Hypovitaminosis D: A Disease Marker in Hospitalized Very Old Persons at Risk of Malnutrition

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Sample Characteristics
3.2. Sample Characteristics Stratified by Vitamin D Status
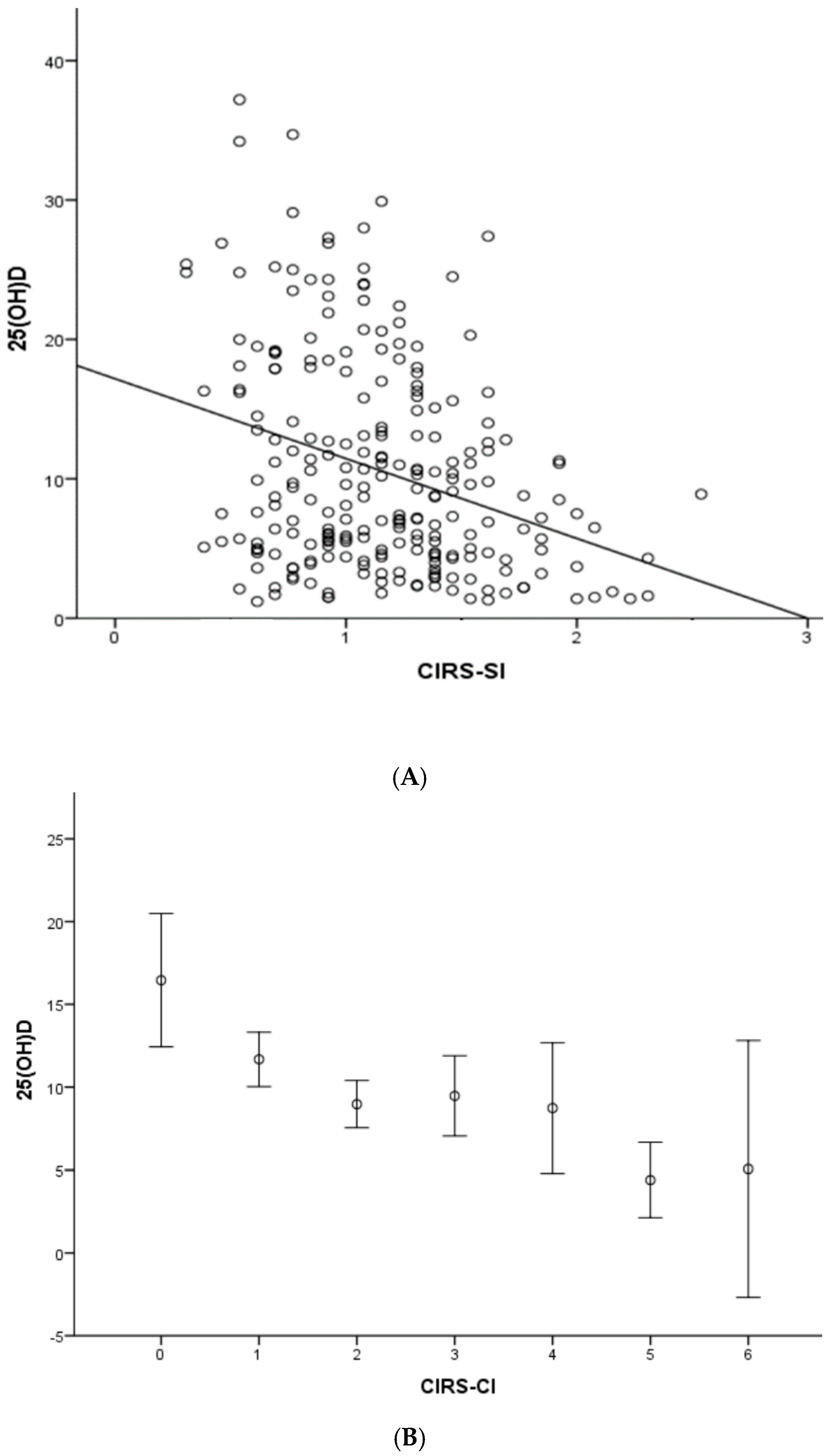
3.3. Vitamin D, Comorbidities Burden, CRP, and Length of Hospital Stay
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Maggio, D.; Cherubini, A.; Lauretani, F.; Russo, R.C.; Bartali, B.; Pierandrei, M.; Ruggiero, C.; Macchiarulo, M.C.; Giorgino, R.; Minisola, S.; et al. 25(OH)D Serum levels decline with age earlier in women than in men and less efficiently prevent compensatory hyperparathyroidism in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 1414–1419. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, M.S.; Grimnes, G.; Joakimsen, R.M.; Figenschau, Y.; Jorde, R. Low serum 25-hydroxyvitamin D levels are associated with increased all-cause mortality risk in a general population: The Tromso study. Eur. J. Endocrinol. 2010, 162, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Melamed, M.L.; Michos, E.D.; Post, W.; Astor, B. 25-hydroxyvitaminD levels and the risk of mortality in the general population. Arch. Intern. Med. 2008, 168, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Autier, P.; Gandini, S. Vitamin D supplementation and total mortality: A meta-analysis of randomized controlled trials. Arch. Intern. Med. 2007, 167, 1730–1737. [Google Scholar] [CrossRef]
- Beauchet, O.; Helard, L.; Montero-Odasso, M.; De Decker, L.; Berrut, G.; Annweiler, C. Hypovitaminosis D in geriatric inpatients: A marker of severity of chronic diseases. Aging Clin. Exp. Res. 2012, 24, 188–192. [Google Scholar]
- Sutra del Galy, A.; Bertrand, M.; Bigot, T.; Abraham, P.; Thomlinson, R.; Paccalin, M.; Beauchet, O.; Annweiler, C. Vitamin D insufficiency and acute care in geriatric inpatients. J. Am. Geriatr. Soc. 2009, 57, 1721–1723. [Google Scholar] [CrossRef] [PubMed]
- Annweiler, C.; Pochic, S.; Fantino, B.; Legrand, E.; Bataille, R.; Montero-Odasso, M.; Beauchet, O. Serum vitamin D concentration and short-term mortality among geriatric inpatients in acute care settings. Adv. Ther. 2010, 27, 245–249. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.P.; Wan, Y.D.; Sun, T.W.; Kan, Q.C.; Wang, L.X. Association between vitamin D deficiency and mortality in critically ill adult patients: A meta-analysis of cohort studies. Crit. Care 2014, 18, 684. [Google Scholar] [CrossRef]
- De Haan, K.; Groeneveld, A.B.; de Geus, H.R.; Egal, M.; Struijs, A. Vitamin D deficiency as a risk factor for infection, sepsis and mortality in the critically ill: Systematic review and meta-analysis. Crit. Care 2014, 18, 660. [Google Scholar] [CrossRef] [PubMed]
- Blay, B.; Thomas, S.; Coffey, R.; Jones, L.; Murphy, C.V. Low Vitamin D Level on Admission for Burn Injury Is Associated with Increased Length of Stay. J. Burn Care Res. 2017, 38, e8–e13. [Google Scholar] [CrossRef] [PubMed]
- Anwar, E.; Hamdy, G.; Taher, E.; Fawzy, E.; Abdulattif, S.; Attia, M.H. Burden and Outcome of Vitamin D Deficiency Among Critically Ill Patients: A Prospective Study. Nutr. Clin. Pract. 2017, 3, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Hélard, L.; Mateus-Hamdan, L.; Beauchet, O.; Annweiler, C. Hypovitaminosis D in Geriatric Acute Care Unit: A Biomarker of Longer Length of Stay. Hindawi Publ. Corp. Dis. Mark. 2013, 35, 525–529. [Google Scholar] [CrossRef]
- Autier, P.; Boniol, M.; Pizot, C.; Mullie, P. Vitamin D status and ill health: A systematic review. Lancet Diabetes Endocrinol. 2014, 2, 76–89. [Google Scholar] [CrossRef]
- Amrein, K.; Schnedl, C.; Holl, A.; Riedl, R.; Christopher, K.B.; Pachler, C.; Urbanic Purkart, T.; Waltensdorfer, A.; Münch, A.; Warnkross, H.; et al. Effect of high-dose vitamin D3 on hospital length of stay in critically ill patients with vitamin D deficiency: The VITdAL-ICU randomized clinical trial. JAMA 2014, 312, 1520–1530. [Google Scholar] [CrossRef] [PubMed]
- Schottker, B.; Saum, K.U.; Perna, L.; Ordóñez-Mena, J.M.; Holleczek, B.; Brenner, H. Is vitamin D deficiency a cause of increased morbidityand mortality at older age or simply an indicator of poor health. Eur. J. Epidemiol. 2014, 29, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Rossini, M.; Adami, S.; Bertoldo, F.; Diacinti, D.; Gatti, D.; Giannini, S.; Giusti, A.; Malavolta, N.; Minisola, S.; Osella, G.; et al. Guidelines for the diagnosis, preventionand management of osteoporosis. Reumatismo 2016, 68, 1–39. [Google Scholar] [CrossRef]
- Folstein, M.; Folstein, S.; McHugh, P.R. Mini Mental State: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged. The index of ADL: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Graf, C. The Lawton instrumental activities of daily living (IADL) scale. Medsurg Nurs. 2008, 17, 343–344. [Google Scholar] [PubMed]
- Guigoz, Y.; Vellas, B. Mini Nutritional Asssessment, a practical assessment tool for grading the nutritional state of elderly patients. Facts Res. Gerontol. 1994, 2, 15–59. [Google Scholar]
- Miller, M.D.; Paradis, C.F.; Houck, P.R.; Mazumdar, S.; Stack, J.A.; Rifai, A.H.; Mulsant, B.; Reynolds, C.F. Rating chronic medical illness burden in geropsychiatric practice and research: Application of the Cumulative Illness Rating Scale. Psychiatry Res. 1992, 41, 237–248. [Google Scholar] [CrossRef]
- Kiebzak, G.M.; Moore, N.L.; Margolis, S.; Hollis, B.; Kevorkian, C.G. Vitamin D status of patients admitted to a hospital rehabilitation unit: Relationship to function and progress. Am. J. Phys. Med. Rehabil. 2007, 86, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Quraishi, S.A.; Bittner, E.A.; Blum, L.; Hutter, M.M.; Camargo, C.A. Association between preoperative 25-hydroxyvitamin D level and hospital-acquired infections following roux-en-Y gastric bypass surgery. JAMA Surg. 2014, 149, 112–118. [Google Scholar] [CrossRef]
- Lee, P.; Eisman, J.A.; Center, J.R. Vitamin D deficiency in critically ill patients. N. Engl. J. Med. 2009, 360, 1912–1914. [Google Scholar] [CrossRef] [PubMed]
- Schwalfenberg, G.K. A review of the critical role of vitamin D in the functioning of the immune system and the clinical implications of vitamin D deficiency. Mol. Nutr. Food Res. 2011, 55, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Maggio, M.; de Vita, F.; Lauretani, F.; Bandinelli, S.; Semba, R.D.; Bartali, B.; Cherubini, A.; Cappola, A.R.; Ceda, G.P.; Ferrucci, L. Relationship between Carotenoids, Retinol, and Estradiol Levels in Older Women. Nutrients 2015, 7, 6506–6519. [Google Scholar] [CrossRef] [Green Version]
- Jafarnejad, S.; Boccardi, V.; Hosseni, B.; Taghizadeh, M.; Hamedifard, Z. A Meta-analysis of Randomized Control Trials: The Impact of Vitamin C Supplementation on Serum CRP and serum hs-CRP Concentrations. Curr. Pharm. Des. 2018, 24, 3520–3528. [Google Scholar] [CrossRef]
- Beauchet, O.; Launay, C.P.; Maunoury, F.; de Decker, L.; Fantino, B.; Annweiler, C. Association between vitamin D deficiency and long hospital stay in geriatric acute care unit: Results from a pilot cohort study. Aging Clin. Exp. Res. 2013, 25, 107–109. [Google Scholar] [CrossRef]
- Beauchet, O.; Launay, C.; de Decker, L.; Fantino, B.; Kabeshova, A.; Annweiler, C. Who is at risk of long hospital stay among patients admitted to geriatric acute care unit? Results fr.om a prospective cohort study. J. Nutr. Health Aging 2013, 17, 695–699. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total Sample N = 237 | Men N = 60 | Women N = 177 | p | |
|---|---|---|---|---|
| Age, y | 86.5 ± 6.2 | 86.12 ± 6.45 | 87.18 ± 6.22 | 0.258 |
| Drugs, n | 6.51 ± 3.20 | 7.43 ± 3.08 | 6.19 ± 3.19 | 0.013 |
| CIRS-SI | 1.87 ± 1.33 | 2.15 ± 1.43 | 1.78 ± 1.28 | 0.062 |
| CIRS-CI | 1.18 ± 0.40 | 1.27 ± 0.41 | 1.16 ± 0.40 | 0.069 |
| MMSE adjusted | 22.8 ± 4.7 | 23.6 ± 4.5 | 22.8 ± 4.4 | 0.532 |
| MMSE ≤ 23 (n, %) | 31 (13.1) | 4 (6.6) | 27 (15.2) | 0.063 |
| BADL | 2.76 ± 2.16 | 2.82 ± 2.39 | 2.73 ± 2.09 | 0.793 |
| IADL | 2.14 ± 2.70 | 2.23 ± 2.60 | 2.10 ± 2.66 | 0.756 |
| MNA | 21.08 ± 3.71 | 21.36 ± 3.50 | 21.04 ± 3.76 | 0.660 |
| 25(OH)D (ng/mL) | 10.58 ± 7.68 | 9.53 ± 7.13 | 10.94 ± 7.83 | 0.218 |
| PTHi (pg/mL) | 112.9 ± 112.9 | 101.16 ± 85.38 | 116.00 ± 121.31 | 0.556 |
| Albumin | 3.26 ± 1.15 | 3.22 ± 1.01 | 3.28 ± 1.20 | 0.733 |
| Calcium, corrected (mg/dL) | 8.55 ± 2.47 | 8.68 ± 2.08 | 8.51 ± 2.59 | 0.651 |
| Phosphorus (mg/dL) | 2.70 ± 1.85 | 2.95 ± 1.91 | 2.61 ± 1.83 | 0.218 |
| Magnesium (mg/dL) | 1.20 ± 1.02 | 1.21 ± 1.03 | 1.19 ± 1.02 | 0.884 |
| CRP (mg/L) | 5.02 ± 6.07 | 6.15 ± 7.10 | 4.64 ± 5.66 | 0.120 |
| Clearance creatinine (BIS1) | 41.3 ± 19.5 | 42.23 ± 22.98 | 39.74 ± 18.00 | 0.027 |
| Length of hospital stay (days) | 12.33 ± 9.22 | 12.10 ± 9.28 | 10.01 ± 9.08 | 0.510 |
| Severe Deficiency (<10 ng/mL) | Deficiency (10–20 ng/mL) | Insufficiency (20–30 ng/mL) | Optimal Range (30–50 ng/mL) | p | |
|---|---|---|---|---|---|
| N (%) | 134 (56.6) | 71 (29.9) | 29(13.2) | 3(1.3) | |
| Age, y | 87.8 ± 6.5 | 85.6 ± 6.4 | 85.7 ± 4.1 | 85.3 ± 2.0 | 0.057 |
| Gender M/F, n | 34/100 | 21/50 | 4/25 | 1/2 | 0.420 |
| Gender M/F, % | 24.4/74.6 | 29.5/70.5 | 13.8/86.2 | 87/12 | 0.420 |
| Drugs, n | 6.21 ± 2.97 | 7.25 ± 3.33 | 6.31 ± 3.87 | 4.50 ± 0.70 | 0.148 |
| CIRS-SI | 1.27 ± 0.43 | 1.14 ± 0.34 | 0.97 ± 0.32 | 0.71 ± 0.07 | <0.0001 |
| CIRS-CI | 2.21 ± 1.42 | 1.56 ± 0.95 | 1.28 ± 1.25 | 0.0 ± 0.0 | <0.0001 |
| MMSE adjusted | 22.40 ± 5.20 | 23.57 ± 4.05 | 23.23 ± 3.08 | 25.75 ± 2.21 | 0.465 |
| BADL | 2.40 ± 2.10 | 3.19 ± 2.93 | 3.26 ± 2.14 | 3.00 ± 2.64 | 0.056 |
| IADL | 1.61 ± 2.35 | 2.90 ± 2.93 | 2.48 ± 2.68 | 3.33 ± 3.51 | 0.009 |
| MNA | 20.36 ± 3.65 | 22.73 ± 2.87 | 19.95 ± 4.54 | 23.67 ± 0.57 | 0.001 |
| PTHi (pg/mL) | 136.7 ± 125.3 | 95.5 ± 101.4 | 61.9 ± 39.1 | 34.0 ± 8.1 | 0.012 |
| Albumin (g/dL) | 3.19 ± 1.16 | 3.35 ± 1.16 | 3.32 ± 1.16 | 3.5 ± 0.36 | 0.757 |
| Calcium, corrected (mg/dL) | 8.45 ± 2.44 | 8.47 ± 2.74 | 9.13 ± 1.99 | 9.42 ± 0.25 | 0.525 |
| Phosphorus (mg/dL) | 2.53 ± 1.99 | 2.76 ± 1.64 | 3.22 ± 1.70 | 3.73 ± 0.92 | 0.226 |
| Magnesium (mg/dL) | 1.08 ± 1.04 | 1.30 ± 0.99 | 1.46 ± 0.94 | 1.36 ± 1.18 | 0.205 |
| CRP (mg/L) | 5.51 ± 6.18 | 4.30 ± 5.98 | 4.70 ± 5.97 | 2.20 ± 2.40 | 0.546 |
| Clearance creatinine (BIS1) | 41.29 ± 18.75 | 42.65 ± 21.82 | 40.23 ± 18.13 | 27.50 ± 5.21 | 0.594 |
| Length of hospital stay (days) | 11.83 ± 8.14 | 13.00 ± 10.87 | 13.06 ± 9.81 | 12.00 ± 9.84 | 0.816 |
| Season | Severe Deficiency (<10 ng/mL) | Deficiency (10–20 ng/mL) | Insufficiency (20–30 ng/mL) | Optimal Range (30–50 ng/mL) |
|---|---|---|---|---|
| Fall n (%) | 39 (56.5) | 18 (26.1) | 10(14.5) | 2(2.9) |
| Winter n (%) | 16 (44.4) | 13 (36.1) | 6(16.7) | 1(2.8) |
| Spring n (%) | 42 (65.6) | 15 (23.4) | 7(10.9) | 0(0) |
| Summer n (%) | 37 (54.4) | 25 (36.8) | 6(8.8) | 0(0) |
| Model 1 | B | p |
| Age | −0.097 | 0.292 |
| Gender | −1.083 | 0.363 |
| Season | −0.583 | 0.181 |
| Albumin | 0.446 | 0.317 |
| BADL | −0.047 | 0.900 |
| IADL | 0.034 | 0.926 |
| BIS1 | 0.083 | 0.793 |
| CIRS-SI | −6.322 | <0.0001 |
| Model 2 | B | p |
| Age | −0.103 | 0.266 |
| Gender | −1.386 | 0.242 |
| Season | −0.726 | 0.101 |
| Albumin | 0.335 | 0.452 |
| BADL | 0.031 | 0.934 |
| IADL | 0.178 | 0.573 |
| BIS1 | 0.000 | 0.995 |
| CIRS-CI | −1.854 | <0.0001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boccardi, V.; Lapenna, M.; Gaggi, L.; Garaffa, F.M.; Croce, M.F.; Baroni, M.; Ercolani, S.; Mecocci, P.; Ruggiero, C. Hypovitaminosis D: A Disease Marker in Hospitalized Very Old Persons at Risk of Malnutrition. Nutrients 2019, 11, 128. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11010128
Boccardi V, Lapenna M, Gaggi L, Garaffa FM, Croce MF, Baroni M, Ercolani S, Mecocci P, Ruggiero C. Hypovitaminosis D: A Disease Marker in Hospitalized Very Old Persons at Risk of Malnutrition. Nutrients. 2019; 11(1):128. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11010128
Chicago/Turabian StyleBoccardi, Virginia, Maria Lapenna, Lorenzo Gaggi, Francesco Maria Garaffa, Michele Francesco Croce, Marta Baroni, Sara Ercolani, Patrizia Mecocci, and Carmelinda Ruggiero. 2019. "Hypovitaminosis D: A Disease Marker in Hospitalized Very Old Persons at Risk of Malnutrition" Nutrients 11, no. 1: 128. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11010128