Novel Crown Cement Containing Antibacterial Monomer and Calcium Phosphate Nanoparticles

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Design
- (1)
- RelyX luting cement (3M, St Paul, MN, USA) (referred to as “Commercial control”) (Table 1);
- (2)
- 55% PEHB + 45% glass fillers (referred to as “Experimental control”) (Table 2);
- (3)
- 55% PEHB + 20% glass fillers + 25% NACP + 0% DMAHDM (referred to as “Glass + NACP + 0% DMAHDM”) (Table 2);
- (4)
- 52% PEHB + 20% glass fillers + 25% NACP + 3% DMAHDM (referred to as “Glass + NACP + 3% DMAHDM”) (Table 3);
- (5)
- 51% PEHB + 20% glass fillers + 25% NACP + 4% DMAHDM (referred to as “Glass + NACP + 4% DMAHDM”) (Table 4);
- (6)
- 50% PEHB + 20% glass fillers + 25% NACP + 5% DMAHDM (referred to as “Glass + NACP + 5% DMAHDM”) (Table 5).
- Formula A contains 4.85% BisGMA;
- Formula B contains 5% BisGMA;
- Formula C contains 6% BisGMA.
2.2. Synthesis of DMAHDM Monomer and NACP Fillers
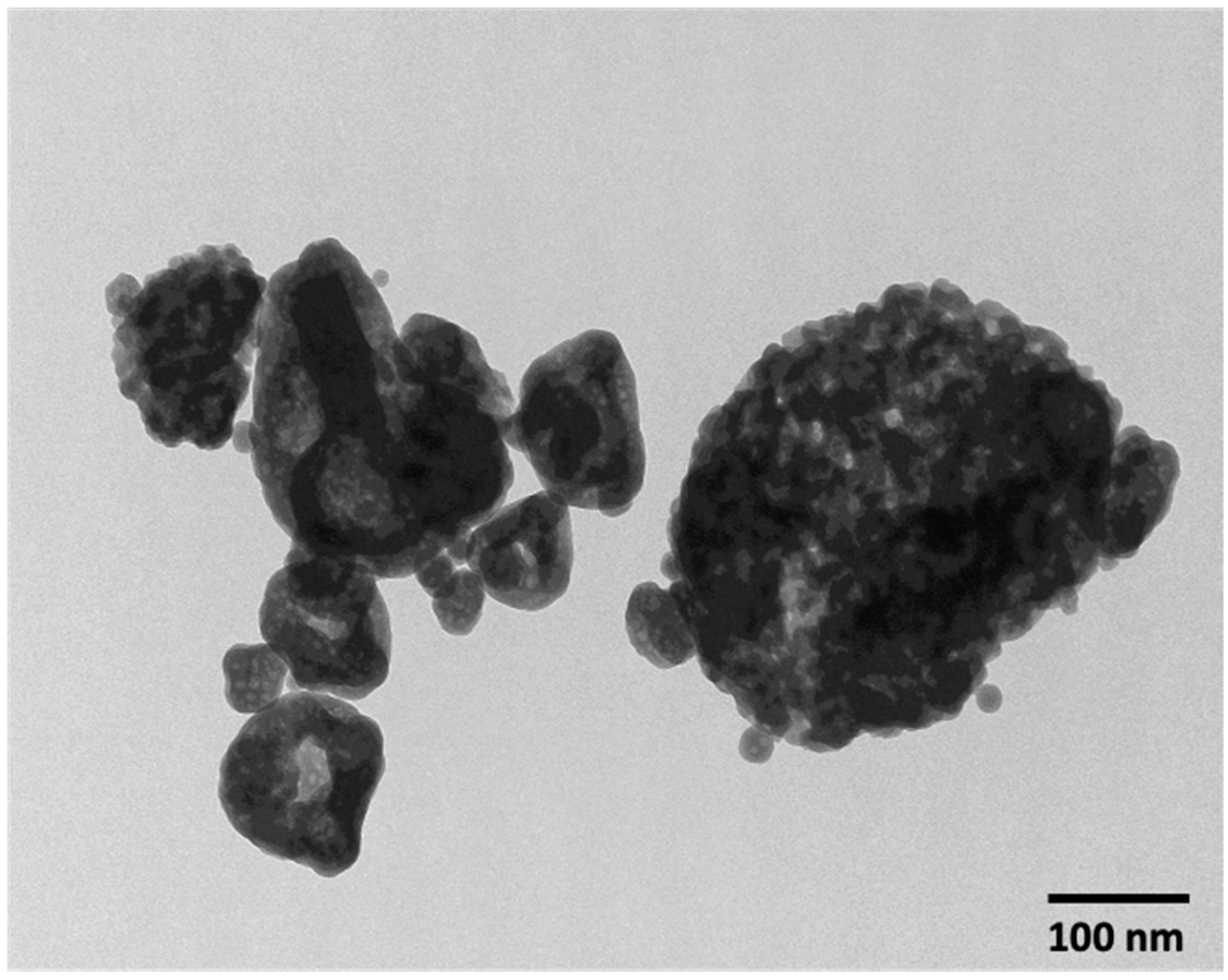
2.3. Characterization of NACP
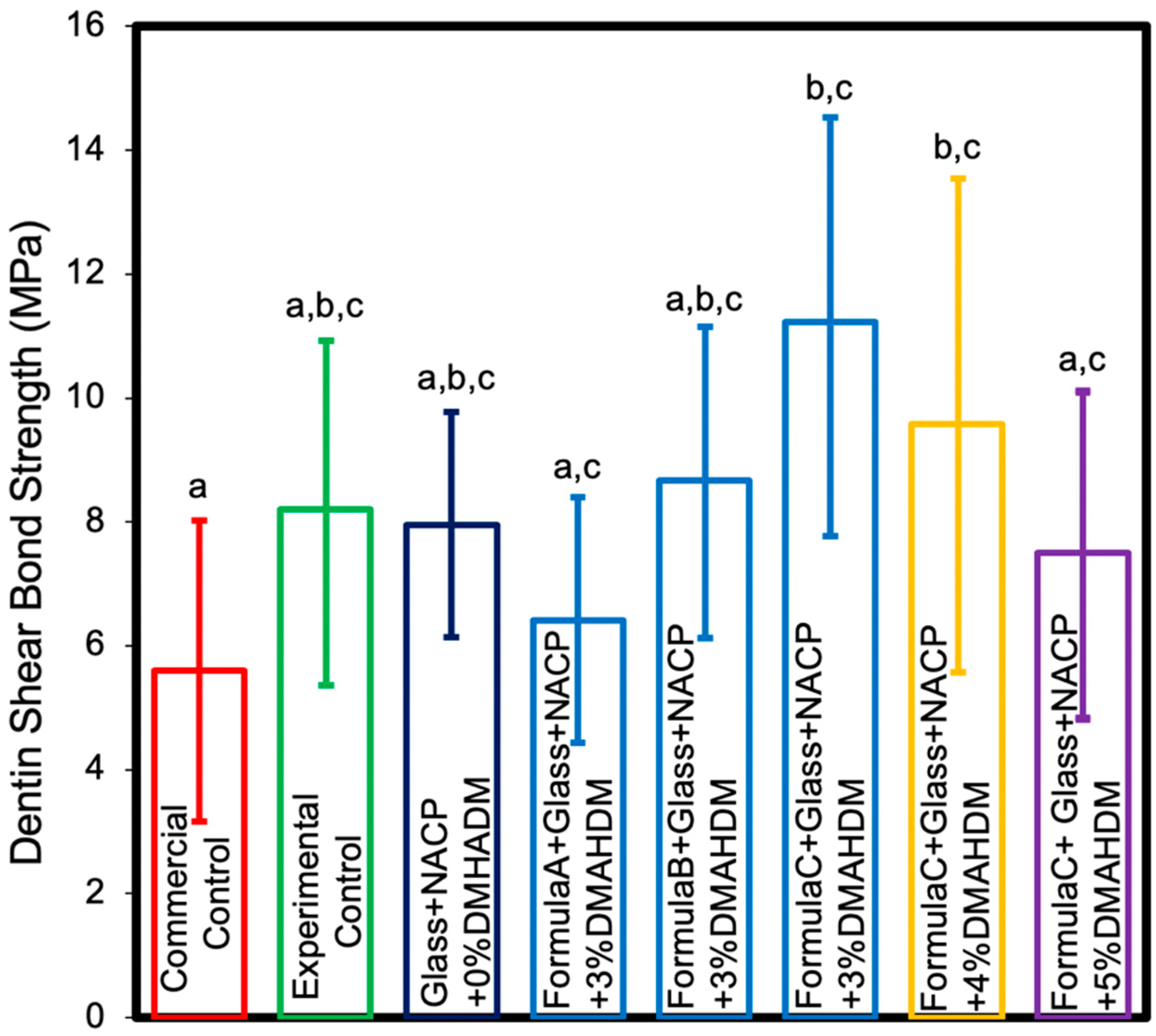
2.4. Dentin Shear Bond. Strength Testing
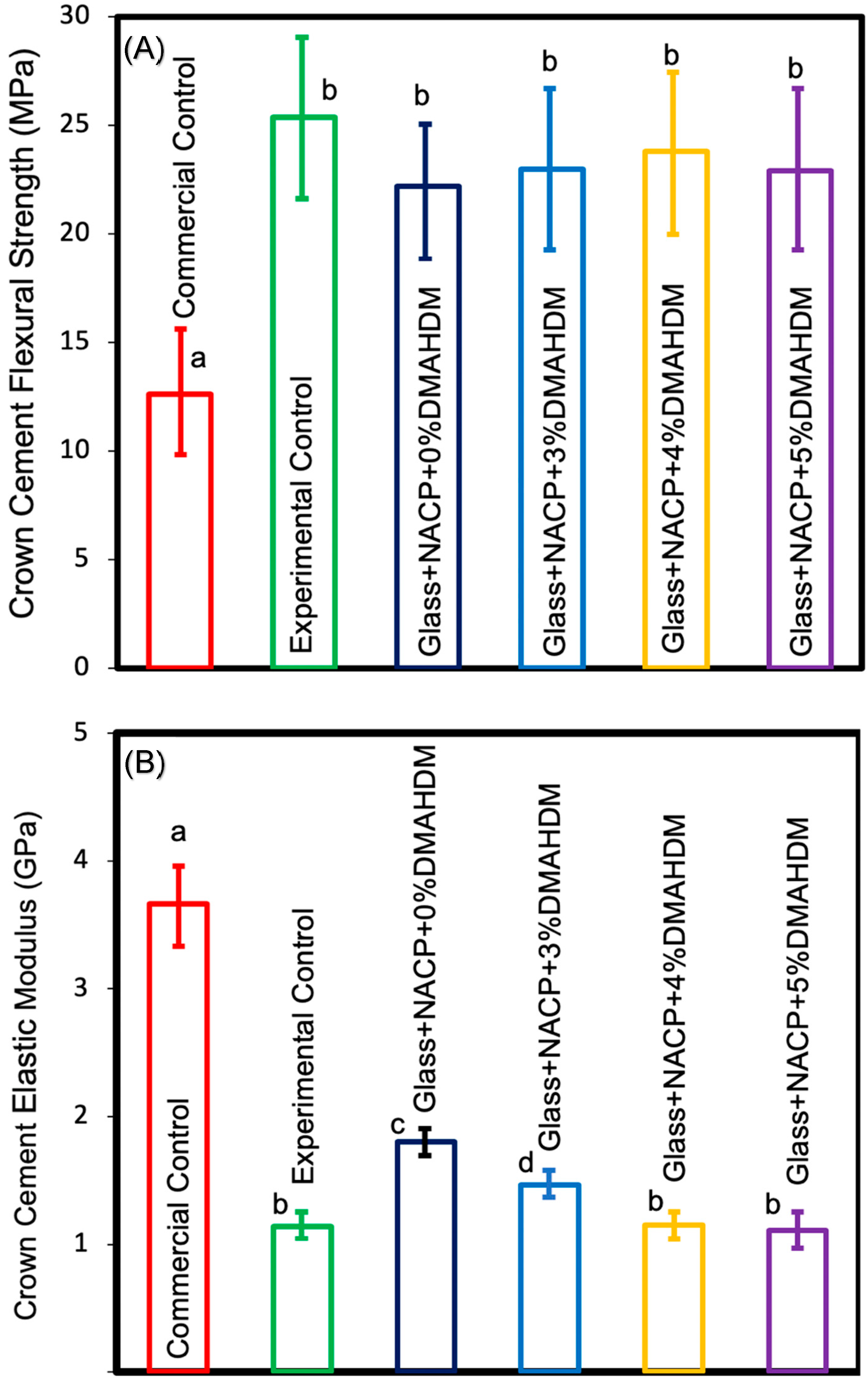
2.5. Flexural Strength and Elastic Modulus
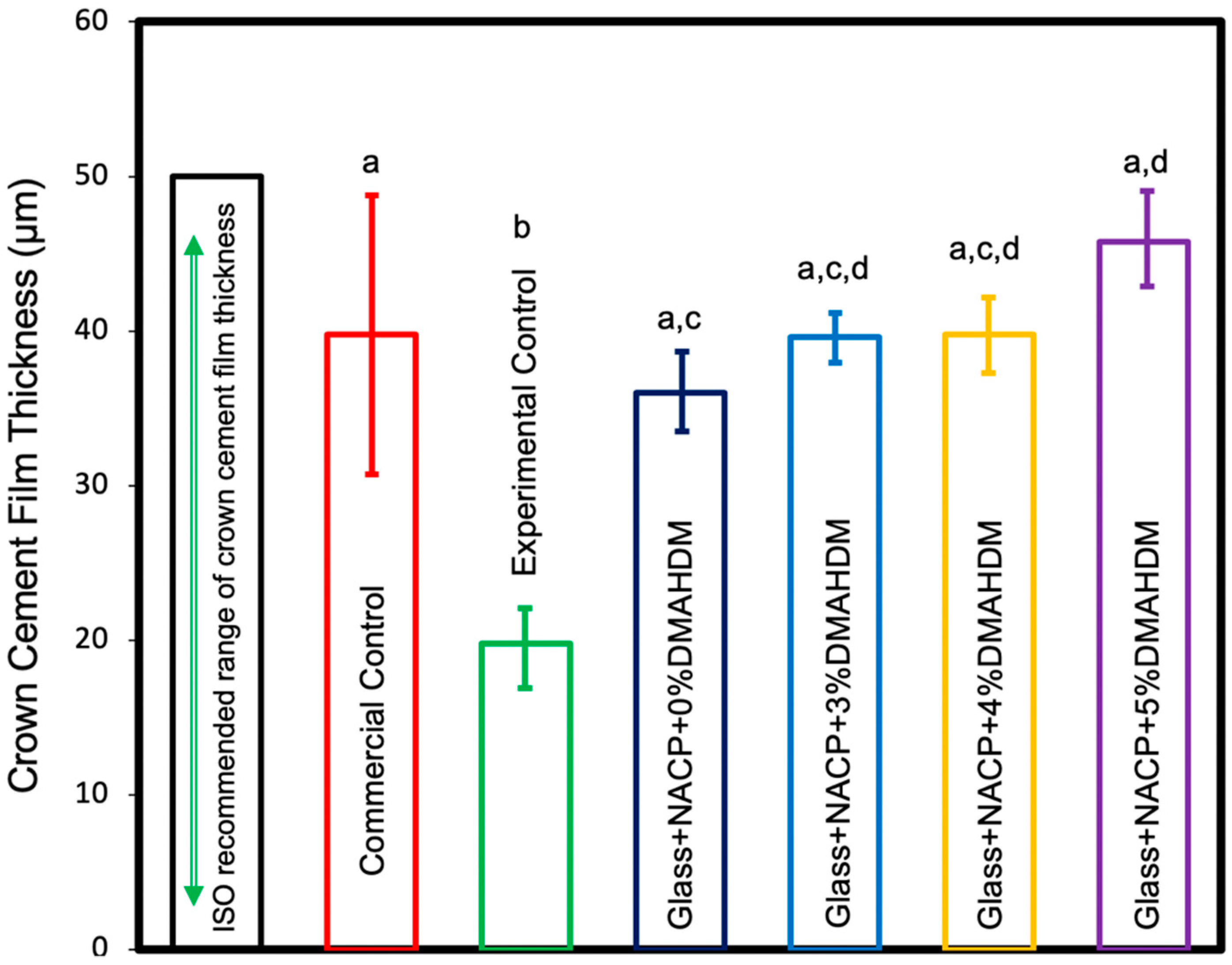
2.6. Film Thickness
2.7. Measurement of Initial Calcium and Phosphate Ions Release
2.8. S. mutans Biofilm Model
2.8.1. Sample Preparation
2.8.2. S. mutans Biofilm Formation
2.8.3. Colony-Forming Unit Counts
2.8.4. Live/Dead Staining of Biofilms
2.8.5. MTT Assay for Quantification of Metabolic Activity of Biofilms
2.9. Statistical Analysis
3. Results
3.1. Characterization of NACP
3.2. Dentin Shear Bond. Strength
3.3. Flexural Strength
3.4. Film Thickness
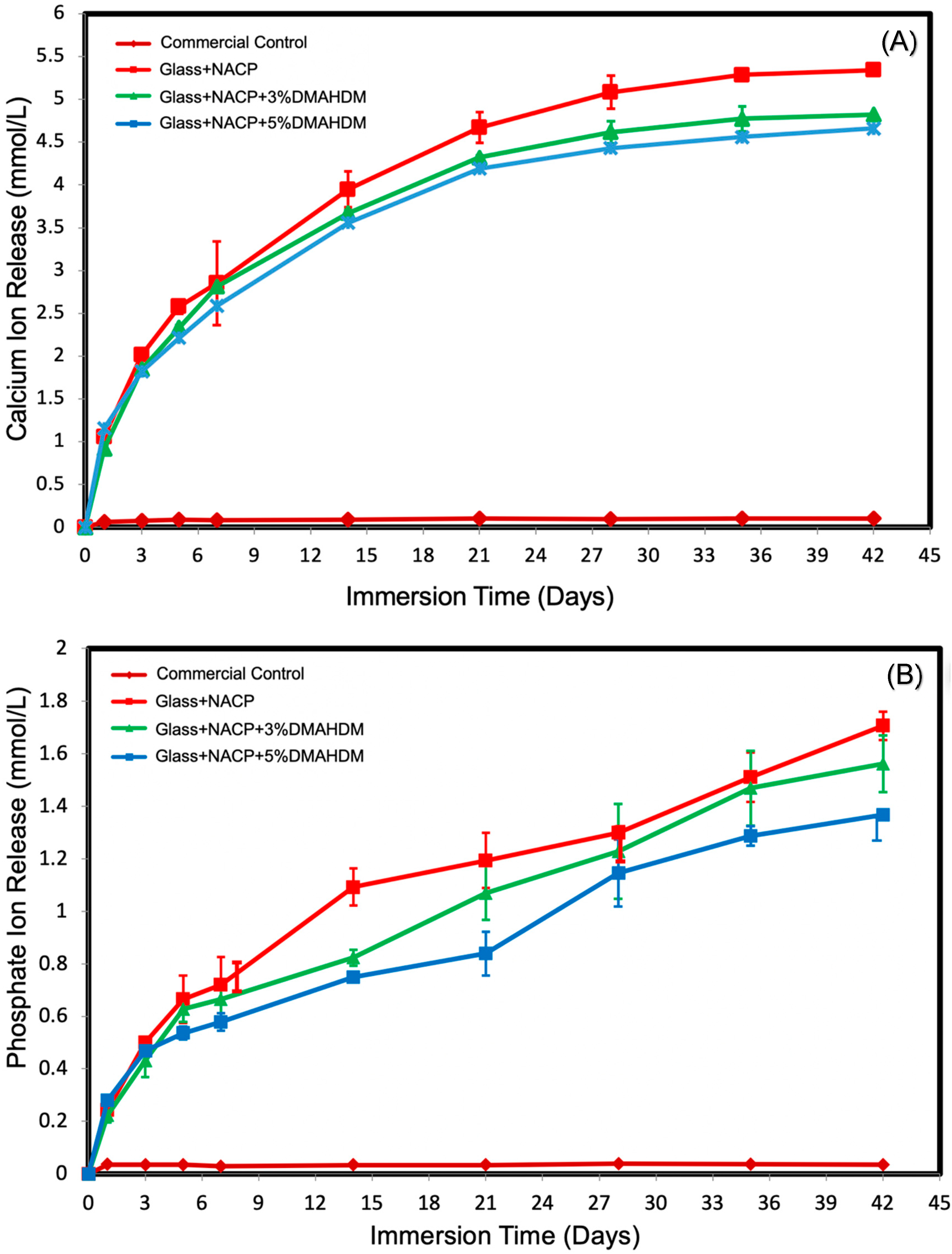
3.5. Initial Calcium and Phosphate Ion. Release
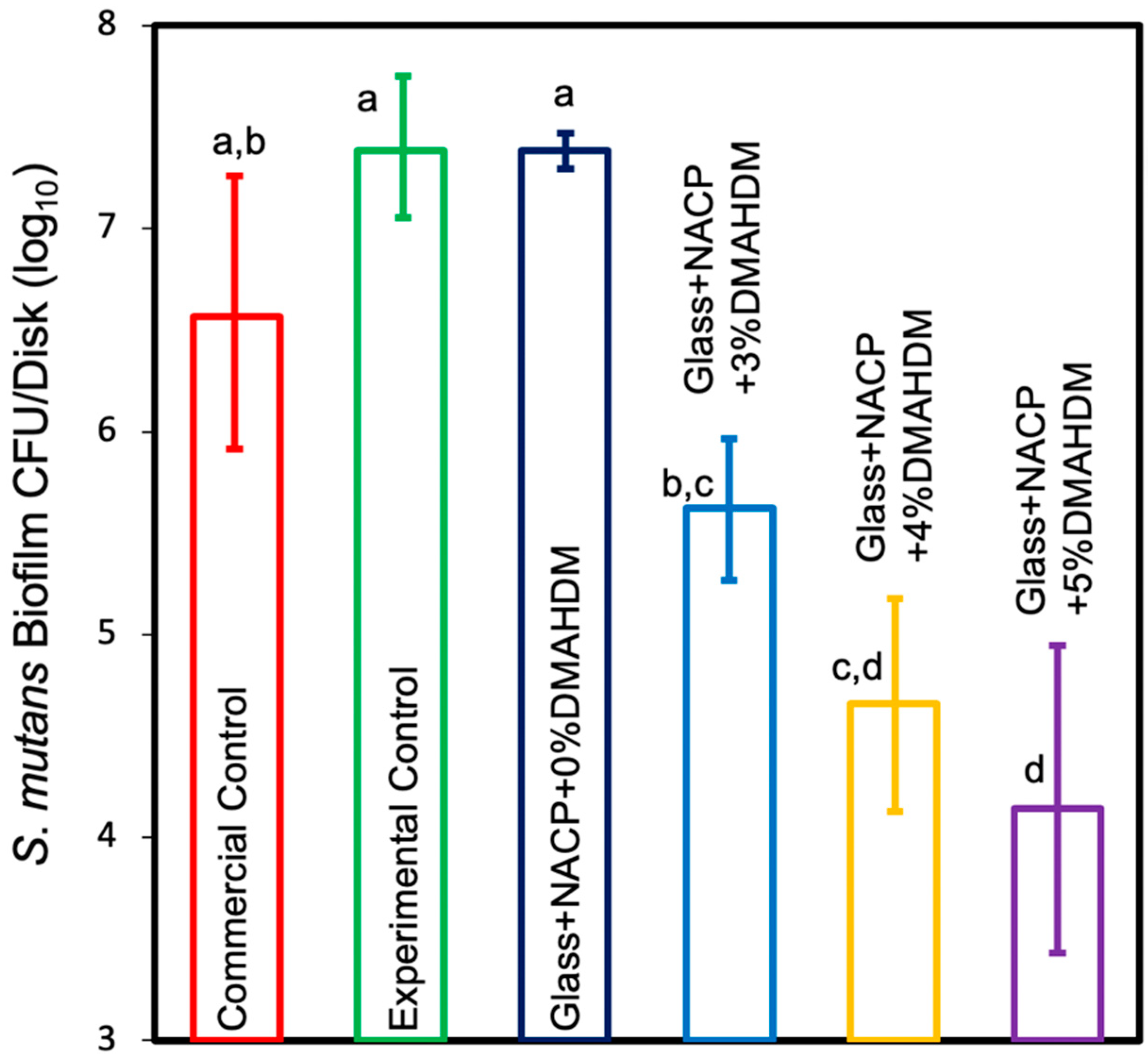
3.5.1. Colony-Forming Unit Counts of S. mutans Biofilm
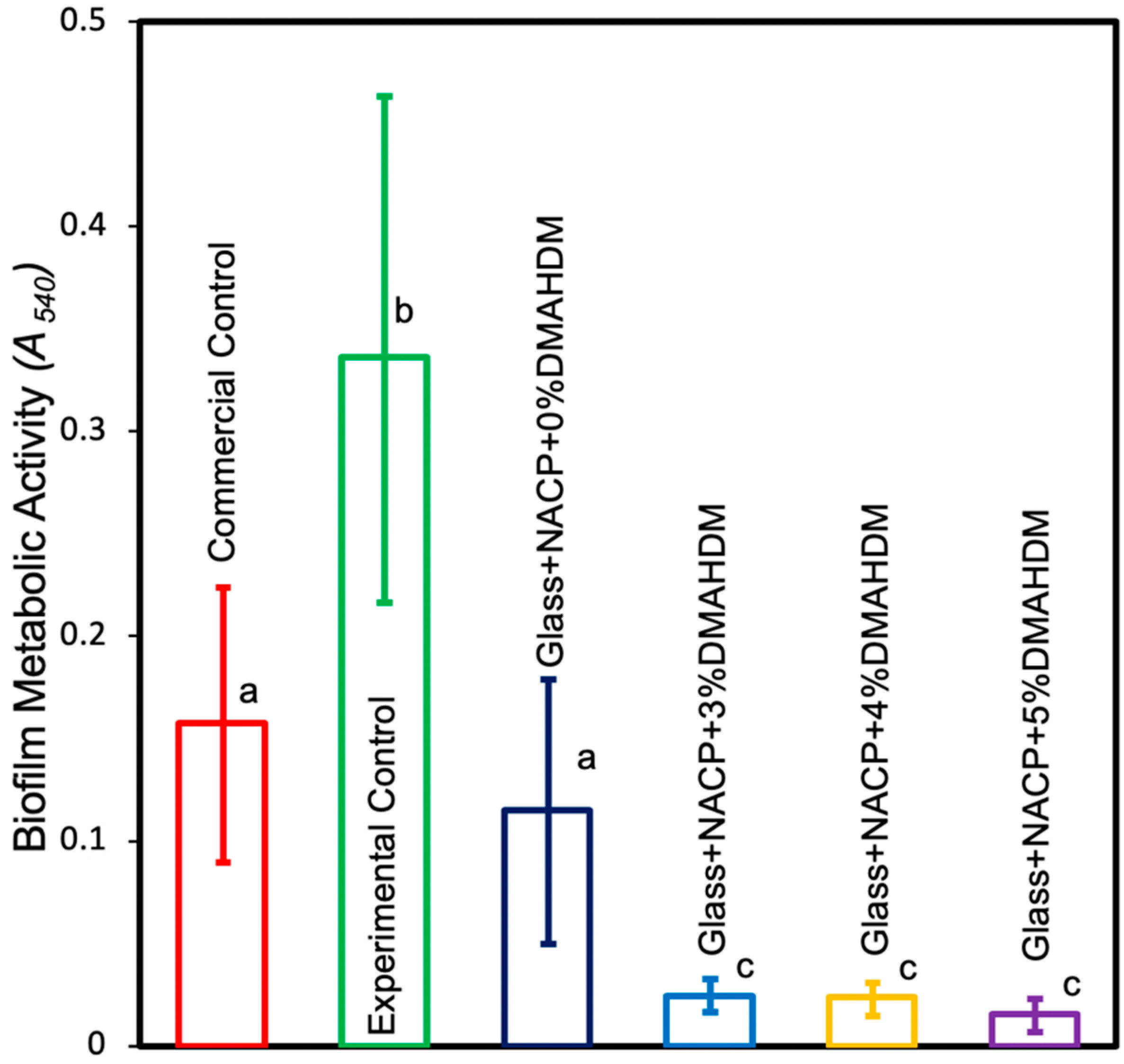
3.5.2. MTT Assay of Metabolic Activity of S. mutans Biofilms
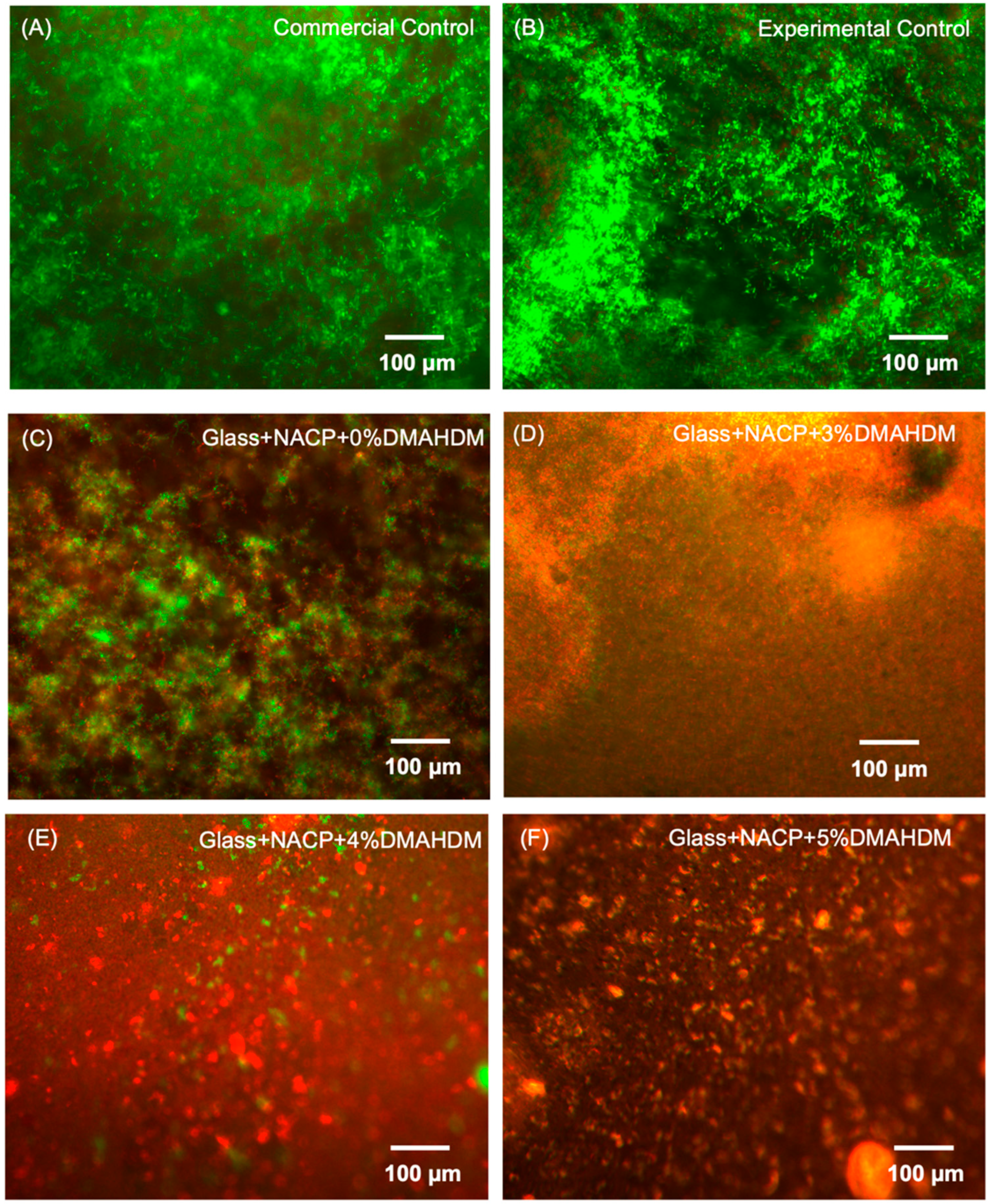
3.5.3. Live/Dead Staining of S. mutans Biofilms
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Behr, M.; Zeman, F.; Baitinger, T.; Galler, J.; Koller, M.; Handel, G.; Rosentritt, M. The clinical performance of porcelain-fused-to-metal precious alloy single crowns: Chipping, recurrent caries, periodontitis, and loss of retention. Int. J. Prosthodont. 2014, 27, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundh, B.; Odman, P. A study of fixed prosthodontics performed at a university clinic 18 years after insertion. Int. J. Prosthodont. 1997, 10, 513–519. [Google Scholar] [PubMed]
- Jokstad, A. Secondary caries and microleakage. Dent. Mater. 2016, 32, 11–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mjor, I.A. Frequency of secondary caries at various anatomical locations. Oper. Dent. 1985, 10, 88–92. [Google Scholar] [PubMed]
- Unosson, E.; Cai, Y.; Jiang, X.; Lööf, J.; Welch, K.; Engqvist, H. Antibacterial properties of dental luting agents: Potential to hinder the development of secondary caries. Int. J. Dent. 2012, 2012, 529495. [Google Scholar] [CrossRef]
- Rosenstiel, S.F.; Land, M.F.; Crispin, B.J. Dental luting agents: A review of the current literature. J. Prosthet. Dent. 1998, 80, 280–301. [Google Scholar] [CrossRef]
- Mjör, I.A.; Jokstad, A.; Qvist, V. Longevity of posterior restorations. Int. Dent. J. 1990, 40, 11–17. [Google Scholar]
- Jokstad, A.; Bayne, S.; Blunck, U.; Tyas, M.; Wilson, N. Quality of dental restorations. FDI Commission Project 2-95. Int. Dent. J. 2001, 51, 117–158. [Google Scholar] [CrossRef]
- Lynch, C.D.; Hale, R.; Chestnutt, I.G.; Wilson, N.H.F. Reasons for placement and replacement of crowns in general dental practice. Br. Dent. J. 2018, 225, 229–234. [Google Scholar] [CrossRef]
- Splieth, C.; Bernhardt, O.; Heinrich, A.; Bernhardt, H.; Meyer, G. Anaerobic microflora under Class I and Class II composite and amalgam restorations. Quintessence Int. 2003, 34, 497–503. [Google Scholar]
- Mo, S.; Bao, W.; Lai, G.; Wang, J.; Li, M. The microfloral analysis of secondary caries biofilm around Class I and Class II composite and amalgam fillings. BMC Infect. Dis. 2010, 10, 241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kidd, E.A.; Joyston-Bechal, S.; Beighton, D. Microbiological validation of assessments of caries activity during cavity preparation. Caries Res. 1993, 27, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Su, N.; Marek, C.L.; Ching, V.; Grushka, M. Caries prevention for patients with dry mouth. J. Can. Dent. Assoc. 2011, 77, b85. [Google Scholar] [PubMed]
- Niklander, S.; Veas, L.; Barrera, C.; Fuentes, F.; Chiappini, G.; Marshall, M. Risk factors, hyposalivation and impact of xerostomia on oral health-related quality of life. Braz. Oral Res. 2017, 31, e14. [Google Scholar] [CrossRef] [Green Version]
- Melo, M.A.S.; Guedes, S.F.F.; Xu, H.H.K.; Rodrigues, L.K.A. Nanotechnology-based restorative materials for dental caries management. Trends Biotechnol. 2013, 31, 459–467. [Google Scholar] [CrossRef] [Green Version]
- Weir, M.D.; Chow, L.C.; Xu, H.H.K. Remineralization of demineralized enamel via calcium phosphate nanocomposite. J. Dent. Res. 2012, 91, 979–984. [Google Scholar] [CrossRef] [Green Version]
- Moreau, J.L.; Sun, L.; Chow, L.C.; Xu, H.H.K. Mechanical and acid neutralizing properties and bacteria inhibition of amorphous calcium phosphate dental nanocomposite. J. Biomed. Mater. Res. Part B Appl. Biomater. 2011, 98, 80–88. [Google Scholar] [CrossRef] [Green Version]
- Xie, X.-J.; Xing, D.; Wang, L.; Zhou, H.; Weir, M.D.; Bai, Y.-X.; Xu, H.H. Novel rechargeable calcium phosphate nanoparticle-containing orthodontic cement. Int. J. Oral Sci. 2017, 9, 24–32. [Google Scholar] [CrossRef]
- Xu, H.H.K.; Moreau, J.L.; Sun, L.; Chow, L.C. Nanocomposite containing amorphous calcium phosphate nanoparticles for caries inhibition. Dent. Mater. 2011, 27, 762–769. [Google Scholar] [CrossRef] [Green Version]
- Melo, M.A.S.; Weir, M.D.; Rodrigues, L.K.A.; Xu, H.H.K. Novel calcium phosphate nanocomposite with caries-inhibition in a human in situ model. Dent. Mater. 2013, 29, 231–240. [Google Scholar] [CrossRef] [Green Version]
- Imazato, S.; Ebi, N.; Takahashi, Y.; Kaneko, T.; Ebisu, S.; Russell, R.R.B. Antibacterial activity of bactericide-immobilized filler for resin-based restoratives. Biomaterials 2003, 24, 3605–3609. [Google Scholar] [CrossRef]
- Simoncic, B.; Tomsic, B. Structures of Novel Antimicrobial Agents for Textiles—A Review. Text. Res. J. 2010, 80, 1721–1737. [Google Scholar] [CrossRef]
- Tiller, J.C.; Liao, C.-J.; Lewis, K.; Klibanov, A.M. Designing surfaces that kill bacteria on contact. Proc. Natl. Acad. Sci. USA 2001, 98, 5981–5985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, F.; Weir, M.D.; Xu, H.H.K. Effects of Quaternary Ammonium Chain Length on Antibacterial Bonding Agents. J. Dent. Res. 2013, 92, 932–938. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, M.S.; Ibrahim, A.S.; Balhaddad, A.A.; Weir, M.D.; Lin, N.J.; Tay, F.R.; Oates, T.W.; Xu, H.H.K.; Melo, M.A.S. A Novel Dental Sealant Containing Dimethylaminohexadecyl Methacrylate Suppresses the Cariogenic Pathogenicity of Streptococcus mutans Biofilms. Int. J. Mol. Sci. 2019, 20, 3491. [Google Scholar] [CrossRef] [Green Version]
- Baras, B.H.; Wang, S.; Melo, M.A.S.; Tay, F.; Fouad, A.F.; Arola, D.D.; Weir, M.D.; Xu, H.H.K. Novel bioactive root canal sealer with antibiofilm and remineralization properties. J. Dent. 2019, 83, 67–76. [Google Scholar] [CrossRef]
- Al-Dulaijan, Y.A.; Cheng, L.; Weir, M.D.; Melo, M.A.S.; Liu, H.; Oates, T.W.; Wang, L.; Xu, H.H.K. Novel rechargeable calcium phosphate nanocomposite with antibacterial activity to suppress biofilm acids and dental caries. J. Dent. 2018, 72, 44–52. [Google Scholar] [CrossRef]
- Cavallaro, A.; Mierczynska, A.; Barton, M.; Majewski, P.; Vasilev, K. Influence of immobilized quaternary ammonium group surface density on antimicrobial efficacy and cytotoxicity. Biofouling 2016, 32, 13–24. [Google Scholar] [CrossRef]
- Lin, W.; Yuan, D.; Deng, Z.; Niu, B.; Chen, Q. The cellular and molecular mechanism of glutaraldehyde-didecyldimethylammonium bromide as a disinfectant against Candida albicans. J. Appl. Microbiol. 2019, 126, 102–112. [Google Scholar] [CrossRef]
- Melo, M.A.S.; Cheng, L.; Weir, M.D.; Hsia, R.-C.; Rodrigues, L.K.A.; Xu, H.H.K. Novel dental adhesive containing antibacterial agents and calcium phosphate nanoparticles. J. Biomed. Mater. Res. Part. B Appl. Biomater. 2013, 101, 620–629. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Weir, M.D.; Hack, G.; Fouad, A.F.; Xu, H.H.K. Rechargeable dental adhesive with calcium phosphate nanoparticles for long-term ion release. J. Dent. 2015, 43, 1587–1595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, M.S.; AlQarni, F.D.; Al-Dulaijan, Y.A.; Weir, M.D.; Oates, T.W.; Xu, H.H.K.; Melo, M.A.S. Tuning Nano-Amorphous Calcium Phosphate Content in Novel Rechargeable Antibacterial Dental Sealant. Materials 2018, 11, 1544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonucci, J.M.; Zeiger, D.N.; Tang, K.; Lin-Gibson, S.; Fowler, B.O.; Lin, N.J. Synthesis and characterization of dimethacrylates containing quaternary ammonium functionalities for dental applications. Dent. Mater. 2012, 28, 219–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, C.; Weir, M.D.; Zhang, K.; Deng, D.; Cheng, L.; Xu, H.H.K. Synthesis of new antibacterial quaternary ammonium monomer for incorporation into CaP nanocomposite. Dent. Mater. 2013, 29, 859–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Qarni, F.D.; Tay, F.; Weir, M.D.; Melo, M.A.S.; Sun, J.; Oates, T.W.; Xie, X.; Xu, H.H.K. Protein-repelling adhesive resin containing calcium phosphate nanoparticles with repeated ion-recharge and re-releases. J. Dent. 2018, 78, 91–99. [Google Scholar] [CrossRef]
- Pereira, P.C.; Castilho, A.A.; Souza, R.O.A.; Passos, S.P.; Takahashi, F.E.; Bottino, M.A. A comparison of the film thickness of two adhesive luting agents and the effect of thermocycling on their microTBs to feldspathic ceramic. Acta Odontol. Latinoam. 2009, 22, 191–200. [Google Scholar]
- Bagheri, R. Film Thickness and Flow Properties of Resin-Based Cements at Different Temperatures. J. Dent. 2013, 14, 57–63. [Google Scholar]
- Chen, C.; Weir, M.D.; Cheng, L.; Lin, N.J.; Lin-Gibson, S.; Chow, L.C.; Zhou, X.; Xu, H.H.K. Antibacterial activity and ion release of bonding agent containing amorphous calcium phosphate nanoparticles. Dent. Mater. 2014, 30, 891–901. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Zhang, L.; Niu, L.; Yu, T.; Xu, H.H.K.; Weir, M.D.; Oates, T.W.; Tay, F.R.; Chen, J. Antibacterial and remineralizing orthodontic adhesive containing quaternary ammonium resin monomer and amorphous calcium phosphate nanoparticles. J. Dent. 2018, 72, 53–63. [Google Scholar] [CrossRef]
- Balhaddad, A.A.; Ibrahim, M.S.; Weir, M.D.; Xu, H.H.K.; Melo, M.A.S. Concentration dependence of quaternary ammonium monomer on the design of high-performance bioactive composite for root caries restorations. Dent. Mater. 2020, 36, e266–e278. [Google Scholar] [CrossRef]
- Mitwalli, H.; Balhaddad, A.A.; AlSahafi, R.; Oates, T.W.; Melo, M.A.S.; Xu, H.H.K.; Weir, M.D. Novel CaF2 Nanocomposites with Antibacterial Function and Fluoride and Calcium Ion Release to Inhibit Oral Biofilm and Protect Teeth. J. Funct. Biomater. 2020, 11, 56. [Google Scholar] [CrossRef] [PubMed]
- Vermeersch, G.; Leloup, G.; Delmée, M.; Vreven, J. Antibacterial activity of glass-ionomer cements, compomers and resin composites: Relationship between acidity and material setting phase. J. Oral Rehabil. 2005, 32, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Lewinstein, I.; Matalon, S.; Slutzkey, S.; Weiss, E.I. Antibacterial properties of aged dental cements evaluated by direct-contact and agar diffusion tests. J. Prosthet. Dent. 2005, 93, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Hiraishi, N.; Kitasako, Y.; Nikaido, T.; Foxton, R.M.; Tagami, J.; Nomura, S. Acidity of conventional luting cements and their diffusion through bovine dentine. Int. Endod. J. 2003, 36, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Cury, J.A.; de Oliveira, B.H.; dos Santos, A.P.P.; Tenuta, L.M.A. Are fluoride releasing dental materials clinically effective on caries control? Dent. Mater. 2016, 32, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Ge, Y.; Wang, S.; Zhou, X.; Wang, H.; Xu, H.H.K.; Cheng, L. The Use of Quaternary Ammonium to Combat Dental Caries. Materials 2015, 8, 3532–3549. [Google Scholar] [CrossRef] [Green Version]
- Zhang, N.; Weir, M.D.; Romberg, E.; Bai, Y.; Xu, H.H.K. Development of novel dental adhesive with double benefits of protein-repellent and antibacterial capabilities. Dent. Mater. 2015, 31, 845–854. [Google Scholar] [CrossRef]
- Michels, H.T.; Keevil, C.W.; Salgado, C.D.; Schmidt, M.G. From Laboratory Research to a Clinical Trial: Copper Alloy Surfaces Kill Bacteria and Reduce Hospital-Acquired Infections. HERD Health Environ. Res. Des. J. 2015. [Google Scholar] [CrossRef]
- Davis, C. Enumeration of probiotic strains: Review of culture-dependent and alternative techniques to quantify viable bacteria. J. Microbiol. Methods 2014, 103, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Berridge, M.V.; Herst, P.M.; Tan, A.S. Tetrazolium dyes as tools in cell biology: New insights into their cellular reduction. Biotechnol. Annu. Rev. 2005, 11, 127–152. [Google Scholar] [CrossRef]
- Zhou, H.; Li, F.; Weir, M.D.; Xu, H.H.K. Dental plaque microcosm response to bonding agents containing quaternary ammonium methacrylates with different chain lengths and charge densities. J. Dent. 2013, 41, 1122–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- G Nigam, A.; Jaiswal, J.; Murthy, R.; Pandey, R. Estimation of Fluoride Release from Various Dental Materials in Different Media—An In Vitro Study. Int. J. Clin. Pediatr. Dent. 2009, 2, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Forsten, L. Fluoride release and uptake by glass-ionomers and related materials and its clinical effect. Biomaterials 1998, 19, 503–508. [Google Scholar] [CrossRef]
- Balhaddad, A.A.; Kansara, A.A.; Hidan, D.; Weir, M.D.; Xu, H.H.K.; Melo, M.A.S. Toward dental caries: Exploring nanoparticle-based platforms and calcium phosphate compounds for dental restorative materials. Bioact. Mater. 2019, 4, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Langhorst, S.E.; O’Donnell, J.N.R.; Skrtic, D. In vitro remineralization of enamel by polymeric amorphous calcium phosphate composite: Quantitative microradiographic study. Dent. Mater. 2009, 25, 884–891. [Google Scholar] [CrossRef] [Green Version]
- International Organization for Standardization. ISO 4049 Dentistry: Polymer-Based Restorative Materials; International Organization for Standardization: Geneva, Switzerland, 2019. [Google Scholar]
- Marshall, S.J.; Bayne, S.C.; Baier, R.; Tomsia, A.P.; Marshall, G.W. A review of adhesion science. Dent. Mater. 2010, 26, e11–e16. [Google Scholar] [CrossRef]
- Schwartz, R.S. Adhesive dentistry and endodontics. Part 2: Bonding in the root canal system-the promise and the problems: A review. J. Endod. 2006, 32, 1125–1134. [Google Scholar] [CrossRef]
- Liu, B.; Lu, C.; Wu, Y.; Zhang, X.; Arola, D.; Zhang, D. The effects of adhesive type and thickness on stress distribution in molars restored with all-ceramic crowns. J. Prosthodont. 2011, 20, 35–44. [Google Scholar] [CrossRef]
- Skrtic, D.; Antonucci, J.M.; Liu, D.-W. Ethoxylated bisphenol dimethacrylate-based amorphous calcium phosphate composites. Acta Biomater. 2006, 2, 85–94. [Google Scholar] [CrossRef] [Green Version]
- Xie, X.; Wang, L.; Xing, D.; Qi, M.; Li, X.; Sun, J.; Melo, M.A.S.; Weir, M.D.; Oates, T.W.; Bai, Y.; et al. Novel rechargeable calcium phosphate nanoparticle-filled dental cement. Dent. Mater. J. 2019, 38, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Pameijer, C.H. A Review of Luting Agents. Int. J. Dent. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Powder | Liquid |
|---|---|
| Fluoroaluminosilicate (FAS) glass Potassium persulfate Ascorbic acid Opacifying agent | Methacrylated polycarboxylic acid Water Hydroxyethyl methacrylate (HEMA) Tartaric acid |
| Part A Part B | |||
| Chemical | Weight% | Chemical | Weight% |
| Cumene hydroperoxide (CHP) | 2% | Benzoyl thiourea (BTU) | 1% |
| 2,6-ditertbutyl-4-methylphenol (BHT) | 0.05% | Camphorquinone (CQ) | 0.4% |
| Pyromellitic glycerol dimethacrylate (PMGDM) | 87.95% | Ethyl-4-N,N-dimethylaminobenzoate (4E) | 1.6% |
| HEMA | 10% | Ethoxylated bisphenol-A-dimethacrylate (EBPADMA) | 77% |
| Bisphenol A-glycidyl methacrylate (BisGMA) | 10% | ||
| HEMA | 10% | ||
| Part A Part B | |||
| Chemical | Weight% | Chemical | Weight% |
| CHP | 2% | BTU | 1% |
| BHT | 0.05% | CQ | 0.4% |
| PMGDM | 81.5% | 4E | 1.6% |
| HEMA | 16.45% | EBPADMA | 70.55% |
| BisGMA | 12% | ||
| DMAHDM HEMA | 10.9% 3.55% | ||
| Part A Part B | |||
| Chemical | Weight% | Chemical | Weight% |
| CHP | 2% | BTU | 1% |
| BHT | 0.05% | CQ | 0.4% |
| PMGDM | 79.68% | 4E | 1.6% |
| HEMA | 14.72% | EBPADMA | 65.18% |
| EBPADMA | 3.55% | BisGMA | 12% |
| DMAHDM HEMA | 14.54% 5.28% | ||
| Part A Part B | |||
| Chemical | Weight% | Chemical | Weight% |
| CHP | 2% | BTU | 1% |
| BHT | 0.05% | CQ | 0.4% |
| PMGDM | 77.95% | 4E | 1.6% |
| HEMA | 16.45% | EBPADMA | 63.45% |
| EBPADMA | 3.55% | BisGMA | 12% |
| DMAHDM HEMA | 18% 3.55% | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlSahafi, R.; Balhaddad, A.A.; Mitwalli, H.; Ibrahim, M.S.; Melo, M.A.S.; Oates, T.W.; Xu, H.H.K.; Weir, M.D. Novel Crown Cement Containing Antibacterial Monomer and Calcium Phosphate Nanoparticles. Nanomaterials 2020, 10, 2001. https://0-doi-org.brum.beds.ac.uk/10.3390/nano10102001
AlSahafi R, Balhaddad AA, Mitwalli H, Ibrahim MS, Melo MAS, Oates TW, Xu HHK, Weir MD. Novel Crown Cement Containing Antibacterial Monomer and Calcium Phosphate Nanoparticles. Nanomaterials. 2020; 10(10):2001. https://0-doi-org.brum.beds.ac.uk/10.3390/nano10102001
Chicago/Turabian StyleAlSahafi, Rashed, Abdulrahman A. Balhaddad, Heba Mitwalli, Maria Salem Ibrahim, Mary Anne S. Melo, Thomas W. Oates, Hockin H.K. Xu, and Michael D. Weir. 2020. "Novel Crown Cement Containing Antibacterial Monomer and Calcium Phosphate Nanoparticles" Nanomaterials 10, no. 10: 2001. https://0-doi-org.brum.beds.ac.uk/10.3390/nano10102001