Changing to a Low-Polyphenol Diet Alters Vascular Biomarkers in Healthy Men after Only Two Weeks

 , and
, and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Subjects
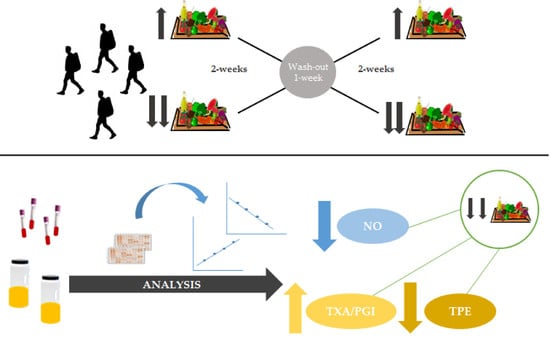
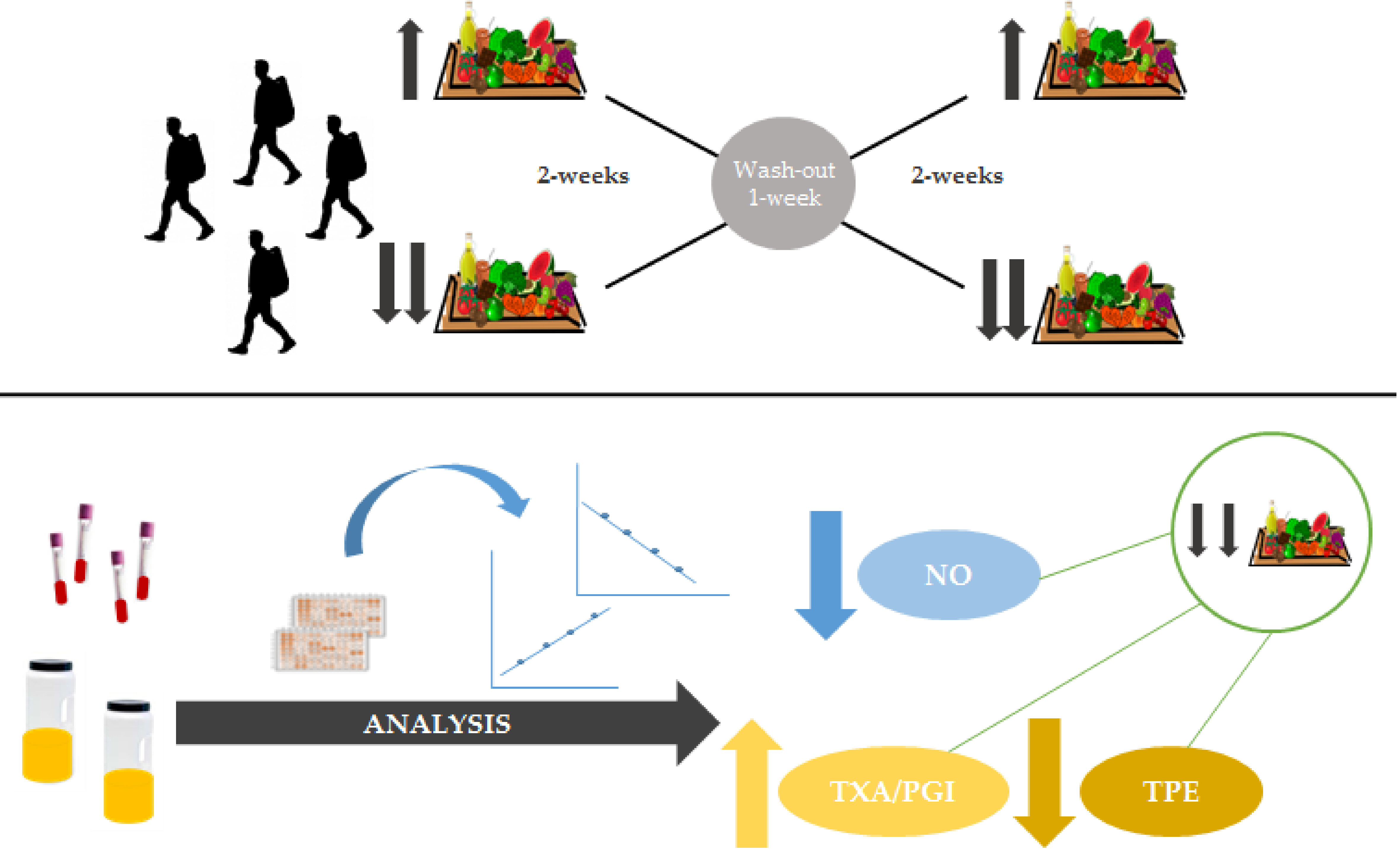
2.2. Study Design
2.3. Dietary and Physical Activity Assessments
2.4. Blood and Urine Collection
2.5. Clinical and Anthropometric Measurements
2.6. Quantification of Total Polyphenol Excretion (TPE) in Urine Samples
2.7. Determination of Plasmatic Inflammatory Biomarkers
2.8. Determination of Eicosanoids in Urine
2.9. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Dietary Intake
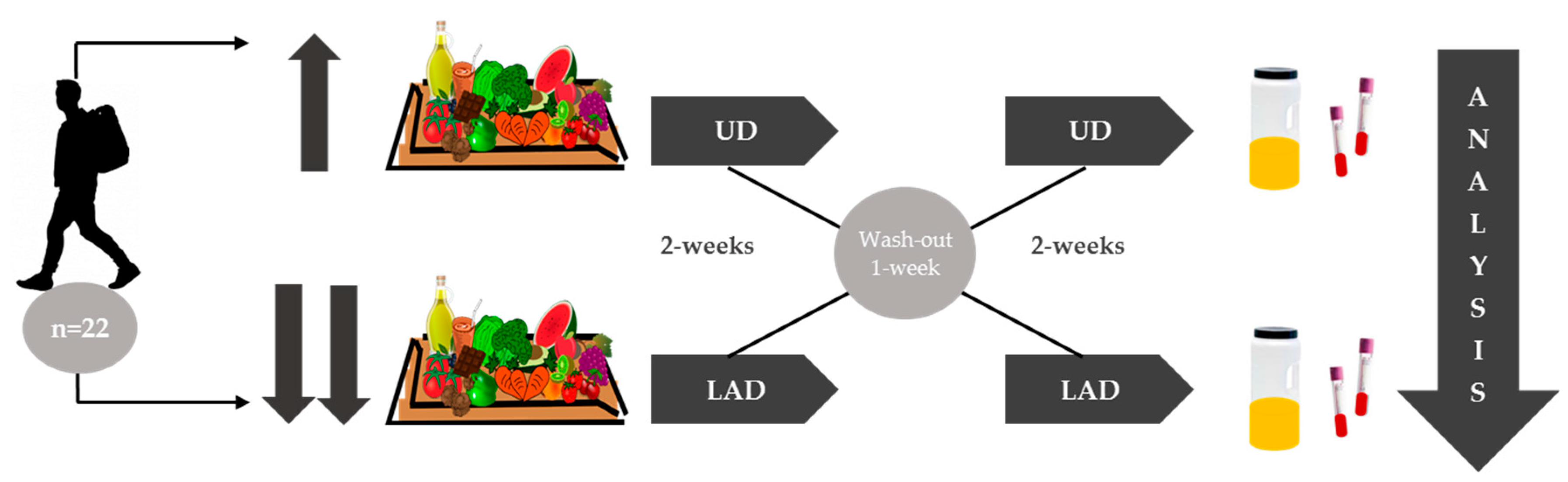
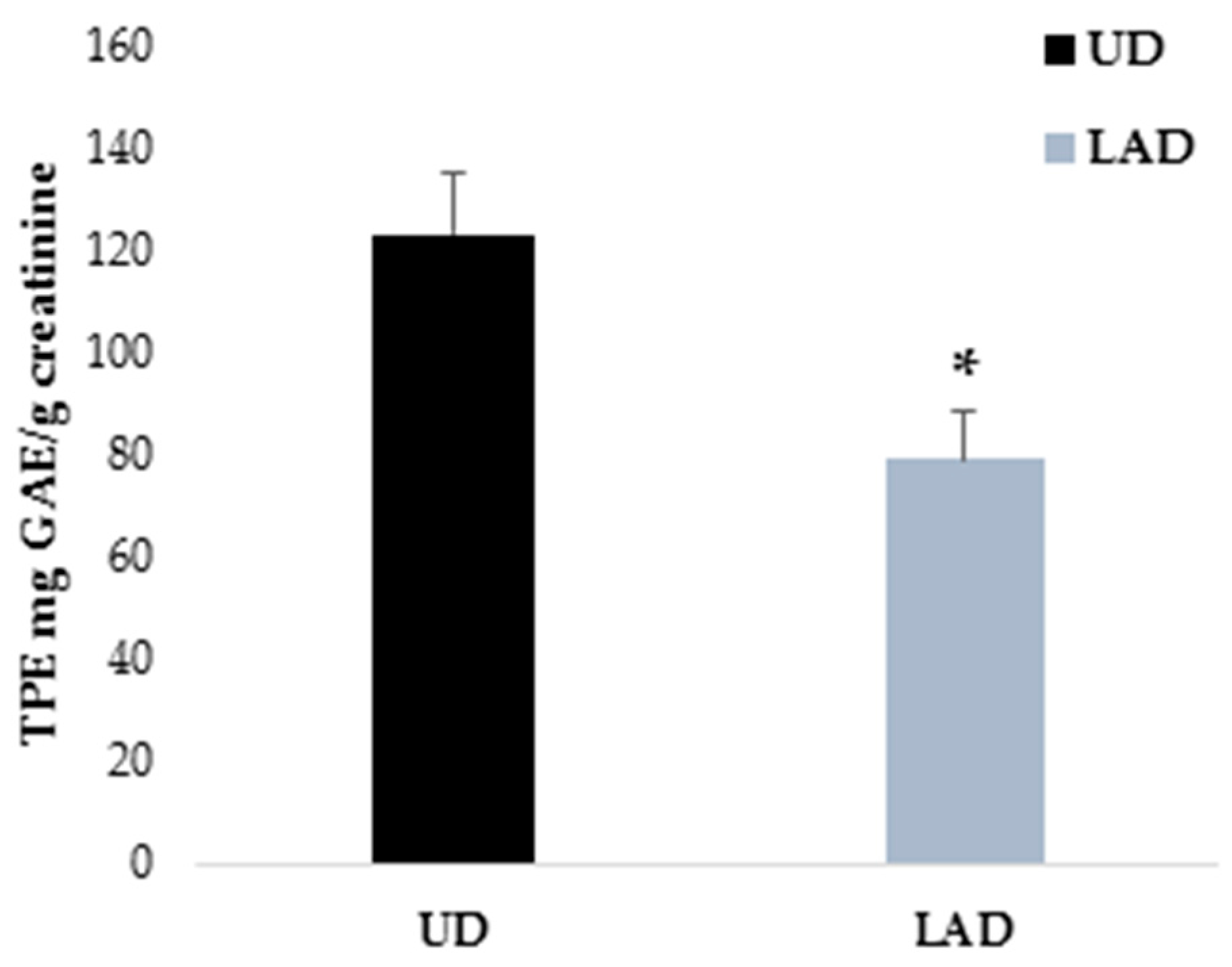
3.3. TPE in Urine after Each Dietary Intervention
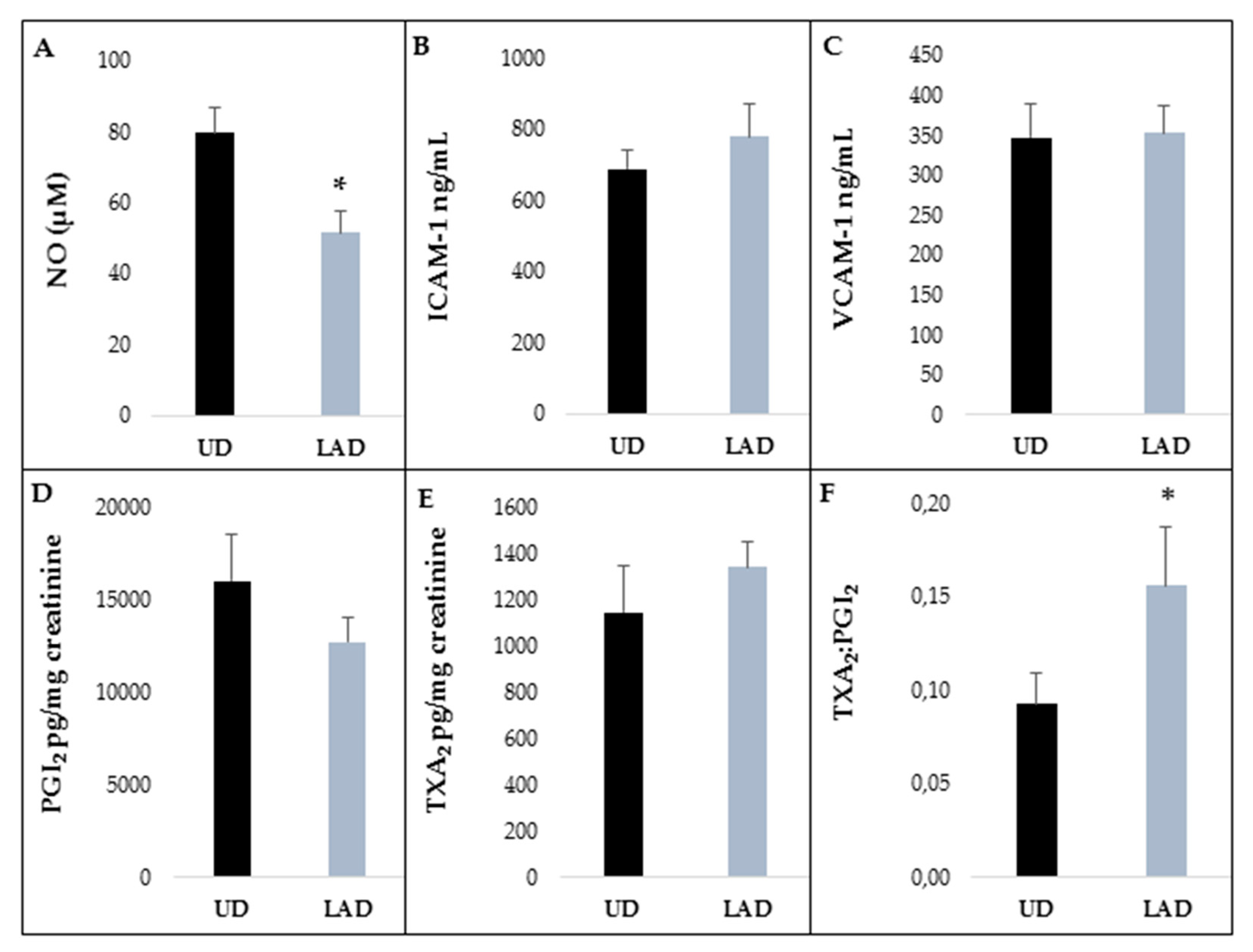
3.4. Inflammatory Molecules in Plasma and Urine
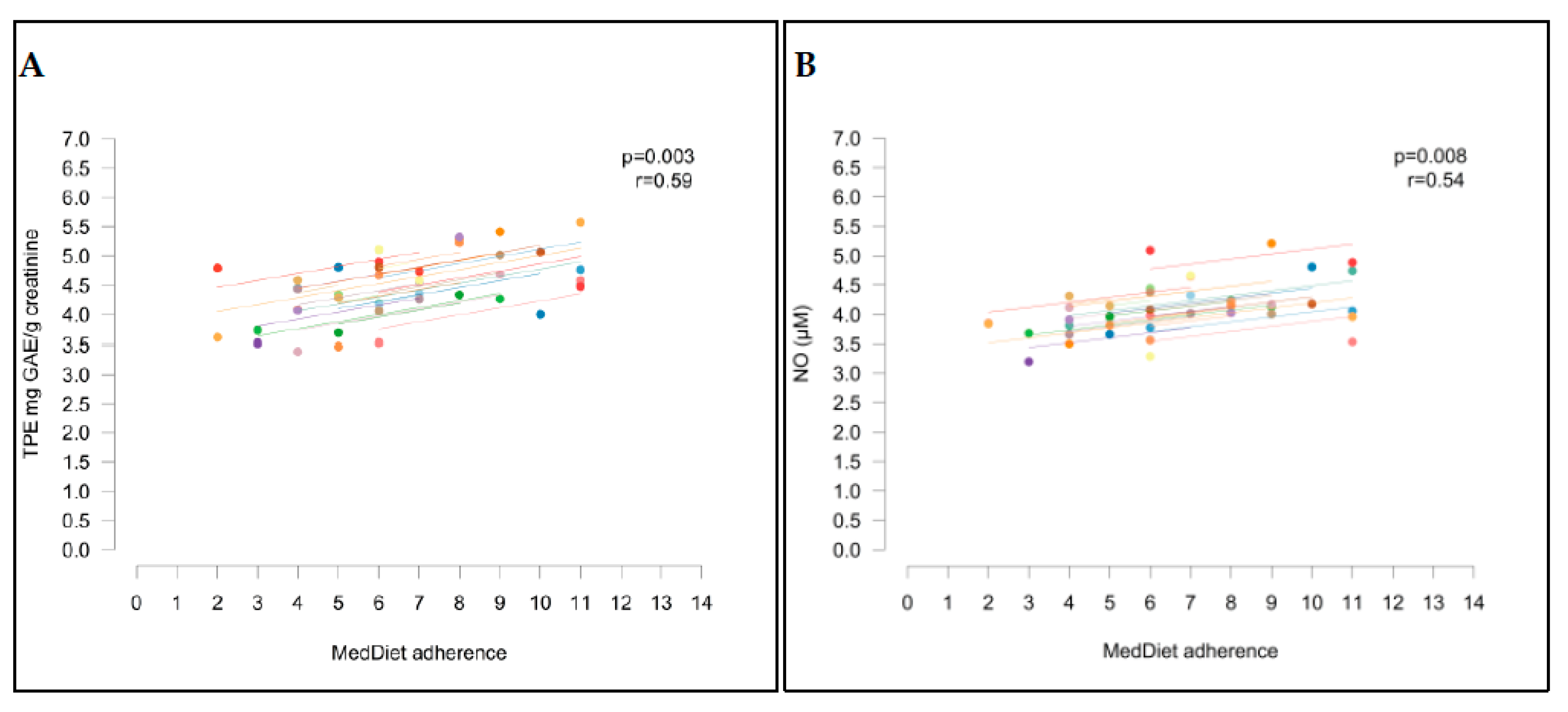
3.5. Correlation between Biomarkers and Mediterranean Diet Adherence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Del Rio, D.; Rodriguez-Mateos, A.; Spencer, J.P.E.; Tognolini, M.; Borges, G.; Crozier, A. Dietary (Poly)phenolics in human health: Structures, bioavailability, and evidence of protective effects against chronic diseases. Antioxid. Redox Signal. 2013, 18, 1818–1892. [Google Scholar] [CrossRef] [PubMed]
- Neveu, V.; Perez-Jiménez, J.; Vos, F.; Crespy, V.; du Chaffaut, L.; Mennen, L.; Knox, C.; Eisner, R.; Cruz, J.; Wishart, D.; et al. Phenol-Explorer: An online comprehensive database on polyphenol contents in foods. Database 2010, 2010, bap024. [Google Scholar] [CrossRef] [PubMed]
- Murillo, A.G.; Fernandez, M.L. The relevance of dietary polyphenols in cardiovascular protection. Curr. Pharm. Des. 2017, 23, 2444–2452. [Google Scholar] [CrossRef] [PubMed]
- Tressera-Rimbau, A.; Arranz, S.; Eder, M.; Vallverdú-Queralt, A. Dietary polyphenols in the prevention of stroke. Oxid. Med. Cell. Longev. 2017, 2017, 7467962. [Google Scholar] [CrossRef] [PubMed]
- Williamson, G. The role of polyphenols in modern nutrition. Nutr. Bull. 2017, 42, 226–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medina-Remón, A.; Casas, R.; Tressserra-Rimbau, A.; Ros, E.; Martínez-González, M.A.; Fitó, M.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventos, R.M.; Estruch, R.; et al. Polyphenol intake from a Mediterranean diet decreases inflammatory biomarkers related to atherosclerosis: A substudy of the PREDIMED trial. Br. J. Clin. Pharmacol. 2017, 83, 114–128. [Google Scholar] [CrossRef] [PubMed]
- Croft, K.D. Dietary polyphenols: Antioxidants or not? Arch. Biochem. Biophys. 2016, 595, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Medina-Remón, A.; Tresserra-Rimbau, A.; Pons, A.; Tur, J.A.; Martorell, M.; Ros, E.; Buil-Cosiales, P.; Sacanella, E.; Covas, M.I.; Corella, D.; et al. Effects of total dietary polyphenols on plasma nitric oxide and blood pressure in a high cardiovascular risk cohort. The PREDIMED randomized trial. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 60–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forte, M.; Conti, V.; Damato, A.; Ambrosio, M.; Puca, A.A.; Sciarretta, S.; Frati, G.; Vecchione, C.; Carrizzo, A. Targeting nitric oxide with natural derived compounds as a therapeutic strategy in vascular diseases. Oxid. Med. Cell. Longev. 2016, 2016, 7364138. [Google Scholar] [CrossRef] [PubMed]
- Oak, M.-H.; Auger, C.; Belcastro, E.; Park, S.-H.; Lee, H.-H.; Schini-Kerth, V.B. Potential mechanisms underlying cardiovascular protection by polyphenols: Role of the endothelium. Free Radic. Biol. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Yamagata, K.; Tagami, M.; Yamori, Y. Dietary polyphenols regulate endothelial function and prevent cardiovascular disease. Nutrition 2015, 31, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Vanhoutte, P.M.; Shimokawa, H.; Feletou, M.; Tang, E.H.C. Endothelial dysfunction and vascular disease-a 30th anniversary update. Acta Physiol. 2017, 219, 22–96. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Vanhoutte, P.M.; Leung, S.W.S. Vascular nitric oxide: Beyond eNOS. J. Pharmacol. Sci. 2015, 129, 83–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vita, J.A.; Keaney, J.F. Endothelial function: A barometer for cardiovascular risk? Circulation 2002, 106, 640–642. [Google Scholar] [CrossRef] [PubMed]
- Herman, A.G.; Moncada, S. Therapeutic potential of nitric oxide donors in the prevention and treatment of atherosclerosis. Eur. Heart J. 2005, 26, 1945–1955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tachibana, H.; Koga, K.; Fujimura, Y.; Yamada, K. A receptor for green tea polyphenol EGCG. Nat. Struct. Mol. Biol. 2004, 11, 380–381. [Google Scholar] [CrossRef] [PubMed]
- Schramm, D.D.; Collins, H.E.; German, J.B. Flavonoid transport by mammalian endothelial cells. J. Nutr. Biochem. 1999, 10, 193–197. [Google Scholar] [CrossRef]
- Jin, X.; Yi, L.; Chen, M.; Chen, C.; Chang, H.; Zhang, T.; Wang, L.; Zhu, J.; Zhang, Q.; Mi, M. Correction: Delphinidin-3-Glucoside protects against oxidized low-density lipoprotein-induced mitochondrial dysfunction in vascular endothelial cells via the sodium-dependent glucose transporter SGLT1. PLoS ONE 2014, 9. [Google Scholar] [CrossRef]
- Kim, J.H.; Auger, C.; Kurita, I.; Anselm, E.; Rivoarilala, L.O.; Lee, H.J.; Lee, K.W.; Schini-Kerth, V.B. Aronia melanocarpa juice, a rich source of polyphenols, induces endothelium-dependent relaxations in porcine coronary arteries via the redox-sensitive activation of endothelial nitric oxide synthase. Nitric Oxide 2013, 35, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Formoso, G.; Li, Y.; Potenza, M.A.; Marasciulo, F.L.; Montagnani, M.; Quon, M.J. Epigallocatechin Gallate, a Green Tea Polyphenol, Mediates NO-dependent Vasodilation Using Signaling Pathways in Vascular Endothelium Requiring Reactive Oxygen Species and Fyn. J. Biol. Chem. 2007, 282, 13736–13745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barona, J.; Aristizabal, J.C.; Blesso, C.N.; Volek, J.S.; Fernandez, M.L. Grape polyphenols reduce blood pressure and increase flow-mediated vasodilation in men with metabolic syndrome. J. Nutr. 2012, 142, 1626–1632. [Google Scholar] [CrossRef] [PubMed]
- Kawano, H.; Motoyama, T.; Kugiyama, K.; Hirashima, O.; Ohgushi, M.; Yoshimura, M.; Ogawa, H.; Okumura, K.; Yasue, H. Menstrual cyclic variation of endothelium-dependent vasodilation of the brachial artery: Possible role of estrogen and nitric oxide. Proc. Assoc. Am. Physicians 1996, 108, 473–480. [Google Scholar] [PubMed]
- Whitcomb, B.W.; Mumford, S.L.; Perkins, N.J.; Wactawski-Wende, J.; Bertone-Johnson, E.R.; Lynch, K.E.; Schisterman, E.F. Urinary cytokine and chemokine profiles across the menstrual cycle in healthy reproductive-aged women. Fertil. Steril. 2014, 101, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A short screener is valid for assessing mediterranean diet adherence among older spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Elosua, R.; Marrugat, J.; Molina, L.; Pons, S.; Pujol, E. Validation of the minnesota leisure time physical activity questionnaire in spanish men. The MARATHOM Investigators. Am. J. Epidemiol. 1994, 139, 1197–1209. [Google Scholar] [CrossRef] [PubMed]
- Medina-Remón, A.; Barrionuevo-González, A.; Zamora-Ros, R.; Andres-Lacueva, C.; Estruch, R.; Martínez-González, M.-Á.; Diez-Espino, J.; Lamuela-Raventos, R.M. Rapid Folin–Ciocalteu method using microtiter 96-well plate cartridges for solid phase extraction to assess urinary total phenolic compounds, as a biomarker of total polyphenols intake. Anal. Chim. Acta 2009, 634, 54–60. [Google Scholar] [CrossRef] [PubMed]
- rmcorr: Repeated Measures Correlation. Available online: https://cran.r-project.org/web/packages/rmcorr/index.html (accessed on 13 November 2018).
- The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 13 November 2018).
- Schroeter, H.; Heiss, C.; Balzer, J.; Kleinbongard, P.; Keen, C.L.; Hollenberg, N.K.; Sies, H.; Kwik-Uribe, C.; Schmitz, H.H.; Kelm, M. (−)-Epicatechin mediates beneficial effects of flavanol-rich cocoa on vascular function in humans. Proc. Natl. Acad. Sci. USA 2006, 103, 1024–1029. [Google Scholar] [CrossRef] [PubMed]
- Storniolo, C.E.; Casillas, R.; Bulló, M.; Castañer, O.; Ros, E.; Sáez, G.T.; Toledo, E.; Estruch, R.; Ruiz-Gutiérrez, V.; Fitó, M.; et al. A Mediterranean diet supplemented with extra virgin olive oil or nuts improves endothelial markers involved in blood pressure control in hypertensive women. Eur. J. Nutr. 2017, 56, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Sanguigni, V.; Manco, M.; Sorge, R.; Gnessi, L.; Francomano, D. Natural antioxidant ice cream acutely reduces oxidative stress and improves vascular function and physical performance in healthy individuals. Nutrition 2017, 33, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Hollands, W.J.; Hart, D.J.; Dainty, J.R.; Hasselwander, O.; Tiihonen, K.; Wood, R.; Kroon, P.A. Bioavailability of epicatechin and effects on nitric oxide metabolites of an apple flavanol-rich extract supplemented beverage compared to a whole apple puree: A randomized, placebo-controlled, crossover trial. Mol. Nutr. Food Res. 2013, 57, 1209–1217. [Google Scholar] [CrossRef] [PubMed]
- Hall, W.L.; Formanuik, N.L.; Harnpanich, D.; Cheung, M.; Talbot, D.; Chowienczyk, P.J.; Sanders, T.A.B. A Meal Enriched with Soy Isoflavones Increases Nitric Oxide-Mediated Vasodilation in Healthy Postmenopausal Women. J. Nutr. 2008, 138, 1288–1292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ochiai, R.; Sugiura, Y.; Otsuka, K.; Katsuragi, Y.; Hashiguchi, T. Coffee bean polyphenols ameliorate postprandial endothelial dysfunction in healthy male adults. Int. J. Food Sci. Nutr. 2015, 66, 350–354. [Google Scholar] [CrossRef] [PubMed]
- Taubert, D.; Roesen, R.; Lehmann, C.; Jung, N.; Schömig, E. Effects of low habitual cocoa intake on blood pressure and bioactive nitric oxide. JAMA 2007, 298, 49. [Google Scholar] [CrossRef] [PubMed]
- Chiva-Blanch, G.; Urpi-Sarda, M.; Ros, E.; Arranz, S.; Valderas-Martinez, P.; Casas, R.; Sacanella, E.; Llorach, R.; Lamuela-Raventos, R.M.; Andres-Lacueva, C.; et al. Dealcoholized red wine decreases systolic and diastolic blood pressure and increases plasma nitric oxide: Short communication. Circ. Res. 2012, 111, 1065–1068. [Google Scholar] [CrossRef] [PubMed]
- Boon, E.A.J.; Croft, K.D.; Shinde, S.; Hodgson, J.M.; Ward, N.C. The acute effect of coffee on endothelial function and glucose metabolism following a glucose load in healthy human volunteers. Food Funct. 2017, 8, 3366–3373. [Google Scholar] [CrossRef] [PubMed]
- Riso, P.; Klimis-Zacas, D.; Del Bo’, C.; Martini, D.; Campolo, J.; Vendrame, S.; Møller, P.; Loft, S.; De Maria, R.; Porrini, M. Effect of a wild blueberry (Vaccinium angustifolium) drink intervention on markers of oxidative stress, inflammation and endothelial function in humans with cardiovascular risk factors. Eur. J. Nutr. 2013, 52, 949–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asgary, S.; Sahebkar, A.; Afshani, M.R.; Keshvari, M.; Haghjooyjavanmard, S.; Rafieian-Kopaei, M. Clinical evaluation of blood pressure lowering, endothelial function improving, hypolipidemic and anti-inflammatory effects of pomegranate juice in hypertensive subjects. Phyther. Res. 2014, 28, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Casas, R.; Sacanella, E.; Urpí-Sardà, M.; Chiva-Blanch, G.; Ros, E.; Martínez-González, M.-A.; Covas, M.-I.; Rosa Ma Lamuela-Raventos, R.M.; Salas-Salvadó, J.; Fiol, M.; et al. The effects of the mediterranean diet on biomarkers of vascular wall inflammation and plaque vulnerability in subjects with high risk for cardiovascular disease. A randomized trial. PLoS ONE 2014, 9, e100084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coimbra, S.R.; Lage, S.H.; Brandizzi, L.; Yoshida, V.; da Luz, P.L. The action of red wine and purple grape juice on vascular reactivity is independent of plasma lipids in hypercholesterolemic patients. Brazilian J. Med. Biol. Res. 2005, 38, 1339–1347. [Google Scholar] [CrossRef] [Green Version]
- Park, E.; Edirisinghe, I.; Choy, Y.Y.; Waterhouse, A.; Burton-Freeman, B. Effects of grape seed extract beverage on blood pressure and metabolic indices in individuals with pre-hypertension: A randomised, double-blinded, two-arm, parallel, placebo-controlled trial. Br. J. Nutr. 2016, 115, 226–238. [Google Scholar] [CrossRef] [PubMed]
- Dohadwala, M.M.; Holbrook, M.; Hamburg, N.M.; Shenouda, S.M.; Chung, W.B.; Titas, M.; Kluge, M.A.; Wang, N.; Palmisano, J.; Milbury, P.E.; et al. Effects of cranberry juice consumption on vascular function in patients with coronary artery disease. Am. J. Clin. Nutr. 2011, 93, 934–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yahfoufi, N.; Alsadi, N.; Jambi, M.; Matar, C.; Yahfoufi, N.; Alsadi, N.; Jambi, M.; Matar, C. The immunomodulatory and anti-inflammatory role of polyphenols. Nutrients 2018, 10, 1618. [Google Scholar] [CrossRef] [PubMed]
- Pignatelli, P.; Pastori, D.; Farcomeni, A.; Nocella, C.; Bartimoccia, S.; Vicario, T.; Bucci, T.; Carnevale, R.; Violi, F. Mediterranean diet reduces thromboxane A2 production in atrial fibrillation patients. Clin. Nutr. 2015, 34, 899–903. [Google Scholar] [CrossRef] [PubMed]
- Bogani, P.; Galli, C.; Villa, M.; Visioli, F. Postprandial anti-inflammatory and antioxidant effects of extra virgin olive oil. Atherosclerosis 2007, 190, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Carnevale, R.; Lofredo, L.; Pignatelli, P.; Nocella, C.; Bartimoccia, S.; Di Santo, S.; Martino, F.; Catasca, E.; Perri, L.; Violi, F. Dark chocolate inhibits platelet isoprostanes via NOX2 down-regulation in smokers. J. Thromb. Haemost. 2012, 10, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.; Vinson, J.A.; Etherton, T.D.; Proch, J.; Lazarus, S.A.; Kris-Etherton, P.M. Effects of cocoa powder and dark chocolate on LDL oxidative susceptibility and prostaglandin concentrations in humans. Am. J. Clin. Nutr. 2001, 74, 596–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Flores, L.A.; Medina, S.; Gómez, C.; Wheelock, C.E.; Cejuela, R.; Martínez-Sanz, J.M.; Oger, C.; Galano, J.-M.; Durand, T.; Hernández-Sáez, Á.; et al. Aronia-citrus juice (polyphenol-rich juice) intake and elite triathlon training: A lipidomic approach using representative oxylipins in urine. Food Funct. 2018, 9, 463–475. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| UD | LAD | p | Adjusted p a | |
|---|---|---|---|---|
| Baseline characteristics | ||||
| Age (years) | 24 ± 1 | |||
| Physical activity (METS/day) | 743 ± 75 | |||
| Anthropometric measurements | ||||
| BMI (kg/m2) | 24.9 ± 0.79 | 24.8 ± 0.79 | 0.375 | 0.33 |
| WHR | 0.84 ± 0.01 | 0.84 ± 0.01 | 1 | 0.89 |
| Clinical measurements | ||||
| SBP (mmHg) | 123 ± 2 | 122 ± 2 | 0.864 | 0.90 |
| DBP (mmHg) | 76 ± 2 | 76 ± 2 | 0.893 | 0.995 |
| HR (bpm) | 66 ± 2 | 63 ± 2 | 0.109 | 0.198 |
| CRP (mg/dL) | 0.10 ± 0.02 | 0.09 ± 0.01 | 0.893 | 0.925 |
| Total cholesterol (mmoles/L) | 3.84 ± 0.12 | 3.80 ± 0.12 | 0.547 | 0.551 |
| HDL (mmoles/L) | 1.37 ± 0.06 | 1.36 ± 0.05 | 0.865 | 0.832 |
| LDL (mmoles/L) | 2.04 ± 0.11 | 1.97 ± 0.11 | 0.250 | 0.306 |
| Triglycerides (mmoles/L) | 0.94 ± 0.08 | 1.04 ± 0.12 | 0.470 | 0.525 |
| Urea (mmoles/L) | 5.56 ± 0.30 | 5.94 ± 0.25 | 0.211 | 0.365 |
| Creatinine (µmoles/L) | 76 ± 1.51 | 76.3 ± 1.60 | 0.510 | 0.752 |
| Uric acid (µmoles/L) | 319 ± 10.95 | 332 ± 10.51 | 0.138 | 0.136 |
| Total proteins (g/L) | 73.1 ± 0.57 | 73.9 ± 0.54 | 0.272 | 0.324 |
| Albumin (g/L) | 46.8 ± 0.50 | 46.6 ± 0.41 | 0.655 | 0.608 |
| UD | LAD | p | Adjusted p a | |
|---|---|---|---|---|
| Nutrients | ||||
| Energy (kcal/day) | 2393 ± 130 | 2194 ± 127 | 0.083 | 0.033 * |
| Carbohydrates (g/day) | 256 ± 15 | 245 ± 14 | 0.445 | 0.498 |
| Fat (g/day) | 106 ± 9 | 83 ± 7 | 0.005 * | 0.001 * |
| Protein (g/day) | 100 ± 6 | 109 ± 7 | 0.256 | 0.473 |
| Cholesterol (mg/day) | 301 ± 30 | 241 ± 21 | 0.046 * | 0.025 * |
| Fiber (g/day) | 30 ± 2 | 16 ± 1 | <0.001 * | <0.001 * |
| Ca (mg/day) | 869±49 | 936 ± 91 | 0.452 | 0.816 |
| P (mg/day) | 1599±82 | 1612 ± 97 | 0.897 | 0.711 |
| Mg (mg/day) | 436±25 | 314 ± 30 | <0.001 * | <0.001 * |
| Na (mg/day) | 2495±273 | 2945 ± 280 | 0.065 | 0.107 |
| K (mg/day) | 4237±180 | 2950 ± 325 | <0.001 * | <0.001 * |
| Fe (mg/day) | 17±0.98 | 12 ± 0.99 | 0.001 * | 0.002 * |
| Zn (mg/day) | 11±0.72 | 10 ± 0.60 | 0.217 | 0.057 |
| Vit. A (mcg r.e./day) | 1460±232 | 242 ± 45 | <0.001 * | <0.001 * |
| Vit E (mg t.e./day) | 15±1.19 | 8 ± 0.70 | <0.001 * | <0.001 * |
| Vit. C (mg/day) | 255±25 | 39 ± 6 | <0.001 * | <0.001 * |
| Folate (mcg/day) | 511±34 | 243 ± 33 | <0.001 * | <0.001 * |
| Food | ||||
| Vegetable (g/day) | 402 ± 38 | 120 ± 25 | <0.001 * | <0.001 * |
| Fruit (g/day) | 368 ± 53 | 48 ± 16 | <0.001 * | <0.001 * |
| Nuts and seeds (g/day) | 15 ± 5 | 0.2 ± 0.2 | <0.001 * | <0.001 * |
| Virgin olive oil (g/day) | 33 ± 2 | 26 ± 2 | 0.009 * | 0.01 * |
| Pulses (g/day) | 19 ± 6 | 16 ± 6 | 0.210 | 0.295 |
| Cereals (g/day) | 202 ± 20 | 275 ± 17 | 0.001 * | 0.001 * |
| Cocoa (g/day) | 13 ± 3 | 0.7 ± 0.6 | <0.001 * | <0.001 * |
| Coffee (g/day) | 63 ± 24 | 23 ± 9 | 0.186 | 0.162 |
| Tea (g/day) | 112 ± 29 | 0 | <0.001 * | <0.001 * |
| White meat (g/day) | 70 ± 14 | 79 ± 14 | 0.353 | 0.312 |
| Fish (g/day) | 61 ± 12 | 65 ± 17 | 0.768 | 0.885 |
| Wine (g/day) | 5 ± 3 | 0 | 0.163 | 0.107 |
| Beer (g/day) | 16 ± 8 | 13 ± 10 | 0.201 | 0.215 |
| Mediterranean diet score | ||||
| MedDiet score † | 8.5 ± 0.4 | 4.7 ± 0.3 | <0.001 * | <0.001 * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hurtado-Barroso, S.; Quifer-Rada, P.; Rinaldi de Alvarenga, J.F.; Pérez-Fernández, S.; Tresserra-Rimbau, A.; Lamuela-Raventos, R.M. Changing to a Low-Polyphenol Diet Alters Vascular Biomarkers in Healthy Men after Only Two Weeks. Nutrients 2018, 10, 1766. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111766
Hurtado-Barroso S, Quifer-Rada P, Rinaldi de Alvarenga JF, Pérez-Fernández S, Tresserra-Rimbau A, Lamuela-Raventos RM. Changing to a Low-Polyphenol Diet Alters Vascular Biomarkers in Healthy Men after Only Two Weeks. Nutrients. 2018; 10(11):1766. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111766
Chicago/Turabian StyleHurtado-Barroso, Sara, Paola Quifer-Rada, José Fernando Rinaldi de Alvarenga, Silvia Pérez-Fernández, Anna Tresserra-Rimbau, and Rosa M. Lamuela-Raventos. 2018. "Changing to a Low-Polyphenol Diet Alters Vascular Biomarkers in Healthy Men after Only Two Weeks" Nutrients 10, no. 11: 1766. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111766