
Rhenium Radioisotopes for Medicine, a Focus on Production and Applications

 , ,
, ,  , , , ,
, , , ,
Abstract
:1. Introduction
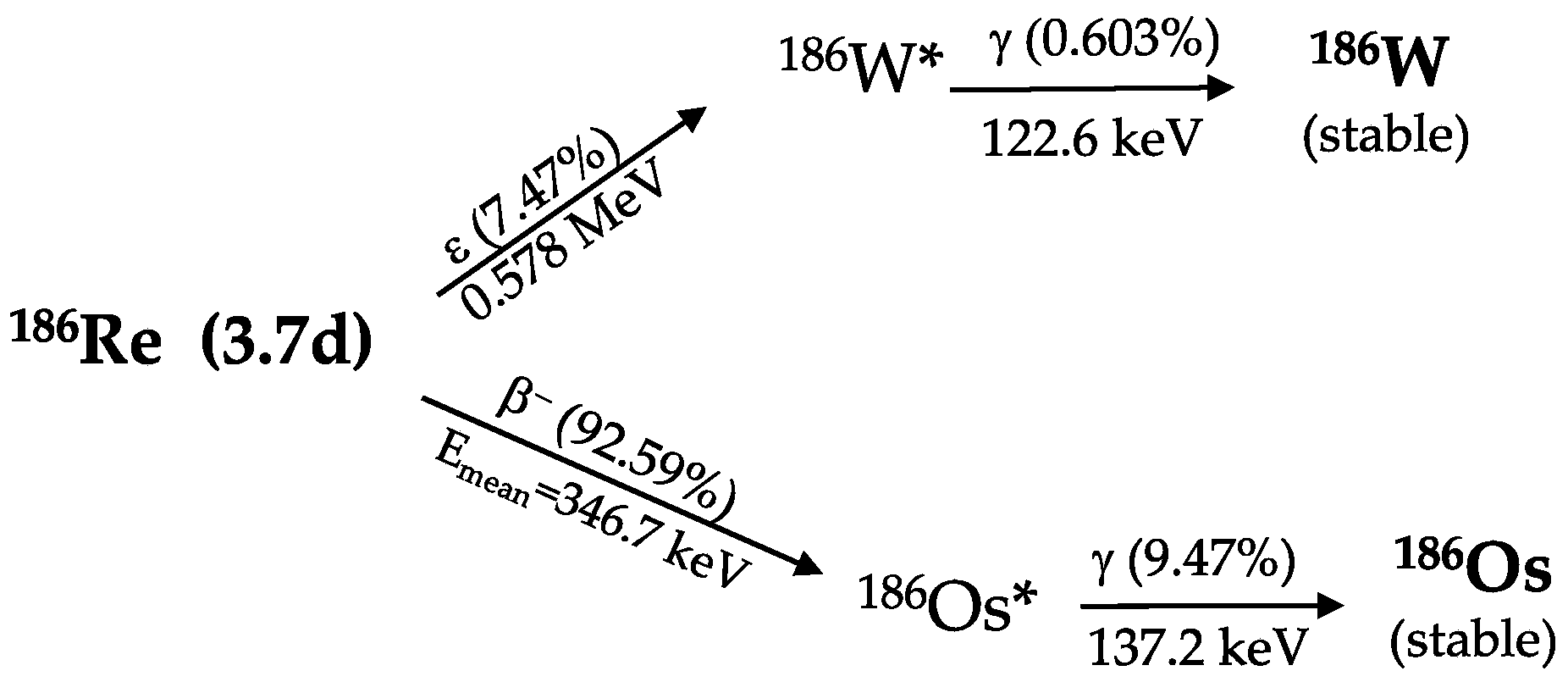
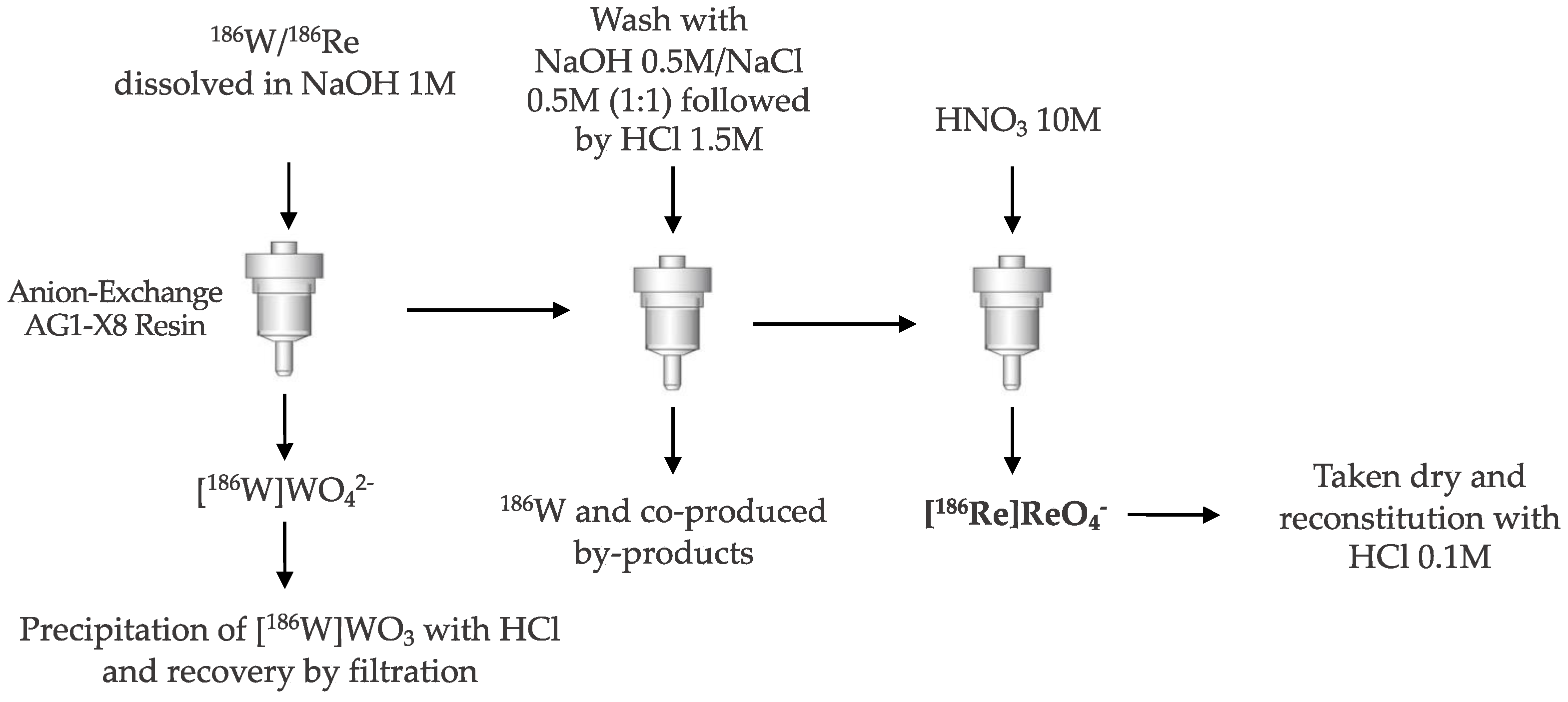
2. Rhenium-186 Nuclear Properties and Production
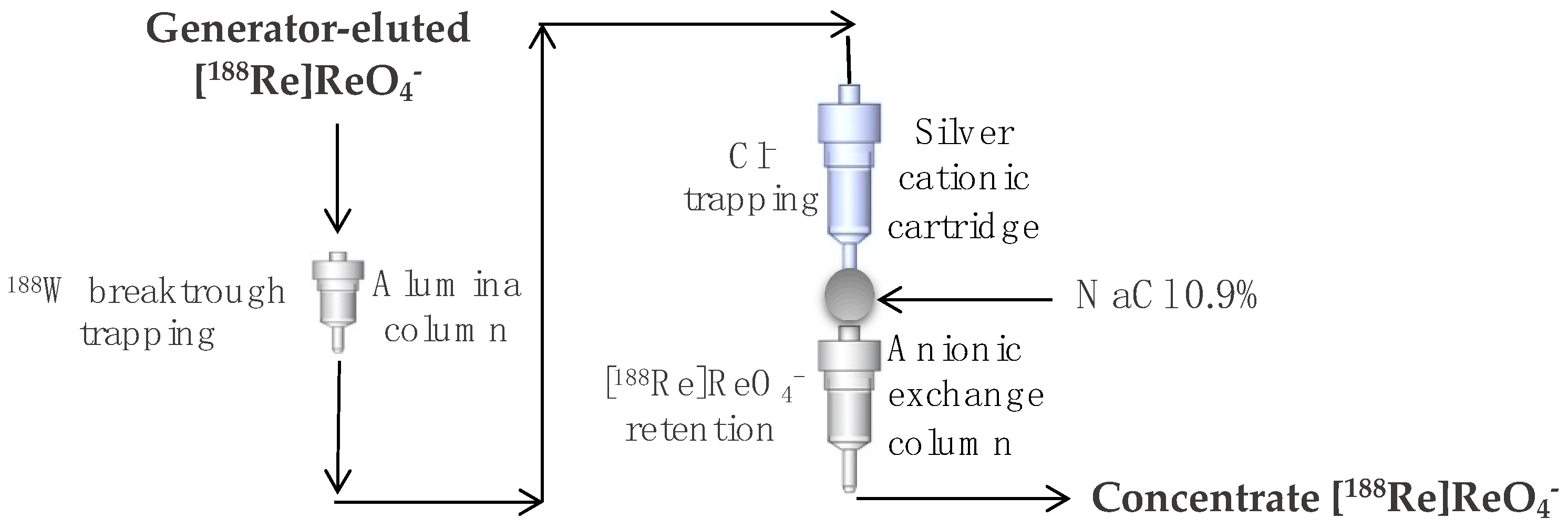
3. Rhenium-188 Nuclear Properties and Production
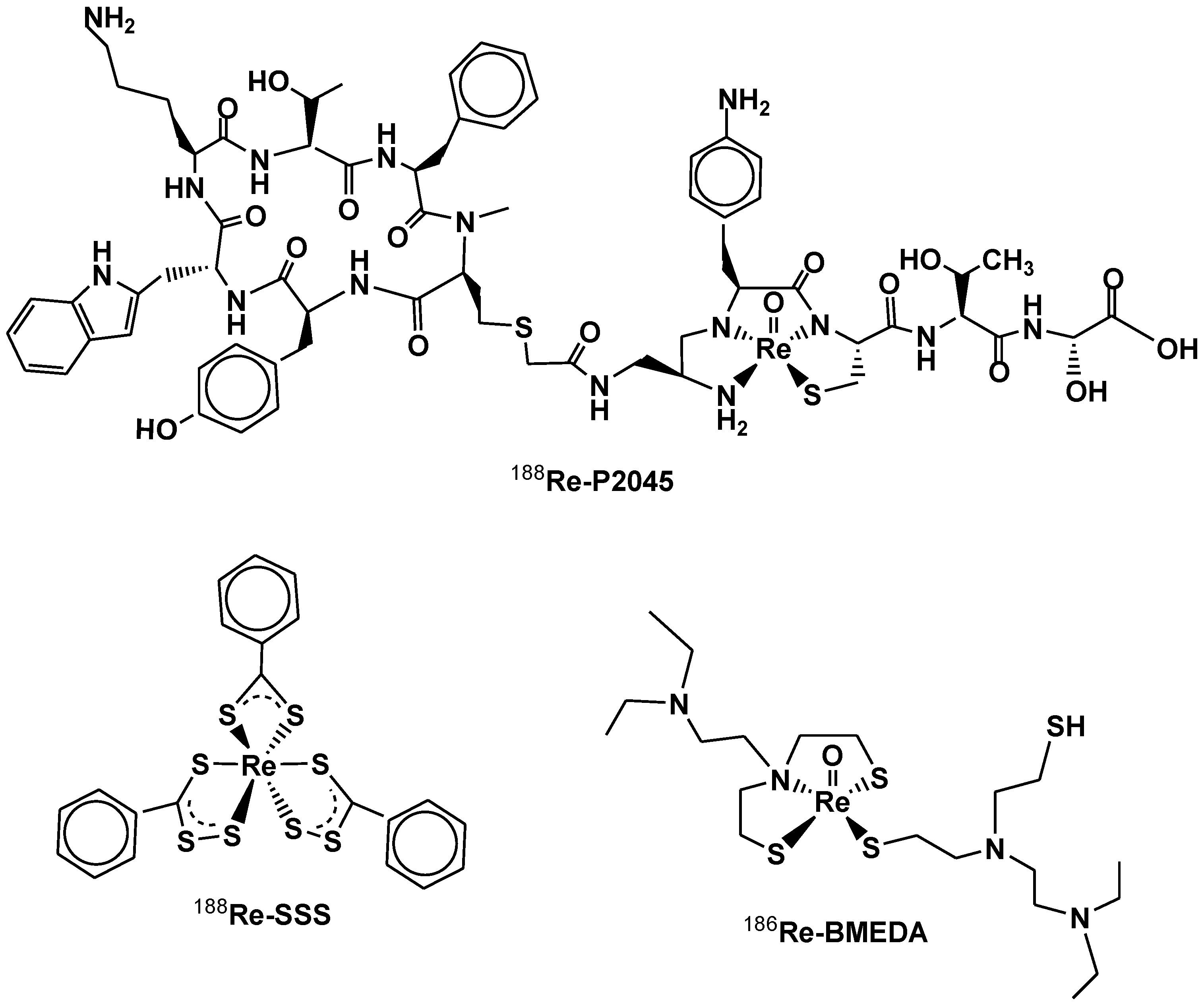
4. Chemistry of Rhenium Radiopharmaceuticals
5. 188/186 Re-Radiopharmaceuticals Clinical Application
5.1. “Maximum Tolerated Dose, Safety, and Efficacy of Rhenium Nanoliposomes in Recurrent Glioma” and “Intraventricular Administration of 186Re-NanoLiposome for Leptomeningeal Metastases”
5.2. “Multicentre Canadian Study to Measure the Safety and Efficacy of Radiosynoviorthesis”
5.3. ”Rhenium-Skin Cancer Therapy (SCT) for the Treatment of Non-Melanoma Skin Cancer” (Phase IV, NCT05135052, Recruiting)
5.4. “Rhenium-188-HEDP vs. Radium-223-chloride in Patients with Advanced Prostate Cancer Refractory to Hormonal Therapy” (Phase III, NCT03458559, Active, Not Recruiting)
5.5. “Rhenium 188Re-P2045 in Small Cell Lung Cancer and Other Advanced Neuroendocrine Carcinoma” and “188Re-P2045 in Patients with Lung Cancer Who Have Received or Refused to Receive Prior Chemotherapy”
5.6. “188Re-SSS Lipiodol to Treat HepatoCellular Carcinomas” (NCT0112646, Phase I, Completed)
5.7. “HER2 Expression Detection and Radionuclide Therapy in Breast Cancer Using 99mTc/188Re Labeled Single Domain Antibody (NCT04674722, Phase I, Recruiting)
5.8. Treatment of Non-Responding to Conventional Therapy Inoperable Liver Cancers by in Situ Introduction of ImDendrim (NCT03255343)
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Qaim, S.M. Nuclear data for medical applications: An overview. Radiochim. Acta 2001, 89, 189–196. [Google Scholar] [CrossRef]
- Boschi, A.; Martini, P.; Uccelli, L. 188Re(V) Nitrido Radiopharmaceuticals for Radionuclide Therapy. Pharmaceuticals 2017, 10, 12. [Google Scholar] [CrossRef]
- Kassis, A.I.; Adelstein, S.J. Radiobiologic Principles in Radionuclide Therapy. J. Nucl. Med. 2005, 46, 4S–12S. [Google Scholar] [PubMed]
- Uccelli, L.; Boschi, A.; Cittanti, C.; Martini, P.; Panareo, S.; Tonini, E.; Nieri, A.; Urso, L.; Caracciolo, M.; Lodi, L.; et al. 90Y/177Lu-DOTATOC: From preclinical studies to application in humans. Pharmaceutics 2021, 13, 1463. [Google Scholar] [CrossRef] [PubMed]
- NNDC. National Nuclear Data Center. Available online: https://www.nndc.bnl.gov/ (accessed on 7 August 2022).
- Mastren, T.; Radchenko, V.; Bach, H.T.; Balkin, E.R.; Birnbaum, E.R.; Brugh, M.; Engle, J.W.; Gott, M.D.; Guthrie, J.; Hennkens, H.M.; et al. Bulk production and evaluation of high specific activity 186gRe for cancer therapy using enriched 186WO3 targets in a proton beam. Nucl. Med. Biol. 2017, 49, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Batchelder, J.C.; Hurst, A.M.; Basunia, M.S. Nuclear Data Sheets for A=186. Nucl. Data Sheets 2022, 183, 346. [Google Scholar] [CrossRef]
- Ehrhardt, G.J.; Ketring, A.R.; Ayers, L.M. Reactor-produced radionuclides at the University of Missouri Research Reactor. Appl. Radiat. Isot. 1998, 49, 295–297. [Google Scholar] [CrossRef]
- NuDat 3. Available online: https://www.nndc.bnl.gov/nudat3/ (accessed on 7 August 2022).
- Szelecsényi, F.; Steyn, A.G.F.; Kovács, A.Z.; Aardaneh, A.K.; Vermeulen, A.C.; Van Der Walt, A.T.N. Production possibility of 186 Re via the 192 Os(p,a3n) 186 Re nuclear reaction. J. Radioanal. Nucl. Chem. 2009, 282, 261–263. [Google Scholar] [CrossRef]
- Hussain, M.; Sudár, S.; Aslam, M.N.; Malik, A.A.; Ahmad, R.; Qaim, S.M. Evaluation of charged particle induced reaction cross section data for production of the important therapeutic radionuclide 186Re. Radiochim. Acta 2010, 98, 385–395. [Google Scholar] [CrossRef]
- Balkin, E.R.; Gagnon, K.; Strong, K.T.; Smith, B.E.; Dorman, E.F.; Emery, R.C.; Pauzauskie, P.J.; Fassbender, M.E.; Cutler, C.S.; Ketring, A.R.; et al. Deuteron irradiation of W and WO3 for production of high specific activity 186Re: Challenges associated with thick target preparation. Appl. Radiat. Isot. 2016, 115, 197–207. [Google Scholar] [CrossRef]
- Balkin, E.R.; Gagnon, K.; Dorman, E.; Emery, R.; Li, Y.; Lake Wooten, A.; Smith, B.E.; Strong, K.T.; Pauzauskie, P.J.; Fassbender, M.E.; et al. Scale-up of high specific activity 186gRe production using graphite-encased thick 186W targets and demonstration of an efficient target recycling process. Radiochim. Acta 2017, 105, 1071–1081. [Google Scholar] [CrossRef]
- Moustapha, M.E.; Ehrhardt, G.J.; Smith, C.J.; Szajek, L.P.; Eckelman, W.C.; Jurisson, S.S. Preparation of cyclotron-produced 186Re and comparison with reactor-produced 186Re and generator-produced 188Re for the labeling of bombesin. Nucl. Med. Biol. 2006, 33, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Richards, V.N.; Rath, N.; Lapi, S.E. Production and separation of 186gRe from proton bombardment of 186WC. Nucl. Med. Biol. 2015, 42, 530–535. [Google Scholar] [CrossRef]
- Novgorodov, A.F.; Bruchertseifer, F.; Brockmann, J.; Lebedev, N.A.; Rösch, F. Thermochromatographic separation of no-carrier-added 186Re or 188Re from tungsten targets relevant to nuclear medical applications. Radiochim. Acta 2000, 88, 163–168. [Google Scholar] [CrossRef]
- Uccelli, L.; Martini, P.; Pasquali, M.; Boschi, A. Monoclonal Antibodies Radiolabeling with Rhenium-188 for Radioimmunotherapy. BioMed Res. Int. 2017, 2017, 5923609. [Google Scholar] [CrossRef]
- Knapp, F.F.; Kropp, J.; Liepe, K. Rhenium-188 Generator-Based Radiopharmaceuticals for Therapy. In Therapeutic Nuclear Medicine; Springer: Berlin/Heidelberg, Germany, 2012; pp. 51–81. (In Russian) [Google Scholar] [CrossRef]
- Boschi, A.; Uccelli, L.; Pasquali, M.; Duatti, A.; Taibi, A.; Pupillo, G.; Esposito, J. 188W/188Re generator system and its therapeutic applications. J. Chem. 2014, 2014, 529406. [Google Scholar] [CrossRef]
- Mirzadeh, S.; Knapp, F.F.; Callahan, A.P. Production of Tungsten-188 and Osmium-194 in a Nuclear Reactor for New Clinical Generators. In Proceedings of the International Conference, Forschungszentrum Jülich, Germany, 13–17 May 1991; pp. 595–597. [Google Scholar] [CrossRef]
- Knapp, F.F. Rhenium-188–A Generator-Derived Radioisotope for Cancer Therapy. Cancer Biother. Radiopharm 2009, 13, 337–349. [Google Scholar] [CrossRef] [PubMed]
- Mushtaq, A. Concentration of 99mtco4−/reo4− by a single, compact, anion exchange cartridge. Nucl. Med. Commun. 2004, 25, 957–962. [Google Scholar] [CrossRef]
- Chakravarty, R.; Dash, A.; Pillai, M.R.A.; Venkatesh, M. Post-elution concentration of 188Re by an electrochemical method. Appl. Radiat. Isot. 2010, 68, 2302–2305. [Google Scholar] [CrossRef]
- Khomutov, N.E. Electrochemistry: Electrodeposition of Metals and Alloys, Achievements in Science: Chemistry Series; Israel Program for Scientific Translations: Jerusalem, Israel, 1969. [Google Scholar]
- Deutsch, E.; Libson, K.; Vanderheyden, J.L.; Ketring, A.R.; Maxon, H.R. The chemistry of rhenium and technetium as related to the use of isotopes of these elements in therapeutic and diagnostic nuclear medicine. Int. J. Radiat. Appl. Instrum. Part B Nucl. Med. Biol. 1986, 13, 465–477. [Google Scholar] [CrossRef]
- Lange, R.; de Klerk, J.M.H.; Bloemendal, H.J.; Ramakers, R.M.; Beekman, F.J.; van der Westerlaken, M.M.L.; Hendrikse, N.H.; ter Heine, R. Drug composition matters: The influence of carrier concentration on the radiochemical purity, hydroxyapatite affinity and in-vivo bone accumulation of the therapeutic radiopharmaceutical 188Rhenium-HEDP. Nucl. Med. Biol. 2015, 42, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Mallia, M.B.; Chirayil, V.; Dash, A. Improved freeze-dried kit for the preparation of 188ReN-DEDC/lipiodol for the therapy of unresectable hepatocellular carcinoma. Appl. Radiat. Isot. 2018, 137, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Bolzati, C.; Boschi, A.; Uccelli, L.; Duatti, A.; Franceschini, R.; Piffanelli, A. An alternative approach to the preparation of 188Re radiopharmaceuticals from generator-produced [188ReO4]−: Efficient synthesis of 188Re(V)-meso-2,3-dimercaptosuccinic acid. Nucl. Med. Biol. 2000, 27, 309–314. [Google Scholar] [CrossRef]
- Boschi, A.; Bolzati, C.; Uccelli, L.; Duatti, A. High-yield synthesis of the terminal 188Re≡N multiple bond from generator-produced [188ReO4]−. Nucl. Med. Biol. 2003, 30, 381–387. [Google Scholar] [CrossRef]
- Smilkov, K.; Janevik, E.; Guerrini, R.; Pasquali, M.; Boschi, A.; Uccelli, L.; Di Domenico, G.; Duatti, A. Preparation and first biological evaluation of novel Re-188/Tc-99m peptide conjugates with substance-P. Appl. Radiat. Isot. 2014, 92, 25–31. [Google Scholar] [CrossRef]
- Boschi, A.; Uccelli, L.; Pasquali, M.; Pasqualini, R.; Guerrini, R.; Duatti, A. Mixed Tridentate π-Donor and Monodentate π-Acceptor Ligands as Chelating Systems for Rhenium-188 and Technetium-99m Nitrido Radiopharmaceuticals. Curr. Radiopharm. 2014, 6, 137–145. [Google Scholar] [CrossRef]
- Vites, J.C.; Lynam, M.M. Rhenium 1996. Coord. Chem. Rev. 1998, 172, 357–388. [Google Scholar] [CrossRef]
- Bao, A.; Goins, B.; Klipper, R.; Negrete, G.; Phillips, W.T. 186Re-Liposome Labeling Using 186Re-SNS/S Complexes: In Vitro Stability, Imaging, and Biodistribution in Rats. J. Nucl. Med. 2003, 44, 1992–1999. [Google Scholar]
- Lepareur, N.; Ardisson, V.; Noiret, N.; Garin, E. Re-SSS/Lipiodol: Development of a Potential Treatment for HCC from Bench to Bedside. Int. J. Mol. Imaging 2012, 2012, 9. [Google Scholar] [CrossRef]
- Biersack, H.-J.; Stelzner, F.; Knapp, F.F. Discovery of rhenium and masurium (technetium) by Ida Noddack-Tacke and Walter Noddack. Nuklearmedizin/Nucl. Med. 2015, 54, N50–N54. [Google Scholar] [CrossRef]
- Lepareur, N.; Lacœuille, F.; Bouvry, C.; Hindré, F.; Garcion, E.; Chérel, M.; Noiret, N.; Garin, E.; Knapp, F.F.R.J. Rhenium-188 Labeled Radiopharmaceuticals: Current Clinical Applications in Oncology and Promising Perspectives. Front. Med. 2019, 6, 132. [Google Scholar] [CrossRef] [PubMed]
- Bauer, E.B.; Haase, A.A.; Reich, R.M.; Crans, D.C.; Kühn, F.E. Organometallic and coordination rhenium compounds and their potential in cancer therapy. Coord. Chem. Rev. 2019, 393, 79–117. [Google Scholar] [CrossRef]
- Hajes, R.L.; Rafter, J.J. Rhenium-188 as a Possible Diagnostic Agent. J. Nucl. Med. 1966, 7, 797. [Google Scholar]
- Bardfeld, P.A.; Shulman, K. Transport and distribution of rhenium-188 in the central nervous system. Exp. Neurol. 1976, 50, 13. [Google Scholar] [CrossRef]
- Spencer, R.P. Therapy in Nuclear Medicine; Grune & Stratton Publisher: New York, NY, USA, 1977. [Google Scholar]
- Uccelli, L.; Martini, P.; Cittanti, C.; Carnevale, A.; Missiroli, L.; Giganti, M.; Bartolomei, M.; Boschi, A. Therapeutic Radiometals: Worldwide Scientific Literature Trend Analysis (2008–2018). Molecules 2019, 24, 640. [Google Scholar] [CrossRef]
- Search of: Rhenium—List Results—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/results?cond=&term=Rhenium&cntry=&state=&city=&dist=. (accessed on 21 July 2022).
- Home—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ (accessed on 7 August 2022).
- Phillips, W.T.; Goins, B.; Bao, A.; Vargas, D.; Guttierez, J.E.; Trevino, A.; Miller, J.R.; Henry, J.; Zuniga, R.; Vecil, G.; et al. Rhenium-186 liposomes as convection-enhanced nanoparticle brachytherapy for treatment of glioblastoma. Neuro-Oncology 2012, 14, 416–425. [Google Scholar] [CrossRef]
- Chang, C.-H.; Chang, M.-C.; Chang, Y.-J.; Chen, L.-C.; Lee, T.-W.; Ting, G. Translating Research for the Radiotheranostics of Nanotargeted 188Re-Liposome. Int. J. Mol. Sci. 2021, 22, 3868. [Google Scholar] [CrossRef]
- Brenner, A.; Floyd, J.; Bao, A.; Phillips, W.; Awasthi, V.; Patel, T.; Weinberg, J. RADT-24. High Absorbed Doses of Rhenium-186 Nanoliposomes (Rnl) in Recurrent Gbm: A Phase 1 Study. Neuro-Oncology 2020, 22, ii186. [Google Scholar] [CrossRef]
- Woodall, R.T.; Hormuth, D.A., II; Wu, C.; Abdelmalik, M.R.; Phillips, W.T.; Bao, A.; Hughes, T.J.; Brenner, A.J.; Yankeelov, T.E. Patient specific, imaging-informed modeling of rhenium-186 nanoliposome delivery via convection-enhanced delivery in glioblastoma multiforme. Biomed. Phys. Eng. Express 2021, 7, 045012. [Google Scholar] [CrossRef]
- Cipriani, C.; Desantis, M.; Dahlhoff, G.; Brown, S.D.; Wendler, T.; Olmeda, M.; Pietsch, G.; Eberlein, B. Personalized irradiation therapy for NMSC by rhenium-188 skin cancer therapy: A long-term retrospective study. J. Dermatol. Treat. 2020, 33, 969–975. [Google Scholar] [CrossRef]
- Castellucci, P.; Savoia, F.; Farina, A.; Lima, G.M.; Patrizi, A.; Baraldi, C.; Zagni, F.; Vichi, S.; Pettinato, C.; Morganti, A.G.; et al. High dose brachytherapy with non sealed 188Re (rhenium) resin in patients with non-melanoma skin cancers (NMSCs): Single center preliminary results. Eur. J. Nucl. Med. Mol. Imaging 2020, 48, 1511–1521. [Google Scholar] [CrossRef] [PubMed]
- Liepe, K.; Shinto, A. From palliative therapy to prolongation of survival: 223RaCl2 in the treatment of bone metastases. Ther. Adv. Med. Oncol. 2016, 8, 294–304. [Google Scholar] [CrossRef] [PubMed]
- Bouman-Wammes, E.W.; de Klerk, J.M.H.; Bloemendal, H.J.; Van Dodewaard-de Jong, J.M.; Lange, R.; ter Heine, R.; Verheul, H.M.W.; Van den Eertwegh, A.J.M. Bone-Targeting Radiopharmaceuticals as Monotherapy or Combined With Chemotherapy in Patients With Castration-Resistant Prostate Cancer Metastatic to Bone. Clin. Genitourin. Cancer 2019, 17, e281–e292. [Google Scholar] [CrossRef]
- Biersack, H.J.; Palmedo, H.; Andris, A.; Rogenhofer, S.; Knapp, F.F.; Guhlke, S.; Ezziddin, S.; Bucerius, J.; Von Mallek, D. Palliation and Survival After Repeated 188Re-HEDP Therapy of Hormone-Refractory Bone Metastases of Prostate Cancer: A Retrospective Analysis. J. Nucl. Med. 2011, 52, 1721–1726. [Google Scholar] [CrossRef] [PubMed]
- Cyr, J.E.; Pearson, D.A.; Wilson, D.M.; Nelson, C.A.; Guaraldi, M.; Azure, M.T.; Lister-James, J.; Dinkelborg, L.M.; Dean, R.T. Somatostatin Receptor-Binding Peptides Suitable for Tumor Radiotherapy with Re-188 or Re-186. Chemistry and Initial Biological Studies. J. Med. Chem. 2007, 50, 1354–1364. [Google Scholar] [CrossRef] [PubMed]
- Pearson, D.A.; Lister-James, J.; McBride, W.J.; Wilson, D.M.; Martel, L.J.; Civitello, E.R.; Taylor, J.E.; Moyer, B.R.; Dean, R.T. Somatostatin Receptor-Binding Peptides Labeled with Technetium-99m: Chemistry and Initial Biological Studies. J. Med. Chem. 1996, 39, 1361–1371. [Google Scholar] [CrossRef] [PubMed]
- Edelman, M.J.; Clamon, G.; Kahn, D.; Magram, M.; Lister-James, J.; Line, B.R. Targeted Radiopharmaceutical Therapy for Advanced Lung Cancer: Phase I Trial of Rhenium Re188 P2045, a Somatostatin Analog. J. Thorac. Oncol. 2009, 4, 1550–1554. [Google Scholar] [CrossRef]
- Phase I/II Trial of Rhenium 188-P2045 in Small Cell Lung Cancer and Other Advanced Neuroendocrine Carcinomas—Full Text View—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT02030184 (accessed on 21 July 2022).
- Rhenium Re 188 P2045 in Patients With Lung Cancer Who Have Received or Refused to Receive Prior Chemotherapy—Full Text View—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT00100256 (accessed on 21 July 2022).
- Lepareur, N.; Garin, E. Transarterial Radionuclide Therapy with 188 Re-Labelled Lipiodol. Int. J. Nucl. Med. Res. Spec. Issue 2017, 56, 79–91. [Google Scholar]
- Paeng, J.C.; Jeong, J.M.; Yoon, C.J.; Lee, Y.-S.; Suh, Y.-G.; Chung, J.W.; Park, J.H.; Chung, J.-K.; Son, M.; Lee, M.C. Lipiodol Solution of 188 Re-HDD as a New Therapeutic Agent for Transhepatic Arterial Embolization in Liver Cancer: Preclinical Study in a Rabbit Liver Cancer Model. J. Nucl. Med. 2003, 44, 2033–2038. [Google Scholar]
- Boschi, A.; Uccelli, L.; Duatti, A.; Colamussi, P.; Cittanti, C.; Filice, A.; Rose, A.H.; Martindale, A.A.; Claringbold, P.G.; Kearney, D.; et al. A kit formulation for the preparation of re-lipiodol: Preclinical studies and preliminary therapeutic evaluation in patients with unresectable hepatocellular carcinoma. Nucl. Med. Commun. 2004, 25, 691–699. [Google Scholar] [CrossRef]
- Keng, G.H.; Sundram, F.X.; Yu, S.W.; Somanesan, S.; Premaraj, J.; Oon, C.J.; Kwok, R.; Htoo, M.M. Preliminary Experience in Radionuclide Therapy of Hepatocellular Carcinoma Using Hepatic Intra-arterial Radio-conjugates. Ann. Acad. Med. Singap. 2002, 31, 382–386. [Google Scholar] [PubMed]
- Sundram, F.; Chau, T.C.M.; Onkhuudai, P.; Bernal, P.; Padhy, A.K. Preliminary results of transarterial rhenium-188 HDD lipiodol in the treatment of inoperable primary hepatocellular carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2004, 31, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Srivastava, D.N.; Chau, T.T.M.; Huynh, D.L.; Bal, C.S.; Chandra, P.; Le, T.C.; Nguyen, V.H.; Thulkar, S.; Sharma, S.; et al. Inoperable hepatocellular carcinoma: Transarterial 188Re HDD-labeled iodized oil for treatment–Prospective multicenter clinical trial. Radiology 2007, 243, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Bernal, P.; Raoul, J.L.; Vidmar, G.; Sereegotov, E.; Sundram, F.X.; Kumar, A.; Jeong, J.M.; Pusuwan, P.; Divgi, C.; Zanzonico, P.; et al. Intra-Arterial Rhenium-188 Lipiodol in the Treatment of Inoperable Hepatocellular Carcinoma: Results of an IAEA-Sponsored Multination Study. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 1448–1455. [Google Scholar] [CrossRef] [PubMed]
- Bernal, P.; Raoul, J.L.; Stare, J.; Sereegotov, E.; Sundram, F.X.; Kumar, A.; Jeong, J.M.; Pusuwan, P.; Divgi, C.; Zanzonico, P.; et al. International Atomic Energy Agency-Sponsored Multination Study of Intra-Arterial Rhenium-188-Labeled Lipiodol in the Treatment of Inoperable Hepatocellular Carcinoma: Results With Special Emphasis on Prognostic Value of Dosimetric Study. Semin. Nucl. Med. 2008, 38, S40–S45. [Google Scholar] [CrossRef]
- De Ruyck, K.; Lambert, B.; Bacher, K.; Gemmel, F.; De Vos, F.; Vral, A.; De Ridder, L.; Dierckx, R.A.; Thierens, H. Biologic Dosimetry of 188 Re-HDD/Lipiodol Versus 131 I-Lipiodol Therapy in Patients with Hepatocellular Carcinoma. J. Nucl. Med. 2004, 45, 612–618. [Google Scholar]
- Lambert, B.; Bacher, K.; Defreyne, L.; Gemmel, F.; Van Vlierberghe, H.; Jeong, J.M.; Dierckx, R.A.; Van de Wiele, C.; Thierens, H.; De Vos, F. 188 Re-HDD/Lipiodol Therapy for Hepatocellular Carcinoma: A Phase I Clinical Trial. J. Nucl. Med. 2005, 46, 60–66. [Google Scholar]
- Lambert, B.; Bacher, K.; De Keukeleire, K.; Smeets, P.; Colle, I.; Jeong, M.J.; Hubert, T.; Troisi, R.; De Vos, F.; Van de Wiele, C. 188 Re-HDD/Lipiodol for Treatment of Hepatocellular Carcinoma: A Feasibility Study in Patients with Advanced Cirrhosis. J. Nucl. Med. 2005, 46, 1326–1332. [Google Scholar]
- Lambert, B.; Praet, M.; Vanlangenhove, P.; Troisi, R.; De Hemptinne, B.; Gemmel, F.; Van Vlierberghe, H.; Van De Wiele, C. Radiolabeled Lipiodol Therapy for Hepatocellular Carcinoma in Patients Awaiting Liver Transplantation: Pathology of the Explant Livers and Clinical Outcome. Cancer Biother. Radiopharm. 2005, 20, 209–214. [Google Scholar] [CrossRef]
- Kumar, A.; Bal, C.; Srivastava, D.N.; Acharya, S.K.; Thulkar, S.P.; Sharma, S.; Duttagupta, S. Transarterial radionuclide therapy with Re-188-HDD-lipiodol in case of unresectable hepatocellular carcinoma with extensive portal vein thrombosis. Eur. J. Radiol. Extra 2005, 56, 55–59. [Google Scholar] [CrossRef]
- Kumar, A.; Srivastava, D.N.; Bal, C. Management of postsurgical recurrence of hepatocellular carcinoma with rhenium 188-HDD labeled iodized oil. J. Vasc. Interv. Radiol. 2006, 17, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Bal, C.; Srivastava, D.N.; Thulkar, S.P.; Sharma, S.; Acharya, S.K.; Duttagupta, S. Management of multiple intrahepatic recurrences after radiofrequency ablation of hepatocellular carcinoma with rhenium-188-HDD-lipiodol. Eur. J. Gastroenterol. Hepatol. 2006, 18, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Lambert, B.; Bacher, K.; Defreyne, L.; Van Vlierberghe, H.; Jae, M.J.; Rong, F.W.; Van Meerbeeck, J.; Smeets, P.; Troisi, R.; Thierens, H.; et al. 188Re-HDD/lipiodol therapy for hepatocellular carcinoma: An activity escalation study. Eur. J. Nucl. Med. Mol. Imaging 2006, 33, 344–352. [Google Scholar] [CrossRef]
- Padhy, A.K.; Dondi, M. A Report on the Implementation Aspects of the International Atomic Energy Agency’s First Doctoral Coordinated Research Project, ‘Management of Liver Cancer Using Radionuclide Methods With Special Emphasis on Trans-Arterial Radio-Conjugate Therapy and Internal Dosimetry’. Semin. Nucl. Med. 2008, 38, S5–S12. [Google Scholar] [CrossRef] [PubMed]
- Khajornjiraphan, N.; Thu, N.A.; Chow, P.K.H. Yttrium-90 Microspheres: A review of its emerging clinical indications. Liver Cancer 2015, 4, 6–15. [Google Scholar] [CrossRef]
- Bozkurt, M.F.; Salanci, B.V.; Uǧur, Ö. Intra-arterial radionuclide therapies for liver tumors. Semin. Nucl. Med. 2016, 46, 324–339. [Google Scholar] [CrossRef]
- Bouvry, C.; Palard, X.; Edeline, J.; Ardisson, V.; Loyer, P.; Garin, E.; Lepareur, N. Transarterial radioembolization (TARE) agents beyond 90 Y-microspheres. BioMed Res. Int. 2018, 2018, 1435302. [Google Scholar] [CrossRef] [PubMed]
- Esquinas, P.L.; Shinto, A.; Kamaleshwaran, K.K.; Joseph, J.; Celler, A. Biodistribution, pharmacokinetics, and organ-level dosimetry for 188 Re-AHDD-Lipiodol radioembolization based on quantitative post-treatment SPECT/CT scans. EJNMMI Phys. 2018, 5, 30. [Google Scholar] [CrossRef]
- Banka, V.K.; Moon, S.H.; Jeong, J.M.; Seelam, S.R.; Lee, Y.S.; Kim, Y.J.; Lee, D.S.; Chung, J.K. Development of 4-hexadecyl-4,7-diaza-1,10-decanedithiol (HDD) kit for the preparation of the liver cancer therapeutic agent Re-188-HDD/lipiodol. Nucl. Med. Biol. 2015, 42, 317–322. [Google Scholar] [CrossRef]
- Delaunay, K.; Edeline, J.; Rolland, Y.; Lepareur, N.; Laffont, S.; Palard, X.; Bouvry, C.; Le Sourd, S.; Pracht, M.; Ardisson, V.; et al. Preliminary results of the Phase 1 Lip-Re I clinical trial: Biodistribution and dosimetry assessments in hepatocellular carcinoma patients treated with 188Re-SSS Lipiodol radioembolization. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1506–1517. [Google Scholar] [CrossRef]
- 188RE-SSS Lipiodol to Treat HepatoCellular Carcinomas—Full Text View—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT01126463?term=rhenium (accessed on 21 July 2022).
- Lepareur, N.; Ardisson, V.; Noiret, N.; Boucher, E.; Raoul, J.L.; Clément, B.; Garin, E. Automation of labelling of Lipiodol with high-activity generator-produced 188Re. Appl. Radiat. Isot. 2011, 69, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Uccelli, L.; Pasquali, M.; Boschi, A.; Giganti, M.; Duatti, A. Automated preparation of Re-188 lipiodol for the treatment of hepatocellular carcinoma. Nucl. Med. Biol. 2011, 38, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Harbeck, N.; Gnant, M. Breast cancer. Lancet 2017, 389, 1134–1150. [Google Scholar] [CrossRef]
- Xing, Y.; Chand, G.; Liu, C.; Cook, G.J.R.; O’Doherty, J.; Zhao, L.; Wong, N.C.L.; Meszaros, L.K.; Ting, H.H.; Zhao, J. Early Phase I Study of a 99mTc-Labeled Anti–Programmed Death Ligand-1 (PD-L1) Single-Domain Antibody in SPECT/CT Assessment of PD-L1 Expression in Non–Small Cell Lung Cancer. J. Nucl. Med. 2019, 60, 1213–1220. [Google Scholar] [CrossRef]
- Salvador, J.-P.; Vilaplana, L.; Marco, M.-P. Nanobody: Outstanding features for diagnostic and therapeutic applications. Anal. Bioanal. Chem. 2019, 411, 1703–1713. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, R.; Goel, S.; Cai, W. Nanobody: The “Magic Bullet” for Molecular Imaging? Theranostics 2014, 4, 386. [Google Scholar] [CrossRef]
- Vaneycken, I.; Devoogdt, N.; Van Gassen, N.; Vincke, C.; Xavier, C.; Wernery, U.; Muyldermans, S.; Lahoutte, T.; Caveliers, V. Preclinical screening of anti-HER2 nanobodies for molecular imaging of breast cancer. FASEB J. 2011, 25, 2433–2446. [Google Scholar] [CrossRef]
- Zhou, Z.; Vaidyanathan, G.; McDougald, D.; Kang, C.M.; Balyasnikova, I.; Devoogdt, N.; Ta, A.N.; McNaughton, B.R.; Zalutsky, M.R. Fluorine-18 Labeling of the HER2-Targeting Single-Domain Antibody 2Rs15d Using a Residualizing Label and Preclinical Evaluation. Mol. Imaging Biol. 2017, 19, 867–877. [Google Scholar] [CrossRef]
- Dekempeneer, Y.; Bäck, T.; Aneheim, E.; Jensen, H.; Puttemans, J.; Xavier, C.; Keyaerts, M.; Palm, S.; Albertsson, P.; Lahoutte, T.; et al. Labeling of Anti-HER2 Nanobodies with Astatine-211: Optimization and the Effect of Different Coupling Reagents on Their in Vivo Behavior. Mol. Pharm. 2019, 16, 3524–3533. [Google Scholar] [CrossRef]
- Pruszynski, M.; D’Huyvetter, M.; Bruchertseifer, F.; Morgenstern, A.; Lahoutte, T. Evaluation of an Anti-HER2 Nanobody Labeled with 225Ac for Targeted α-Particle Therapy of Cancer. Mol. Pharm. 2018, 15, 1457–1466. [Google Scholar] [CrossRef]
- Bridoux, J.; Broos, K.; Lecocq, Q.; Debie, P.; Martin, C.; Ballet, S.; Raes, G.; Neyt, S.; Vanhove, C.; Breckpot, K.; et al. Anti-Human PD-L1 Nanobody for Immuno-PET Imaging: Validation of a Conjugation Strategy for Clinical Translation. Biomolecules 2020, 10, 1388. [Google Scholar] [CrossRef]
- Xavier, C.; Vaneycken, I.; D’huyvetter, M.; Heemskerk, J.; Keyaerts, M.; Vincke, C.; Devoogdt, N.; Muyldermans, S.; Lahoutte, T.; Caveliers, V. Synthesis, Preclinical Validation, Dosimetry, and Toxicity of 68Ga-NOTA-Anti-HER2 Nanobodies for iPET Imaging of HER2 Receptor Expression in Cancer. J. Nucl. Med. 2013, 54, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Keyaerts, M.; Xavier, C.; Heemskerk, J.; Devoogdt, N.; Everaert, H.; Ackaert, C.; Vanhoeij, M.; Duhoux, F.P.; Gevaert, T.; Simon, P.; et al. Phase I Study of 68Ga-HER2-Nanobody for PET/CT Assessment of HER2 Expression in Breast Carcinoma. J. Nucl. Med. 2016, 57, 27–33. [Google Scholar] [CrossRef]
- Xavier, C.; Blykers, A.; Laoui, D.; Bolli, E.; Vaneyken, I.; Bridoux, J.; Baudhuin, H.; Raes, G.; Everaert, H.; Movahedi, K.; et al. Clinical Translation of [68Ga]Ga-NOTA-anti-MMR-sdAb for PET/CT Imaging of Protumorigenic Macrophages. Mol. Imaging Biol. 2019, 21, 898–906. [Google Scholar] [CrossRef]
- Zhao, L.; Liu, C.; Xing, Y.; He, J.; O’Doherty, J.; Huang, W.; Zhao, J. Development of a 99mTc-Labeled Single-Domain Antibody for SPECT/CT Assessment of HER2 Expression in Breast Cancer. Mol. Pharm. 2021, 18, 3616–3622. [Google Scholar] [CrossRef]
- Belhadj-Tahar, H.; Chen, A.; Jia, Y.; Wu, S.; Sadeg, N.; Zhao, H.; Li, C.; Gu, G.; Gao, Y.; Yang, G. In situ anti-cancer agent derived from [188re]rhenium nitro-imidazole ligand loaded poly-l-lysine dendrimer administrated by direct CT guided stereotactic intrahepatic injection. J. Clin. Oncol. 2018, 36, e15569. [Google Scholar] [CrossRef]
- Belhadj-Tahar, H.; Chen, J.; Song, P.; Zhao, J.; Quan, M.; Li, C.; Gu, X.; Yang, G.; Gao, Y. Novel CT-guided 188-rhenium brachytherapy device for local primary and secondary lung malignancies. J. Glob. Oncol. 2019, 5, 96. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Eβ- [keV] (Int %) | EAuger e- [keV] (Int %) | Eγ [keV] (Int %) | EX-rays [keV] (Int %) | |
|---|---|---|---|---|
| 186Re→186W | 6.53 (4.96%) | 122.64 (0.603%) | 8.4 (1.96%) | |
| 45.7 (0.29%) | 57.981 (1.72%) | |||
| 59.318 (2.95%) | ||||
| Mean energy: | 1.3 (57%) | 122.64 (0.603%) | 46 (8.3%) | |
| 186Re→186Os | 306.1 (21.54%) | 6.88(6.55%) | 137.157 (9.47%) | 8.91(2.92%) |
| 359.2 (70.99%) | 48.3(0.179%) | 61.486 (1.14%) | ||
| 63.0 (1.94%) | ||||
| Mean energy: | 346.7 (92.59%) | 1.3 (71%) | 106 (12.1%) | 38 (7.3%) |
| Eβ- [keV] (Int %) | EAuger e- [keV] (Int %) | Eγ [keV] (Int %) | EX-rays [keV] (Int %) | |
|---|---|---|---|---|
| 188Re→188Os | 527.779 (1.85%) | 6.88 (6.84%) | 155.044 (15.49%) | 8.91 (3.04%) |
| 728.88 (25.8%) | 48.3 (0.219%) | 478.00 (1.076%) | 61.486 (1.40%) | |
| 795.41 (70.7%) | 6.33.03 (1.370%) | 63.0 (2.38%) | ||
| Mean energy: | 763 (100.2%) | 1.3 (75%) | 40.8 (8.4%) |
| Reaction | E°Re [V] | E°Tc [V] | ΔE° [V] |
|---|---|---|---|
| MO4− + 3e− + 4H+ → MO2 + 2H2O | 0.51 | 0.74 | −0.23 |
| MO4− + 7e− + 8H+ → M + 4H2O | 0.36 | 0.47 | −0.11 |
| Actual Start/End Study Date and Status | Brief Title | Brief Summary | Study Phase | Condition | Drug/Device | Study Sponsor |
|---|---|---|---|---|---|---|
| January 2000/February 2001 Completed | Biodistribution Study With 186Re-labelled Humanised Monoclonal Antibody BIWA 4 in Patients With Adenocarcinoma of the Breast. NCT02204046 | To evaluate the safety and tolerability of 186Re-bivatuzumab administered intravenously (i.v.) and to study biodistribution and pharmacokinetics in patients with breast adenocarcinoma. | Phase I | Brest Adenocarcinoma | 186Re-labelled humanized monoclonal antibody BIWA 4 | Boehringer Ingelheim |
| December 1999/February 2001 Completed | Biodistribution Study With 186Re-labelled Humanised Monoclonal Antibody BIWA 4 in Patients With Non-small Cell Lung Cancer NCT02204059 | To evaluate the safety and tolerability of 186Re-bivatuzumab administered intravenously (i.v.) and to study biodistribution and pharmacokinetics in patients with non-small cell lung cancer (NSCLC). | Phase I | Carcinoma, Non-Small-Cell Lung | 186Re-labelled humanized monoclonal antibody BIWA 4 | Boehringer Ingelheim |
| March 1999/June 2001 Completed | Dose Escalation Study With 99mTC—or 186 Re-labelled Humanised Monoclonal Antibody (hMAb) BIWA 4 in Patients With Head and Neck Cancer. NCT02204033 | To evaluate the safety and tolerability of 186Re-bivatuzumab administered intravenously (i.v.) and to study biodistribution and pharmacokinetics in patients with Head and Neck Neoplasms. | Phase I | Head and Neck Neoplasms | 186Re-labelled humanized monoclonal antibody BIWA 4 | Boehringer Ingelheim |
| April 2006/April 2007 Completed | Identification of Sentinel Lymph Nodes With Methylene Blue and Isotope NCT00314405 | To evaluate the performance of a double labeling method using isotope and methylene blue dye injection to localize precisely Sentinel Lymph Node (SLN) in a series of 100 patients with infiltrative breast cancer justifying SLN excision. | NA | Infiltrative Breast Cancer | 186Re-Sulfide (Device) | University Hospital, Strasbourg, France |
| 31 May 2012/31 December 2018 Completed | Multicentre Canadian Study to Measure the Safety and Efficacy of Radiosynoviorthesis NCT01615991 | Multicentre Canadian Study to Measure the Safety and Efficacy of Synoviorthesis Performed With 90Y- or 186Re-Sulfide. | Phase III | Arthritis or chronic inflammatory joint disease. | 186Re-Sulfide | Centre de recherche du Centre hospitalier universitaire de Sherbrooke |
| 3 June 2015/January 2025 Recruiting | Maximum Tolerated Dose, Safety, and Efficacy of Rhenium Nanoliposomes in Recurrent Glioma (ReSPECT). NCT01906385 | Volume and dose escalation study of the safety, tolerability, and distribution of 186RNL in patients with recurrent or progressive malignant glioma after standard surgical, radiation, and/or chemotherapy treatment. | Phase I; Phase II | Glioma. | 186Re-NanoLiposomes (186RNL) | Plus Therapeutics |
| 6 December 2021/30 December 2022 Recruiting | Intraventricular Administration of 186Re-NanoLiposome for Leptomeningeal Metastases NCT05034497 | An open-label Phase I clinical study that will administer a single dose of 186RNL via intraventricular catheter for the treatment of Leptomeningeal Metastases (LM). | Phase I | Leptomeningeal Metastasis | 186Re-NanoLiposomes (186RNL) | Plus Therapeutics |
| 26 May 2010/6 August 2019 Completed | 188Re-SSS Lipiodol to Treat HepatoCellular Carcinomas NCT01126463 | To determine the maximum tolerated dose and the recommended 188Re-SSS Lipiodol activity for hepatic intra-arterial injection in patients with hepato-cellular carcinoma. | Phase I | Hepatocellular Carcinomas | 188Re-SSS Lipiodol | Center Eugene Marquis |
| 17 January 2022/15 May 2024 Recruiting | Rhenium-Skin Cancer Therapy (SCT) for the Treatment of Non-Melanoma Skin Cancer. NCT05135052 | Efficacy of Personalized Irradiation with 188Rhenium-Skin Cancer Therapy (SCT) for the treatment of non-melanoma skin cancer. | Phase IV | Non-melanoma Skin Cancer. | 188Re-resin (Rhenium-SCT®) | OncoBeta International GmbH (OncoBeta Therapeutics) |
| 24 August 2020/30 September 2022 Recruiting | HER2 Expression Detection and Radionuclide Therapy in Breast Cancer Using 99mTc/188Re Labeled Single Domain Antibody NCT04674722 | To evaluate the safety, dosimetry, and efficacy of 99mTc/188Re labeled anti-HER2-single domain antibody (Product Code Name: 99mTc-NM-02 and 188Re-NM-02) SPECT/CT imaging of HER2 expression and radionuclide therapy in Breast Cancer. | Phase I | Breast Cancer Radiotoxicity | 99mTc or 188Re labeled anti-HER2 sdAb. | Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine |
| 16 May 2018/16 May 2024 Active, not recruiting | Rhenium-188-HEDP vs. Radium-223-chloride in Patients With Advanced Prostate Cancer Refractory to Hormonal Therapy. NCT03458559 | To investigate if treatment with 188Re-HEDP results in an improvement in overall survival compared to treatment with 223Ra-chloride. | Phase III | Prostate Cancer Metastatic to Bone. | 188Re-HEDP vs. 223RaChloride | Amsterdam UMC, location VUmc |
| June 2017/June 2019 Withdrawn | Rhenium 188-P2045 in Small Cell Lung Cancer and Other Advanced Neuroendocrine Carcinomas. NCT02030184 | 188Re-P2045 in small lung cancer and other advanced NE carcinomas. | Phase I; Phase II | Small Cell Lung Cancer (SCLC); Neuroendocrine (NE) Tumors; Large Cell Neuroendocrine (NE) Tumors. | 188Re-P2045 | University of Maryland, Baltimore |
| January 2004/April 2020 Unknown status | 188Re-P2045 in Patients With Lung Cancer Who Have Received or Refused to Receive Prior Chemotherapy. NCT00100256 | To determine the maximum dose that is safely tolerated for the experimental drug 188Re-P2045. | Phase I; Phase II | Lung Neoplasms Carcinoma; Non-Small-Cell Lung Carcinoma; Small Cell Neoplasm Recurrence. | 188Re-P2045 | Andarix Pharmaceuticals |
| 13 March 2017/31 October 2017 Unknown status | Treatment of Non-responding to Conventional Therapy Inoperable Liver Cancers by in Situ Introduction of ImDendrim. NCT03255343 | To evaluate the efficacy and safety of treatment of non-responding to conventional therapy inoperable liver cancers by in situ introduction of ImDendrim. | NA | Liver tumor non operable | [188Re]Complex Coupled to an Imidazolic Ligand and Associated With a Dendrime (Device) | French Association for the Advancement Medical Research |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uccelli, L.; Martini, P.; Urso, L.; Ghirardi, T.; Marvelli, L.; Cittanti, C.; Carnevale, A.; Giganti, M.; Bartolomei, M.; Boschi, A. Rhenium Radioisotopes for Medicine, a Focus on Production and Applications. Molecules 2022, 27, 5283. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules27165283
Uccelli L, Martini P, Urso L, Ghirardi T, Marvelli L, Cittanti C, Carnevale A, Giganti M, Bartolomei M, Boschi A. Rhenium Radioisotopes for Medicine, a Focus on Production and Applications. Molecules. 2022; 27(16):5283. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules27165283
Chicago/Turabian StyleUccelli, Licia, Petra Martini, Luca Urso, Teresa Ghirardi, Lorenza Marvelli, Corrado Cittanti, Aldo Carnevale, Melchiore Giganti, Mirco Bartolomei, and Alessandra Boschi. 2022. "Rhenium Radioisotopes for Medicine, a Focus on Production and Applications" Molecules 27, no. 16: 5283. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules27165283