Efficacy and Safety of Lactobacillus Plantarum C29-Fermented Soybean (DW2009) in Individuals with Mild Cognitive Impairment: A 12-Week, Multi-Center, Randomized, Double-Blind, Placebo-Controlled Clinical Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Outcome Measures
2.3.1. Measurement of Cognitive Functions
2.3.2. Safety Measures
2.3.3. Measurement of Serum BDNF levels
2.3.4. Fecal Microbiota Analysis
2.4. Statistical Analysis
3. Results
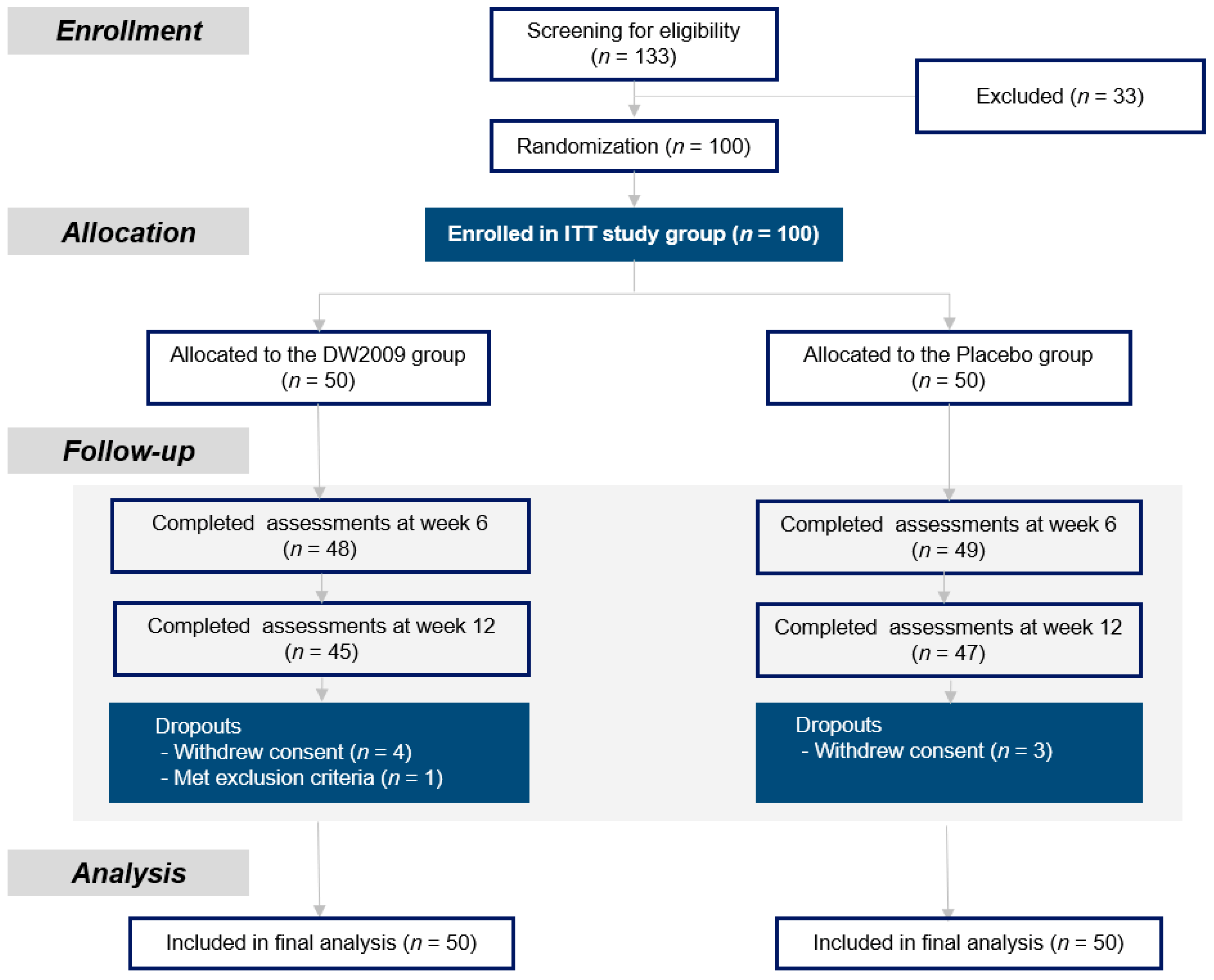
3.1. Participant Characteristics
3.2. Adherence to Treatment
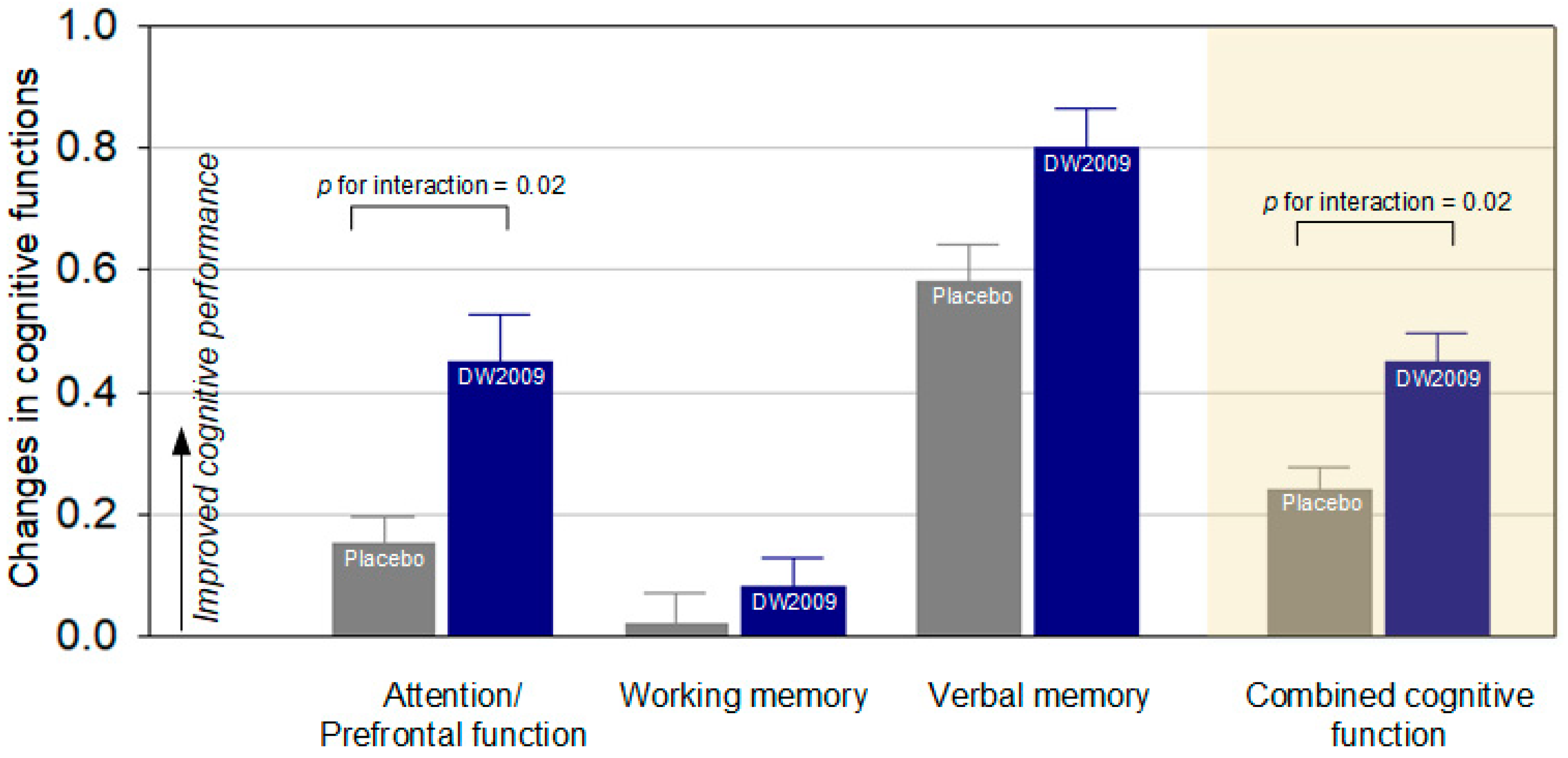
3.3. Primary Outcome Measure
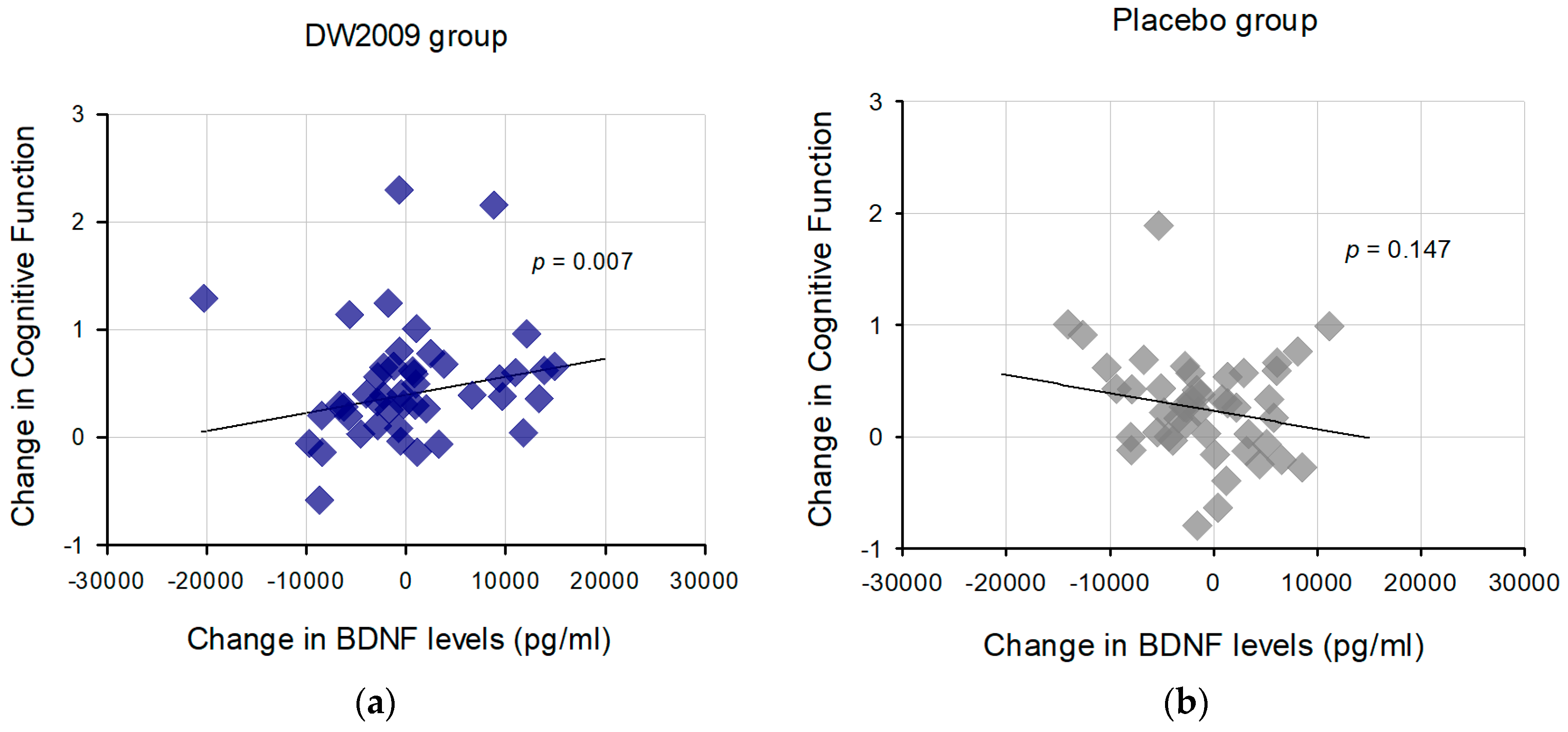
3.4. Associations between Changes in Serum BDNF Levels and Cognitive Performance
3.5. Change in Gut Microbiota Composition
3.6. Safety and Tolerability
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gauthier, S.; Reisberg, B.; Zaudig, M.; Petersen, R.C.; Ritchie, K.; Broich, K.; Belleville, S.; Brodaty, H.; Bennett, D.; Chertkow, H.; et al. Mild cognitive impairment. Lancet 2006, 367, 1262–1270. [Google Scholar] [CrossRef]
- Petersen, R.C. Clinical practice. Mild cognitive impairment. N. Engl. J. Med. 2011, 364, 2227–2234. [Google Scholar] [CrossRef] [PubMed]
- Panza, F.; D’Introno, A.; Colacicco, A.M.; Capurso, C.; Del Parigi, A.; Caselli, R.J.; Pilotto, A.; Argentieri, G.; Scapicchio, P.L.; Scafato, E.; et al. Current epidemiology of mild cognitive impairment and other predementia syndromes. Am. J. Geriatr. Psychiatry 2005, 13, 633–644. [Google Scholar] [CrossRef] [PubMed]
- Boyle, P.; Wilson, R.; Aggarwal, N.; Tang, Y.; Bennett, D. Mild cognitive impairment: Risk of Alzheimer disease and rate of cognitive decline. Neurology 2006, 67, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Akbari, E.; Asemi, Z.; Daneshvar Kakhaki, R.; Bahmani, F.; Kouchaki, E.; Tamtaji, O.R.; Hamidi, G.A.; Salami, M. Effect of probiotic supplementation on cognitive function and metabolic status in Alzheimer’s disease: A randomized, double-blind and controlled trial. Front. Aging Neurosci. 2016, 8, 1–8. [Google Scholar] [CrossRef]
- Jung, I.H.; Jung, M.A.; Kim, E.J.; Han, M.; Kim, D.H. Lactobacillus pentosus var. plantarum C29 protects scopolamine-induced memory deficit in mice. J. Appl. Microbiol. 2012, 113, 1498–1506. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.J.; Woo, J.Y.; Kim, K.A.; Han, M.; Kim, D.H. Lactobacillus pentosus var. plantarum C29 ameliorates age-dependent memory impairment in Fischer 344 rats. Lett. Appl. Microbiol. 2015, 60, 307–314. [Google Scholar] [CrossRef]
- Lee, H.J.; Jeong, J.J.; Han, M.J.; Kim, D.H. Lactobacillus plantarum C29 Alleviates TNBS-Induced Memory Impairment in Mice. J. Microbiol. Biotechnol. 2018, 28, 175–179. [Google Scholar] [CrossRef]
- File, S.E.; Jarrett, N.; Fluck, E.; Duffy, R.; Casey, K.; Wiseman, H. Eating soya improves human memory. Psychopharmacology 2001, 157, 430–436. [Google Scholar] [CrossRef]
- Hong, S.-W.; Heo, H.; Yang, J.-h.; Han, M.; Kim, D.-H.; Kwon, Y.K. Soyasaponin I improved neuroprotection and regeneration in memory deficient model rats. PLoS ONE 2013, 8, 1–17. [Google Scholar] [CrossRef]
- Xi, Y.-D.; Li, X.-Y.; Ding, J.; Yu, H.-L.; Ma, W.-W.; Yuan, L.-H.; Wu, J.; Xiao, R. Soy isoflavone alleviates Aβ1-42-induced impairment of learning and memory ability through the regulation of RAGE/LRP-1 in neuronal and vascular tissue. Curr. Neurovasc. Res. 2013, 10, 144–156. [Google Scholar] [CrossRef] [PubMed]
- Sirilun, S.; Sivamaruthi, B.S.; Kesika, P.; Peerajan, S.; Chaiyasut, C. Lactic acid bacteria mediated fermented soybean as a potent nutraceutical candidate. Asian Pac. J. Trop. Biomed. 2017, 7, 930–936. [Google Scholar] [CrossRef]
- Lee, H.J.; Hwang, Y.H.; Kim, D.H. Lactobacillus plantarum C29-fermented soybean (DW2009) alleviates memory impairment in 5XFAD transgenic mice by regulating microglia activation and gut microbiota composition. Mol. Nutr. Food Res. 2018, 62, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Yanhong, O.; Chandra, M.; Venkatesh, D. Mild cognitive impairment in adult: A neuropsychological review. Ann. Indian Acad. Neur. 2013, 16, 310–318. [Google Scholar] [CrossRef]
- Saunders, N.L.; Summers, M.J. Attention and working memory deficits in mild cognitive impairment. J. Clin. Exp. Neuropsychol. 2010, 32, 350–357. [Google Scholar] [CrossRef]
- Yoo, D.-H.; Kim, D.-H. Lactobacillus pentosus var. plantarum C29 increases the protective effect of soybean against scopolamine-induced memory impairment in mice. Int. J. Food Sci. Nutr. 2015, 66, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Ha, K.S.; Kwon, J.S.; Lyoo, I.K.; Kong, S.W.; Lee, D.W.; Youn, T. Development and standardization process, and factor analysis of the computerized cognitive function test system for Korean adults. J. Korean Neuropsychiatr. Assoc. 2002, 41, 551–562. [Google Scholar]
- Kwon, J.S.; Lyoo, I.K.; Hong, K.S.; Yeon, B.K.; Ha, K.S. Development and standardization of the computerized memory assessment for Korean adults. J. Korean Neuropsychiatr. Assoc. 2002, 41, 347–362. [Google Scholar]
- Ha, K.S.; Kwon, J.S.; Lyoo, I.K. Development and standardization of the computerized attention assessment for Korean adults. J. Korean Neuropsychiatr. Assoc. 2002, 41, 335–346. [Google Scholar]
- Mattson, M.P.; Maudsley, S.; Martin, B. BDNF and 5-HT: A dynamic duo in age-related neuronal plasticity and neurodegenerative disorders. Trends Neurosci. 2004, 27, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Bekinschtein, P.; Cammarota, M.; Igaz, L.M.; Bevilaqua, L.R.; Izquierdo, I.; Medina, J.H. Persistence of long-term memory storage requires a late protein synthesis-and BDNF-dependent phase in the hippocampus. Neuron 2007, 53, 261–277. [Google Scholar] [CrossRef] [PubMed]
- Lu, B.; Chow, A. Neurotrophins and hippocampal synaptic transmission and plasticity. J. Neurosci. Res. 1999, 58, 76–87. [Google Scholar] [CrossRef]
- Kerschensteiner, M.; Gallmeier, E.; Behrens, L.; Leal, V.V.; Misgeld, T.; Klinkert, W.E.; Kolbeck, R.; Hoppe, E.; Oropeza-Wekerle, R.L.; Bartke, I.; et al. Activated human T cells, B cells, and monocytes produce brain-derived neurotrophic factor in vitro and in inflammatory brain lesions: A neuroprotective role of inflammation? J. Exp. Med. 1999, 189, 865–870. [Google Scholar] [CrossRef] [PubMed]
- Egan, M.F.; Kojima, M.; Callicott, J.H.; Goldberg, T.E.; Kolachana, B.S.; Bertolino, A.; Zaitsev, E.; Gold, B.; Goldman, D.; Dean, M.; et al. The BDNF val66met polymorphism affects activity-dependent secretion of BDNF and human memory and hippocampal function. Cell 2003, 112, 257–269. [Google Scholar] [CrossRef]
- Rybakowski, J.; Borkowska, A.; Skibinska, M.; Hauser, J. Illness-specific association of val66met BDNF polymorphism with performance on Wisconsin Card Sorting Test in bipolar mood disorder. Mol. Psychiatry 2006, 11, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Laske, C.; Stransky, E.; Leyhe, T.; Eschweiler, G.; Wittorf, A.; Richartz, E.; Bartels, M.; Buchkremer, G.; Schott, K. Stage-dependent BDNF serum concentrations in Alzheimer’s disease. J. Neural Transm. 2006, 113, 1217–1224. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Makizako, H.; Yoshida, D.; Tsutsumimoto, K.; Anan, Y.; Uemura, K.; Lee, S.; Park, H.; Suzuki, T. A large, cross-sectional observational study of serum BDNF, cognitive function, and mild cognitive impairment in the elderly. Front. Aging Neurosci. 2014, 6, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Dinan, T.G.; Stilling, R.M.; Stanton, C.; Cryan, J.F. Collective unconscious: How gut microbes shape human behavior. J. Psychiatr. Res. 2015, 63, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de J. R. De-Paula, V.; Forlenza, A.S.; Forlenza, O.V. Relevance of gut microbiota in cognition, behaviour and Alzheimer’s disease. Pharmacol. Res. 2018, 136, 29–34. [Google Scholar] [CrossRef]
- Tan, J.; McKenzie, C.; Potamitis, M.; Thorburn, A.N.; Mackay, C.R.; Macia, L. The Role of Short-Chain Fatty Acids in Health and Disease. Adv. Immunol. 2014, 121, 91–119. [Google Scholar] [CrossRef]
- Lee, H.-J.; Lim, S.-M.; Ko, D.-B.; Jeong, J.-J.; Hwang, Y.-H.; Kim, D.-H. Soyasapogenol B and genistein attenuate lipopolysaccharide-induced memory impairment in mice by the modulation of NF-κB-mediated BDNF expression. J. Agric. Food Chem. 2017, 65, 6877–6885. [Google Scholar] [CrossRef] [PubMed]
- Flint, H.J.; Scott, K.P.; Louis, P.; Duncan, S.H. The role of the gut microbiota in nutrition and health. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 577–589. [Google Scholar] [CrossRef] [PubMed]
- Martí, J.M.; Martínez-Martínez, D.; Rubio, T.; Gracia, C.; Peña, M.; Latorre, A.; Moya, A.; Garay, C.P. Health and disease imprinted in the time variability of the human microbiome. mSystems 2017, 2, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Salminen, S.; von Wright, A.; Morelli, L.; Marteau, P.; Brassart, D.; de Vos, W.M.; Fondén, R.; Saxelin, M.; Collins, K.; Mogensen, G. Demonstration of safety of probiotics—A review. Int. J. Food Microbiol. 1998, 44, 93–106. [Google Scholar] [CrossRef]
- Cryan, J.F.; Dinan, T.G. Mind-altering microorganisms: The impact of the gut microbiota on brain and behaviour. Nat. Rev. Neurosci. 2012, 13, 701–712. [Google Scholar] [CrossRef]
- Dinan, T.G.; Cryan, J.F. Brain-gut-microbiota axis and mental health. Psychosom. Med. 2017, 79, 920–926. [Google Scholar] [CrossRef]
- Krikorian, R.; Shidler, M.D.; Nash, T.A.; Kalt, W.; Vinqvist-Tymchuk, M.R.; Shukitt-Hale, B.; Joseph, J.A. Blueberry supplementation improves memory in older adults. J. Agric. Food Chem. 2010, 58, 3996–4000. [Google Scholar] [CrossRef]
- Desideri, G.; Kwik-Uribe, C.; Grassi, D.; Necozione, S.; Ghiadoni, L.; Mastroiacovo, D.; Raffaele, A.; Ferri, L.; Bocale, R.; Lechiara, M.C.; et al. Benefits in cognitive function, blood pressure, and insulin resistance through cocoa flavanol consumption in elderly subjects with mild cognitive impairment: The Cocoa, Cognition, and Aging (CoCoA) study. Hypertension 2012, 60, 794–801. [Google Scholar] [CrossRef]
- Ito, N.; Saito, H.; Seki, S.; Ueda, F.; Asada, T. Effects of composite supplement containing astaxanthin and sesamin on cognitive functions in people with mild cognitive impairment: A randomized, double-blind, placebo-controlled trial. J. Alzheimers Dis. 2018, 62, 1767–1775. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Treatment Groups | p-Value | |
|---|---|---|---|
| Placebo (n = 50) | DW2009 Group (n = 50) | ||
| Demographic characteristics | |||
| Age, mean, (SD) | 69.2 (7.00) | 68.0 (5.12) | 0.35 |
| Women, No. (%) | 36 (72.0) | 30 (60.0) | 0.21 |
| Education, No. (%) | |||
| 0–11 years | 25 (50.0) | 30 (60.0) | 0.43 |
| 12 years | 17 (34.0) | 16 (32.0) | |
| 13 years or more | 8 (16.0) | 4 (8.00) | |
| Marital status, No. (%) | |||
| Married | 50 (100) | 49 (98.0) | 1.00 |
| Divorced, widowed, or separated | 0 (0.00) | 1 (2.00) | |
| Clinical characteristics | |||
| Auditory continuous performance test 1 | |||
| Reaction time | 0.77 (0.08) | 0.79 (0.08) | 0.13 |
| Correct response | 127 (9.41) | 121 (20.2) | 0.04 |
| Incorrect response | 6.29 (6.15) | 9.22 (8.12) | 0.05 |
| Omission error | 7.71 (9.40) | 14.2 (20.2) | 0.04 |
| Digit span test | |||
| List memory score | 7.44 (3.35) | 7.34 (3.66) | 0.89 |
| Tracking score | 5.26 (1.23) | 5.34 (1.45) | 0.77 |
| Verbal learning test | |||
| Immediate recall | 9.04 (2.22) | 8.30 (2.35) | 0.11 |
| Delayed recall | 7.30 (2.62) | 6.84 (2.91) | 0.41 |
| Recognition | 11.3 (2.34) | 10.6 (3.21) | 0.19 |
| Placebo | DW2009 | z | p for Interaction | p for Group | p for Time | |||
|---|---|---|---|---|---|---|---|---|
| Baseline (n = 50) | Follow-up (n = 47) | Baseline (n = 50) | Follow-up (n = 45) | |||||
| Attention/Prefrontal function 1 | ||||||||
| Reaction time | 0.77 (0.08) | 0.78 (0.08) | 0.79 (0.08) | 0.77 (0.09) | −2.99 | 0.003 | 0.50 | 0.25 |
| Correct response | 127 (9.41) | 130 (8.38) | 121 (20.2) | 125 (16.2) | 1.59 | 0.11 | 0.38 | 0.06 |
| Incorrect response | 6.29 (6.15) | 4.96 (5.27) | 9.22 (8.12) | 6.00 (5.84) | −1.64 | 0.10 | 0.32 | 0.07 |
| Omission error | 7.71 (9.40) | 5.22 (8.38) | 14.2 (20.2) | 9.56 (16.2) | −1.62 | 0.11 | 0.38 | 0.06 |
| Domain composite score | 0.00 (0.82) | 0.15 (0.70) | −0.54 (1.44) | −0.09 (1.05) | 2.34 | 0.02 | 0.24 | 0.11 |
| Working memory function | ||||||||
| List memory score | 7.44 (3.35) | 7.68 (3.65) | 7.34 (3.66) | 7.87 (3.57) | 0.92 | 0.36 | 0.81 | 0.29 |
| Tracking score | 5.26 (1.23) | 5.21 (1.30) | 5.34 (1.45) | 5.38 (1.39) | 0.79 | 0.43 | 0.82 | 0.87 |
| Domain composite score | 0.00 (0.98) | 0.02 (1.06) | 0.02 (1.12) | 0.11 (1.08) | 0.63 | 0.53 | 0.90 | 0.69 |
| Verbal memory function | ||||||||
| Immediate recall | 9.04 (2.22) | 10.4 (2.48) | 8.30 (2.35) | 10.2 (2.77) | 1.09 | 0.28 | 0.67 | <0.001 |
| Delayed recall | 7.30 (2.62) | 9.19 (3.10) | 6.84 (2.91) | 9.11 (2.81) | 0.53 | 0.60 | 0.72 | <0.001 |
| Recognition | 11.3 (2.34) | 12.4 (1.94) | 10.6 (3.21) | 12.2 (2.18) | 1.16 | 0.25 | 0.53 | <0.001 |
| Domain composite score | 0.00 (0.87) | 0.58 (0.93) | −0.28 (0.99) | 0.52 (0.98) | 1.26 | 0.21 | 0.66 | <0.001 |
| Combined cognitive function | ||||||||
| Domain composite score | 0.01 (0.68) | 0.25 (0.65) | −0.27 (0.95) | 0.18 (0.79) | 2.36 | 0.02 | 0.55 | <0.001 |
| Gut Microbiota Composition | Placebo Group | DW2009 Group | ||||
|---|---|---|---|---|---|---|
| Baseline | Follow-up | n | Baseline | Follow-up | n | |
| Bifidobacterium spp. | 2.99 × 1011 (1.13 × 1012) | 4.46 × 1010 (1.11 × 1011) | 40 | 4.16 × 1011 (1.16 × 1012) | 5.04 × 1011 (1.75 × 1012) | 38 |
| Lactobacillus spp. | 3.52 × 1010 (1.22 × 1011) | 6.80 × 1010 (1.69 × 1011) | 38 | 1.82 × 1010 (3.43 × 1010) | 8.04 × 1010 * (1.82 × 1011) | 37 |
| Clostridium spp. | 2.20 × 1011 (8.46 × 1011) | 6.60 × 1010 (1.41 × 1011) | 40 | 8.00 × 1010 (1.80 × 1011) | 8.38 × 1010 (2.32 × 1011) | 38 |
| Laboratory Profiles | Baseline | Follow-up | ||||
|---|---|---|---|---|---|---|
| Placebo (n = 50) | DW2009 (n = 50) | p | Placebo (n = 47) | DW2009 (n = 45) | p | |
| Systolic blood pressure (mmHg) | 129 (13.3) | 130 (13.5) | 0.64 | 125 (13.4) | 126 (12.8) | 0.67 |
| Diastolic blood pressure (mmHg) | 78.3 (9.20) | 81.4 (7.37) | 0.06 | 76.2 (9.75) | 77.4 (7.26) | 0.52 |
| Pulse rate (beats/min) | 73.0 (10.1) | 73.4 (11.1) | 0.84 | 72.7 (7.58) | 71.2 (8.64) | 0.38 |
| Body weight (kg) | 60.3 (11.2) | 63.2 (8.27) | 0.15 | 60.0 (10.4) | 62.6 (8.25) | 0.19 |
| Body mass index (kg/m2) | 24.0 (3.41) | 24.7 (3.16) | 0.30 | 23.9 (3.16) | 24.6 (3.31) | 0.29 |
| Laboratory Profiles | Baseline | Follow-up | ||||
|---|---|---|---|---|---|---|
| Placebo (n = 50) | DW2009 (n = 50) | p | Placebo (n = 47) | DW2009 (n = 45) | p | |
| Complete blood cell count | ||||||
| WBC (109/L) | 5.43 (1.16) | 5.63 (1.19) | 0.39 | 5.77 (1.51) | 5.77 (1.45) | 0.99 |
| RBC (1012/L) | 4.33 (0.33) | 4.43 (0.33) | 0.12 | 4.29 (0.32) | 4.41 (0.30) | 0.06 |
| Hemoglobin (g/L) | 134 (10.4) | 137 (10.7) | 0.23 | 133 (10.2) | 136 (8.92) | 0.11 |
| Hematocrit (proportion of 1.0) | 0.40 (0.03) | 0.41 (0.03) | 0.29 | 0.40 (0.03) | 0.41 (0.03) | 0.13 |
| Platelet (109/L) | 239 (53.9) | 246 (56.7) | 0.55 | 241 (54.9) | 248 (55.3) | 0.57 |
| Neutrophil (proportion of 1.0) | 0.54 (0.08) | 0.57 (0.09) | 0.11 | 0.55 (0.09) | 0.57 (0.08) | 0.25 |
| Blood chemistry | ||||||
| Total Protein (g/L) | 73.1 (4.16) | 73.6 (3.76) | 0.55 | 73.4 (3.75) | 72.7 (3.62) | 0.37 |
| Albumin (g/L) | 42.3 (1.88) | 42.9 (2.14) | 0.15 | 42.4 (1.75) | 42.4 (1.84) | 0.95 |
| AST (µkat/L) | 0.42 (0.11) | 0.41 (0.11) | 0.74 | 0.43 (0.13) | 0.40 (0.10) | 0.12 |
| ALT (µkat/L) | 0.33 (0.17) | 0.35 (0.16) | 0.47 | 0.34 (0.13) | 0.32 (0.11) | 0.63 |
| ALP (µkat/L) | 1.23 (0.32) | 1.33 (0.50) | 0.24 | 1.25 (0.31) | 1.32(0.45) | 0.43 |
| Total Bilirubin (µmol/L) | 14.4 (5.20) | 15.1 (6.06) | 0.58 | 13.1 (4.05) | 14.4 (6.98) | 0.26 |
| Total Cholesterol (mmol/L) | 5.23 (0.81) | 5.02 (0.98) | 0.26 | 5.08 (0.64) | 4.97 (0.88) | 0.51 |
| Glucose (mmol/L) | 5.32 (0.79) | 5.30 (0.71) | 0.92 | 5.36 (0.83) | 5.31 (0.69) | 0.79 |
| Creatinine (µmol/L) | 61.7 (13.5) | 63.6 (13.3) | 0.48 | 61.5 (13.3) | 62.5 (14.3) | 0.74 |
| BUN (mmol/L) | 5.50 (1.19) | 5.56 (1.35) | 0.80 | 5.73 (1.57) | 5.89 (1.45) | 0.63 |
| Uric acid (µmol/L) | 286 (78.1) | 299 (71.0) | 0.40 | 286 (75.0) | 311 (69.8) | 0.11 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, Y.-H.; Park, S.; Paik, J.-W.; Chae, S.-W.; Kim, D.-H.; Jeong, D.-G.; Ha, E.; Kim, M.; Hong, G.; Park, S.-H.; et al. Efficacy and Safety of Lactobacillus Plantarum C29-Fermented Soybean (DW2009) in Individuals with Mild Cognitive Impairment: A 12-Week, Multi-Center, Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Nutrients 2019, 11, 305. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11020305
Hwang Y-H, Park S, Paik J-W, Chae S-W, Kim D-H, Jeong D-G, Ha E, Kim M, Hong G, Park S-H, et al. Efficacy and Safety of Lactobacillus Plantarum C29-Fermented Soybean (DW2009) in Individuals with Mild Cognitive Impairment: A 12-Week, Multi-Center, Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Nutrients. 2019; 11(2):305. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11020305
Chicago/Turabian StyleHwang, Yun-Ha, Shinwon Park, Jong-Woo Paik, Soo-Wan Chae, Dong-Hyun Kim, Doc-Gyun Jeong, Eunji Ha, Myeongju Kim, Gahae Hong, Soo-Hyun Park, and et al. 2019. "Efficacy and Safety of Lactobacillus Plantarum C29-Fermented Soybean (DW2009) in Individuals with Mild Cognitive Impairment: A 12-Week, Multi-Center, Randomized, Double-Blind, Placebo-Controlled Clinical Trial" Nutrients 11, no. 2: 305. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11020305