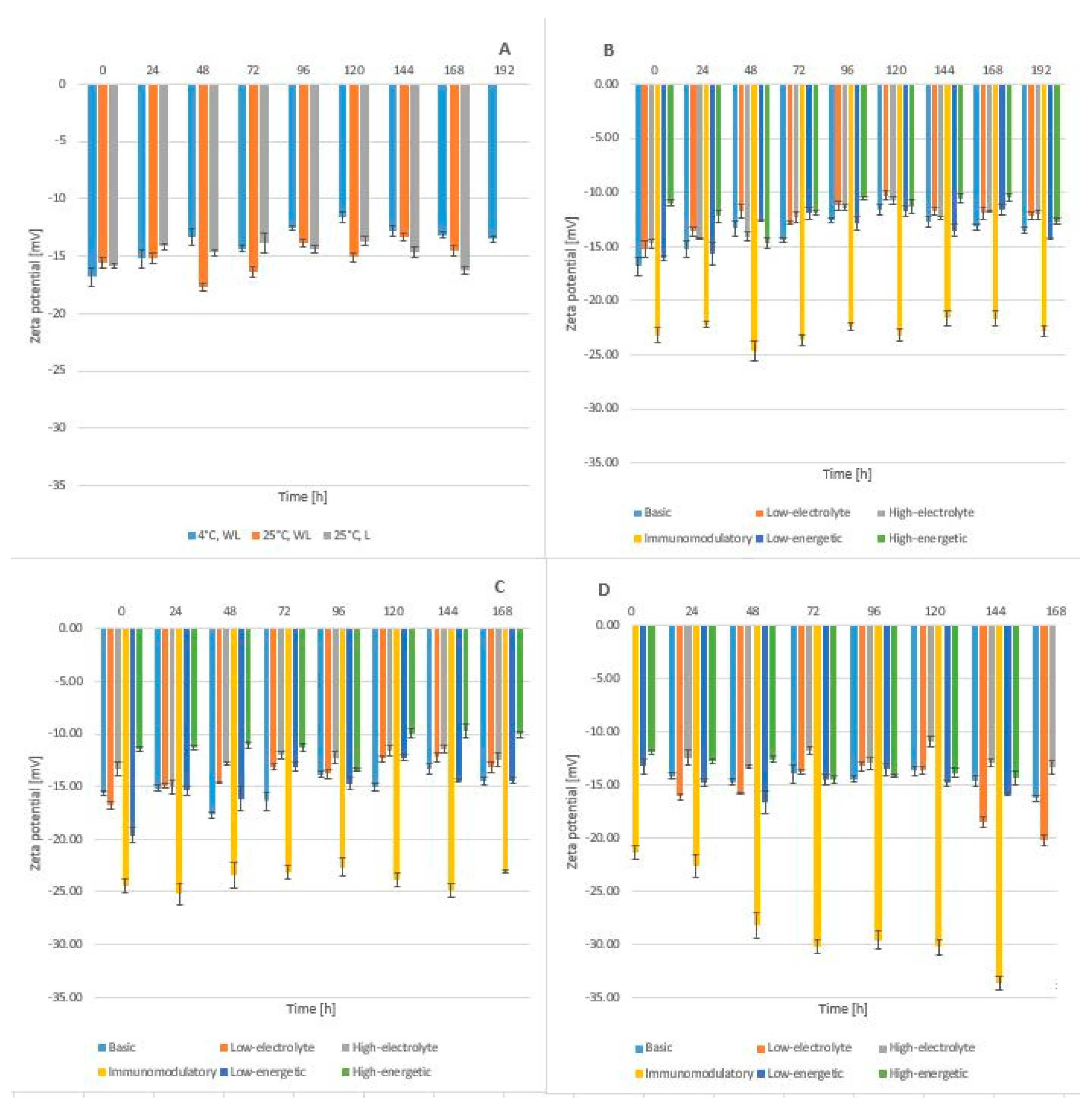
2.2. Compatibility Studies
3. Materials and Methods
3.1. Materials
3.2. Reagents
3.3. Preparation of Total Parenteral Nutrition Mixtures
3.4. Preparation of TPN Mixtures with Linezolid
3.5. Extraction of Linezolid from TPN Mixtures for HPLC Analysis
3.5.1. HPLC Analysis
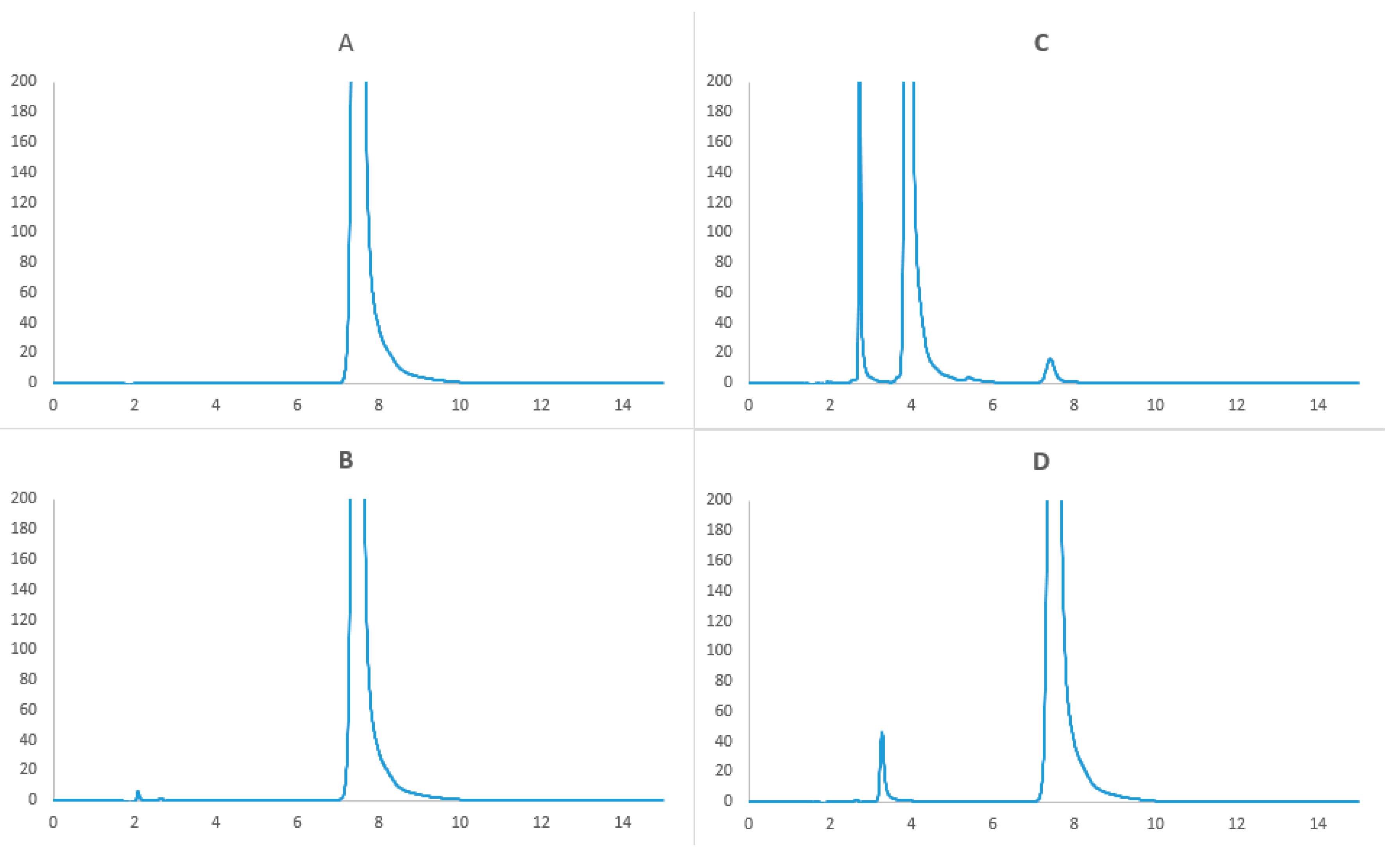
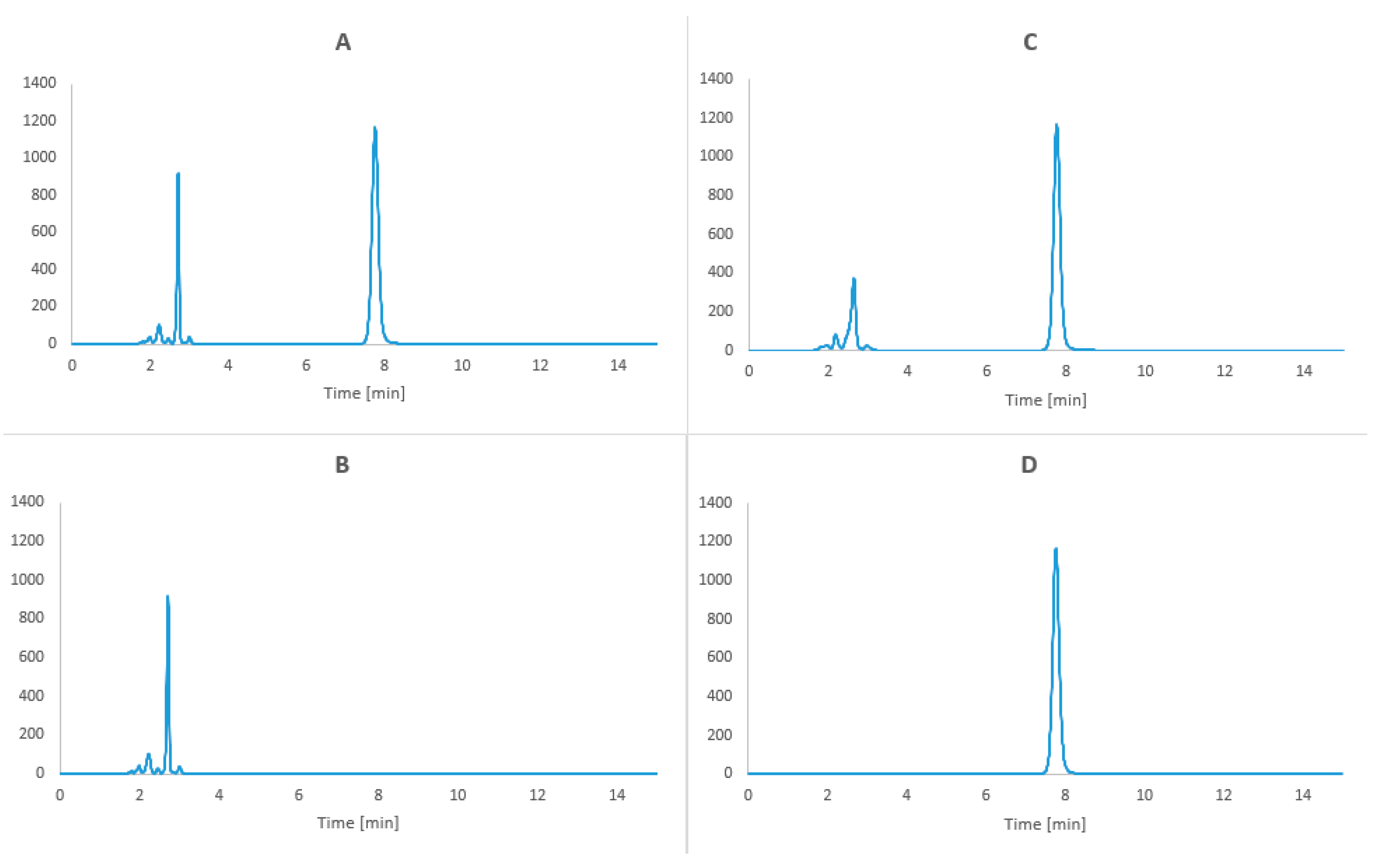
3.5.2. Forced Degradation Study
3.5.3. Selectivity
3.5.4. Linearity
3.5.5. Precision and Repeatability
3.5.6. Detection and Quantitation Limits
3.5.7. Range
3.5.8. pH Measurement
3.5.9. Particle Size Measurements
3.5.10. Zeta Potential Measurements
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ziegler, T.R. Parenteral Nutrition in the Critically Ill Patient. New Engl. J. Med. 2009, 361, 1088–1097. [Google Scholar] [CrossRef]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef] [PubMed]
- Preiser, J.-C.; Ichai, C.; Orban, J.-C.; Groeneveld, A.B.J. Metabolic response to the stress of critical illness. Br. J. Anaesth. 2014, 113, 945–954. [Google Scholar] [CrossRef]
- Vanhorebeek, I.; Van den Berghe, G. Hormonal and metabolic strategies to attenuate catabolism in critically ill patients. Curr. Opin. Pharmacol. 2004, 4, 621–628. [Google Scholar] [CrossRef]
- Puthucheary, Z.A.; Rawal, J.; McPhail, M.; Connolly, B.; Ratnayake, G.; Chan, P.; Hopkinson, N.S.; Padhke, R.; Dew, T.; Sidhu, P.S.; et al. Acute Skeletal Muscle Wasting in Critical Illness. JAMA 2013, 310, 1591–1600. [Google Scholar] [CrossRef]
- Mogensen, K.M.; Robinson, M.K.; Casey, J.D.; Gunasekera, N.S.; Moromizato, T.; Rawn, J.D.; Christopher, K.B. Nutritional Status and Mortality in the Critically Ill*. Crit. Care Med. 2015, 43, 2605–2615. [Google Scholar] [CrossRef] [PubMed]
- Ridley, E.J.; Davies, A.R.; Parke, R.; Bailey, M.; McArthur, C.; Gillanders, L.; Cooper, D.J.; McGuinness, S.; Cooper, D.J. Supplemental parenteral nutrition in critically ill patients: A study protocol for a phase II randomised controlled trial. Trials 2015, 16, 587. [Google Scholar] [CrossRef] [PubMed]
- Bozzetti, F.; Arends, J.; Lundholm, K.; Micklewright, A.; Zürcher, G.; Muscaritoli, M. ESPEN Guidelines on Parenteral Nutrition: Non-surgical oncology. Clin. Nutr. 2009, 28, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Messing, B.; Joly, F. Guidelines for Management of Home Parenteral Support in Adult Chronic Intestinal Failure Patients. Gastroenterology 2006, 130, S43–S51. [Google Scholar] [CrossRef] [PubMed]
- Allwood, M.C. Pharmaceutical aspects of parenteral nutrition: From now to the future. Nutrition 2000, 16, 615–618. [Google Scholar] [CrossRef]
- Barnett, M.I.; Cosslett, A.G.; Duffield, J.R.; Evans, D.A.; Hall, S.B.; Williams, D.R. Parenteral Nutrition. Drug Saf. 1990, 5, 101–106. [Google Scholar] [CrossRef]
- Maudar, K. TOTAL PARENTERAL NUTRITION. Med J. Forces 2017, 51, 122–126. [Google Scholar] [CrossRef]
- Stawny, M.; Olijarczyk, R.; Jaroszkiewicz, E.; Jelińska, A.; Jeliń Ska, A. Pharmaceutical Point of View on Parenteral Nutrition. Sci. J. 2013, 2013, 415310. [Google Scholar] [CrossRef]
- Billion-Rey, F.; Guillaumont, M.; Frederich, A.; Aulagner, G. Stability of Fat-Soluble Vitamins A (Retinol Palmitate), E (Tocopherol Acetate), and K1 (Phylloquinone) in Total Parenteral Nutrition at Home. J. Parenter. Enter. Nutr. 1993, 17, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Wade, C.S.; Lampasona, V.; Mullins, R.E.; Parks, R.B. Stability of ceftazidime and amino acids in parenteral nutrient solutions. Am. J. Heal. Pharm. 1991, 48, 1515–1519. [Google Scholar] [CrossRef]
- Driscoll, D.F. Stability and compatibility assessment techniques for total parenteral nutrition admixtures: Setting the bar according to pharmacopeial standards. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, O.; Alvarez, F.; Oltra, R.; Cereijo, E.; Latorre, M.M.; Martínez, H. Use of linezolid in critically ill patients admitted to intensive care units. Rev. Esp. Quimioter. 2009, 22, 68–75. [Google Scholar] [PubMed]
- Sirvent, J.-M.; Piñeiro, L.; De La Torre, M.; Motjé, M.; De Batlle, J.; Bonet, A. Linezolid more efficacious than vancomycin to eradicate infecting organism in critically ill patients with Gram-positive infections. Rev. Esp. Quimioter. 2010, 23, 27–35. [Google Scholar]
- Cepeda, J.A.; Whitehouse, T.; Cooper, B.; Hails, J.; Jones, K.; Kwaku, F.; Taylor, L.; Hayman, S.; Shaw, S.; Kibbler, C.; et al. Linezolid versus teicoplanin in the treatment of Gram-positive infections in the critically ill: A randomized, double-blind, multicentre study. J. Antimicrob. Chemother. 2004, 53, 345–355. [Google Scholar] [CrossRef]
- Hashemian, S.M.R.; Farhadi, T.; Ganjparvar, M. Linezolid: A review of its properties, function, and use in critical care. Drug Des. Dev. Ther. 2018, 12, 1759–1767. [Google Scholar] [CrossRef]
- Krueger, W.A.; Unertl, K.E. Neue Therapieoption für Intensivpatienten mit Infektionen durch Gram-positive Bakterien - Überblick über Linezolid. Anästhesiol Intensivmed Notfallmed Schmerzther 2002, 37, 199–204. [Google Scholar] [CrossRef]
- Barbachyn, M.R.; Ford, C.W. Oxazolidinone Structure–Activity Relationships Leading to Linezolid. Angew. Chem. Int. Ed. 2003, 42, 2010–2023. [Google Scholar] [CrossRef] [PubMed]
- Mendes, R.E.; Deshpande, L.M.; Jones, R.N. Linezolid update: Stable in vitro activity following more than a decade of clinical use and summary of associated resistance mechanisms. Drug Resist. Updat. 2014, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Shaw, K.J.; Barbachyn, M.R. The oxazolidinones: Past, present, and future. Ann. N. Y. Acad. Sci. 2011, 1241, 48–70. [Google Scholar] [CrossRef] [PubMed]
- McKee, E.E.; Ferguson, M.; Bentley, A.T.; Marks, T.A. Inhibition of Mammalian Mitochondrial Protein Synthesis by Oxazolidinones. Antimicrob. Agents Chemother. 2006, 50, 2042–2049. [Google Scholar] [CrossRef]
- Wilson, D.; Schluenzen, F.; Harms, J.M.; Starosta, A.L.; Connell, S.R.; Fucini, P. The oxazolidinone antibiotics perturb the ribosomal peptidyl-transferase center and effect tRNA positioning. Proc. Natl. Acad. Sci. USA 2008, 105, 13339–13344. [Google Scholar] [CrossRef]
- Locke, J.B.; Finn, J.; Hilgers, M.; Morales, G.; Rahawi, S.; C., K.G.; Picazo, J.J.; Im, W.; Shaw, K.J.; Stein, J.L. Structure-Activity Relationships of Diverse Oxazolidinones for Linezolid-Resistant Staphylococcus aureus Strains Possessing the cfr Methyltransferase Gene or Ribosomal Mutations. Antimicrob. Agents Chemother. 2010, 54, 5337–5343. [Google Scholar] [CrossRef]
- Beringer, P.; Nguyen, M.; Hoem, N.; Louie, S.; Gill, M.; Gurevitch, M.; Wong-Beringer, A. Absolute Bioavailability and Pharmacokinetics of Linezolid in Hospitalized Patients Given Enteral Feedings. Antimicrob. Agents Chemother. 2005, 49, 3676–3681. [Google Scholar] [CrossRef]
- Narayana, C.L.; Suresh, T.; Rao, S.M.; Dubey, P.; Babu, J.M. A validated chiral HPLC method for the enantiomeric separation of Linezolid on amylose based stationary phase. J. Pharm. Biomed. Anal. 2003, 32, 21–28. [Google Scholar] [CrossRef]
- Belal, F.F.; El-Din, M.K.S.; Eid, M.I.; El-Gamal, R.M. Micellar HPLC method using monolithic column for the simultaneous determination of linezolid and rifampicin in pharmaceuticals and biological fluids. Anal. Methods 2013, 5, 6165. [Google Scholar] [CrossRef]
- Cios, A.; Kuś, K.; Szymura-Oleksiak, J. Determination of linezolid in human serum by reversed-phase high-performance liquid chromatography with ultraviolet and diode array detection. Pol. Pharm. Drug Res. 2013, 70, 631–641. [Google Scholar]
- Agrawal, H.; Mahadik, K.R.; Paradkar, A.R.; Kaul, N. Stability Indicating HPTLC Determination of Linezolid as Bulk Drug and in Pharmaceutical Dosage Form. Drug Dev. Ind. Pharm. 2003, 29, 1119–1126. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Patel, P.; Patel, N.; Patel, M.; Bangoriya, U. High Performance Thin Layer Chromatographic Method for Estimation of Linezolid in Tablets. J. Pharm. Sci. 2007, 69, 571. [Google Scholar] [CrossRef]
- Michalska, K.; Pajchel, G.; Tyski, S. Determination of linezolid and its achiral impurities using sweeping preconcentration by micellar capillary electrophoresis. J. Pharm. Biomed. Anal. 2008, 48, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.; Sunderland, B.; Luna, G.; Czarniak, P. Evaluation of the stability of linezolid in aqueous solution and commonly used intravenous fluids. Drug Des. Dev. Ther. 2017, 11, 2087–2097. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug Administration. Drug Approval Package. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2000/21130_Zyvox.cfm (accessed on 20 October 2018).
- Dryden, M.S. Linezolid pharmacokinetics and pharmacodynamics in clinical treatment. J. Antimicrob. Chemother. 2011, 66, iv7–iv15. [Google Scholar] [CrossRef]
- Mimoz, O.; Montravers, P.; Paiva, J.-A. Continuous administration of linezolid in pneumonia: What is the level of proof? Intensiv. Care Med. 2014, 41, 157–159. [Google Scholar] [CrossRef]
- Driscoll, D.F.; Bhargava, H.N.; Li, L.; Zaim, R.H.; Babayan, V.K.; Bistrian, B.R. Physicochemical stability of total nutrient admixtures. Am. J. Heal. Pharm. 1995, 52, 623–634. [Google Scholar] [CrossRef]
- International Organization for Standardization (ISO). Lexikon des gesamten Buchwesens Online. 2017, 22412. Available online: https://0-referenceworks-brillonline-com.brum.beds.ac.uk/browse/lexikon-des-gesamten-buchwesens-online (accessed on 15 February 2019).
- Driscoll, D.F.; Nehne, J.; Peterss, H.; Klutsch, K.; Bistrian, B.R.; Niemann, W. Physical Assessments of Lipid Injectable Emulsions via Microscopy: A Comparison to Methods Proposed in United States Pharmacopeia Chapter 729. Int. J. Pharm. Compd. 2006, 10, 309–315. [Google Scholar]
- The United States Pharmacopeia Convention. Globule Size Distribution in Lipid Injectable Emulsions. 2009, pp. 314–316. Available online: http://pssnicomp.cn/upload/201466922331.pdf (accessed on 16 February 2019).
- Washington, C. Stability of lipid emulsions for drug delivery. Adv. Drug Deliv. Rev. 1996, 20, 131–145. [Google Scholar] [CrossRef]
- Washington, C. The electrokinetic properties of phospholipid stabilized fat emulsions VI. Zeta potentials of Intralipid 20% in TPN mixtures. Int. J. Pharm. 1992, 87, 167–174. [Google Scholar] [CrossRef]
- Washington, C. The electrokinetic properties of phospholipid-stabilized fat emulsions. Int. J. Pharm. 1990, 64, 67–73. [Google Scholar] [CrossRef]
- Télessy, I.; Balogh, J.; Csempesz, F.; Szente, V.; Dredán, J.; Zelko, R. Comparison of the physicochemical properties of MCT-containing fat emulsions in total nutrient admixtures. Colloids Surfaces B: Biointerfaces 2009, 72, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN guideline: Clinical nutrition in surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.R. Safe Practices for Compounding of Parenteral Nutrition. J. Parenter. Enter. Nutr. 2012, 36, 14–19. [Google Scholar] [CrossRef] [PubMed]
- ICH Harmonised Tripartite Guideline: Validation of Analytical Procedure Development and Revision of Q2(R1). Available online: https://www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Quality/Q2_R1/Step4/Q2_R1__Guideline.pdf (accessed on 17 February 2019).
Sample Availability: Not available. |









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TPN Mixture Elements | Composition | |||||
|---|---|---|---|---|---|---|
| Basic | Immuno-modulatory | High-Electrolyte | Low-Electrolyte | High-Energetic | Low-Energetic | |
| Aminoplasmal® B. Braun 10% E | 600 | 600 | 600 | 600 | 600 | 0 |
| Aminoplasmal HEPA® 10% | 0 | 0 | 0 | 0 | 0 | 600 |
| Glucose 40% | 481.49 | 481.49 | 481.49 | 481.49 | 581.49 | 431.49 |
| LIPIDem® | 0 | 300 | 0 | 0 | 0 | 0 |
| Lipofundin® MCT/LCT 20% | 300 | 0 | 300 | 300 | 350 | 150 |
| Aqua pro iniectione | 372.77 | 372.77 | 308.77 | 405.77 | 222.77 | 572.77 |
| Natrium chloratum 10% | 57.74 | 57.74 | 77.74 | 37.74 | 57.74 | 57.74 |
| Kalium chloratum 15% WZF | 40 | 40 | 60 | 35 | 40 | 40 |
| Calcium gluconate 10% | 20 | 20 | 30 | 20 | 20 | 20 |
| Glycophos | 20 | 20 | 30 | 15 | 20 | 20 |
| Inj. Magnesii sulfurici 20% | 8 | 8 | 12 | 5 | 8 | 8 |
| Linezolid Polpharma | 600 | 600 | 600 | 600 | 600 | 600 |
| Total volume [mL] | 2500 | 2500 | 2500 | 2500 | 2500 | 2500 |
| Parameters | Acceptance Criteria | Results |
|---|---|---|
| Selectivity Influence of interfering substances | Separation of linezolid peak from peaks of TPN mixture ingredients | Acceptable Amino acids, tR 1.5–4.2 min Linezolid tR = 7.8 min |
| Linearity Correlation coefficient r for equation y = ax | r ≥ 0.990 | Acceptable y = (29252.4 ± 286.5)x; r = 0.9998 |
| Repeatability - intra-day - inter-day | RSD ≤ 5% | Acceptable RSD = 0.31% RSD = 0.23% |
| Limits of detection and quantitation | QL = 0.013; DL = 0.040 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomczak, S.; Stawny, M.; Dettlaff, K.; Kieliszek, M.; Słomińska, D.; Jelińska, A. Physicochemical Compatibility and Stability of Linezolid with Parenteral Nutrition. Molecules 2019, 24, 1242. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules24071242
Tomczak S, Stawny M, Dettlaff K, Kieliszek M, Słomińska D, Jelińska A. Physicochemical Compatibility and Stability of Linezolid with Parenteral Nutrition. Molecules. 2019; 24(7):1242. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules24071242
Chicago/Turabian StyleTomczak, Szymon, Maciej Stawny, Katarzyna Dettlaff, Maria Kieliszek, Daria Słomińska, and Anna Jelińska. 2019. "Physicochemical Compatibility and Stability of Linezolid with Parenteral Nutrition" Molecules 24, no. 7: 1242. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules24071242