
Nanodelivery Strategies for Skin Diseases with Barrier Impairment: Focusing on Ceramides and Glucocorticoids




Abstract
:1. Introduction
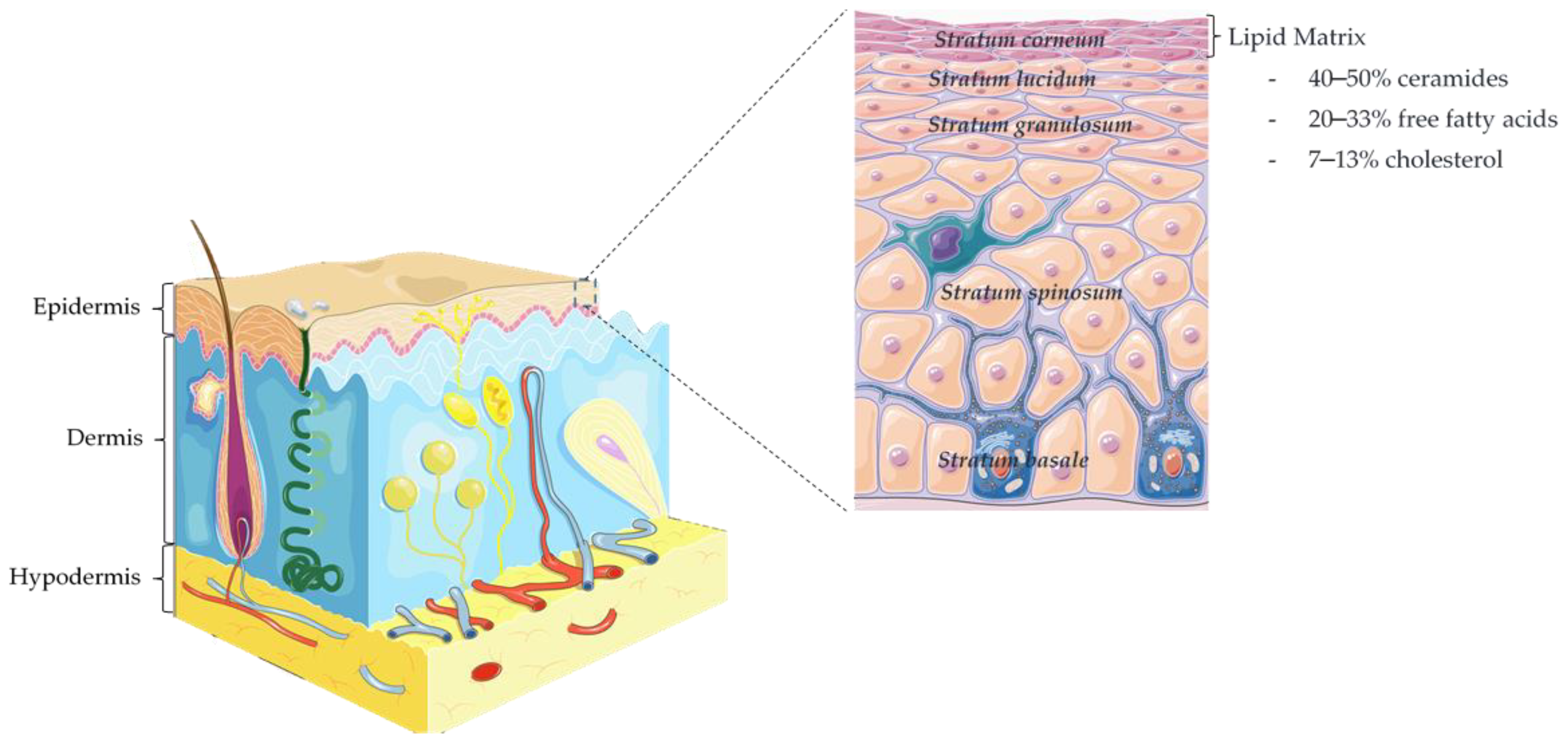
1.1. Epidermis and Skin Barrier Function
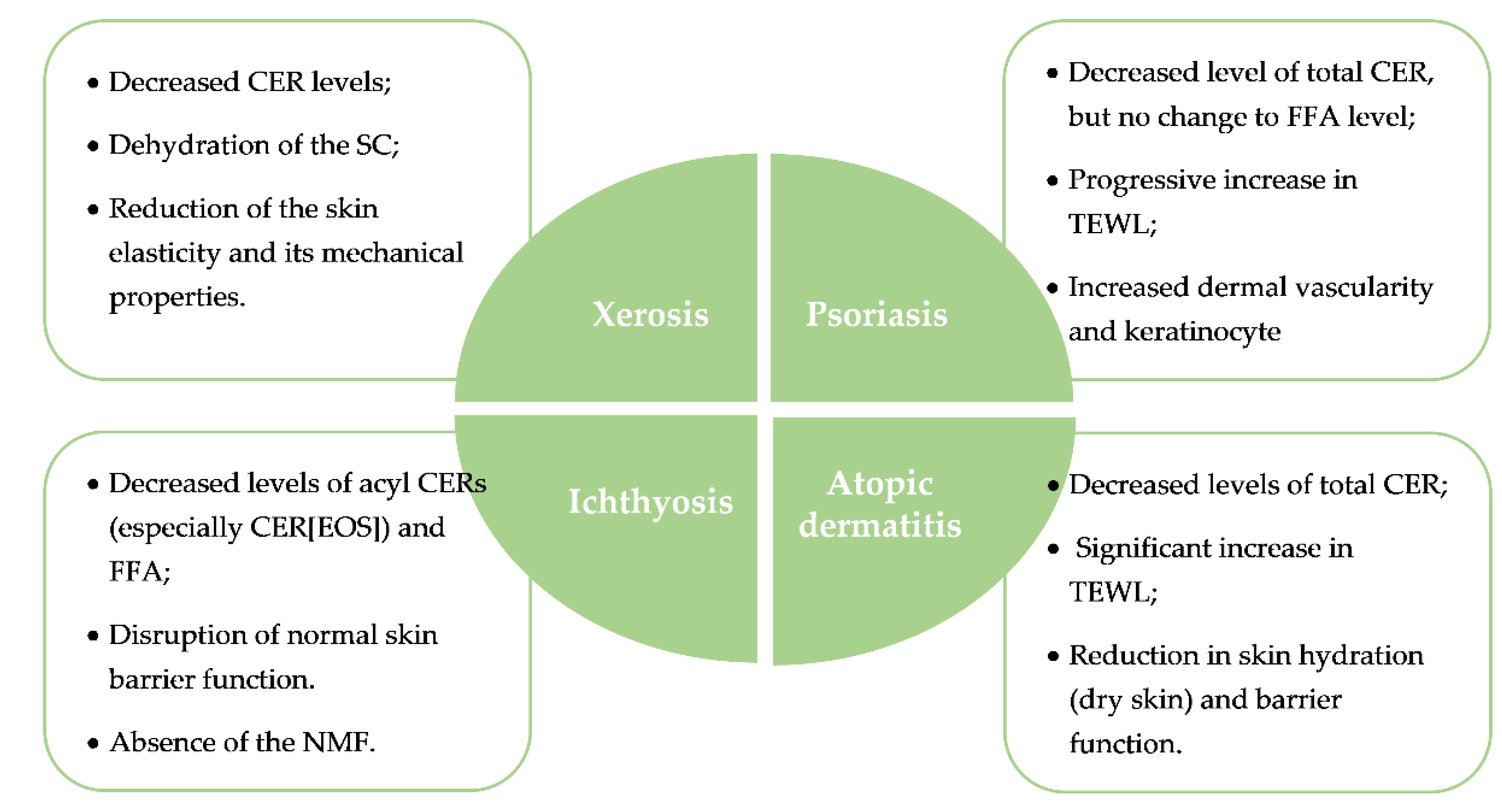
1.2. Skin Pathologies Associated with Barrier Impairment
1.2.1. Xerosis
1.2.2. Ichthyosis
1.2.3. Atopic Dermatitis
1.2.4. Psoriasis
2. Nanocarriers for Topical Delivery
2.1. Topical Nanodelivery of Glucocorticoids
2.1.1. Polymeric Nanoparticles
2.1.2. Lipid-Based Nanoparticles
2.1.3. Hybrid Nanoparticles
2.2. Topical Nanodelivery of Ceramides
2.2.1. Polymeric Nanoparticles
2.2.2. Lipid-Based Nanoparticles
3. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Abdo, J.M.; Sopko, N.A.; Milner, S.M. The applied anatomy of human skin: A model for regeneration. Wound Med. 2020, 28, 100179. [Google Scholar] [CrossRef]
- Karimkhani, C.; Dellavalle, R.P.; Coffeng, L.E.; Flohr, C.; Hay, R.J.; Langan, S.M.; Nsoesie, E.O.; Ferrari, A.J.; Erskine, H.E.; Silverberg, J.I.; et al. Global Skin Disease Morbidity and Mortality. JAMA Dermatol. 2017, 153, 406–412. [Google Scholar] [CrossRef]
- Garg, N.; Silverberg, J.I. Epidemiology of childhood atopic dermatitis. Clin. Dermatol. 2015, 33, 281–288. [Google Scholar] [CrossRef]
- Helmick, C.G.; Lee-Han, H.; Hirsch, S.C.; Baird, T.L.; Bartlett, C.L. Prevalence of Psoriasis Among Adults in the U.S. Am. J. Prev. Med. 2014, 47, 37–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zink, A.; Arents, B.; Fink-Wagner, A.; Seitz, I.; Mensing, U.; Wettemann, N.; Carlo, G.; Ring, J. Out-of-pocket Costs for Individuals with Atopic Eczema: A Cross-sectional Study in Nine European Countries. Acta Derm. Venereol. 2019, 99, 263–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comellas, M.; de Paz, H.D.; Marti, I.; Casañas, M.; Lizan, L.; Cortes, X. Social and Economic Burden of Skin Disease in Europe. A Narrative review of the Literature. Value Health 2016, 19, A567. [Google Scholar] [CrossRef]
- Chu, S.; Mehrmal, S.; Uppal, P.; Giesey, R.L.; Delost, M.E.; Delost, G.R. Burden of skin disease and associated socioeconomic status in Europe: An ecologic study from the Global Burden of Disease Study 2017. JAAD 2020, 1, 95–103. [Google Scholar] [CrossRef]
- Brezinski, E.A.; Dhillon, J.S.; Armstrong, A.W. Economic Burden of Psoriasis in the United States. JAMA Dermatol. 2015, 151, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Sahle, F.F.; Gebre-Mariam, T.; Dobner, B.; Wohlrab, J.; Neubert, R.H.H. Skin Diseases Associated with the Depletion of Stratum Corneum Lipids and Stratum Corneum Lipid Substitution Therapy. Skin Pharmacol. Physiol. 2015, 28, 42–55. [Google Scholar] [CrossRef]
- Bouwstra, J.A.; Ponec, M. The skin barrier in healthy and diseased state. Biochim. Biophys. Acta Biomembr. 2006, 1758, 2080–2095. [Google Scholar] [CrossRef] [Green Version]
- Wickett, R.R.; Visscher, M.O. Structure and function of the epidermal barrier. Am. J. Infect. Control 2006, 34, S98–S110. [Google Scholar] [CrossRef]
- Ishida-Yamamoto, A.; Igawa, S. The biology and regulation of corneodesmosomes. J. Cell Tissue Res. 2015, 360, 477–482. [Google Scholar] [CrossRef]
- Millington, P.F.; Wilkinson, R. Skin; Cambridge University Press: Cambridge, UK, 2009. [Google Scholar]
- Holleran, W.M.; Takagi, Y.; Uchida, Y. Epidermal sphingolipids: Metabolism, function, and roles in skin disorders. FEBS Lett. 2006, 580, 5456–5466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatfield, R.M.; Fung, L.W. Molecular properties of a stratum corneum model lipid system: Large unilamellar vesicles. Biophys. J. 1995, 68, 196–207. [Google Scholar] [CrossRef] [Green Version]
- Hatta, I.; Ohta, N.; Inoue, K.; Yagi, N. Coexistence of two domains in intercellular lipid matrix of stratum corneum. Biochim. Biophys. Acta Biomembr. 2006, 1758, 1830–1836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, L.; Ho, P.C.; Chan, S.Y. Interactions between a skin penetration enhancer and the main components of human stratum corneum lipids. J. Therm. Anal. Calorim. 2006, 83, 27–30. [Google Scholar] [CrossRef]
- Joo, K.-M.; Nam, G.-W.; Park, S.Y.; Han, J.Y.; Jeong, H.-J.; Lee, S.-Y.; Kim, H.K.; Lim, K.-M. Relationship between cutaneous barrier function and ceramide species in human stratum corneum. J. Dermatol. Sci. 2010, 60, 47–50. [Google Scholar] [CrossRef]
- Bonté, F.; Pinguet, P.; Chevalier, J.M.; Meybeck, A. Analysis of all stratum corneum lipids by automated multiple development high-performance thin-layer chromatography. J. Chromatogr. B Biomed. Sci. Appl. 1995, 664, 311–316. [Google Scholar] [CrossRef]
- Masukawa, Y.; Narita, H.; Sato, H.; Naoe, A.; Kondo, N.; Sugai, Y.; Oba, T.; Homma, R.; Ishikawa, J.; Takagi, Y.; et al. Comprehensive quantification of ceramide species in human stratum corneum. J. Lipid Res. 2009, 50, 1708–1719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Smeden, J.; Hoppel, L.; van der Heijden, R.; Hankemeier, T.; Vreeken, R.J.; Bouwstra, J.A. LC/MS analysis of stratum corneum lipids: Ceramide profiling and discovery. J. Lipid Res. 2011, 52, 1211–1221. [Google Scholar] [CrossRef] [Green Version]
- Elias, P.M. Epidermal barrier function: Intercellular lamellar lipid structures, origin, composition and metabolism. J. Control. Release 1991, 15, 199–208. [Google Scholar] [CrossRef]
- Wertz, P.W. Lipids and barrier function of the skin. Acta Derm. Venereol. 2000, 80, 7–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kendall, A.C.; Kiezel-Tsugunova, M.; Brownbridge, L.C.; Harwood, J.L.; Nicolaou, A. Lipid functions in skin: Differential effects of n-3 polyunsaturated fatty acids on cutaneous ceramides, in a human skin organ culture model. Biochim. Biophys. Acta Biomembr. 2017, 1859, 1679–1689. [Google Scholar] [CrossRef]
- Moore, D.J.; Rawlings, A.V. The chemistry, function and (patho)physiology of stratum corneum barrier ceramides. Int. J. Cosmet. Sci. 2017, 39, 366–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao-Qiang, M.; Elias, P.M.; Feingold, K.R. Fatty acids are required for epidermal permeability barrier function. J. Clin. Investig. 1993, 92, 791–798. [Google Scholar] [CrossRef] [Green Version]
- Jenerowicz, D.; Silny, W.; Dańczak-Pazdrowska, A.; Polańska, A.; Osmola-Mańkowska, A.; Olek-Hrab, K. Environmental factors and allergic diseases. Ann. Agric. Environ. Med. 2012, 19, 475–481. [Google Scholar]
- Rogers, J.; Harding, C.; Mayo, A.; Banks, J.; Rawlings, A. Stratum corneum lipids: The effect of ageing and the seasons. Arch. Dermatol. Res. 1996, 288, 765–770. [Google Scholar] [CrossRef]
- Jin, K.; Higaki, Y.; Takagi, Y.; Higuchi, K.; Yada, Y.; Kawashima, M.; Imokawa, G. Analysis of beta-glucocerebrosidase and ceramidase activities in atopic and aged dry skin. Acta Derm. Venereol. 1994, 74, 337–340. [Google Scholar] [CrossRef]
- Altemus, M.; Rao, B.; Dhabhar, F.S.; Ding, W.; Granstein, R.D. Stress-Induced Changes in Skin Barrier Function in Healthy Women. J. Investig. Dermatol. 2001, 117, 309–317. [Google Scholar] [CrossRef]
- White-Chu, E.F.; Reddy, M. Dry skin in the elderly: Complexities of a common problem. Clin. Dermatol. 2011, 29, 37–42. [Google Scholar] [CrossRef]
- Murphree, R.W. Impairments in Skin Integrity. Nurs. Clin. N. Am. 2017, 52, 405–417. [Google Scholar] [CrossRef]
- Rawlings, A.; Sabin, R.; Harding, C.; Watkinson, A.; Banks, J.; Ackerman, C. The effect of glycerol and humidity on desmosome degradation in stratum corneum. Arch. Dermatol. Res. 1995, 287, 457–464. [Google Scholar] [CrossRef]
- Rudikoff, D. The effect of dryness on the skin. Clin. Dermatol. 1998, 16, 99–107. [Google Scholar] [CrossRef]
- Rawlings, A.V.; Watkinson, A.; Rogers, J.; Mayo, A.M.; Hope, J.; Scott, I.R. Abnormalities in stratum corneum structure, 561 lipid composition, and desmosome degradation in soap-induced winter xerosis. J. Soc. Cosmet. Chem. 1994, 45, 203–220. [Google Scholar]
- Fowler, J. Understanding the Role of Natural Moisturizing Factor in Skin Hydration Components collectively called natural moisturizing factor (NMF) that occur naturally in the skin can be delivered topically to treat xerotic, dry skin. Pract. Derm. 2012, 36–40. [Google Scholar]
- Takeichi, T.; Akiyama, M. Inherited ichthyosis: Non-syndromic forms. J. Dermatol. 2016, 43, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Smith, F.J.D.; Irvine, A.D.; Terron-Kwiatkowski, A.; Sandilands, A.; Campbell, L.E.; Zhao, Y.; Liao, H.; Evans, A.T.; Goudie, D.R.; Lewis-Jones, S.; et al. Loss-of-function mutations in the gene encoding filaggrin cause ichthyosis vulgaris. Nat. Genet. 2006, 38, 337–342. [Google Scholar] [CrossRef]
- Elias, P.M.; Williams, M.L.; Holleran, W.M.; Jiang, Y.J.; Schmuth, M. Thematic review series: Skin Lipids. Pathogenesis of permeability barrier abnormalities in the ichthyoses: Inherited disorders of lipid metabolism. J. Lipid Res. 2008, 49, 697–714. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, L.; Buxman, M.; Weiss, R.; Vidgoff, J.; Dimond, R.; Roller, J.; Wells, R.S. Enzymatic basis of typical x-linked ichthyosis. Lancet 1978, 312, 756–757. [Google Scholar] [CrossRef]
- Eckl, K.-M.; Tidhar, R.; Thiele, H.; Oji, V.; Hausser, I.; Brodesser, S.; Preil, M.-L.; Önal-Akan, A.; Stock, F.; Müller, D.; et al. Impaired Epidermal Ceramide Synthesis Causes Autosomal Recessive Congenital Ichthyosis and Reveals the Importance of Ceramide Acyl Chain Length. J. Investig. Dermatol. 2013, 133, 2202–2211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nutten, S. Atopic Dermatitis: Global Epidemiology and Risk Factors. Ann. Nutr. Metab. 2015, 66, 8–16. [Google Scholar] [CrossRef]
- Weidinger, S.; Beck, L.A.; Bieber, T.; Kabashima, K.; Irvine, A.D. Atopic dermatitis. Nat. Rev. Dis. Primers 2018, 4, 18003. [Google Scholar] [CrossRef] [PubMed]
- Han, H.; Roan, F.; Ziegler, S.F. The atopic march: Current insights into skin barrier dysfunction and epithelial cell-derived cytokines. Immunol. Rev. 2017, 278, 116–130. [Google Scholar] [CrossRef] [PubMed]
- Imokawa, G.; Abe, A.; Jin, K.; Higaki, Y.; Kawashima, M.; Hidano, A. Decreased Level of Ceramides in Stratum Corneum of Atopic Dermatitis: An Etiologic Factor in Atopic Dry Skin? J. Investig. Dermatol. 1991, 96, 523–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, C.N.A.; Irvine, A.D.; Terron-Kwiatkowski, A.; Zhao, Y.; Liao, H.; Lee, S.P.; Goudie, D.R.; Sandilands, A.; Campbell, L.E.; Smith, F.J.D.; et al. Common loss-of-function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis. Nat. Genet. 2006, 38, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Fariñas, M.; Tintle, S.J.; Shemer, A.; Chiricozzi, A.; Nograles, K.; Cardinale, I.; Duan, S.; Bowcock, A.M.; Krueger, J.G.; Guttman-Yassky, E. Nonlesional atopic dermatitis skin is characterized by broad terminal differentiation defects and variable immune abnormalities. J. Allergy Clin. Immunol. 2011, 127, 954–964.e954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang-Yi, C.; Kusuda, S.; Seguchi, T.; Takahashi, M.; Aisu, K.; Tezuka, T. Decreased Level of Prosaposin in Atopic Skin. J. Investig. Dermatol. 1997, 109, 319–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arikawa, J.; Ishibashi, M.; Kawashima, M.; Takagi, Y.; Ichikawa, Y.; Imokawa, G. Decreased Levels of Sphingosine, a Natural Antimicrobial Agent, may be Associated with Vulnerability of the Stratum Corneum from Patients with Atopic Dermatitis to Colonization by Staphylococcus aureus. J. Investig. Dermatol. 2002, 119, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Janssens, M.; van Smeden, J.; Gooris, G.S.; Bras, W.; Portale, G.; Caspers, P.J.; Vreeken, R.J.; Hankemeier, T.; Kezic, S.; Wolterbeek, R.; et al. Increase in short-chain ceramides correlates with an altered lipid organization and decreased barrier function in atopic eczema patients. J. Lipid Res. 2012, 53, 2755–2766. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharya, N.; Sato, W.J.; Kelly, A.; Ganguli-Indra, G.; Indra, A.K. Epidermal Lipids: Key Mediators of Atopic Dermatitis Pathogenesis. Trends Mol. Med. 2019, 25, 551–562. [Google Scholar] [CrossRef]
- Li, S.; Ganguli-Indra, G.; Indra, A.K. Lipidomic analysis of epidermal lipids: A tool to predict progression of inflammatory skin disease in humans. Expert Rev. Proteomics 2016, 13, 451–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greb, J.E.; Goldminz, A.M.; Elder, J.T.; Lebwohl, M.G.; Gladman, D.D.; Wu, J.J.; Mehta, N.N.; Finlay, A.Y.; Gottlieb, A.B. Psoriasis. Nat. Rev. Dis. Primers 2016, 2, 16082. [Google Scholar] [CrossRef] [PubMed]
- Alshobaili, H.A.; Shahzad, M.; Al-Marshood, A.; Khalil, A.; Settin, A.; Barrimah, I. Genetic background of psoriasis. Int. J. Health Sci. 2010, 4, 23–29. [Google Scholar]
- Roberson, E.D.O.; Bowcock, A.M. Psoriasis genetics: Breaking the barrier. Trends Genet. 2010, 26, 415–423. [Google Scholar] [CrossRef] [Green Version]
- Tawada, C.; Kanoh, H.; Nakamura, M.; Mizutani, Y.; Fujisawa, T.; Banno, Y.; Seishima, M. Interferon-γ Decreases Ceramides with Long-Chain Fatty Acids: Possible Involvement in Atopic Dermatitis and Psoriasis. J. Investig. Dermatol. 2014, 134, 712–718. [Google Scholar] [CrossRef] [Green Version]
- Moon, S.-H.; Kim, J.-Y.; Song, E.-H.; Shin, M.-K.; Cho, Y.-H.; Kim, N.-I. Altered Levels of Sphingosine and Sphinganine in Psoriatic Epidermis. Ann. Dermatol. 2013, 25, 321. [Google Scholar] [CrossRef]
- Motta, S.; Monti, M.; Sesana, S.; Caputo, R.; Carelli, S.; Ghidoni, R. Ceramide composition of the psoriatic scale. Biochim. Biophys. Acta Mol. Basis Dis. 1993, 1182, 147–151. [Google Scholar] [CrossRef]
- Ruvolo, P.P. Ceramide regulates cellular homeostasis via diverse stress signaling pathways. Leukemia 2001, 15, 1153–1160. [Google Scholar] [CrossRef] [Green Version]
- Lew, B.-L.; Cho, Y.; Kim, J.; Sim, W.-Y.; Kim, N.-I. Ceramides and Cell Signaling Molecules in Psoriatic Epidermis: Reduced Levels of Ceramides, PKC-α, and JNK. J. Korean Med. Sci. 2006, 21, 95. [Google Scholar] [CrossRef] [Green Version]
- Damiani, G.; Pacifico, A.; Linder, D.M.; Pigatto, P.D.M.; Conic, R.; Grada, A.; Bragazzi, N.L. Nanodermatology-based solutions for psoriasis: State-of-the art and future prospects. Dermatol. Ther. 2019, 32, 1–15. [Google Scholar] [CrossRef]
- Draelos, Z.D. New treatments for restoring impaired epidermal barrier permeability: Skin barrier repair creams. Clin. Dermatol. 2012, 30, 345–348. [Google Scholar] [CrossRef]
- Sala, M.; Elaissari, A.; Fessi, H. Advances in psoriasis physiopathology and treatments: Up to date of mechanistic insights and perspectives of novel therapies based on innovative skin drug delivery systems (ISDDS). J. Control. Release 2016, 239, 182–202. [Google Scholar] [CrossRef]
- Gupta, M.; Agrawal, U.; Vyas, S.P. Nanocarrier-based topical drug delivery for the treatment of skin diseases. Expert Opin. Drug Deliv. 2012, 9, 783–804. [Google Scholar] [CrossRef]
- Rawat, M.; Singh, D.; Saraf, S.A.S.S.; Saraf, S. Nanocarriers: Promising Vehicle for Bioactive Drugs. Biol. Pharm. Bull. 2006, 29, 1790–1798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esfahani, D.R.; Tangen, K.M.; Sadeh, M.; Seksenyan, A.; Neisewander, B.L.; Mehta, A.I.; Linninger, A.A. Systems Engineers’ 630 Role in Biomedical Research. Convection-Enhanced Drug Delivery, 1st ed.; Elsevier B.V.: Amsterdam, The Netherlands, 2018; Volume 42. [Google Scholar]
- Jain, A.K.; Thareja, S. In vitro and in vivo characterization of pharmaceutical nanocarriers used for drug delivery. Artif. Cells Nanomed. Biotechnol. 2019, 47, 524–539. [Google Scholar] [CrossRef] [Green Version]
- Lombardo, D.; Kiselev, M.A.; Caccamo, M.T. Smart Nanoparticles for Drug Delivery Application: Development of Versatile Nanocarrier Platforms in Biotechnology and Nanomedicine. J. Nanomater. 2019, 2019, 1–26. [Google Scholar] [CrossRef]
- Santos, H.; Bimbo, L.; Peltonen, L.; Hirvonen, J. Inorganic Nanoparticles in Targeted Drug Delivery and Imaging. In Targeted Drug Delivery: Concepts and Design; Devarajan, P.V., Jain, S., Eds.; Springer: Mumbai/Mohali, India, 2015; pp. 571–613. [Google Scholar]
- Palmer, B.; DeLouise, L. Nanoparticle-Enabled Transdermal Drug Delivery Systems for Enhanced Dose Control and Tissue Targeting. Molecules 2016, 21, 1719. [Google Scholar] [CrossRef] [PubMed]
- Goyal, R.; Macri, L.K.; Kaplan, H.M.; Kohn, J. Nanoparticles and nanofibers for topical drug delivery. J. Control. Release 2016, 240, 77–92. [Google Scholar] [CrossRef] [Green Version]
- Roberts, M.S.; Mohammed, Y.; Pastore, M.N.; Namjoshi, S.; Yousef, S.; Alinaghi, A.; Haridass, I.N.; Abd, E.; Leite-Silva, V.R.; Benson, H.A.E.; et al. Topical and cutaneous delivery using nanosystems. J. Control. Release 2017, 247, 86–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, J.; Shanmugam, S.; Song, C.-K.; Kim, D.-D.; Choi, H.-G.; Yong, C.-S.; Woo, J.-S.; Yoo, B.K. Skin penetration and retention of L-Ascorbic acid 2-phosphate using multilamellar vesicles. Arch. Pharmacal Res. 2008, 31, 1652–1658. [Google Scholar] [CrossRef]
- Amnuaikit, T.; Limsuwan, T.; Khongkow, P.; Boonme, P. Vesicular carriers containing phenylethyl resorcinol for topical delivery system; liposomes, transfersomes and invasomes. Asian J. Pharm. Sci. 2018, 13, 472–484. [Google Scholar] [CrossRef] [PubMed]
- Fernández-García, R.; Lalatsa, A.; Statts, L.; Bolás-Fernández, F.; Ballesteros, M.P.; Serrano, D.R. Transferosomes as nanocarriers for drugs across the skin: Quality by design from lab to industrial scale. Int. J. Pharm. 2020, 573, 118817. [Google Scholar] [CrossRef]
- Naseri, N.; Valizadeh, H.; Zakeri-Milani, P. Solid Lipid Nanoparticles and Nanostructured Lipid Carriers: Structure, Preparation and Application. Adv. Pharm. Bull. 2015, 5, 305–313. [Google Scholar] [CrossRef] [Green Version]
- Gordillo-Galeano, A.; Mora-Huertas, C.E. Solid lipid nanoparticles and nanostructured lipid carriers: A review emphasizing on particle structure and drug release. Eur. J. Pharm. Biopharm. 2018, 133, 285–308. [Google Scholar] [CrossRef] [PubMed]
- Solaro, R.; Chiellini, F.; Battisti, A. Targeted Delivery of Protein Drugs by Nanocarriers. Materials 2010, 3, 1928–1980. [Google Scholar] [CrossRef] [Green Version]
- Souto, E.B.; Almeida, A.J.; Müller, R.H. Lipid Nanoparticles (SLN®, NLC®) for Cutaneous Drug Delivery:Structure, Protection and Skin Effects. J. Biomed. Nanotechnol. 2007, 3, 317–331. [Google Scholar] [CrossRef]
- Pardeike, J.; Hommoss, A.; Müller, R.H. Lipid nanoparticles (SLN, NLC) in cosmetic and pharmaceutical dermal products. Int. J. Pharm. 2009, 366, 170–184. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, S. Natural Polymer Drug Delivery Systems: Nanoparticles, Plants, and Algae; Springer International Publishing: Cham, Switzerland, 2016. [Google Scholar] [CrossRef]
- Zhang, Z.; Tsai, P.-C.; Ramezanli, T.; Michniak-Kohn, B.B. Polymeric nanoparticles-based topical delivery systems for the treatment of dermatological diseases. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2013, 5, 205–218. [Google Scholar] [CrossRef] [Green Version]
- El-Say, K.M.; El-Sawy, H.S. Polymeric nanoparticles: Promising platform for drug delivery. Int. J. Pharm. 2017, 528, 675–691. [Google Scholar] [CrossRef]
- Kumari, A.; Yadav, S.K.; Yadav, S.C. Biodegradable polymeric nanoparticles based drug delivery systems. Colloids Surf. B 2010, 75, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Da Costa, L.A.G.; de Souza, M.L.; de Sousa, A.L.M.D.; Silva, E.D.O.; da Silva, R.M.F.; Rolim, L.A.; Rolim-Neto, P.J. Innovation Overview of Nanoparticle-Based Dermatological Products: A Patent Study. Recent Pat. Nanotechnol. 2020, 14, 128–140. [Google Scholar] [CrossRef]
- Ghosh, P.; Han, G.; De, M.; Kim, C.; Rotello, V. Gold nanoparticles in delivery applications☆. Adv. Drug Delivery Rev. 2008, 60, 1307–1315. [Google Scholar] [CrossRef]
- Yeh, Y.-C.; Creran, B.; Rotello, V.M. Gold nanoparticles: Preparation, properties, and applications in bionanotechnology. Nanoscale 2012, 4, 1871–1880. [Google Scholar] [CrossRef]
- Gurunathan, S.; Park, J.H.; Han, J.W.; Kim, J.-H. Comparative assessment of the apoptotic potential of silver nanoparticles synthesized by Bacillus tequilensis and Calocybe in MDA-MB-231 human breast cancer cells: Targeting p53 for anticancer therapy. Int. J. Nanomed. 2015, 10, 4203–4223. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.-F.; Liu, Z.-G.; Shen, W.; Gurunathan, S. Silver Nanoparticles: Synthesis, Characterization, Properties, Applications, and Therapeutic Approaches. Int. J. Mol. Sci. 2016, 17, 1534. [Google Scholar] [CrossRef] [PubMed]
- Jafari, S.; Derakhshankhah, H.; Alaei, L.; Fattahi, A.; Varnamkhasti, B.S.; Saboury, A.A. Mesoporous silica nanoparticles for therapeutic/diagnostic applications. Biomed. Pharmacother. 2019, 109, 1100–1111. [Google Scholar] [CrossRef] [PubMed]
- Nicolaides, N.C.; Charmandari, E.; Chrousos, G.P. Overview of Glucocorticoids. In Encyclopedia of Endocrine Diseases; Elsevier: Amsterdam, The Netherlands, 2018; pp. 64–71. [Google Scholar] [CrossRef]
- Ference, J.D.; Last, A.R. Choosing topical corticosteroids. Am. Fam. Physician 2009, 79, 135–140. [Google Scholar]
- Ahluwalia, A. Topical glucocorticoids and the skin-mechanisms of action: An update. Mediat. Inflamm. 1998, 7, 183–193. [Google Scholar] [CrossRef]
- Narasimha Murthy, S.; Shivakumar, H.N. Topical and Transdermal Drug Delivery. In Handbook of Non-Invasive Drug Delivery Systems; Kulkarni, V.S., Ed.; William Andrew Publishing: Kidlington, Oxford, UK, 2010; pp. 1–36. [Google Scholar] [CrossRef]
- Lutz, M.E.; El-Azhary, R.A. Allergic Contact Dermatitis Due to Topical Application of Corticosteroids: Review and Clinical Implications. Mayo Clin. Proc. 1997, 72, 1141–1144. [Google Scholar] [CrossRef] [PubMed]
- Laws, P.M.; Young, H.S. Current and Emerging Systemic Treatment Strategies for Psoriasis. Drugs 2012, 72, 1867–1880. [Google Scholar] [CrossRef]
- Pople, P.V.; Singh, K.K. Development and evaluation of colloidal modified nanolipid carrier: Application to topical delivery of tacrolimus. Eur. J. Pharm. Biopharm. 2011, 79, 82–94. [Google Scholar] [CrossRef]
- Balzus, B.; Sahle, F.F.; Hönzke, S.; Gerecke, C.; Schumacher, F.; Hedtrich, S.; Kleuser, B.; Bodmeier, R. Formulation and ex vivo evaluation of polymeric nanoparticles for controlled delivery of corticosteroids to the skin and the corneal epithelium. Eur. J. Pharm. Biopharm. 2017, 115, 122–130. [Google Scholar] [CrossRef]
- Dong, P.; Sahle, F.F.; Lohan, S.B.; Saeidpour, S.; Albrecht, S.; Teutloff, C.; Bodmeier, R.; Unbehauen, M.; Wolff, C.; Haag, R.; et al. pH-sensitive Eudragit® L 100 nanoparticles promote cutaneous penetration and drug release on the skin. J. Control. Release 2019, 295, 214–222. [Google Scholar] [CrossRef]
- Rosado, C.; Silva, C.; Reis, C.P. Hydrocortisone-loaded poly(ε-caprolactone) nanoparticles for atopic dermatitis treatment. Pharm. Dev. Technol. 2013, 18, 710–718. [Google Scholar] [CrossRef] [Green Version]
- Hussain, Z.; Katas, H.; Mohd Amin, M.C.; Kumolosasi, E.; Sahudin, S. Downregulation of immunological mediators in 2,4-dinitrofluorobenzene-induced atopic dermatitis-like skin lesions by hydrocortisone-loaded chitosan nanoparticles. Int. J. Nanomed. 2014, 9, 5143–5156. [Google Scholar] [CrossRef] [Green Version]
- Beber, T.C.; de Andrade, D.F.; Santos Chaves, P.D.; Pohlmann, A.R.; Guterres, S.S.; Ruver Beck, R.C. Cationic Polymeric Nanocapsules as a Strategy to Target Dexamethasone to Viable Epidermis: Skin Penetration and Permeation Studies. J. Nanosci. Nanotechnol. 2016, 16, 1331–1338. [Google Scholar] [CrossRef]
- Pandey, M.; Choudhury, H.; Gunasegaran, T.A.P.; Nathan, S.S.; Md, S.; Gorain, B.; Tripathy, M.; Hussain, Z. Hyaluronic acid-modified betamethasone encapsulated polymeric nanoparticles: Fabrication, characterisation, in vitro release kinetics, and dermal targeting. Drug Deliv. Transl. Res. 2019, 9, 520–533. [Google Scholar] [CrossRef] [PubMed]
- Schlupp, P.; Blaschke, T.; Kramer, K.D.; Höltje, H.D.; Mehnert, W.; Schäfer-Korting, M. Drug Release and Skin Penetration from Solid Lipid Nanoparticles and a Base Cream: A Systematic Approach from a Comparison of Three Glucocorticoids. Skin Pharmacol. Physiol. 2011, 24, 199–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pradhan, M.; Singh, D.; Singh, M.R. Influence of selected variables on fabrication of Triamcinolone acetonide loaded solid lipid nanoparticles for topical treatment of dermal disorders. Artif. Cells Nanomed. Biotechnol. 2016, 44, 392–400. [Google Scholar] [CrossRef]
- Bikkad, M.L.; Nathani, A.H.; Mandlik, S.K.; Shrotriya, S.N.; Ranpise, N.S. Halobetasol propionate-loaded solid lipid nanoparticles (SLN) for skin targeting by topical delivery. J. Liposome Res. 2014, 24, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, M.; Singh, D.; Murthy, S.N.; Singh, M.R. Design, characterization and skin permeating potential of Fluocinolone acetonide loaded nanostructured lipid carriers for topical treatment of psoriasis. Steroids 2015, 101, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, M.; Singh, D.; Singh, M.R. Fabrication, optimization and characterization of Triamcinolone acetonide loaded nanostructured lipid carriers for topical treatment of psoriasis: Application of Box Behnken design, in vitro and ex vivo studies. J. Drug Deliv. Sci. Technol. 2017, 41, 325–333. [Google Scholar] [CrossRef]
- Silva, L.A.D.; Andrade, L.M.; de Sá, F.A.P.; Marreto, R.N.; Lima, E.M.; Gratieri, T.; Taveira, S.F. Clobetasol-loaded nanostructured lipid carriers for epidermal targeting. J. Pharm. Pharmacol. 2016, 68, 742–750. [Google Scholar] [CrossRef]
- Pukale, S.S.; Sharma, S.; Dalela, M.; Singh, A.K.; Mohanty, S.; Mittal, A.; Chitkara, D. Multi-component clobetasol-loaded monolithic lipid-polymer hybrid nanoparticles ameliorate imiquimod-induced psoriasis-like skin inflammation in Swiss albino mice. Acta Biomater. 2020, 115, 393–409. [Google Scholar] [CrossRef] [PubMed]
- Date, T.; Nimbalkar, V.; Kamat, J.; Mittal, A.; Mahato, R.I.; Chitkara, D. Lipid-polymer hybrid nanocarriers for delivering cancer therapeutics. J. Control. Release 2018, 271, 60–73. [Google Scholar] [CrossRef]
- Imokawa, G. A possible mechanism underlying the ceramide deficiency in atopic dermatitis: Expression of a deacylase enzyme that cleaves the N-acyl linkage of sphingomyelin and glucosylceramide. J. Dermatol. Sci. 2009, 55, 1–9. [Google Scholar] [CrossRef]
- Pappas, A. Epidermal surface lipids. Derm. Endocrinol. 2009, 1, 72–76. [Google Scholar] [CrossRef] [Green Version]
- Madaan, A. Epiceram for the treatment of atopic dermatitis. Drugs Today 2008, 44, 751. [Google Scholar] [CrossRef]
- DFB Pharmaceuticals Technology LTD. CeraVe. Available online: https://www.cerave.com/ (accessed on 7 January 2022).
- Vávrová, K.; Hrabálek, A.; Mac-Mary, S.; Humbert, P.; Muret, P. Ceramide analogue 14S24 selectively recovers perturbed human skin barrier. Br. J. Dermatol. 2007, 157, 704–712. [Google Scholar] [CrossRef]
- Bellew, S.; Del Rosso, J.Q. Overcoming the Barrier Treatment of Ichthyosis: A Combination-therapy Approach. J. Clin. Aesthet. Dermatol. 2010, 3, 49–53. [Google Scholar]
- Koppes, S.; Charles, F.; Lammers, L.; Frings-Dresen, M.; Kezic, S.; Rustemeyer, T. Efficacy of a Cream Containing Ceramides and Magnesium in the Treatment of Mild to Moderate Atopic Dermatitis: A Randomized, Double-blind, Emollient- and Hydrocortisone-controlled Trial. Acta Derm. Venereol. 2016, 96, 948–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishida, K.; Takahashi, A.; Bito, K.; Draelos, Z.; Imokawa, G. Treatment with Synthetic Pseudoceramide Improves Atopic Skin, Switching the Ceramide Profile to a Healthy Skin Phenotype. J. Investig. Dermatol. 2020, 140, 1762–1770.e1768. [Google Scholar] [CrossRef]
- Su, R.; Yang, L.; Wang, Y.; Yu, S.; Guo, Y.; Deng, J.; Zhao, Q.; Jin, X. Formulation, development, and optimization of a novel octyldodecanol-based nanoemulsion for transdermal delivery of ceramide IIIB. Int. J. Nanomed. 2017, 12, 5203–5221. [Google Scholar] [CrossRef] [Green Version]
- Kahraman, E.; Kaykın, M.; Şahin Bektay, H.; Güngör, S. Recent Advances on Topical Application of Ceramides to Restore Barrier Function of Skin. Cosmetics 2019, 6, 52. [Google Scholar] [CrossRef] [Green Version]
- Van Smeden, J.; Bouwstra, J.A. Stratum Corneum Lipids: Their Role for the Skin Barrier Function in Healthy Subjects and Atopic Dermatitis Patients. Curr. Probl. Dermatol. 2016, 49, 8–26. [Google Scholar] [CrossRef]
- Jung, S.-M.; Yoon, G.H.; Lee, H.C.; Jung, M.H.; Yu, S.I.; Yeon, S.J.; Min, S.K.; Kwon, Y.S.; Hwang, J.H.; Shin, H.S. Thermodynamic Insights and Conceptual Design of Skin-Sensitive Chitosan Coated Ceramide/PLGA Nanodrug for Regeneration of Stratum Corneum on Atopic Dermatitis. Sci. Rep. 2015, 5, 18089. [Google Scholar] [CrossRef] [PubMed]
- Tessema, E.N.; Gebre-Mariam, T.; Paulos, G.; Wohlrab, J.; Neubert, R.H.H. Delivery of oat-derived phytoceramides into the stratum corneum of the skin using nanocarriers: Formulation, characterization and in vitro and ex-vivo penetration studies. Eur. J. Pharm. Biopharm. 2018, 127, 260–269. [Google Scholar] [CrossRef]
- Deli, G.; Hatziantoniou, S.; Nikas, Y.; Demetzos, C. Solid lipid nanoparticles and nanoemulsions containing ceramides: Preparation and physicochemical characterization. J. Liposome Res. 2009, 19, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Gaur, P.K.; Mishra, S.; Verma, A.; Verma, N. Ceramide–palmitic acid complex based Curcumin solid lipid nanoparticles for transdermal delivery: Pharmacokinetic and pharmacodynamic study. J. Exp. Nanosci. 2016, 11, 38–53. [Google Scholar] [CrossRef] [Green Version]
- Noh, G.Y.; Suh, J.Y.; Park, S.N. Ceramide-based nanostructured lipid carriers for transdermal delivery of isoliquiritigenin: Development, physicochemical characterization, and in vitro skin permeation studies. Korean J. Chem. Eng. 2017, 34, 400–406. [Google Scholar] [CrossRef]
- Yilmaz, E.; Borchert, H.-H. Design of a phytosphingosine-containing, positively-charged nanoemulsion as a colloidal carrier system for dermal application of ceramides. Eur. J. Pharm. Biopharm. 2005, 60, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Abdelgawad, R.; Nasr, M.; Moftah, N.H.; Hamza, M.Y. Phospholipid membrane tubulation using ceramide doping “Cerosomes”: Characterization and clinical application in psoriasis treatment. Eur. J. Pharm. Sci. 2017, 101, 258–268. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Library of Medicine. Trial to Assess the Potency of SOR007 Ointment in a Psoriasis Plaque Test. Available online: https://clinicaltrials.gov/ct2/show/NCT03004339 (accessed on 7 January 2022).



{kind=link}
{kind=link}
| Type of Nanocarrier | Advantages | Disadvantages | Potential for Topical Applications | Ref. | |
|---|---|---|---|---|---|
| Lipid-based nanoparticles |
| High flexibility, biocompatibility, and biodegradability. | Short shelf life; low stability; low encapsulation efficacy. | Improved the penetration of drugs through the skin. | [68,74,75,76] |
| High biocompatibility and biodegradability; Easier to scale-up the production. | Long-term instability in terms of size and loading capacity. | Improved skin permeability and retention time of drugs in SC; Decreased water loss and enhanced skin hydration. | [77,78,79] | |
| Greater stability and higher loading capacity than SLN; Reduction of the drug expulsion during storage. | Long-term instability is still possible. | [76,77,79,80] | ||
| Polymeric nanoparticles |
| Highly biocompatible; Non-toxic. | Susceptibility to pH variations; Low reproducibility; Prone to degradation; Potentially antigenic. | Decreased adverse reactions due to applied drugs; decreased skin rash; enhanced skin permeation; increased retention of lipophilic drugs. | [68,78,81,82] |
| Higher stability in biological fluids and controllable physicochemical properties; High versatility and ease of production; Low costs. | Some polymers’ cytotoxicity. | [78,82,83,84] | ||
| Metallic nanoparticles |
| Easily prepared, functionalized and dispersed in liquids; Versatile platform for therapeutic agents. | Biosafety issues of gold; high costs. | Antioxidant and antimicrobial activity; antiaging properties. | [85,86,87] |
| Application as antimicrobial, anti-inflammatory, antiangiogenic, and anticancer agent; green chemistry techniques show high yield, solubility and high stability. | Conventional methods of preparation are considered expensive and use toxic substances; biosafety issues of silver. | Antimicrobial activity potential for wound- or burn-dressings. | [88,89] | |
| Silica nanoparticles | Good biocompatibility and controllable size; easy surface and pore functionalization; high drug loading; good thermal and chemical stability. | Difficult production protocols; instability of the colloidal suspensions. | Possibility to load hydrophylic/lipophilic compounds. | [68,90] | |
| Type of Nanoparticle | Composition | Glucocorticoid | Type of study | Ref. |
|---|---|---|---|---|
| Polymeric nanoparticles | Ethyl cellulose and Eudragit® | Dexamethasone | In vitro & Ex vivo | [98] |
| Eudragit® L100 | Dexamethasone | In vitro & Ex vivo | [99] | |
| Poly (ε-caprolactone) | Hydrocortisone | In vitro | [100] | |
| Chitosan | Hydrocortisone | In vitro & Preclinical (mice) | [101] | |
| Eudragit® RS 100 | Dexamethasone | In vitro & Ex vivo | [102] | |
| Hyaluronic acid-coated chitosan | Betamethasone | In vitro & Ex vivo | [103] | |
| Solid lipid nanoparticles | Compritol® 888 ATO, Poloxamer® 188 | Prednisolone, diester prednicarbate, betamethasone 17-valerate | In vitro & Ex vivo | [104] |
| Compritol® 888 ATO, Poloxamer® 188, soya lecithin | Triamcinolone Acetonide | In vitro & Ex vivo | [105] | |
| Glycerol monostearate | Halobetasol Propionate | Ex vivo & Preclinical (rabbit) | [106] | |
| Nanostructured lipid carriers | Compritol® 888 ATO and Miglyol® 812 | Fluocinolone Acetonide | In vitro & Ex vivo | [107] |
| Compritol® 888 ATO and Miglyol® 812 | Triamcinolone Acetonide | In vitro & Ex vivo | [108] | |
| Stearic acid, oleic acid, and lecithin. Chitosan for coating. | Clobetasol Propionate | In vitro & Ex vivo | [109] | |
|
Hybrid nanoparticles | mPEG-PLA copolymer, Precirol® ATO5 and glycerol monostearate, linoleic and oleic acid | Clobetasol Propionate | In vitro, Ex vivo & Preclinical (mice) | [110] |
| Type of Nanoparticle | Composition | Ceramides | Type of Study | Ref. |
|---|---|---|---|---|
| Polymeric nanoparticles | Chitosan-coated PLGA | NR | In vitro, Ex vivo & Preclinical (rats) | [123] |
| Cassava starch acetate | Oat glucosylceramides | In vitro & Ex vivo | [124] | |
| Solid lipid nanoparticles | Lecithin and caprylic/capric triglycerides | Egg-ceramides | In vitro | [125] |
| Glyceryl monostearate, stearic acid, and palmitic acid | N-stearoyl-DL-sphinganin | In vito, Ex vivo & Preclinical (rats) | [126] | |
| Nanostructured lipid carriers | Cholesterol and caprylic-capric triglyceride | DS-Ceramide Y30 | In vitro & Ex vivo | [127] |
| Nanoemulsions | Lipoid E-80®, cholesterol, palmitic acid and α-tocopherol | Ceramide III, ceramide IIIB, and phytosphingosine (PS) | In vitro | [128] |
| Vesicular nanosystems | Epikuron 200, Sodium deoxycholate and tween 80 | Ceramide VI | In vitro, Ex vivo & Clinical | [129] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida, C.; Filipe, P.; Rosado, C.; Pereira-Leite, C. Nanodelivery Strategies for Skin Diseases with Barrier Impairment: Focusing on Ceramides and Glucocorticoids. Nanomaterials 2022, 12, 275. https://0-doi-org.brum.beds.ac.uk/10.3390/nano12020275
Almeida C, Filipe P, Rosado C, Pereira-Leite C. Nanodelivery Strategies for Skin Diseases with Barrier Impairment: Focusing on Ceramides and Glucocorticoids. Nanomaterials. 2022; 12(2):275. https://0-doi-org.brum.beds.ac.uk/10.3390/nano12020275
Chicago/Turabian StyleAlmeida, Cíntia, Patrícia Filipe, Catarina Rosado, and Catarina Pereira-Leite. 2022. "Nanodelivery Strategies for Skin Diseases with Barrier Impairment: Focusing on Ceramides and Glucocorticoids" Nanomaterials 12, no. 2: 275. https://0-doi-org.brum.beds.ac.uk/10.3390/nano12020275