
Evaluating Feasibility of Human Tissue Engineered Respiratory Epithelium Construct as a Potential Model for Tracheal Mucosal Reconstruction

 ,
,  ,
,
Abstract
:1. Introduction
2. Results
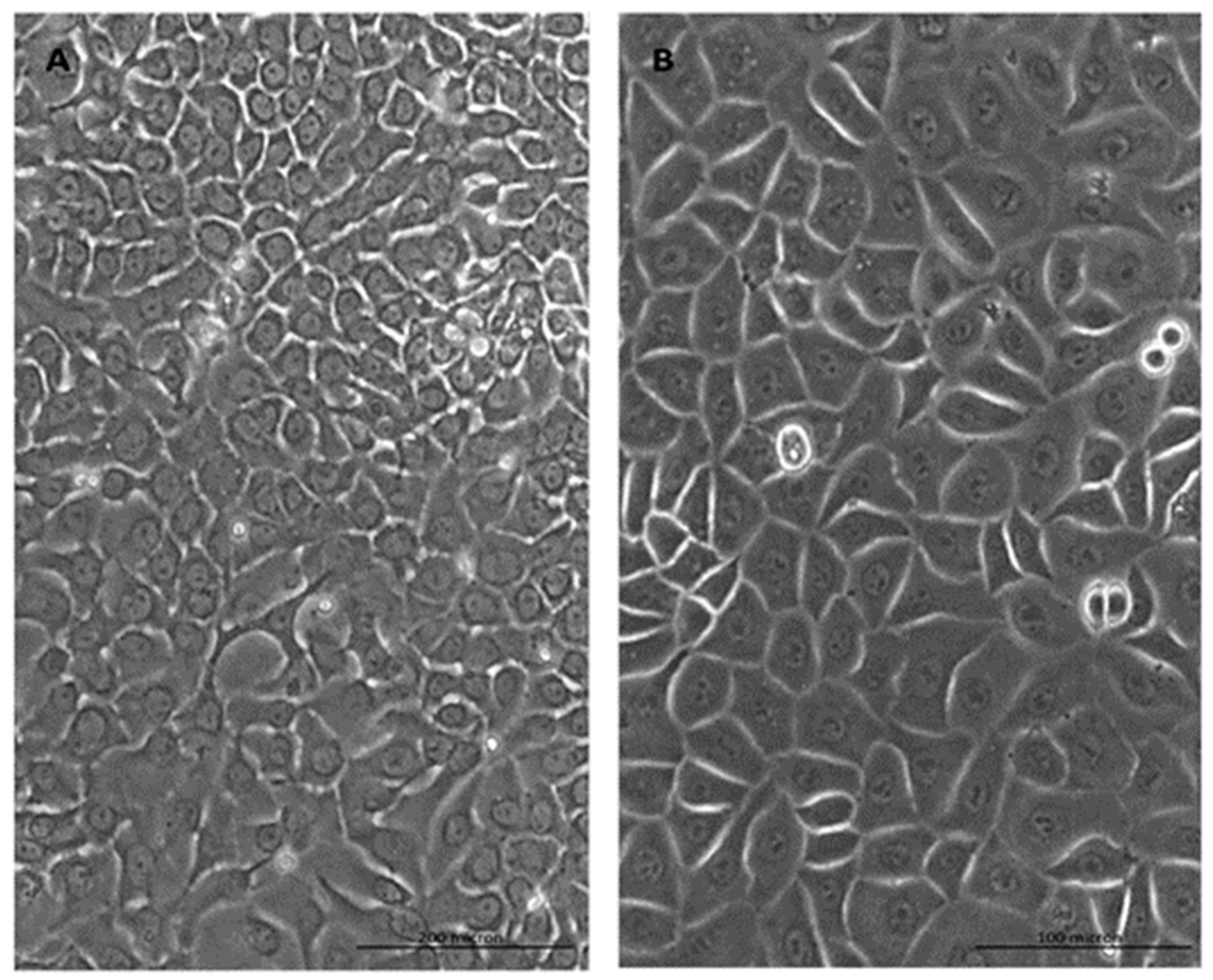
2.1. Cell Morphology
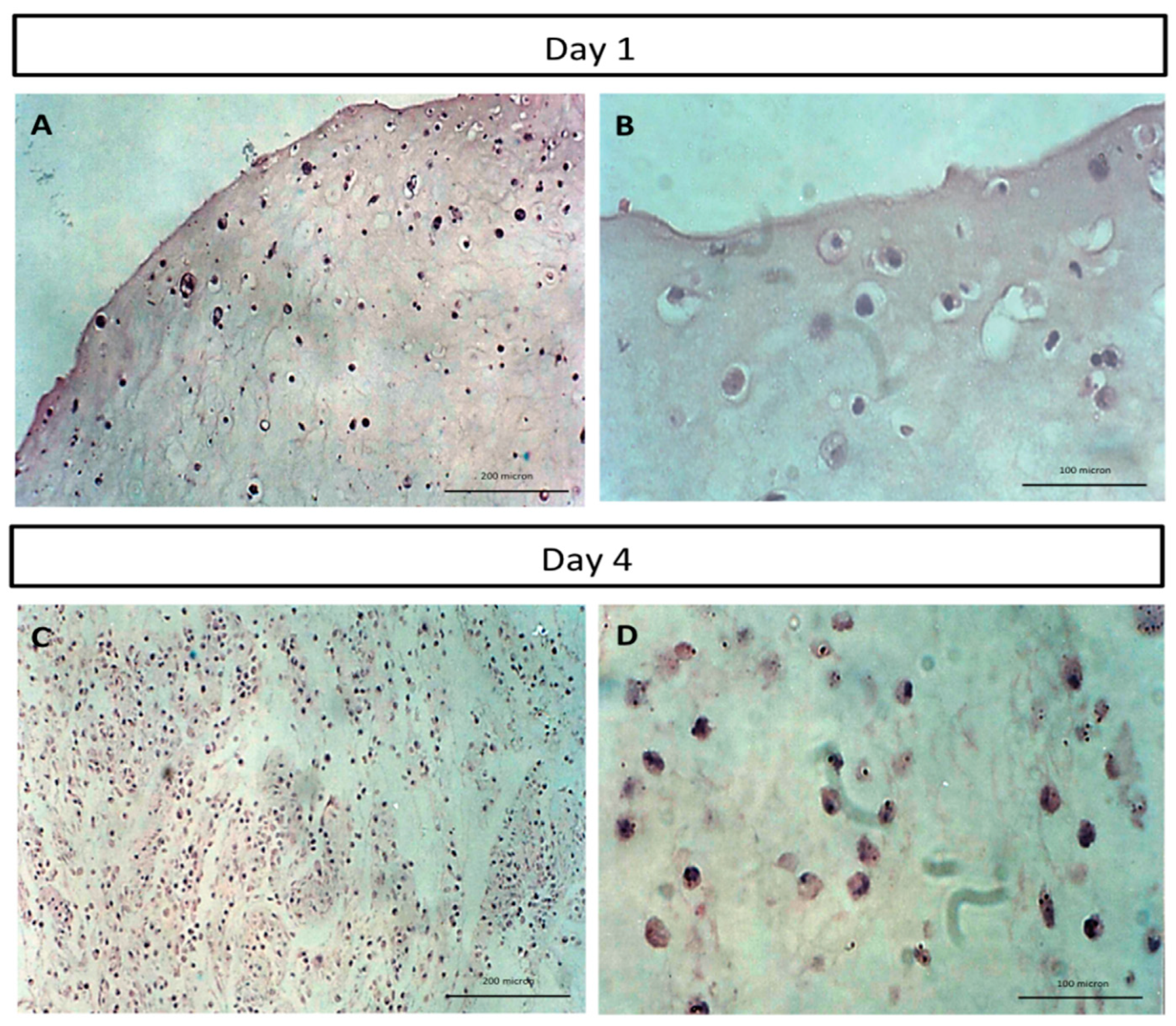
2.2. Histological Analysis of Human Tissue Respiratory Epithelial Construct Cell Morphology
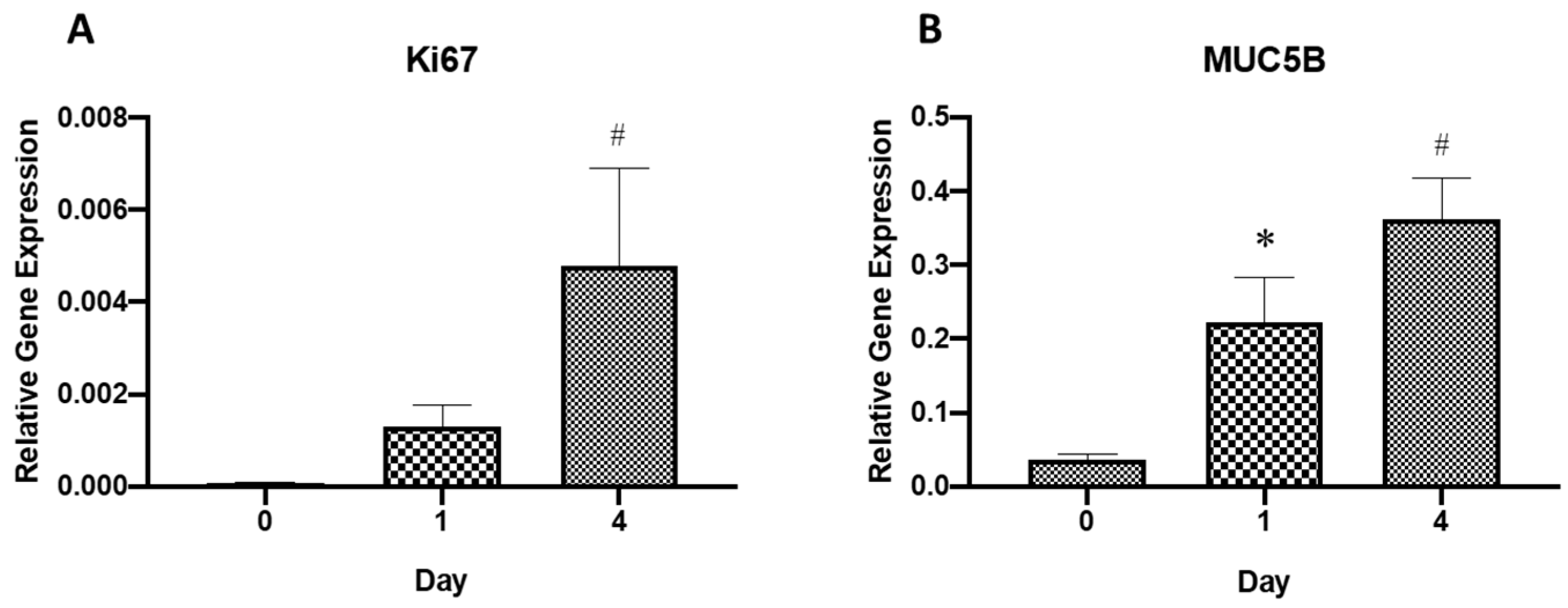
2.3. Gene Expression Analysis
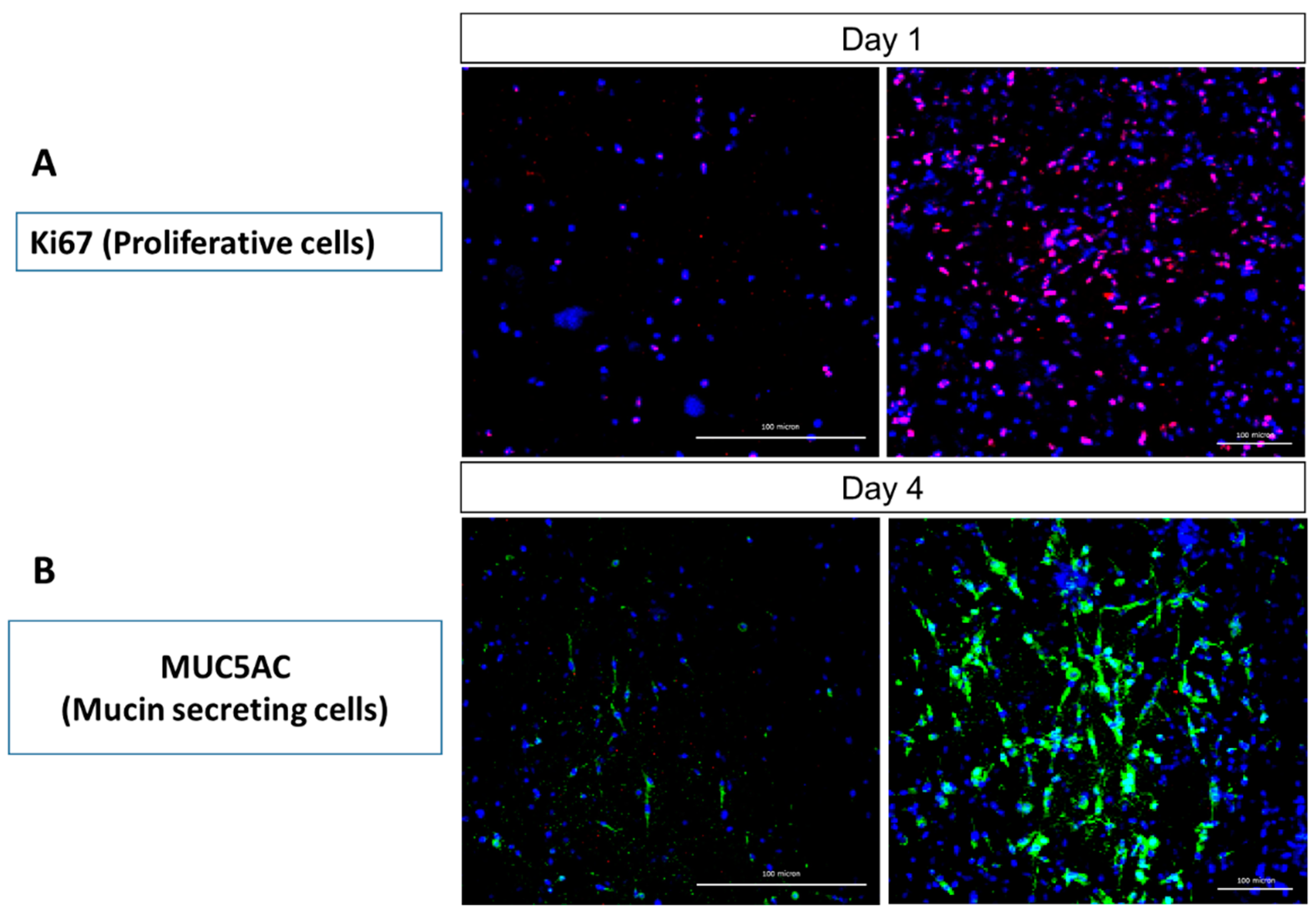
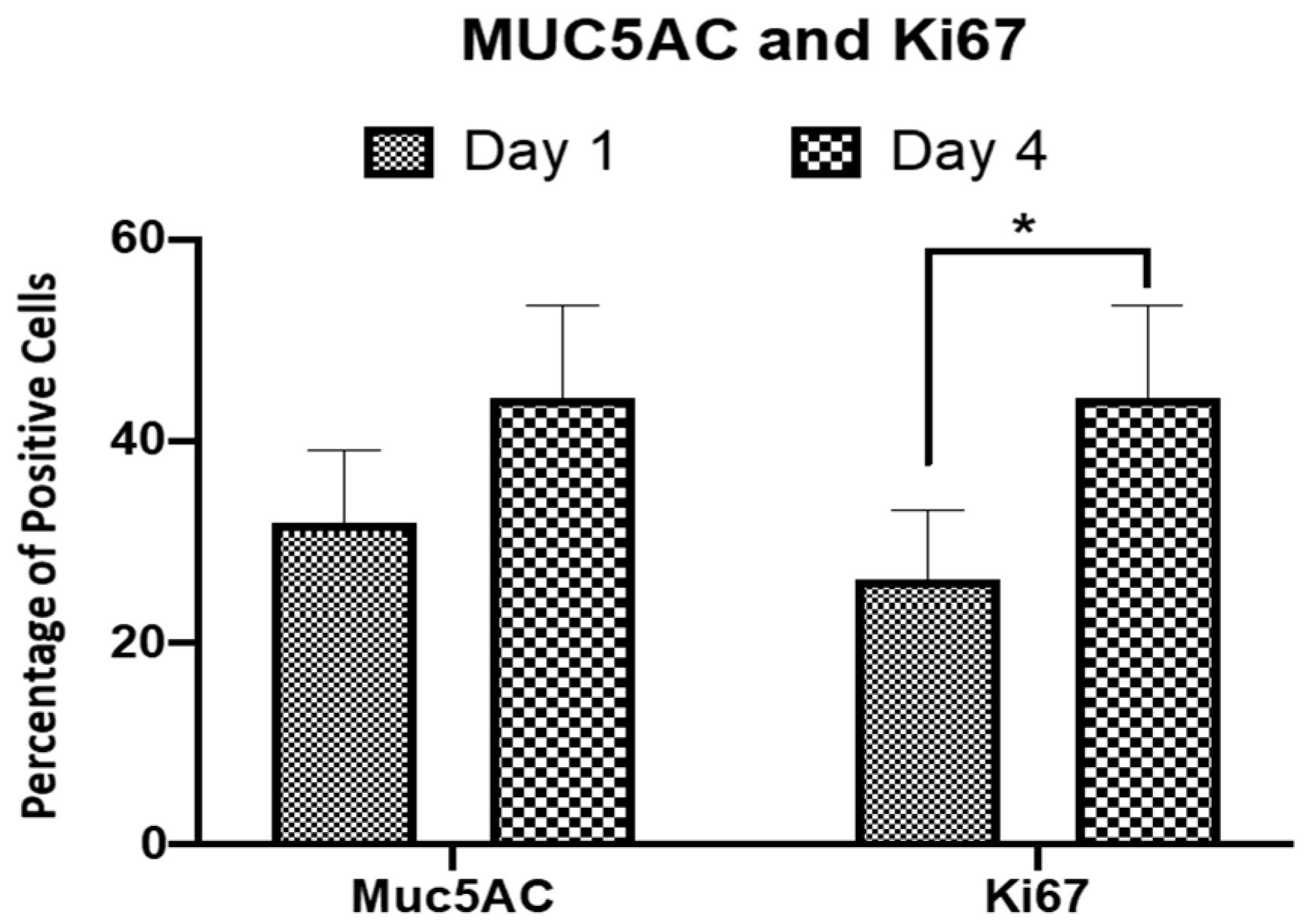
2.4. Immunocytochemical Analysis
2.5. Profile of Respiratory Epithelial Cell Population within HTREC
3. Discussion
4. Materials and Methods
4.1. Respiratory Epithelial and Fibroblast Cell Isolation and Culture
4.2. Human Plasma Preparation as Biomaterial
4.3. Human Tissue Respiratory Epithelial Construct (HTREC) Formation
4.4. Histological Analysis
4.5. Gene Expression Analysis
4.5.1. Total RNA Extraction
4.5.2. Complementary DNA Synthesis and Real-Time Reverse Transcriptase Polymerase Chain Reaction
4.6. Immunocytochemistry
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Sample Availability
References
- Vu, H.V.; Huynh, K.; Nguyen, V.D.Q. Surgical reconstruction for congenital tracheal malformation and pulmonary artery sling. J. Cardiothorac. Surg. 2019, 14, 49. [Google Scholar] [CrossRef] [Green Version]
- Maller, B.; Kaszuba, F.; Tanvetyanon, T. Complete Tumor Response of Tracheal Squamous Cell Carcinoma After Treatment with Pembrolizumab. Ann. Thorac. Surg. 2019, 107, e273–e274. [Google Scholar] [CrossRef]
- Daidoji, T.; Kajikawa, J.; Arai, Y.; Watanabe, Y.; Hirose, R.; Nakaya, T. Infection of Human Tracheal Epithelial Cells by H5 Avian Influenza Virus Is Regulated by the Acid Stability of Hemagglutinin and the pH of Target Cell Endosomes. Viruses 2020, 12, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casazza, G.; Graham, M.E.; Nelson, U.; Chaulk, D.; Sandweiss, D.; Meier, J. Pediatric Bacterial Tracheitis—A Variable Entity: Case Series with Literature Review. Otolaryngol. Neck Surg. 2018, 160, 546–549. [Google Scholar] [CrossRef]
- Abou-Arab, O.; Huette, P.; Berna, P.; Mahjoub, Y. Tracheal trauma after difficult airway management in morbidly obese patients with COVID-19. Br. J. Anaesth. 2020, 125, e168–e170. [Google Scholar] [CrossRef] [PubMed]
- Daneshi, A.; Mohammadi, S.; Hassannia, F. Delayed Laryngotracheal Reconstruction with Titanium Plate: Report of 10 Cases. J. Voice 2010, 24, 755–757. [Google Scholar] [CrossRef]
- Yener, M.; Acar, G.O.; Cansiz, H.; Öz, B.; Cigerciogullari, E.; Seymen, O. Use of titanium mesh in laryngotracheal reconstruction: An experimental study on rabbits. Eur. Arch. Oto-Rhino-Laryngol. 2010, 267, 1247–1253. [Google Scholar] [CrossRef]
- Carvalho, T.; Guedes, G.; Sousa, F.L.; Freire, C.; Santos, H.A. Latest Advances on Bacterial Cellulose-Based Materials for Wound Healing, Delivery Systems, and Tissue Engineering. Biotechnol. J. 2019, 14, 1900059. [Google Scholar] [CrossRef] [PubMed]
- Aoki, F.; Varma, R.; Marin-Araujo, A.E.; Lee, H.; Soleas, J.P.; Li, A.H.; Soon, K.; Romero, D.; Moriya, H.T.; Haykal, S.; et al. De-epithelialization of porcine tracheal allografts as an approach for tracheal tissue engineering. Sci. Rep. 2019, 9, 12034. [Google Scholar] [CrossRef]
- Lokanathan, Y.; Fauzi, M.; Man, R.C.; Rashidbenam, Z.; Bin Saim, A.; Idrus, R.B.H.; Yunus, M.M. Preliminary Study on the Development of In Vitro Human Respiratory Epithelium Using Collagen Type I Scaffold as a Potential Model for Future Tracheal Tissue Engineering. Appl. Sci. 2021, 11, 1787. [Google Scholar] [CrossRef]
- Miyamoto, T.; Takahashi, S.-I.; Ito, H.; Inagaki, H.; Noishiki, Y. Tissue biocompatibility of cellulose and its derivatives. J. Biomed. Mater. Res. 1989, 23, 125–133. [Google Scholar] [CrossRef]
- Märtson, M.; Viljanto, J.; Hurme, T.; Laippala, P.; Saukko, P. Is cellulose sponge degradable or stable as implantation material? An in vivo subcutaneous study in the rat. Biomaterials 1999, 20, 1989–1995. [Google Scholar] [CrossRef]
- Tsukada, H.; Gangadharan, S.; Garland, R.; Herth, F.; DeCamp, M.; Ernst, A. Tracheal Replacement with a Bioabsorbable Scaffold in Sheep. Ann. Thorac. Surg. 2010, 90, 1793–1797. [Google Scholar] [CrossRef]
- Cheng, S.-F.; Wu, S.; Li, Q.-P.; Sang, H.-Y.; Fan, Z.-Y. Airway reconstruction using decellularized aortic xenografts in a dog model. Organogenesis 2020, 16, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Macchiarini, P.; Jungebluth, P.; Go, T.; Asnaghi, M.A.; Rees, L.E.; Cogan, T.A.; Dodson, A.; Martorell, J.; Bellini, S.; Parnigotto, P.P.; et al. Clinical transplantation of a tissue-engineered airway. Lancet 2008, 372, 2023–2030. [Google Scholar] [CrossRef]
- Heikal, M.; Aminuddin, B.; Jeevana, J.; Chen, H.C.; Sharifah, S.; Ruszymah, B.H. A scanning electron microscopic study of in vivi tissue engineered respiratory epithelium in sheep. Med. J. Malays. 2008, 63 (Suppl. A), 34. [Google Scholar]
- Heikal, M.M.; Aminuddin, B.; Jeevanan, J.; Chen, H.; Sharifah, S.; Ruszymah, B. Autologous Implantation of Bilayered Tissue-Engineered Respiratory Epithelium for Tracheal Mucosal Regenesis in a Sheep Model. Cells Tissues Organs 2010, 5, 292–302. [Google Scholar] [CrossRef]
- Heikal, M.; Roy Chowdhury, S.; Busra, M.; Aminuddin, B.; Ruszymah, B. Quality evaluation of human tissue engineered respiratory epithelium constructs. Regen. Res. 2012, 1, 61. [Google Scholar]
- Hsu, D.; Katelaris, C. Long-term management of patients taking immunosuppressive drugs. Aust. Prescr. 2009, 32, 68–71. [Google Scholar] [CrossRef]
- Kobayashi, K.; Nomoto, Y.; Suzuki, T.; Tada, Y.; Miyake, M.; Hazama, A.; Kanemaru, S.; Nakamura, T.; Omori, K. Effect of Fibroblasts on Tracheal Epithelial Regeneration in Vitro. Tissue Eng. 2006, 12, 2619–2628. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Stratton, C.W.; Tang, Y.-W. Outbreak of pneumonia of unknown etiology in Wuhan, China: The mystery and the miracle. J. Med. Virol. 2020, 92, 401–402. [Google Scholar] [CrossRef] [Green Version]
- Dinakaran, D.; Manjunatha, N.; Kumar, C.N.; Suresh, B.M. Aspectos neuropsiquiátricos de la pandemia de COVID-19: Una revisión selectiva. Asian J. Psychiatry 2020, 53, 102188. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Sandefur, B.J.; Niven, A.S.; Gleich, S.J.; Daxon, B. Practical Guidance for Tracheal Intubation of Patients with COVID-19. Mayo Clin. Proc. 2020, 95, 2327–2331. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, A.; Sokhi, J.; Lockie, C.; Ward, P.A. Emergency Tracheal Intubation in Patients with COVID-19: Experience from a UK Centre. Anesthesiol. Res. Pr. 2020, 2020, 8816729. [Google Scholar]
- Lim, H.; Kim, J.H.; Kim, D.; Lee, J.; Son, J.S.; Kim, D.C.; Ko, S. Tracheal rupture after endotracheal intubation—A report of three cases. Korean J. Anesthesiol. 2012, 62, 277–280. [Google Scholar] [CrossRef] [Green Version]
- Sristava, P.; Kumar, A.; Asaf, B.B. Tracheal Reconstruction after Post-Tracheostomy Tracheal Stenosis under Cross-Field Anesthesia. J. Anesth. Crit. Care Open Access 2017, 9, 00331. [Google Scholar]
- Luengen, A.E.; Kniebs, C.; Buhl, E.M.; Cornelissen, C.G.; Schmitz-Rode, T.; Jockenhoevel, S.; Thiebes, A.L. Choosing the Right Differentiation Medium to Develop Mucociliary Phenotype of Primary Nasal Epithelial Cells In Vitro. Sci. Rep. 2020, 10, 6963. [Google Scholar] [CrossRef]
- Maughan, E.F.; Hynds, R.E.; Proctor, T.J.; Janes, S.M.; Elliott, M.; Birchall, M.A.; Lowdell, M.W.; De Coppi, P. Autologous Cell Seeding in Tracheal Tissue Engineering. Curr. Stem Cell Rep. 2017, 3, 279–289. [Google Scholar] [CrossRef] [Green Version]
- Kojima, K.; Bonassar, L.J.; Roy, A.K.; Mizuno, H.; Cortiella, J.; Vacanti, C.A. A composite tissue-engineered trachea using sheep nasal chondrocyte and epithelial cells. FASEB J. 2003, 17, 823–828. [Google Scholar] [CrossRef] [PubMed]
- Noruddin, N.A.A.; Bin Saim, A.; Chua, K.H.; Idrus, R. Human Nasal Turbinates as a Viable Source of Respiratory Epithelial Cells Using Co-Culture System Versus Dispase Dissociation Technique. Laryngoscope 2007, 117, 2139–2145. [Google Scholar] [CrossRef] [PubMed]
- Yunus, M.H.M.; Siang, K.C.; Hashim, N.I.; Zhi, N.P.; Zamani, N.F.; Sabri, P.P.; Busra, M.F.; Chowdhury, S.R.; Idrus, R.B.H. The effects of human serum to the morphology, proliferation and gene expression level of the respiratory epithelium in vitro. Tissue Cell 2014, 46, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.-W.; Li, S.-T.; Young, T.-H. Chitosan-hyaluronan: Promotion of mucociliary differentiation of respiratory epithelial cells and development of olfactory receptor neurons. Artif. Cells Nanomed. Biotechnol. 2019, 47, 564–570. [Google Scholar] [CrossRef] [Green Version]
- Man, R.C.; Lokanathan, Y.; Razali, R.A.; Chowdury, S.R.; Bin Saim, A.; Idrus, R.B.H. Nasal Fibroblast Conditioned Medium Promotes Cell Attachment and Migration of Human Respiratory Epithelium. Sains Malays. 2020, 49, 429–437. [Google Scholar] [CrossRef]
- Rabiatul, A.; Lokanathan, Y.; Rohaina, C.; Chowdhury, S.; Aminuddin, B.; Ruszymah, B. Surface modification of electrospun poly(methyl methacrylate) (PMMA) nanofibers for the development of in vitro respiratory epithelium model. J. Biomater. Sci. Polym. Ed. 2016, 26, 1297–1311. [Google Scholar] [CrossRef]
- Park, J.H.; Hong, J.M.; Ju, Y.M.; Jung, J.W.; Kang, H.-W.; Lee, S.J.; Yoo, J.J.; Kim, S.W.; Kim, S.H.; Cho, D.-W. A novel tissue-engineered trachea with a mechanical behavior similar to native trachea. Biomaterials 2015, 62, 106–115. [Google Scholar] [CrossRef]
- Cheung, N.H.; Napolitano, L.M. Tracheostomy: Epidemiology, Indications, Timing, Technique, and Outcomes. Respir. Care 2014, 59, 895–919. [Google Scholar] [CrossRef] [Green Version]
- Alam, H.; Sehgal, L.; Kundu, S.; Dalal, S.N.; Vaidya, M.M. Novel function of keratins 5 and 14 in proliferation and differentiation of stratified epithelial cells. Mol. Biol. Cell 2011, 22, 4068–4078. [Google Scholar] [CrossRef]
- Dowsett, M.; Nielsen, T.O.; A’Hern, R.; Bartlett, J.; Coombes, R.C.; Cuzick, J.; Ellis, M.; Henry, N.L.; Hugh, J.C.; Lively, T.; et al. Assessment of Ki67 in Breast Cancer: Recommendations from the International Ki67 in Breast Cancer Working Group. J. Natl. Cancer Inst. 2011, 103, 1656–1664. [Google Scholar] [CrossRef] [Green Version]
- Menz, A.; Weitbrecht, T.; Gorbokon, N.; Büscheck, F.; Luebke, A.M.; Kluth, M.; Hube-Magg, C.; Hinsch, A.; Höflmayer, D.; Weidemann, S.; et al. Diagnostic and prognostic impact of cytokeratin 18 expression in human tumors: A tissue microarray study on 11,952 tumors. Mol. Med. 2021, 27, 16. [Google Scholar] [CrossRef]
- Okuda, K.; Chen, G.; Subramani, D.B.; Wolf, M.; Gilmore, R.C.; Kato, T.; Radicioni, G.; Kesimer, M.; Chua, M.; Dang, H.; et al. Localization of Secretory Mucins MUC5AC and MUC5B in Normal/Healthy Human Airways. Am. J. Respir. Crit. Care Med. 2019, 199, 715–727. [Google Scholar] [CrossRef]
- Kanaji, N.; Bandoh, S.; Ishii, T.; Fujita, J.; Ishida, T.; Matsunaga, T.; Kubo, A. Cytokeratins negatively regulate the invasive potential of lung cancer cell lines. Oncol. Rep. 2011, 26, 763–768. [Google Scholar] [CrossRef]
- Leiva-Juárez, M.M.; Kolls, J.K.; Evans, S.E. Lung epithelial cells: Therapeutically inducible effectors of antimicrobial defense. Mucosal Immunol. 2018, 11, 21–34. [Google Scholar] [CrossRef]
- Lillehoj, E.P.; Kato, K.; Lu, W.; Kim, K.C. Cellular and Molecular Biology of Airway Mucins. Int. Rev. Cell Mol. Biol. 2013, 303, 139–202. [Google Scholar] [PubMed] [Green Version]
- Crystal, R.G.; Randell, S.H.; Engelhardt, J.F.; Voynow, J.; Sunday, M.E. Airway Epithelial Cells: Current Concepts and Challenges. Proc. Am. Thorac. Soc. 2008, 5, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Santos, S.C.N.D.S.; Sigurjonsson, Ó.E.; Custódio, C.D.A.; Mano, J.F. Blood Plasma Derivatives for Tissue Engineering and Regenerative Medicine Therapies. Tissue Eng. Part B Rev. 2018, 24, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Lin, T.; Huang, N.; Xia, X.; Li, J.; Qiu, Y.; Yang, X.; Mao, H.; Huang, F. Plasma fibrinogen and mortality in patients undergoing peritoneal dialysis: A prospective cohort study. BMC Nephrol. 2020, 21, 349. [Google Scholar] [CrossRef] [PubMed]
- Egorikhina, M.N.; Aleynik, D.Y.; Rubtsova, Y.P.; Levin, G.Y.; Charykova, I.N.; Semenycheva, L.L.; Bugrova, M.L.; Zakharychev, E.A. Hydrogel scaffolds based on blood plasma cryoprecipitate and collagen derived from various sources: Structural, mechanical and biological characteristics. Bioact. Mater. 2019, 4, 334–345. [Google Scholar] [CrossRef] [PubMed]
- Hielscher, A.; Ellis, K.; Qiu, C.; Porterfield, J.; Gerecht, S. Fibronectin deposition participates in extracellular matrix assembly and vascular morphogenesis. PLoS ONE 2016, 11, 0147600. [Google Scholar] [CrossRef] [Green Version]
- Martino, M.; Briquez, P.S.; Ranga, A.; Lutolf, M.P.; Hubbell, J.A. Heparin-binding domain of fibrin(ogen) binds growth factors and promotes tissue repair when incorporated within a synthetic matrix. Proc. Natl. Acad. Sci. USA 2013, 110, 4563–4568. [Google Scholar] [CrossRef] [Green Version]
- Hadjipanayi, E.; Kuhn, P.-H.; Moog, P.; Bauer, A.-T.; Kuekrek, H.; Mirzoyan, L.; Hummel, A.; Kirchhoff, K.; Salgin, B.; Isenburg, S.; et al. The fibrin matrix regulates angiogenic responses within the hemostatic microenvironment through biochemical control. PLoS ONE 2015, 10, 0135618. [Google Scholar] [CrossRef]
- Meinhart, J.; Fussenegger, M.; Höbling, W. Stabilization of Fibrin-Chondrocyte Constructs for Cartilage Reconstruction. Ann. Plast. Surg. 1999, 42, 673–678. [Google Scholar] [CrossRef]
- Natarajan, N.; Shashirekha, V.; Noorjahan, S.E.; Rameshkumar, M.; Rose, C.; Sastry, T.P. Fibrin–Chitosan–Gelatin Composite Film: Preparation and Characterization. J. Macromol. Sci. Part A Pure Appl. Chem. 2005, 42A, 945–953. [Google Scholar] [CrossRef]
- Trombi, L.; Danti, S.; Savelli, S.; Moscato, S.; D’Alessandro, D.; Ricci, C.; Giannotti, S.; Petrini, M. Mesenchymal Stromal Cell Culture and Delivery in Autologous Conditions: A Smart Approach for Orthopedic Applications. J. Vis. Exp. 2016, 2016, 54845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barmore, W.; Bajwa, T.; Burns, B. Biochemistry, Clotting Factors; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar] [PubMed]
- Gessmann, J.; Seybold, D.; Peter, E.; Schildhauer, T.A.; Köller, M. Plasma clots gelled by different amounts of calcium for stem cell delivery. Langenbecks Arch. Surg. 2012, 398, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi-Ataabadi, M.; Mostafavi-Pour, Z.; Vojdani, Z.; Sani, M.; Latifi, M.; Talaei-Khozani, T. Fabrication and characterization of platelet-rich plasma scaffolds for tissue engineering applications. Mater. Sci. Eng. C 2017, 71, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Singh, D.; Choi, S.M.; Han, S.S. Enhanced Proliferation and Growth of Human Lung Epithelial Cells on Gelatin Microparticle Loaded with Ephedra Extracts. J. Nanomater. 2013, 2013, 14. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Accession No. | Primers 5′ → 3′ |
|---|---|---|
| GADPH | BC0203308 | F: 5′-TCC CTG AGC TGA ACG GGA AG-3′ R: 5′-GGA GGA GTG GGT GTC GCT GT-3′ |
| MUC5B | U95031 | F: 5′-GTC AAC AGC CAT GTG GAC AAC-3′ R: 5′-CTC CTC ACA GGA GTA GCA GCA-3′ |
| Ki67 | NM-002417 | F: 5′-GGC TCT AGA GGA CCT GGT TGG-3′ R: 5′-GCT GAC TGC TAG GGG CTC TTC-3′ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohd Yunus, M.H.; Rashidbenam, Z.; Fauzi, M.B.; Bt Hj Idrus, R.; Bin Saim, A. Evaluating Feasibility of Human Tissue Engineered Respiratory Epithelium Construct as a Potential Model for Tracheal Mucosal Reconstruction. Molecules 2021, 26, 6724. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26216724
Mohd Yunus MH, Rashidbenam Z, Fauzi MB, Bt Hj Idrus R, Bin Saim A. Evaluating Feasibility of Human Tissue Engineered Respiratory Epithelium Construct as a Potential Model for Tracheal Mucosal Reconstruction. Molecules. 2021; 26(21):6724. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26216724
Chicago/Turabian StyleMohd Yunus, Mohd Heikal, Zahra Rashidbenam, Mh Busra Fauzi, Ruszymah Bt Hj Idrus, and Aminuddin Bin Saim. 2021. "Evaluating Feasibility of Human Tissue Engineered Respiratory Epithelium Construct as a Potential Model for Tracheal Mucosal Reconstruction" Molecules 26, no. 21: 6724. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26216724