Tri-Ponderal Mass Index vs. Fat Mass/Height3 as a Screening Tool for Metabolic Syndrome Prediction in Colombian Children and Young People

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Sample Population
2.2. Data Collection
2.3. Metabolic Syndrome Diagnosis
2.4. Statistical Analysis
3. Results
3.1. Study Participants
3.2. Relationship between BMI, FMI, TMI, and MetS Score
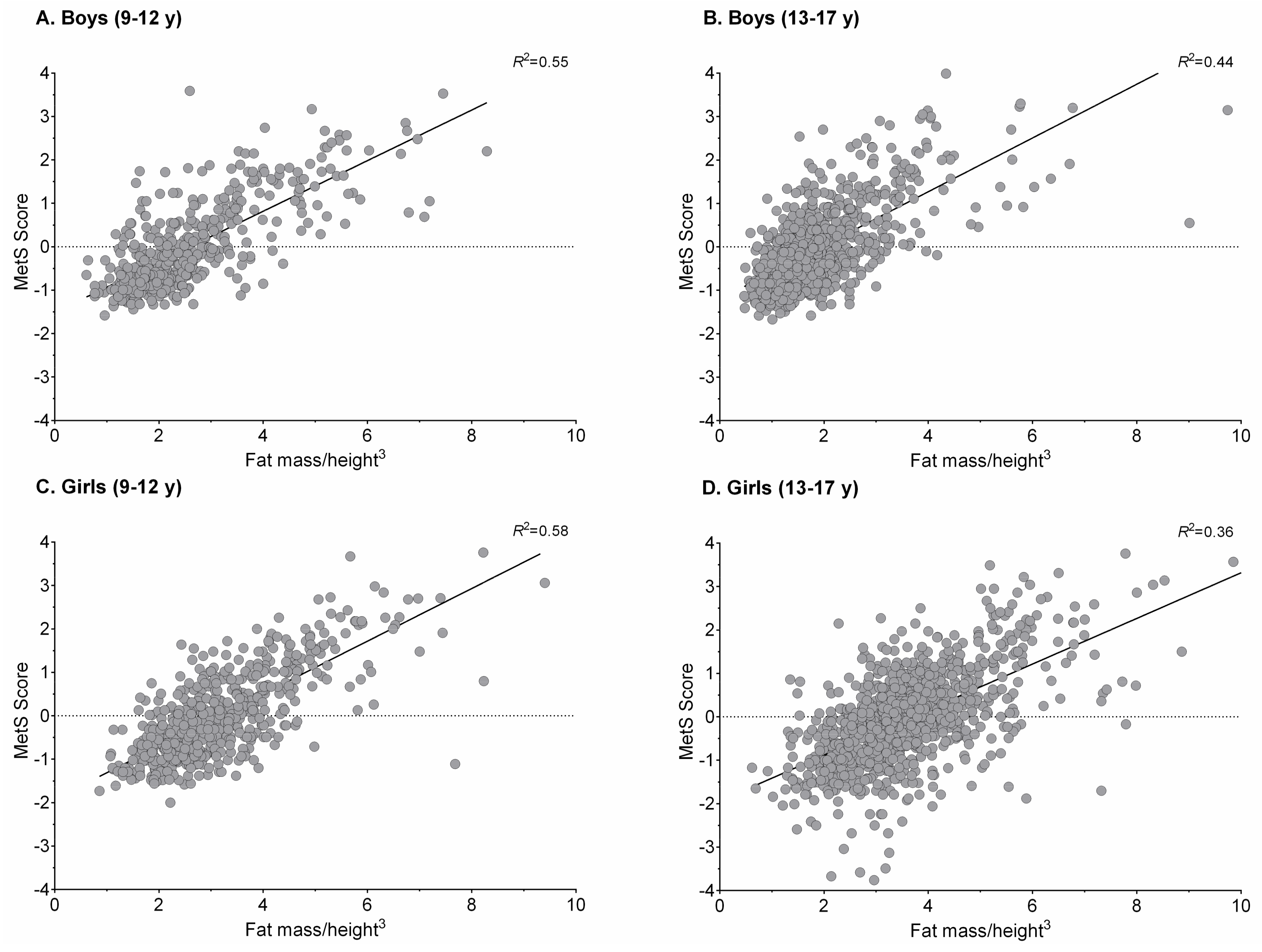
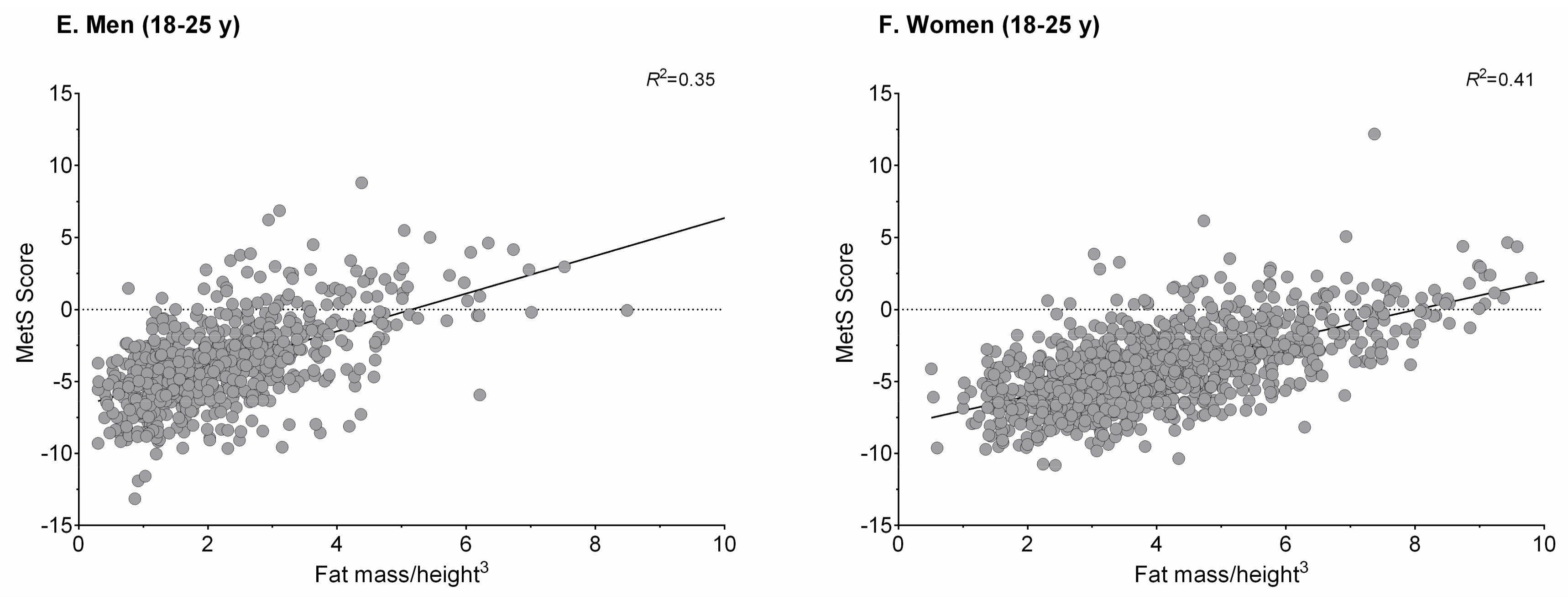
3.3. Association between FMI, TMI, and MetS Score
3.4. Optimal Cut-Off Value in the Screening of MetS
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| BF | body fat |
| BIA | bioelectrical impedance analysis |
| BMI | body mass index |
| CI | confidence interval |
| CVD | cardiovascular disease |
| FUPRECOL | in Spanish: Association between Muscular Strength and Metabolic Risk Factors in Colombia |
| FMI | fat mass index |
| HDL-C | high-density lipoprotein cholesterol |
| IDF | International Diabetes Federation |
| LDL-C | low-density lipoprotein cholesterol |
| MetS | metabolic syndrome |
| SD | standard deviation |
| TMI | tri-ponderal mass index |
| WC | waist circumference |
References
- Bonora, E.; Targher, G.; Formentini, G.; Calcaterra, F.; Lombardi, S.; Marini, F.; Zenari, L.; Saggiani, F.; Poli, M.; Perbellini, S.; et al. The Metabolic Syndrome is an independent predictor of cardiovascular disease in Type 2 diabetic subjects. Prospective data from the Verona Diabetes Complications Study. Diabet. Med. 2004, 21, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Despres, J.-P.; Lemieux, I.; Bergeron, J.; Pibarot, P.; Mathieu, P.; Larose, E.; Rodés-Cabau, J.; Bertrand, O.F.; Poirier, P. Abdominal Obesity and the Metabolic Syndrome: Contribution to Global Cardiometabolic Risk. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Zambon, S.; Zanoni, S.; Romanato, G.; Corti, M.C.; Noale, M.; Sartori, L.; Musacchio, E.; Baggio, G.; Crepaldi, G.; Manza, E. Metabolic syndrome and all-cause and cardiovascular mortality in an Italian elderly population: The Progetto Veneto Anziani (Pro.V.A.) Study. Diabetes Care 2009, 32, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Palaniappan, L.; Carnethon, M.R.; Wang, Y.; Hanley, A.J.; Fortmann, S.P.; Haffner, S.M.; Wagenknecht, L. Insulin Resistance Atherosclerosis Study. Predictors of the incident metabolic syndrome in adults: The Insulin Resistance Atherosclerosis Study. Diabetes Care 2004, 27, 788–793. [Google Scholar] [CrossRef] [PubMed]
- Mancia, G.; Bombelli, M.; Corrao, G.; Facchetti, R.; Madotto, F.; Giannattasio, C.; Trevano, F.Q.; Grassi, G.; Zanchetti, A.; Sega, R. Metabolic Syndrome in the Pressioni Arteriose Monitorate E Loro Associazioni (PAMELA) Study: Daily Life Blood Pressure, Cardiac Damage, and Prognosis. Hypertension 2007, 49, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Moreira, G.C.; Cipullo, J.P.; Ciorlia, L.A.; Cesarino, C.B.; Vilela-Martin, J.F. Prevalence of Metabolic Syndrome: Association with Risk Factors and Cardiovascular Complications in an Urban Population. PLoS ONE 2014, 9, e105056. [Google Scholar] [CrossRef] [PubMed]
- González, S.A.; Castiblanco, M.A.; Arias-Gómez, L.F.; Martinez-Ospina, A.; Cohen, D.D.; Holguin, G.A.; Almanza, A.; Lemos, D.M.; Correa-Bautista, J.E.; Escobar, I.D.; et al. Results From Colombia’s 2016 Report Card on Physical Activity for Children and Youth. J. Phys. Act. Health 2016, 13, S129–S136. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Correa-Bautista, J.E.; González-Ruíz, K.; Vivas, A.; Triana-Reina, H.R.; Martínez-Torres, J.; Prieto-Benavides, D.H.; Carrillo, H.A.; Ramos-Sepúlveda, J.A.; Villa-González, E.; et al. Body Adiposity Index Performance in Estimating Body Fat Percentage in Colombian College Students: Findings from the FUPRECOL-Adults Study. Nutrients 2017, 9, 40. [Google Scholar] [CrossRef] [PubMed]
- Mallare, J.T.; Karabell, A.H.; Velasquez-Mieyer, P.; Stender, S.R.S.; Christensen, M.L. Current and Future Treatment of Metabolic Syndrome and Type 2 Diabetes in Children and Adolescents. Diabetes Spectr. 2005, 18, 220–228. [Google Scholar] [CrossRef]
- Kaur, J. A comprehensive review on metabolic syndrome. Cardiol. Res. Pract. 2014, 2014, 943162. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Anzola, A.; Martinez-Torres, J.; Vivas, A.; Tordecilla-Sanders, A.; Prieto-Benavides, D.; Izquierdo, M.; Correa-Bautista, J.E.; Garcia-Hermoso, A. Metabolic Syndrome and Associated Factors in a Population-Based Sample of Schoolchildren in Colombia: The FUPRECOL Study. Metab. Syndr. Relat. Disord. 2016, 14, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Torres, J.; Correa-Bautista, J.; González-Ruíz, K.; Vivas, A.; Triana-Reina, H.R.; Prieto-Benavidez, D.H.; Carrillo, H.A.; Ramos-Sepúlveda, J.A.; Villa-González, E.; García-Hermoso, A.; et al. A Cross-Sectional Study of the Prevalence of Metabolic Syndrome and Associated Factors in Colombian Collegiate Students: The FUPRECOL-Adults Study. Int. J. Environ. Res. Public Health 2017, 14, 233. [Google Scholar] [CrossRef] [PubMed]
- Cole, T. Weight-stature indices to measure underweight, overweight and obesity. In Anthr Assess Nutrition Status; Wiley-Liss: New York, NY, USA, 1991; pp. 83–111. [Google Scholar]
- Peterson, C.M.; Su, H.; Thomas, D.M.; Golnabi, A.H.; Pietrobelli, A.; Heymsfield, S.B. Tri-Ponderal Mass Index vs Body Mass Index in Estimating Body Fat During Adolescence. JAMA Pediatr. 2017, 171, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J. Weight/heightp compared to weight/height2 for assessing adiposity in childhood: Influence of age and bone age on p during puberty. Ann. Hum. Biol. 1986, 13, 433–451. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Correa-Bautista, J.; Sanders-Tordecilla, A.; Ojeda-Pardo, M.L.; Cobo-Mejía, E.A.; Castellanos-Vega, R.D.P.; García-Hermoso, A.; González-Jiménez, E.; Schmidt-RioValle, J.; González-Ruíz, K.; et al. Percentage of Body Fat and Fat Mass Index as a Screening Tool for Metabolic Syndrome Prediction in Colombian University Students. Nutrients 2017, 9, 1009. [Google Scholar] [CrossRef] [PubMed]
- Burton, R.F. Why is the body mass index calculated as mass/height2, not as mass/height3? Ann. Hum. Biol. 2007, 34, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Burton, R.F. Measures of adiposity: The inappropriate use of the fat mass index. Int. J. Obes. 2010, 34, 213. [Google Scholar] [CrossRef] [PubMed]
- VanItallie, T.B.; Yang, M.U.; Heymsfield, S.B.; Funk, R.C.; Boileau, R.A. Height-normalized indices of the body’s fat-free mass and fat mass: Potentially useful indicators of nutritional status. Am. J. Clin. Nutr. 1990, 52, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; Mander, A.P.; Jones, L.R.; Emmett, P.M.; Jebb, S.A. A prospective analysis of dietary energy density at age 5 and 7 years and fatness at 9 years among UK children. Int. J. Obes. 2008, 32, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Ma, F.; Lou, H.; Liu, Y. The utility of fat mass index vs. body mass index and percentage of body fat in the screening of metabolic syndrome. BMC Public Health 2013, 13, 629. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; García-Hermoso, A.; Agostinis-Sobrinho, C.; Mota, J.; Santos, R.; Correa-Bautista, J.E.; Peña-Guzmán, C.A.; Domínguez-Sánchez, M.A.; Schmidt-RioValle, J.; González-Jiménez, E. Pubertal Stage, Body Mass Index, and Cardiometabolic Risk in Children and Adolescents in Bogotá, Colombia: The Cross-Sectional Fuprecol Study. Nutrients 2017, 9, 644. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Correa-Bautista, J.E.; Lobelo, F.; Izquierdo, M.; Alonso-Martínez, A.; Rodríguez-Rodríguez, F.; Cristi-Montero, C. High muscular fitness has a powerful protective cardiometabolic effect in adults: Influence of weight status. BMC Public Health 2016, 16, 1012. [Google Scholar] [CrossRef] [PubMed]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Marfell-Jones, M.; Olds, T.; Stewart, A. International standards for anthropometric assessment. Int. Soc. Adv. Kinanthropometry 2011. [Google Scholar] [CrossRef]
- Rodríguez-Rodríguez, F.; Cristi-Montero, C.; González-Ruíz, K.; Correa-Bautista, J.E.; Ramírez-Vélez, R. Bioelectrical Impedance Vector Analysis and Muscular Fitness in Healthy Men. Nutrients 2016, 8, 407. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Correa-Bautista, J.; Martínez-Torres, J.; González-Ruíz, K.; González-Jiménez, E.; Schmidt-RioValle, J.; Garcia-Hermoso, A. Performance of Two Bioelectrical Impedance Analyses in the Diagnosis of Overweight and Obesity in Children and Adolescents: The FUPRECOL Study. Nutrients 2016, 8, 575. [Google Scholar] [CrossRef] [PubMed]
- De Ferranti, S.D.; Gauvreau, K.; Ludwig, D.S.; Neufeld, E.J.; Newburger, J.W.; Rifai, N. Prevalence of the Metabolic Syndrome in American Adolescents: Findings From the Third National Health and Nutrition Examination Survey. Circulation 2004, 110, 2494–2497. [Google Scholar] [CrossRef] [PubMed]
- Magge, S.N.; Goodman, E.; Armstrong, S.C.; Committee on Nutrition; Section On Endocrinology; Section on Obesity. The Metabolic Syndrome in Children and Adolescents: Shifting the Focus to Cardiometabolic Risk Factor Clustering. Pediatrics 2017, e20171603. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Bewick, V.; Cheek, L.; Ball, J. Statistics review 13: Receiver operating characteristic curves. Crit. Care 2004, 8, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Fluss, R.; Faraggi, D.; Reiser, B. Estimation of the Youden Index and its associated cutoff point. Biom. J. 2005, 47, 458–472. [Google Scholar] [CrossRef] [PubMed]
- Ruano Nieto, C.I.; Melo Pérez, J.D.; Mogrovejo Freire, L.; De Paula Morales, K.R.; Espinoza Romero, C.V. Prevalence of metabolic syndrome and associated risk factors in ecuadorian university students. Nutr. Hosp. 2015, 31, 1574–1581. [Google Scholar] [CrossRef] [PubMed]
- Eissa, M.A.; Dai, S.; Mihalopoulos, N.L.; Day, R.S.; Harrist, R.B.; Labarthe, D.R. Trajectories of fat mass index, fat free-mass index, and waist circumference in children: Project HeartBeat! Am. J. Prev. Med. 2009, 37, S34–S39. [Google Scholar] [CrossRef] [PubMed]
- Maynard, L.M.; Wisemandle, W.; Roche, A.F.; Chumlea, W.C.; Guo, S.S.; Siervogel, R.M. Childhood body composition in relation to body mass index. Pediatrics 2001, 107, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.S.; Wang, J.; Maynard, L.M.; Thornton, J.C.; Mei, Z.; Pierson, R.N.; Dietz, W.H.; Horlick, M. Relation of BMI to fat and fat-free mass among children and adolescents. Int. J. Obes. 2005, 29, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nakao, T.; Komiya, S. Reference norms for a fat-free mass index and fat mass index in the Japanese child population. J. Physiol. Anthropol. Appl. Hum. Sci. 2003, 22, 293–298. [Google Scholar] [CrossRef]
- Gishti, O.; Kruithof, C.J.; Felix, J.F.; Raat, H.; Hofman, A.; Duijts, L.; Gaillard, R.; Jaddoe, V.W. Ethnic disparities in general and abdominal adiposity at school age: A multiethnic population-based cohort study in the Netherlands. Ann. Nutr. Metab. 2014, 64, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kubik, M.Y. Child’s Weight Status and Parent’s Response to a School-Based Body Mass Index Screening and Parent Notification Program. J. Sch. Nurs. 2015, 31, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Laurson, K.R.; Eisenmann, J.C.; Welk, G.J. Body Fat Percentile Curves for U.S. Children and Adolescents. Am. J. Prev. Med. 2011, 41, S87–S92. [Google Scholar] [CrossRef] [PubMed]
- Rolland-Cachera, M.F. Body composition during adolescence: Methods, limitations and determinants. Horm. Res. 1993, 39, 25–40. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Children 9–12 Years (n = 1047) | Adolescents 13–17 Years (n = 1830) | Young Adults 18–25 Years (n = 1796) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Girls (n = 582) | Boys (n = 465) | p-Value | Girls (n = 986) | Boys (n = 844) | p-Value | Women (n = 1104) | Men (n = 692) | p-Value | |
| Anthropometric variable | |||||||||
| Age (years) | 10.8 (1.1) | 10.7 (1.1) | 0.104 | 14.6 (1.3) | 14.7 (1.3) | 0.077 | 21.9 (1.9) | 22.6 (1.2) | 0.624 |
| Weight (kg) | 38.2 (8.8) | 37.6 (9.6) | 0.353 | 50.9 (8.6) | 53.0 (10.4) | <0.001 | 58.7 (10.3) | 68.9 (12.1) | <0.001 |
| Height (m) | 1.43 (0.09) | 1.42 (0.10) | 0.526 | 1.55 (0.06) | 1.63 (0.10) | <0.001 | 1.59 (0.05) | 1.72 (0.06) | <0.001 |
| WC (cm) | 60.1 (7.1) | 62.2 (7.7) | <0.001 | 65.9 (6.8) | 67.5 (6.8) | <0.001 | 71.5 (8.0) | 78.2 (8.0) | <0.001 |
| BMI (kg/m2) | 18.5 (2.8) | 18.4 (3.0) | 0.312 | 21.0 (3.0) | 19.9 (2.8) | <0.001 | 23.2 (3.7) | 23.1 (3.6) | 0.810 |
| BMI z | 0.91 (0.4) | 1.12 (0.7) | <0.001 | 0.51 (0.5) | 0.39 (0.3) | <0.001 | - | - | - |
| Overweight by BMI/z-BMI n (%) * | 141 (24.4) | 78 (16.9) | 0.001 | 221 (22.5) | 82 (9.8) | 0.001 | 236 (21.4) | 144 (20.8) | 0.724 |
| Obesity by BMI/z-BMI n (%) * | 51 (8.8) | 47 (10.2) | 0.001 | 43 (4.4) | 23 (2.7) | 0,001 | 61 (5.5) | 33 (4.8) | 0.722 |
| TMI (kg/m3) | 13.0 (1.9) | 12.9 (1.9) | 0.447 | 13.6 (1.9) | 12.2 (1.7) | <0.001 | 14.6 (2.4) | 13.4 (2.1) | <0.001 |
| Body fat (%) | 23.6 (5.8) | 19.3 (6.5) | <0.001 | 25.7 (6.0) | 15.1 (5.9) | <0.001 | 27.0 (7.2) | 15.6 (6.5) | <0.001 |
| FMI (fat mass)/height3) | 3.2 (1.2) | 2.6 (1.3) | <0.001 | 3.6 (1.3) | 1.9 (1.1) | <0.001 | 4.0 (1.7) | 2.2 (1.3) | <0.001 |
| Blood pressure | |||||||||
| Systolic blood pressure (mmHg) | 109.6 (13.8) | 111.0 (13.7) | 0.113 | 110.6 (11.5) | 114.4 (14.0) | <0.001 | 111.2 (11.1) | 120.2 (12.9) | <0.001 |
| Diastolic blood pressure (mmHg) | 67.1 (8.6) | 66.6 (8.9) | 0389 | 69.4 (8.6) | 68.9 (9.4) | 0.288 | 71.7 (9.3) | 74.1 (11.4) | <0.001 |
| Mean arterial pressure (mmHg) | 81.2 (8.7) | 81.4 (8.9) | 0.797 | 83.1 (8.2) | 84.0 (9.4) | 0.020 | 91.5 (8.9) | 97.2 (10.9) | <0.001 |
| Metabolic biomarkers | |||||||||
| Total cholesterol (mg/dL) | 151.3 (29.3) | 152.1 (30.3) | 0.656 | 148.3 (31.3) | 132.9 (30.3) | <0.001 | 146.3 (33.3) | 132.7 (30.2) | <0.001 |
| Triglycerides (mg/dL) | 96.0 (60.4) | 86.8 (44.7) | 0.006 | 96.7 (50.2) | 84.4 (35.8) | <0.001 | 88.5 (45.3) | 93.7 (48.5) | 0.020 |
| LDL-C (mg/dL) | 86.0 (26.6) | 86.6 (30.0) | 0.756 | 84.6 (29.4) | 78.6 (35.9) | <0.001 | 87.9 (26.1) | 81.0 (26.0) | <0.001 |
| HDL-C (mg/dL) | 48.4 (13.0) | 51.5 (13.1) | <0.001 | 46.9 (11.7) | 44.4 (11.2) | <0.001 | 43.9 (12.8) | 39.5 (10.6) | <0.001 |
| Glucose (mg/dL) | 83.3 (15.0) | 85.3 (16.2) | 0.038 | 80.5 (16.1) | 82.3 (15.5) | 0.015 | 86.0 (11.5) | 85.5 (11.7) | <0.001 |
| MetS score | -0.12 (0.13) | -0.14 (0.12) | 0.008 | -0.13 (0.11) | -0.14 (0.09) | 0.077 | −3.94 (2.66) | −3.90 (2.78) | 0.501 |
| Metabolic Syndrome n (%) * | |||||||||
| Yes | 85 (14.6) | 60 (12.9) | 0.428 | 80 (8.1) | 56 (6.5) | 0.229 | 82 (7.4) | 166 (9.2) | 0.001 |
| Group and Variable | MetS Score | TMI (kg/m3) | FMI (Fat Mass)/Height3) | BMI |
|---|---|---|---|---|
| Children 9–12 years (n = 1047) | ||||
| BMI | 0.534 * | 0.938 * | 0.942 * | 1 |
| FMI (fat mass)/height3) | 0.522 * | 0.911 * | 1 | |
| TMI (kg/m3) | 0.462 * | 1 | ||
| cMets | 1 | |||
| Adolescents 13–17 years (n = 1830) | ||||
| BMI | 0.455 * | 0.942 * | 0.882 * | 1 |
| FMI (fat mass)/height3) | 0.427 * | 0.846 * | 1 | |
| TMI (kg/m3) | 0.386 * | 1 | ||
| cMets | 1 | |||
| Young adults 18–25 years (n = 1796) | ||||
| BMI | 0.600 * | 0.971 * | 0.943 * | 1 |
| FMI (fat mass)/height3) | 0.602 * | 0.912 * | 1 | |
| TMI (kg/m3) | 0.554 * | 1 | ||
| cMets | 1 |
| High Risk of MetS | |||
|---|---|---|---|
| Parameter | TMI (kg/m3) | FMI (Fat Mass)/Height3) | |
| Girls (9–12 years) | AUC | 0.674 | 0.698 |
| 95% CI | 0.608–0.740 | 0.634–0.763 | |
| p-value | <0.0001 | <0.0001 | |
| J-Youden | 0.19 | 0.18 | |
| Cut-off | 12.13 | 2.59 | |
| Sensitivity (%) | 80 | 85 | |
| Specificity (%) | 61 | 59 | |
| LR (+) | 2.04 | 2.05 | |
| LR (−) | 0.33 | 0.26 | |
| Boys (9–12 years) | AUC | 0.755 | 0.752 |
| 95% CI | 0.677–0.833 | 0.676–0.828 | |
| p value | <0.0001 | <0.0001 | |
| J-Youden | 0.17 | 0.19 | |
| Cut-off | 12.10 | 1.98 | |
| Sensitivity (%) | 85 | 82 | |
| Specificity (%) | 59 | 60 | |
| LR (+) | 2.05 | 2.04 | |
| LR (−) | 0.26 | 0.31 | |
| Girls (13–17 years) | AUC | 0.684 | 0.699 |
| 95% CI | 0.619–0.748 | 0.635–0.762 | |
| p-value | <0.0001 | <0.0001 | |
| J-Youden | 0.11 | 0.13 | |
| Cut-off | 12.48 | 3.12 | |
| Sensitivity (%) | 86 | 87 | |
| Specificity (%) | 70 | 66 | |
| LR (+) | 2.87 | 2.55 | |
| LR (−) | 0.20 | 0.19 | |
| Boys (13–17 years) | AUC | 0.729 | 0.745 |
| 95% CI | 0.654–0.797 | 0.675–0.816 | |
| p-value | <0.0001 | <0.0001 | |
| J-Youden | 0.19 | 0.18 | |
| Cut-off | 11.19 | 1.46 | |
| Sensitivity (%) | 93 | 84 | |
| Specificity (%) | 70 | 60 | |
| LR (+) | 3.09 | 2.10 | |
| LR (−) | 0.10 | 0.27 | |
| High Risk of MetS | |||
|---|---|---|---|
| Parameter | TMI (kg/m3) | FMI (Fat Mass)/Height3) | |
| Women (18–25 years) | AUC | 0.854 | 0.882 |
| 95% CI | 0.805–0.903 | 0.840–0.924 | |
| p-value | <0.0001 | <0.0001 | |
| J-Youden | 0.14 | 0.12 | |
| Cut-off | 13.21 | 3.27 | |
| Sensitivity (%) | 94 | 95 | |
| Specificity (%) | 67 | 62 | |
| LR (+) | 2.81 | 2.52 | |
| LR (−) | 0.09 | 0.08 | |
| Men (18–25 years) | AUC | 0.814 | 0.848 |
| 95% CI | 0.759–0.869 | 0.800–0.896 | |
| p-value | <0.0001 | <0.0001 | |
| J-Youden | 0.10 | 0.15 | |
| Cut-off | 12.19 | 1.65 | |
| Sensitivity (%) | 94 | 93 | |
| Specificity (%) | 70 | 57 | |
| LR (+) | 3.11 | 2.14 | |
| LR (−) | 0.09 | 0.13 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramírez-Vélez, R.; Correa-Bautista, J.E.; Carrillo, H.A.; González-Jiménez, E.; Schmidt-RioValle, J.; Correa-Rodríguez, M.; García-Hermoso, A.; González-Ruíz, K. Tri-Ponderal Mass Index vs. Fat Mass/Height3 as a Screening Tool for Metabolic Syndrome Prediction in Colombian Children and Young People. Nutrients 2018, 10, 412. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10040412
Ramírez-Vélez R, Correa-Bautista JE, Carrillo HA, González-Jiménez E, Schmidt-RioValle J, Correa-Rodríguez M, García-Hermoso A, González-Ruíz K. Tri-Ponderal Mass Index vs. Fat Mass/Height3 as a Screening Tool for Metabolic Syndrome Prediction in Colombian Children and Young People. Nutrients. 2018; 10(4):412. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10040412
Chicago/Turabian StyleRamírez-Vélez, Robinson, Jorge Enrique Correa-Bautista, Hugo Alejandro Carrillo, Emilio González-Jiménez, Jacqueline Schmidt-RioValle, María Correa-Rodríguez, Antonio García-Hermoso, and Katherine González-Ruíz. 2018. "Tri-Ponderal Mass Index vs. Fat Mass/Height3 as a Screening Tool for Metabolic Syndrome Prediction in Colombian Children and Young People" Nutrients 10, no. 4: 412. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10040412