
Clinical Prognosis for SAH Consistent with Redox Imbalance and Lipid Peroxidation

 ,
,
Abstract
:1. Introduction
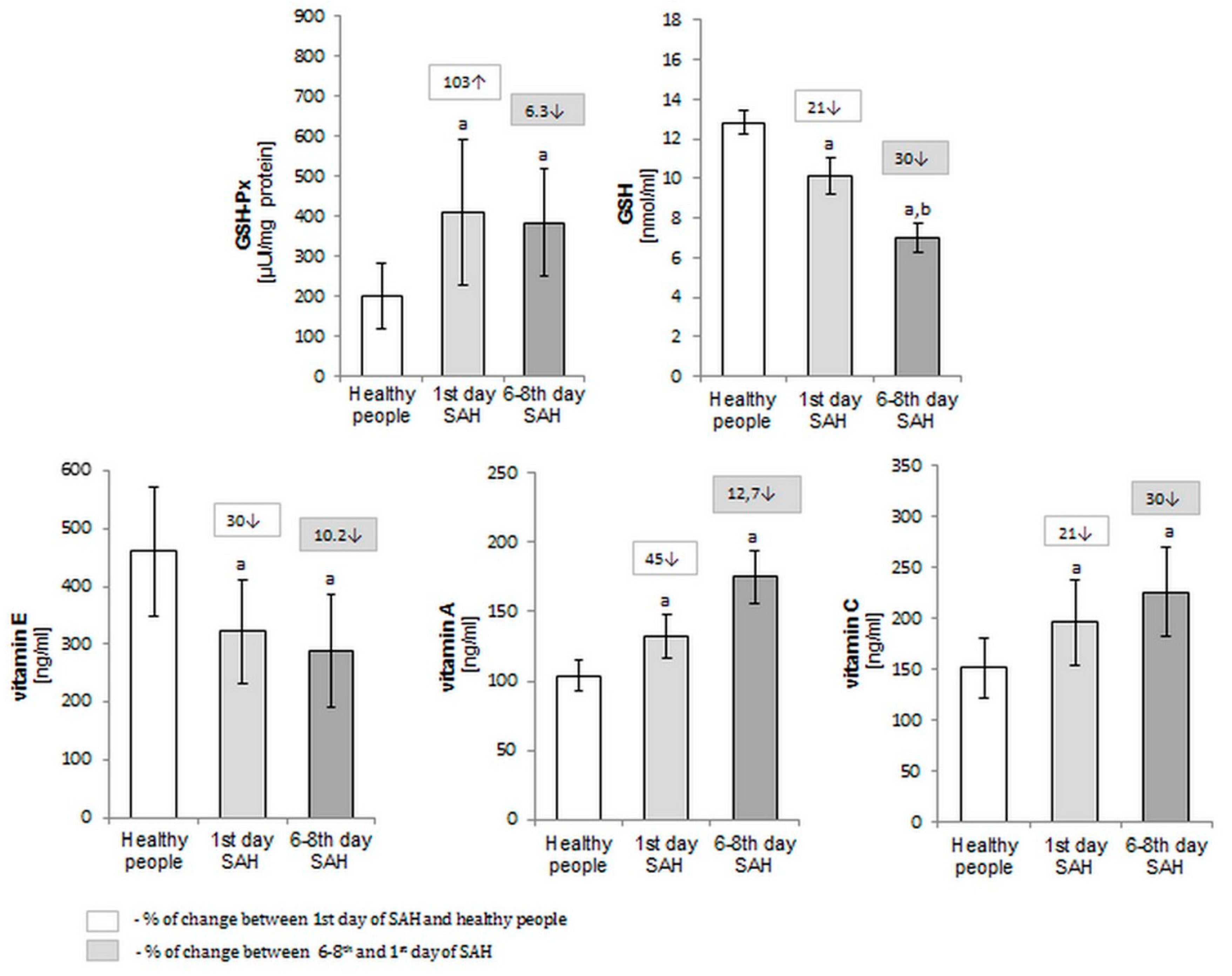
2. Results
3. Discussion
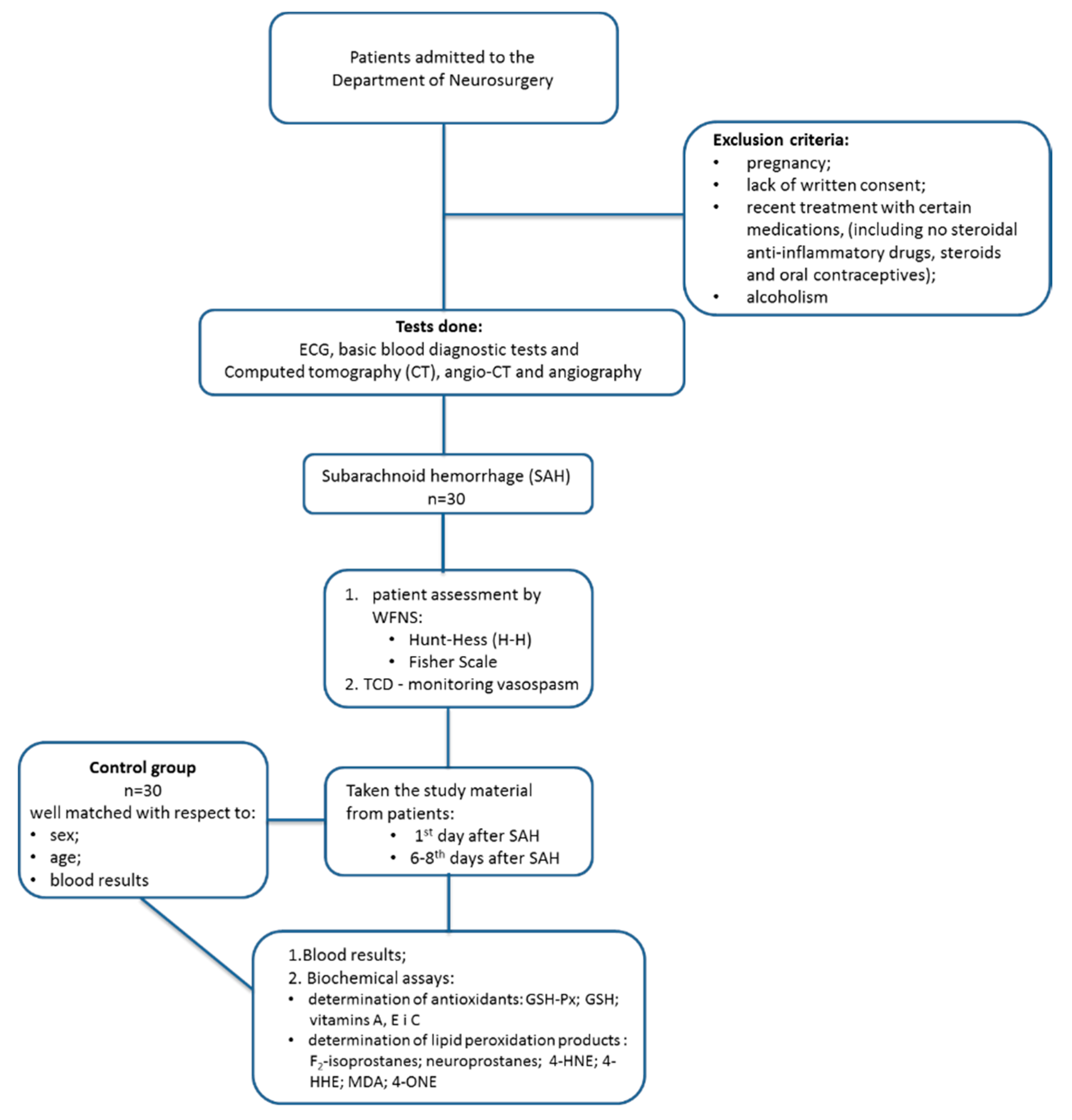
4. Materials and Methods
4.1. Reagents
4.2. Materials
4.3. Samples and Laboratory Measurements
4.4. Biochemical Assays
4.4.1. Determination of Antioxidants
4.4.2. Determination of Lipid Peroxidation Products
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Frosen, J.; Tulamo, R.; Paetau, A.; Laaksamo, E.; Korja, M.; Laakso, A.; Niemela, M.; Hernesniemi, J. Saccular intracranial aneurysm: Pathology and mechanisms. Acta Neuropathol. 2012, 123, 773–786. [Google Scholar] [CrossRef] [PubMed]
- Nieuwkamp, D.J.; Setz, L.E.; Algra, A.; Linn, F.H.; de Rooij, N.K.; Rinkel, G.J. Changes in case fatality of aneurysmal subarachnoid hemorrhage over time, according to age, sex, and region: A meta-analysis. Lancet Neurol. 2009, 8, 635–642. [Google Scholar] [CrossRef]
- Huhtakangas, J.; Lehto, H.; Seppä, K.; Kivisaari, R.; Niemelä, M.; Hernesniemi, J.; Lehecka, M. Long-term excess mortality after aneurysmal subarachnoid hemorrhage: Patients with multiple aneurysms at risk. Stroke 2015, 46, 1813–1818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Chen, S.; Zhang, J.M. The updated role of oxidative stress in subarachnoid hemorrhage. Curr. Drug Deliv. 2017, 14, 832–842. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Su, J.; Liu, X.; Zhao, Y.; Wang, C.; Li, X. Naringin alleviates early brain injury after experimental subarachnoid hemorrhage by reducing oxidative stress and inhibiting apoptosis. Brain Res. Bull. 2017, 133, 42–50. [Google Scholar] [CrossRef]
- Nishihashi, T.; Trandafir, C.C.; Wang, A.; Ji, X.; Shimizu, Y.; Kurahashi, K. Hypersensitivity to hydroxyl radicals in rat basilar artery after subarachnoid hemorrhage. J. Pharmacol. Sci. 2006, 100, 234–236. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.L.; Hsu, Y.T.; Lin, T.K.; Morrow, J.D.; Hsu, J.C.; Hsu, Y.H.; Hsieh, T.C.; Tsay, P.K.; Yen, H.C. Increased levels of F2-isoprostanes following aneurysmal subarachnoid hemorrhage in humans. Free Radic. Biol. Med. 2006, 40, 1466–1473. [Google Scholar] [CrossRef]
- Reeder, B.J. The redox activity of hemoglobins: From physiologic functions t pathologic mechanisms. Antioxid. Redox Signal. 2010, 13, 1087–1123. [Google Scholar] [CrossRef]
- Ward, R.J.; Zucca, F.A.; Duyn, J.H.; Crichton, R.R.; Zecca, L. The role of iron in brain ageing and neurodegenerative disorders. Lancet Neurol. 2014, 13, 1045–1060. [Google Scholar] [CrossRef] [Green Version]
- Konior, A.; Schramm, A.; Czesnikiewicz-Guzik, M.; Guzik, T.J. NADPH oxidases in vascular pathology. Antioxid. Redox. Signal. 2014, 20, 2794–2814. [Google Scholar] [CrossRef] [Green Version]
- Emeto, T.I.; Moxon, J.V.; Au, M.; Golledge, J. Oxidative stress and abdominal aortic aneurysm: Potential treatment targets. Clin. Sci. (Lond.) 2016, 130, 301–315. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Koide, M.; Dumont, T.M.; Russell, S.R.; Tranmer, B.I.; Wellman, G.C. Subarachnoid hemorrhage induces gliosis and increased expression of the pro-inflammatory cytokine high mobility group box 1 protein. Transl. Stroke Res. 2001, 2, 72–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salim, S. Oxidative Stress and the Central Nervous System. J. Pharmacol. Exp. Ther. 2017, 360, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Mori, T.; Nagata, K.; Town, T.; Tan, J.; Matsui, T.; Asano, T. Intracisternal increase of superoxide anion production in a canine subarachnoid hemorrhage model. Stroke 2001, 32, 636–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erşahin, M.; Ozsavcı, D.; Sener, A.; Ozakpınar, O.B.; Toklu, H.Z.; Akakin, D.; Sener, G.; Yeğen, B.Ç. Obestatin alleviates subarachnoid haemorrhage-induced oxidative injury in rats via its anti-apoptotic and antioxidant effects. Brain Inj. 2013, 27, 1181–1189. [Google Scholar] [CrossRef]
- Endo, H.; Nito, C.; Kamada, H.; Yu, F.; Chan, P.H. Reduction in oxidative stress by superoxide dismutase overexpression attenuates acute brain injury after subarachnoid hemorrhage via activation of Akt/glycogen synthase kinase-3beta survival signaling. J. Cereb. Blood Flow Metab. 2007, 27, 975–982. [Google Scholar] [CrossRef] [Green Version]
- Nurden, A.T. Platelets, inflammation and tissue regeneration. Thromb. Haemost. 2011, 105, 13–33. [Google Scholar] [CrossRef]
- Parrella, E.; Porrini, V.; Benarese, M.; Pizzi, M. The role of mast cells in stroke. Cells 2019, 8, 437. [Google Scholar] [CrossRef] [Green Version]
- Ocak, U.; Ocak, P.E.; Wang, A.; Zhang, J.H.; Boling, W.; Wu, P.; Mo, J.; Zhang, T.; Huang, L. Targeting mast cell as a neuroprotective strategy. Brain Inj. 2019, 33, 723–733. [Google Scholar] [CrossRef]
- Taylor, B.E.S.; Appelboom, G.; Zilinyi, R.; Goodman, A.; Chapel, D.; LoPresti, M.; Connolly, E.S., Jr. Role of the complement cascade in cerebral aneurysm formation, growth, and rupture. Neuroimmunol. Neuroinflammation 2015, 2, 93–101. [Google Scholar]
- Laaksamo, E.; Tulamo, R.; Liiman, A.; Baumann, M.; Friedlander, R.M.; Hernesniemi, J.; Kangasniemi, M.; Niemelä, M.; Laakso, A.; Frösen, J. Oxidative stress is associated with cell death, wall degradation, and increased risk of rupture of the intracranial aneurysm wall. Neurosurgery 2013, 72, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.D.; Broderick, J.P. Unruptured intracranial aneurysms: Epidemiology, natural history, management options, and familial screening. Lancet Neurol. 2014, 13, 393–404. [Google Scholar] [CrossRef]
- Syta-Krzyżanowska, A.; Jarocka-Karpowicz, I.; Kochanowicz, J.; Turek, G.; Rutkowski, R.; Gorbacz, K.; Mariak, Z.; Skrzydlewska, E. F2-isoprostanes and F4-neuroprostanes as markers of intracranial aneurysm development. Adv. Clin. Exp. Med. 2018, 27, 673–680. [Google Scholar] [CrossRef]
- Domingues, R.M.; Domingues, P.; Melo, T.; Perez-Sala, D.; Reis, A.; Spickett, C.M. Lipoxidation adducts with peptides and proteins: Deleterious modifications or signalling mechanisms? J. Proteomics 2013, 92, 110–131. [Google Scholar] [CrossRef] [PubMed]
- Barrow, J.W.; Turan, N.; Wangmo, P.; Roy, A.K.; Pradilla, G. The role of inflammation and potential use of sex steroids in intracranial aneurysms and subarachnoid hemorrhage. Surg. Neurol. Int. 2018, 26, 150. [Google Scholar]
- Starke, R.M.; Chalouhi, N.; Ali, M.S.; Jabbour, P.M.; Tjoumakaris, S.I.; Gonzalez, L.F.; Rosenwasser, R.H.; Koch, W.J.; Dumont, A.S. The role of oxidative stress in cerebral aneurysm formation and rupture. Curr. Neurovasc. Res. 2013, 10, 247–255. [Google Scholar] [CrossRef] [Green Version]
- Pyne-Geithman, G.J.; Caudell, D.N.; Prakash, P.; Clark, J.F. Glutathione peroxidase and subarachnoid hemorrhage: Implications for the role of oxidative stress in cerebral vasospasm. Neurol. Res. 2009, 31, 195–199. [Google Scholar] [CrossRef] [Green Version]
- La Fata, G.; Weber, P.; Mohajeri, M.H. Effects of vitamin E on cognitive performance during ageing and in Alzheimer’s disease. Nutrients 2014, 6, 5453–5472. [Google Scholar] [CrossRef] [Green Version]
- Shirley, R.; Ord, E.N.; Work, L.M. Oxidative stress and the use of antioxidants in stroke. Antioxidants 2014, 3, 472–501. [Google Scholar] [CrossRef] [Green Version]
- Brigelius-Flohe, R.; Maiorino, M. Glutathione peroxidases. Biochim. Biophys. Acta. 2013, 1830, 3289–3303. [Google Scholar] [CrossRef]
- Bazinet, R.P.; Layé, S. Polyunsaturated fatty acids and their metabolites in brain function and disease. Nat. Rev. Neurosci. 2014, 15, 771–785. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Wang, S.; Mao, L.; Leak, R.K.; Shi, Y.; Zhang, W.; Hu, X.; Sun, B.; Cao, G.; Gao, Y.; et al. Omega-3 fatty acids protect the brain against ischemic injury by activating Nrf2 and upregulating heme oxygenase 1. J. Neurosci. 2014, 34, 1903–1915. [Google Scholar] [CrossRef] [PubMed]
- Downey, L.A.; Simpson, T.; Timmer, J.; Nolidin, K.; Croft, K.; Wesnes, K.A. Impaired verbal episodic memory in healthy older adults is marked by increased F2-Isoprostanes. Prostaglandins. Leukot. Essent. Fat. Acids 2018, 129, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Milne, G.L.; Dai, Q.; Roberts, L.J., 2nd. The isoprostanes-25 years later. Biochim. Biophys. Acta 2015, 1851, 433–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corcoran, T.B.; Mas, E.; Barden, A.E.; Durand, T.; Galano, J.M.; Roberts, L.J.; Phillips, M.; Ho, K.M.; Mori, T.A. Are isofurans and neuroprostanes increased after subarachnoid hemorrhage and traumatic brain injury? Antioxid. Redox Signal. 2011, 15, 2663–2667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, E.K.; Murphy, T.C.; Leiphon, L.J.; Watt, J.; Morrow, J.D.; Milne, G.L.; Howard, J.R.; Picklo, M.J. Trans-4-hydroxy-2-hexenal is a neurotoxic product of docosahexaenoic (22:6; n-3) acid oxidation. J. Neurochem. 2008, 105, 714–724. [Google Scholar] [CrossRef]
- Miller, E.; Morel, A.; Saso, L.; Saluk, J. Isoprostanes and neuroprostanes as biomarkers of oxidative stress in neurodegenerative diseases. Oxid. Med. Cell Longev. 2014, 2014, 572491. [Google Scholar] [CrossRef]
- Kelle, J.N.; Mark, R.J.; Bruce, A.J.; Blanc, E.; Rothstein, J.D.; Uchida, K.; Waeg, G.; Mattson, M.P. 4-hydroxynonenal, an aldehydic product of membrane lipid peroxidation, impairs glutamate transport and mitochondrial function in synaptosomes. Neuroscience 1997, 80, 685–696. [Google Scholar] [CrossRef]
- Guzik, B.; Sagan, A.; Ludew, D.; Mrowiecki, W.; Chwała, M.; Bujak-Gizycka, B.; Filip, G.; Grudzien, G.; Kapelak, B.; Zmudka, K.; et al. Mechanisms of oxidative stress in human aortic aneurysms--association with clinical risk factors for atherosclerosis and disease severity. Int. J. Cardiol. 2013, 168, 2389–2396. [Google Scholar] [CrossRef] [Green Version]
- Otnes, S.; Fogh-Andersen, N.; Rømsing, J.; Thomsen, H.S. Analytical Interference by Contrast Agents in Biochemical Assays. Contrast Media Mol. Imaging. 2017, 2017, 1323802. [Google Scholar] [CrossRef]
- Lippi, G.; Daves, M.; Mattiuzzi, C. Interference of medical contrast media on laboratory testing. Biochem. Med. (Zagreb). 2014, 24, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Kaynar, M.Y.; Tanriverdi, T.; Kemerdere, R.; Atukeren, P.; Gumustas, K. Cerebrospinal fluid superoxide dismutase and serum malondialdehyde levels in patients with aneurysmal subarachnoid hemorrhage: Preliminary results. Neurol. Res. 2005, 27, 562–567. [Google Scholar] [CrossRef] [PubMed]
- Łuczaj, W.; Gęgotek, A.; Skrzydlewska, E. Antioxidants and HNE in redox homeostasis. Free Radic. Biol. Med. 2017, 111, 87–101. [Google Scholar] [CrossRef] [PubMed]
- Moniuszko-Malinowska, A.; Łuczaj, W.; Jarocka-Karpowicz, I.; Pancewicz, S.; Zajkowska, J.; Andrisic, L.; Zarkovic, N.; Skrzydlewska, E. Lipid peroxidation in the pathogenesis of neuroborreliosis. Free Radic. Biol. Med. 2016, 96, 255–263. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, S. Aneurysmal Subarachnoid Hemorrhage. J. Neurosurg. Anesthesiol. 2015, 27, 222–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gostner, J.M.; Becker, K.; Ueberall, F.; Fuchs, D. The good and bad of antioxidant foods: An immunological perspective. Food Chem. Toxicol. 2015, 80, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Munakata, A.; Ohkuma, H.; Nakano, T.; Shimamura, N.; Asano, K.; Naraoka, M. Effect of a free radical scavenger, edaravone, in the treatment of patients with aneurysmal subarachnoid hemorrhage. Neurosurgery 2009, 64, 423–429. [Google Scholar] [CrossRef]
- Teasdale, G.M.; Drake, C.G.; Hunt, W.; Kassell, N.; Sano, K.; Pertuiset, B.; de Villiers, J.C. A universal subarachnoid haemorrhage scale: Report of a committee of the Word Federation of Neurosurgical Societies. J. Neurol. Neurosurg. Psychiatry 1988, 51, 1457. [Google Scholar] [CrossRef] [Green Version]
- Fisher, C.M.; Kistler, J.P.; Davis, J.M. Relation of cerebral vasospasm to subarachnoid hemorrhage visualized by computerized tomographic scanning. Neurosurgery 1980, 6, 1–9. [Google Scholar] [CrossRef]
- Naraoka, M.; Matsuda, N.; Shimamura, N.; Asano, K.; Ohkuma, H. The role of arterioles and the microcirculation in the development of vasospasm after aneurysmal SAH. Biomed. Res. Int. 2014, 2014, 253746. [Google Scholar] [CrossRef]
- Gęgotek, A.; Biernacki, M.; Ambrożewicz, E.; Surażyński, A.; Wroński, A.; Skrzydlewska, E. The cross-talk between electrophiles, antioxidant defence and the endocannabinoid system in fibroblasts and keratinocytes after UVA and UVB irradiation. J. Dermatol. Sci. 2016, 81, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Gęgotek, A.; Rybałtowska-Kawałko, P.; Skrzydlewska, E. Rutin as a mediator of lipid metabolism and cellular signaling pathways interactions in fibroblasts altered by UVA and UVB radiation. Oxid. Med. Cell Longev. 2017, 2017, 4721352. [Google Scholar] [CrossRef] [PubMed]
- Ivanović, D.; Popović, A.; Radulović, D.; Medenica, M. Reversed-phase ion-pair HPLC determination of some water-soluble vitamins in pharmaceuticals. J. Pharm. Biomed. Anal. 1999, 18, 999–1004. [Google Scholar] [CrossRef]
- Maeso, N.; Garcıa-Martınez, D.; Ruperez, F.J.; Cifuentes, A.; Barbas, C. Capillary electrophoresis of glutathione to monitor oxidative stress and response to antioxidant treatments in an animal model. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2005, 822, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.P.; Yazdanpanah, M.; Bhooi, N.; Lehotay, D.C. Determination of aldehydes and other lipid peroxidation products in biological samples by gas chromatography-mass spectrometry. Ana.L Biochem. 1995, 228, 294–298. [Google Scholar] [CrossRef]
- Coolen, S.A.; van Buuren, B.; Duchateau, G.; Upritchard, J.; Verhagen, H. Kinetics of biomarkers: Biological and technical validity of isoprostanes in plasma. Amino Acids 2005, 29, 429–436. [Google Scholar] [CrossRef]
- Fam, S.S.; Murphey, L.J.; Terry, E.S.; Zackert, W.E.; Chen, Y.; Gao, L.; Pandalai, S.; Milne, G.L.; Roberts, L.J.; Porter, N.A.; et al. Formation of highly reactive A-ring and J-ring isoprostane-like compounds (A4/J4-neuroprostanes) in vivo from docosahexaenoic acid. J. Biol. Chem. 2002, 277, 36076–36084. [Google Scholar] [CrossRef] [Green Version]
Sample availability: Compounds of the samples are not available from the authors. |




{kind=link}
{kind=link}
{kind=link}
| Parameters | GSH-Px (uU/mg Protein) | GSH (nmol/mL) | Vit. E (ng/mL) | Vit. A (ng/mL) | Vit. C (ng/mL) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Day | 1st | 6–8th | 1st | 6–8th | 1st | 6–8th | 1st | 6–8th | 1st | 6–8th | |
| Focal signs | /-/ n = 25 | 408 ± 119 | 393 ± 138 | 10.0 ± 0.9 | 7.0 ± 0.7 a | 313 ± 91 | 294 ± 101 | 43.7 ± 13.9 | 38.0 ± 12.5 | 23.6 ± 13.4 | 27.3 ± 11.7 |
| /+/ n = 5 | 438 ± 168 | 371 ± 106 | 10.3 ± 0.9 | 7.2 ± 0.7 a | 364 ± 69 | 298 ± 94 | 55.2 ± 18.6 | 33.1 ± 6.3 a | 35.1 ± 17.1 | 27.3 ± 14.1 | |
| Hunt-Hess scale | /1/ n = 19 | 415 ± 141 | 387 ± 98 | 9.9 ± 0.8 | 6.8 ± 0.7 a | 312 ± 94 | 279 ± 97 | 41.8 ± 13.7 | 37.3 ± 13.1 | 26.4 ± 10.7 | 28.0 ± 11.3 |
| /2-4/ n = 11 | 387 ± 98 | 390 ± 164 | 10.2 ± 0.9 | 7.3 ± 0.5 a | 312 ± 92 | 281 ± 79 | 48.0 ± 16.7 | 40.9 ± 10.9 | 29.2 ± 13.0 | 27.2 ± 10.5 | |
| WFNS | /1/ n = 23 | 418 ± 138 | 402 ± 134 | 10.1 ± 0.9 | 7.0 ± 0.7 a | 315 ± 94 | 287 ± 101 | 42.5 ± 14.3 | 37.5 ± 12.5 | 27.4 ± 11.0 | 28.4 ± 11.5 |
| /2-4/ n = 7 | 394 ± 102 | 332 ± 122 | 9.9 ± 0.8 | 7.2 ± 0.7 a | 284 ± 107 | 284 ± 82 | 43.1 ± 21.9 | 41.5 ± 11.4 | 31.1 ± 15.8 | 30.1 ± 12.5 | |
| Fisher scale | /1-2/ n = 11 | 407 ± 133 | 344 ± 98 | 9.9 ± 0.8 | 7.3 ± 0.6 a | 308 ± 94 | 279 ± 97 | 41.4 ± 13.7 | 37.3 ± 13.1 | 26.4 ± 10.7 | 28.0 ± 11.3 |
| /3-4/ n = 19 | 414 ± 129 | 407 ± 145 | 10.3 ± 0.9 | 6.6 ± 0.7 a | 412 ± 165 | 325 ± 184 | 53.7 ± 37.9 | 38.2 ± 17.6 | 23.8 ± 10.6 | 25.5 ± 10.7 | |
| Brain edema | /-/ n = 11 | 391 ± 135 | 355 ± 81 | 10.2 ± 0.9 | 7.2 ± 0.6 a | 308 ± 94 | 279 ± 97 | 41.4 ± 13.7 | 37.3 ± 13.1 | 26.4 ± 10.7 | 28.0 ± 11.3 |
| /+/ n = 19 | 424 ± 126 | 402 ± 153 | 9.9 ± 0.9 | 6.7 ± 0.7 a | 397 ± 173 | 349 ± 161 | 56.0 ± 38.6 | 38.7 ± 16.3 a | 28.9 ± 10.3 | 27.3 ± 12.0 | |
| Hematoma | /-/ n = 25 | 400 ± 125 | 375 ± 121 | 10.0 ± 0.9 | 7.0 ± 0.7 a | 324 ± 91 | 290 ± 101 | 43.7 ± 13.9 | 37.6 ± 12.5 | 26.8 ± 10.7 | 27.3 ± 11.7 |
| /+/ n = 5 | 473 ± 143 | 437 ± 187 | 10.3 ± 0.9 | 7.2 ± 0.5 a | 308 ± 83 | 275 ± 72 | 45.5 ± 9.2 | 44.3 ± 13.8 | 30.1 ± 10.5 | 26.1 ± 12.0 | |
| Complications | /-/ n = 25 | 406 ± 134 | 376 ± 129 | 10.1 ± 0.9 | 7.0 ± 0.7 a | 324 ± 91 | 290 ± 101 | 43.7 ± 13.9 | 37.6 ± 12.5 | 26.8 ± 10.7 | 27.3 ± 11.7 |
| /+/ n = 5 | 455 ± 62 | 430 ± 157 | 9.9 ± 0.9 | 7.2 ± 0.6 a | 373 ± 150 | 368 ± 193 | 40.0 ± 9.2 | 47.7 ± 16.3 | 26.8 ± 5.2 | 24.9 ± 2.9 | |
| Gender | /W/ n = 21 | 440 ± 132 | 385 ± 138 | 9.9 ± 0.8 | 7.1 ± 0.6 a | 355 ± 134 | 337 ± 113 | 44.4 ± 14.4 | 42.0 ± 12.1 | 29.1 ± 12.9 | 26.3 ± 10.7 |
| /M/ n = 9 | 347 ± 96 | 387 ± 126 | 10.3 ± 0.9 | 6.8 ± 0.9 a | 327 ± 107 | 218 ± 103 a | 58.6 ± 42.4 | 32.3 ± 15.1 a | 29.4 ± 10.3 | 28.1 ± 11.4 | |
| Parameters | F2-isoprostanes [ng/ml] | Neuroprostanes [ng/ml] | 4-HNE [nmol/ml] | 4-HHE [pmol/ml] | MDA [nmol/ml] | 4-ONE [pmol/ml] | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Day | 1st | 6–8th | 1st | 6–8th | 1st | 6–8th | Day | 1st | 6–8th | 1st | 6–8th | 1st | |
| Focal signs | /-/ n = 25 | 1.12 ± 0.55 | 0.86 ± 0.30 a | 6.11 ± 2.62 | 3.88 ± 2.17 a | 0.57 ± 0.39 | 0.28 ± 0.21 a | 3.36 ± 1.58 | 3.65 ± 1.51 | 7.05 ± 4.98 | 5.74 ± 3.88 | 0.19 ± 0.15 | 0.15 ± 0.12 |
| /+/ n = 5 | 1.17 ± 0.85 | 0.71 ± 0.41 | 7.11 ± 2.65 | 4.14 ± 1.08 a | 0.94 ± 0.62 | 0.24 ± 0.14 a | 2.90 ± 1.03 | 3.20 ± 1.47 | 8.90 ± 6.25 | 6.63 ± 4.82 | 0.20 ± 0.13 | 0.13 ± 0.03 | |
| Hunt-Hess scale | /1/ n = 19 | 1.13 ± 0.49 | 0.85 ± 0.40 a | 6.25 ± 2.82 | 3.75 ± 1.83 a | 0.62 ± 0.45 | 0.25 ± 0.16 a | 3.51 ± 1.87 | 3.78 ± 1.41 | 6.22 ± 4.37 | 5.17 ± 3.07 | 0.15 ± 0.11 | 0.14 ± 0.10 |
| /2-4/ n = 11 | 1.11 ± 0.78 | 0.84 ± 0.37 | 6.04 ± 2.22 | 4.36 ± 2.71 | 0.69 ± 0.49 | 0.34 ± 0.26 a | 3.05 ±1.30 | 2.84 ± 1.14 | 9.04 ± 5.46 | 7.74 ± 5.17 | 0.25 ± 0.18 | 0.17 ± 0.15 | |
| WFNS | /1/ n = 23 | 1.02 ± 0.50 | 0.83 ± 0.42 | 6.02 ± 2.72 | 4.08 ± 2.26 | 0.66 ± 0.47 | 0.29 ± 0.22 a | 3.17 ± 1.48 | 3.42 ± 1.27 | 6.31 ± 4.19 | 5.73 ± 3.51 | 0.19 ± 0.14 | 0.16 ± 0.11 |
| /2-4/ n = 7 | 1.32 ± 0.76 | 0.83 ± 0.32 | 6.42 ± 2.00 | 3.36 ± 1.17 a | 0.60 ± 0.38 | 0.25 ± 0.13 a | 3.39 ± 1.17 | 3.87 ± 1.35 | 9.28 ± 6.59 | 6.98 ± 5.22 | 0.19 ± 0.16 | 0.10 ± 0.09 | |
| Fisher scale | /1-2/ n = 11 | 1.05 ± 0.57 | 0.78 ± 0.44 | 6.36 ± 3.42 | 4.00 ± 2.12 a | 0.66 ± 0.46 | 0.30 ± 0.20 a | 4.11 ± 1.79 | 4.34 ± 1.99 | 7.47 ± 4.99 | 4.64 ± 3.12 | 0.15 ± 0.12 | 0.15 ± 0.10 |
| /3-4/ n = 19 | 1.13 ± 0.61 | 0.86 ± 0.37 | 5.99 ± 2.04 | 3.89 ± 2.12 a | 0.64 ± 0.45 | 0.27 ± 0.21 a | 2.85 ± 1.15 | 3.04 ± 1.21 | 6.85 ± 5.03 | 6.82 ± 4.24 | 0.21 ± 0.15 | 0.15 ± 0.12 | |
| Brain edema | /-/ n = 11 | 1.11 ± 0.54 | 0.89 ± 0.44 | 5.63 ± 1.65 | 3.73 ± 1.45 a | 0.71 ± 0.53 | 0.23 ± 0.19 a | 4.28 ± 1.64 | 3.93 ± 1.43 | 6.88 ± 5.36 | 5.07 ± 3.73 | 0.14 ± 0.13 | 0.16 ± 0.10 |
| /+/ n = 19 | 1.09 ± 0.62 | 0.79 ± 0.30 a | 6.42 ± 2.98 | 4.05 ± 2.42 a | 0.62 ± 0.42 | 0.31 ± 0.20 a | 2.57 ± 1.35 | 3.33 ± 1.60 | 7.13 ± 4.87 | 6.51 ± 4.09 | 0.21 ± 0.15 | 0.15 ± 0.12 | |
| Hematoma | /-/ n = 25 | 1.09 ± 0.55 | 0.88 ± 0.40 | 6.16 ± 2.67 | 3.73 ± 1.63 a | 0.59 ± 0.44 | 0.26 ± 0.15 a | 3.53 ± 1.41 | 3.75 ± 1.31 | 6.64 ± 5.02 | 5.40 ± 3.61 | 0.16 ± 0.12 | 0.13 ± 0.09 |
| /+/ n = 5 | 1.14 ± 0.85 | 0.66 ± 0.35 | 5.85 ± 1.97 | 5.22 ± 4.08 | 0.92 ± 0.44 | 0.39 ± 0.35 | 1.84 ± 0.40 | 2.38 ± 0.50 | 8.92 ± 4.51 | 9.74 ± 4.34 | 0.30 ± 0.20 | 0.29 ± 0.18 | |
| Complications | /-/ n = 25 | 1.16 ± 0.56 | 0.89 ± 0.37 | 6.32 ± 2.59 | 3.80 ± 1.90 a | 0.64 ± 0.46 | 0.24 ± 0.12 a | 3.42 ± 1.26 | 3.74 ± 1.74 | 7.40 ± 5.24 | 5.92 ± 3.96 | 0.18 ± 0.14 | 0.13 ± 0.09 |
| /+/ n = 5 | 0.57 ± 0.51 | 0.33 ± 0.04 | 5.00 ± 2.22 | 4.56 ± 2.99 | 0.71 ± 0.38 | 0.46 ± 0.38 a | 1.32 ± 0.34 | 2.03 ± 0.56 | 5.47 ± 3.06 | 6.70 ± 4.42 | 0.23 ± 0.14 | 0.22 ± 0.17 | |
| Gender | /W/ n = 21 | 0.98 ± 0.54 | 0.78 ± 0.38 | 6.36 ± 2.78 | 3.94 ± 1.90 a | 0.67 ± 0.42 | 0.25 ± 0.16 a | 3.01 ± 1.60 | 3.33 ± 1.63 | 6.89 ± 4.94 | 6.17 ± 4.02 | 0.16 ± 0.13 | 0.14 ± 0.10 |
| /M/ n = 9 | 1.38 ± 0.62 | 0.92 ± 0.42 a | 5.30 ± 1.40 | 3.91 ± 2.67 | 0.66 ± 0.42 | 0.35 ± 0.26 | 3.76 ± 2.19 | 4.01 ± 2.00 | 7.53 ± 5.28 | 5.78 ± 4.13 | 0.25 ± 0.16 | 0.18 ± 0.16 | |
| Parameters | Healthy Subjects n = 30 | SAH Patients n = 30 | |
|---|---|---|---|
| WBC (103/mm3) | 5.21 ± 1.12 | 11.15 ± 3.67 | |
| RBC (106/µl) | 4.21 ± 0.34 | 4.09 ± 0.52 | |
| PLT (×100,000/mm3) | 167 ± 42 | 203 ± 61 | |
| Sex | male:female | 9:21 | 9:21 |
| Age | <50 y:>50 y | 13:17 | 13:17 |
| Number of aneurysms 1:>1 | - | 21:9 | |
| Size of aneurysm <10 mm:>10 mm | - | 26:4 | |
| Embolization:Clipping | - | 19:11 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jarocka-Karpowicz, I.; Syta-Krzyżanowska, A.; Kochanowicz, J.; Mariak, Z.D. Clinical Prognosis for SAH Consistent with Redox Imbalance and Lipid Peroxidation. Molecules 2020, 25, 1921. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules25081921
Jarocka-Karpowicz I, Syta-Krzyżanowska A, Kochanowicz J, Mariak ZD. Clinical Prognosis for SAH Consistent with Redox Imbalance and Lipid Peroxidation. Molecules. 2020; 25(8):1921. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules25081921
Chicago/Turabian StyleJarocka-Karpowicz, Iwona, Anna Syta-Krzyżanowska, Jan Kochanowicz, and Zenon Dionizy Mariak. 2020. "Clinical Prognosis for SAH Consistent with Redox Imbalance and Lipid Peroxidation" Molecules 25, no. 8: 1921. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules25081921