Potential Biomarkers for Fat from Dairy and Fish and Their Association with Cardiovascular Risk Factors: Cross-sectional Data from the LifeLines Biobank and Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Dietary Intake
2.3. Data on Education, Smoking Habits and General Health
2.4. Clinical Measurements
2.5. Biochemical Measurements
2.6. Fatty Acid Analyses
2.7. Statistical Analyses
3. Results
3.1. The Lifelines Population
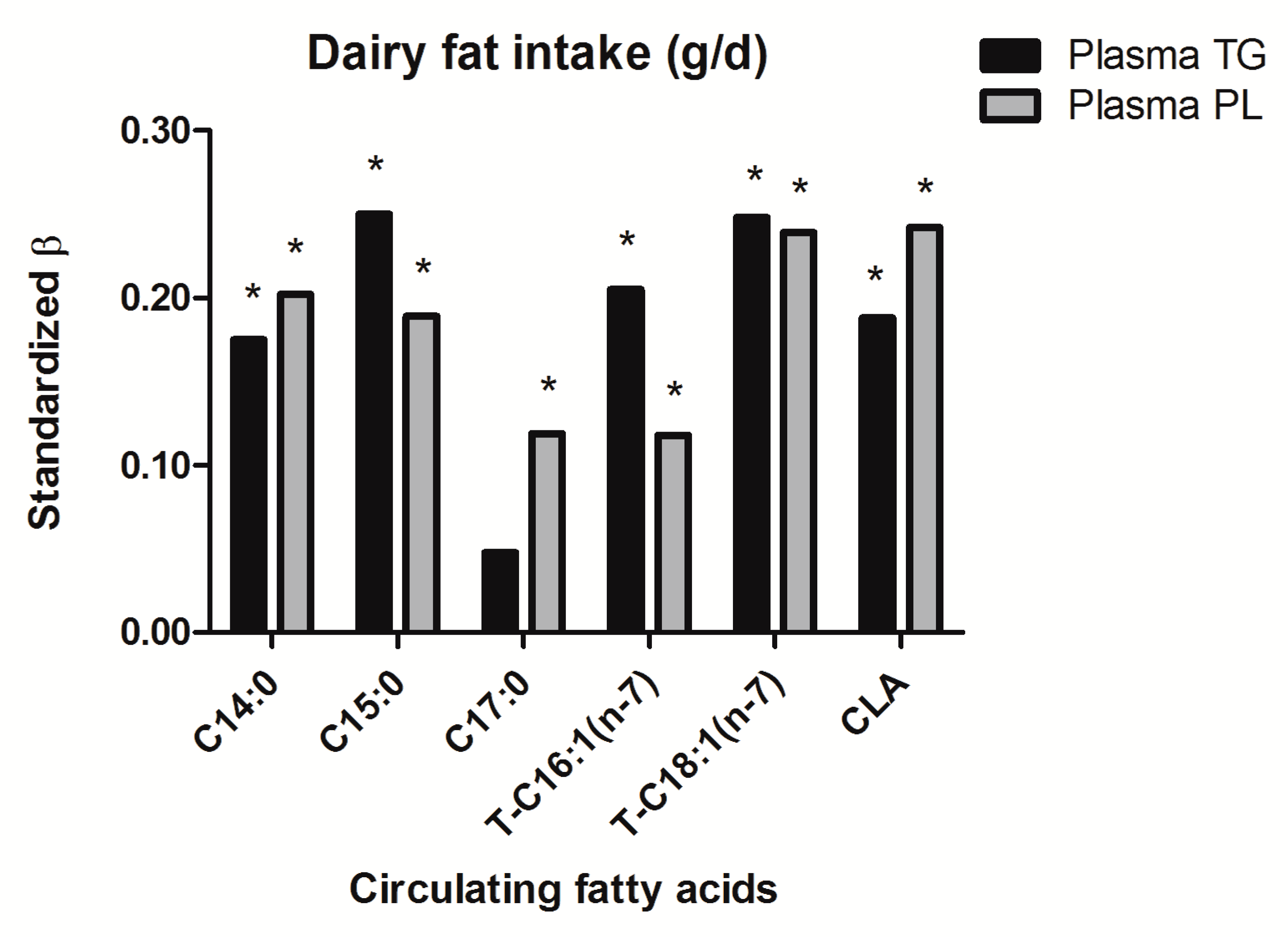
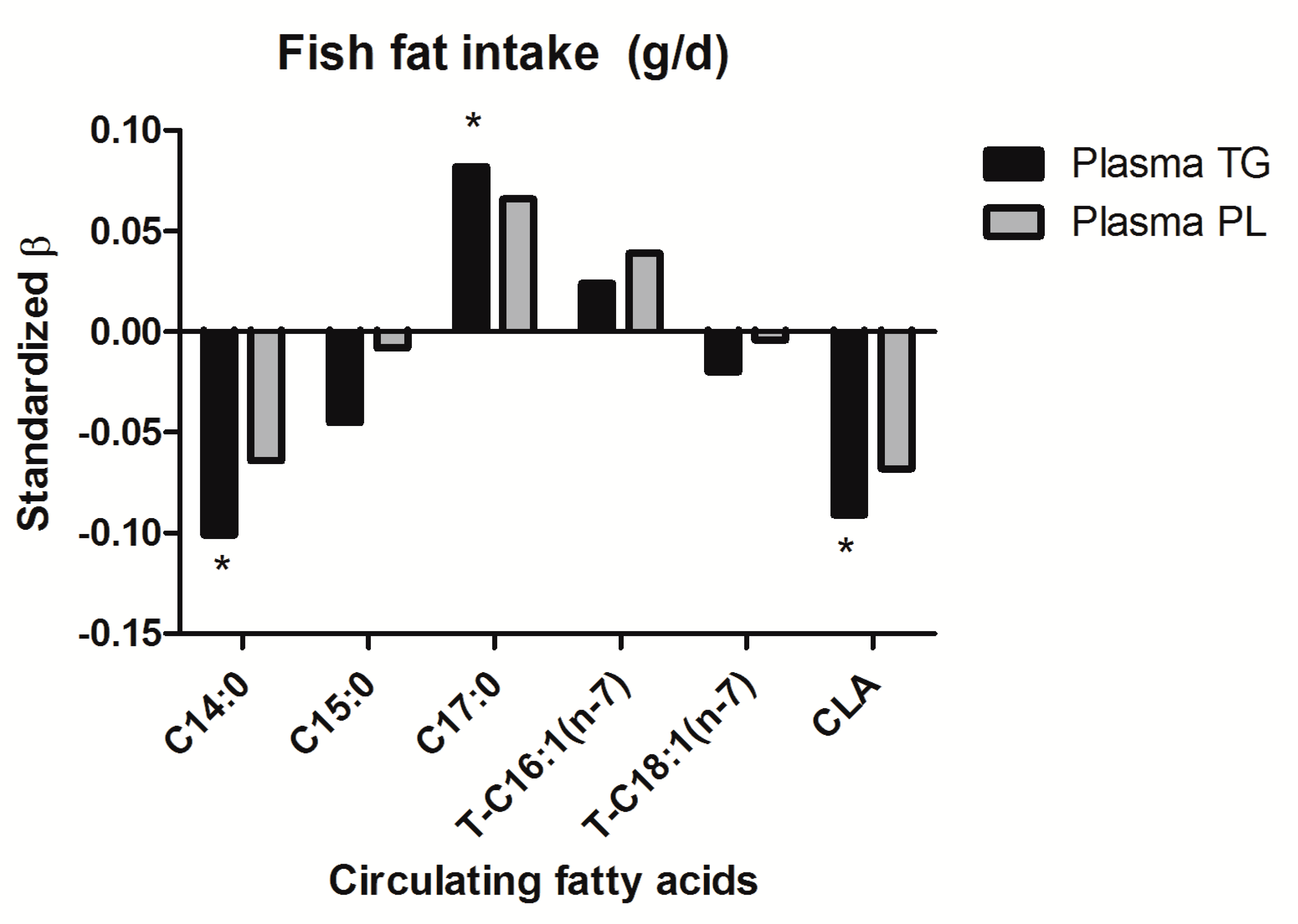
3.2. Biomarkers for Dairy Fat or Fish Fat
3.3. Circulating Fatty Acids in Plasma TG and Cardiovascular Risk Factors
3.4. Circulating Fatty Acids in Plasma PL and Cardiovascular Risk Factors
3.5. Dairy Fat Intake, Fish Fat Intake and Cardiovascular Risk Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO (World Health Organization). Cardiovascular Diseases (CVDs) Fact Sheet; WHO: Geneva, Switzerland, 2017; p. 2017. [Google Scholar]
- Wanders, A.J.; Alssema, M.; de Koning, E.J.; le Cessie, S.; de Vries, J.H.; Zock, P.L.; Rosendaal, F.R.; Heijer, M.D.; de Mutsert, R. Fatty Acid Intake and its Dietary Sources in Relation with Markers of Type 2 Diabetes Risk: The NEO Study. Eur. J. Clin. Nutr. 2017, 71, 245–251. [Google Scholar] [CrossRef]
- De Oliveira Otto, M.C.; Mozaffarian, D.; Kromhout, D.; Bertoni, A.G.; Sibley, C.T.; Jacobs, D.R., Jr.; Nettleton, J.A. Dietary Intake of Saturated Fat by Food Source and Incident Cardiovascular Disease: The Multi-Ethnic Study of Atherosclerosis. Am. J. Clin. Nutr. 2012, 96, 397–404. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira Otto, M.C.; Nettleton, J.A.; Lemaitre, R.N.; Steffen, L.M.; Kromhout, D.; Rich, S.S.; Tsai, M.Y.; Jacobs, D.R.; Mozaffarian, D. Biomarkers of Dairy Fatty Acids and Risk of Cardiovascular Disease in the Multi-Ethnic Study of Atherosclerosis. J. Am. Heart Assoc. 2013, 2, e000092. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Ma, J.; Campos, H.; Hu, F.B. Plasma and Erythrocyte Biomarkers of Dairy Fat Intake and Risk of Ischemic Heart Disease. Am. J. Clin. Nutr. 2007, 86, 929–937. [Google Scholar] [CrossRef] [PubMed]
- Warensjo, E.; Jansson, J.H.; Cederholm, T.; Boman, K.; Eliasson, M.; Hallmans, G.; Johansson, I.; Sjogren, P. Biomarkers of Milk Fat and the Risk of Myocardial Infarction in Men and Women: A Prospective, Matched Case-Control Study. Am. J. Clin. Nutr. 2010, 92, 194–202. [Google Scholar] [CrossRef]
- Warensjo, E.; Smedman, A.; Stegmayr, B.; Hallmans, G.; Weinehall, L.; Vessby, B.; Johansson, I. Stroke and Plasma Markers of Milk Fat Intake—A Prospective Nested Case-Control Study. Nutr. J. 2009, 8, 21. [Google Scholar] [CrossRef]
- Gebauer, S.K.; Chardigny, J.M.; Jakobsen, M.U.; Lamarche, B.; Lock, A.L.; Proctor, S.D.; Baer, D.J. Effects of Ruminant Trans Fatty Acids on Cardiovascular Disease and Cancer: A Comprehensive Review of Epidemiological, Clinical, and Mechanistic Studies. Adv. Nutr. 2011, 2, 332–354. [Google Scholar] [CrossRef] [PubMed]
- Kromhout, D.; Menotti, A.; Bloemberg, B.; Aravanis, C.; Blackburn, H.; Buzina, R.; Dontas, A.S.; Fidanza, F.; Giampaoli, S.; Jansen, A. Dietary Saturated and Trans Fatty Acids and Cholesterol and 25-Year Mortality from Coronary Heart Disease: The Seven Countries Study. Prev. Med. 1995, 24, 308–315. [Google Scholar] [CrossRef]
- Li, H.; Zhang, Q.; Song, J.; Wang, A.; Zou, Y.; Ding, L.; Wen, Y. Plasma Trans-Fatty Acids Levels and Mortality: A Cohort Study Based on 1999–2000 National Health and Nutrition Examination Survey (NHANES). Lipids Health Dis. 2017, 16, 176. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Katan, M.B.; Ascherio, A.; Stampfer, M.J.; Willett, W.C. Trans Fatty Acids and Cardiovascular Disease. N. Engl. J. Med. 2006, 354, 1601–1613. [Google Scholar] [CrossRef]
- Sofie Biong, A.; Berstad, P.; Pedersen, J.I. Biomarkers for Intake of Dairy Fat and Dairy Products. Eur. J. Lipid Sci. Technol. 2006, 108, 827–834. [Google Scholar] [CrossRef]
- Warensjo Lemming, E.; Nalsen, C.; Becker, W.; Ridefelt, P.; Mattisson, I.; Lindroos, A.K. Relative Validation of the Dietary Intake of Fatty Acids among Adults in the Swedish National Dietary Survey using Plasma Phospholipid Fatty Acid Composition. J. Nutr. Sci. 2015, 4, e25. [Google Scholar] [CrossRef]
- Lund-Blix, N.A.; Ronningen, K.S.; Boas, H.; Tapia, G.; Andersen, L.F. Plasma Phospholipid Pentadecanoic Acid, EPA, and DHA, and the Frequency of Dairy and Fish Product Intake in Young Children. Food Nutr. Res. 2016, 60, 31933. [Google Scholar] [CrossRef]
- Yakoob, M.Y.; Shi, P.; Willett, W.C.; Rexrode, K.M.; Campos, H.; Orav, E.J.; Hu, F.B.; Mozaffarian, D. Circulating Biomarkers of Dairy Fat and Risk of Incident Diabetes Mellitus among Men and Women in the United States in Two Large Prospective Cohorts. Circulation 2016, 133, 1645–1654. [Google Scholar] [CrossRef] [PubMed]
- Aslibekyan, S.; Campos, H.; Baylin, A. Biomarkers of Dairy Intake and the Risk of Heart Disease. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 1039–1045. [Google Scholar] [CrossRef] [PubMed]
- Ratnayake, W.M. Concerns about the use of 15:0, 17:0, and Trans-16:1n-7 as Biomarkers of Dairy Fat Intake in Recent Observational Studies that Suggest Beneficial Effects of Dairy Food on Incidence of Diabetes and Stroke. Am. J. Clin. Nutr. 2015, 101, 1102–1103. [Google Scholar] [CrossRef] [PubMed]
- Ozogul, Y.; Ozogul, F.; Cicek, E.; Polat, A.; Kuley, E. Fat Content and Fatty Acid Compositions of 34 Marine Water Fish Species from the Mediterranean Sea. Int. J. Food Sci. Nutr. 2009, 60, 464–475. [Google Scholar] [CrossRef]
- Lankinen, M.; Schwab, U. Biomarkers of Dairy Fat. Am. J. Clin. Nutr. 2015, 101, 1101–1102. [Google Scholar] [CrossRef]
- Mori, T.A. Marine OMEGA-3 Fatty Acids in the Prevention of Cardiovascular Disease. Fitoterapia 2017, 123, 51–58. [Google Scholar] [CrossRef]
- Whelton, S.P.; He, J.; Whelton, P.K.; Muntner, P. Meta-Analysis of Observational Studies on Fish Intake and Coronary Heart Disease. Am. J. Cardiol. 2004, 93, 1119–1123. [Google Scholar] [CrossRef]
- Maki, K.C.; Palacios, O.M.; Bell, M.; Toth, P.P. Use of Supplemental Long-Chain Omega-3 Fatty Acids and Risk for Cardiac Death: An Updated Meta-Analysis and Review of Research Gaps. J. Clin. Lipidol. 2017, 11, 1152–1160.e2. [Google Scholar] [CrossRef]
- Stolk, R.P.; Rosmalen, J.G.; Postma, D.S.; de Boer, R.A.; Navis, G.; Slaets, J.P.; Ormel, J.; Wolffenbuttel, B.H. Universal Risk Factors for Multifactorial Diseases: LifeLines: A Three-Generation Population-Based Study. Eur. J. Epidemiol. 2008, 23, 67–74. [Google Scholar] [CrossRef]
- Scholtens, S.; Smidt, N.; Swertz, M.A.; Bakker, S.J.; Dotinga, A.; Vonk, J.M.; van Dijk, F.; van Zon, S.K.; Wijmenga, C.; Wolffenbuttel, B.H.; et al. Cohort Profile: LifeLines, a Three-Generation Cohort Study and Biobank. Int. J. Epidemiol. 2015, 44, 1172–1180. [Google Scholar] [CrossRef] [PubMed]
- Klijs, B.; Scholtens, S.; Mandemakers, J.J.; Snieder, H.; Stolk, R.P.; Smidt, N. Representativeness of the LifeLines Cohort Study. PLoS ONE 2015, 10, e0137203. [Google Scholar] [CrossRef]
- Nederland, S.V. Zo Eet Nederland: Resultaten Van De Voedselconsumptiepeiling 1997–1998; Voedingscentrum: Den Haag, The Netherlands, 1998. [Google Scholar]
- Iwani, N.A.; Jalaludin, M.Y.; Zin, R.M.; Fuziah, M.Z.; Hong, J.Y.; Abqariyah, Y.; Mokhtar, A.H.; Wan Nazaimoon, W.M. Triglyceride to HDL-C Ratio is Associated with Insulin Resistance in Overweight and Obese Children. Sci. Rep. 2017, 7, 40055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoving, E.B.; Jansen, G.; Volmer, M.; Van Doormaal, J.J.; Muskiet, F.A. Profiling of Plasma Cholesterol Ester and Triglyceride Fatty Acids as their Methyl Esters by Capillary Gas Chromatography, Preceded by a Rapid Aminopropyl-Silica Column Chromatographic Separation of Lipid Classes. J. Chromatogr. 1988, 434, 395–409. [Google Scholar] [CrossRef]
- Folch, J.; Lees, M.; Sloane Stanley, G.H. A Simple Method for the Isolation and Purification of Total Lipides from Animal Tissues. J. Biol. Chem. 1957, 226, 497–509. [Google Scholar]
- Kaluzny, M.A.; Duncan, L.A.; Merritt, M.V.; Epps, D.E. Rapid Separation of Lipid Classes in High Yield and Purity using Bonded Phase Columns. J. Lipid Res. 1985, 26, 135–140. [Google Scholar]
- Robberecht, E.; Koletzko, B.; Christophe, A. Several Mechanisms Contribute to the Abnormal Fatty Acid Composition of Serum Phospholipids and Cholesterol Esters in Cholestatic Children with Extrahepatic Biliary Atresia. Prostaglandins Leukot. Essent. Fatty Acids 1997, 56, 199–204. [Google Scholar] [CrossRef]
- Smedman, A.E.; Gustafsson, I.B.; Berglund, L.G.; Vessby, B.O. Pentadecanoic Acid in Serum as a Marker for Intake of Milk Fat: Relations between Intake of Milk Fat and Metabolic Risk Factors. Am. J. Clin. Nutr. 1999, 69, 22–29. [Google Scholar] [CrossRef]
- Wolk, A.; Vessby, B.; Ljung, H.; Barrefors, P. Evaluation of a Biological Marker of Dairy Fat Intake. Am. J. Clin. Nutr. 1998, 68, 291–295. [Google Scholar] [CrossRef]
- Wolk, A.; Furuheim, M.; Vessby, B. Fatty Acid Composition of Adipose Tissue and Serum Lipids are Valid Biological Markers of Dairy Fat Intake in Men. J. Nutr. 2001, 131, 828–833. [Google Scholar] [CrossRef]
- Golley, R.K.; Hendrie, G.A. Evaluation of the Relative Concentration of Serum Fatty Acids C14:0, C15:0 and C17:0 as Markers of Children’s Dairy Fat Intake. Ann. Nutr. Metab. 2014, 65, 310–316. [Google Scholar] [CrossRef]
- Yakoob, M.Y.; Shi, P.; Hu, F.B.; Campos, H.; Rexrode, K.M.; Orav, E.J.; Willett, W.C.; Mozaffarian, D. Circulating Biomarkers of Dairy Fat and Risk of Incident Stroke in U.S. Men and Women in 2 Large Prospective Cohorts. Am. J. Clin. Nutr. 2014, 100, 1437–1447. [Google Scholar] [CrossRef]
- Smit, L.A.; Baylin, A.; Campos, H. Conjugated Linoleic Acid in Adipose Tissue and Risk of Myocardial Infarction. Am. J. Clin. Nutr. 2010, 92, 34–40. [Google Scholar] [CrossRef]
- Jiang, J.; Wolk, A.; Vessby, B. Relation between the Intake of Milk Fat and the Occurrence of Conjugated Linoleic Acid in Human Adipose Tissue. Am. J. Clin. Nutr. 1999, 70, 21–27. [Google Scholar] [CrossRef]
- Rosell, M.; Johansson, G.; Berglund, L.; Vessby, B.; de Faire, U.; Hellenius, M.L. Associations between the Intake of Dairy Fat and Calcium and Abdominal Obesity. Int. J. Obes. Relat. Metab. Disord. 2004, 28, 1427–1434. [Google Scholar] [CrossRef]
- Brouwer-Brolsma, E.; Sluik, D.; Singh-Povel, C.; Feskens, E. Dairy shows Different Associations with Abdominal and BMI-Defined Overweight: Cross-Sectional Analyses Exploring a Variety of Dairy Products. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 451–460. [Google Scholar] [CrossRef]
- Kratz, M.; Baars, T.; Guyenet, S. The Relationship between High-Fat Dairy Consumption and Obesity, Cardiovascular, and Metabolic Disease. Eur. J. Nutr. 2013, 52, 1–24. [Google Scholar] [CrossRef]
- Mozaffarian, D.; de Oliveira Otto, M.C.; Lemaitre, R.N.; Fretts, A.M.; Hotamisligil, G.; Tsai, M.Y.; Siscovick, D.S.; Nettleton, J.A. Trans-Palmitoleic Acid, Other Dairy Fat Biomarkers, and Incident Diabetes: The Multi-Ethnic Study of Atherosclerosis (MESA). Am. J. Clin. Nutr. 2013, 97, 854–861. [Google Scholar] [CrossRef]
- Hansen, C.P.; Berentzen, T.L.; Halkjaer, J.; Tjonneland, A.; Sorensen, T.I.; Overvad, K.; Jakobsen, M.U. Intake of Ruminant Trans Fatty Acids and Changes in Body Weight and Waist Circumference. Eur. J. Clin. Nutr. 2012, 66, 1104–1109. [Google Scholar] [CrossRef]
- Kratz, M.; Marcovina, S.; Nelson, J.E.; Yeh, M.M.; Kowdley, K.V.; Callahan, H.S.; Song, X.; Di, C.; Utzschneider, K.M. Dairy Fat Intake is Associated with Glucose Tolerance, Hepatic and Systemic Insulin Sensitivity, and Liver Fat but Not Beta-Cell Function in Humans. Am. J. Clin. Nutr. 2014, 99, 1385–1396. [Google Scholar] [CrossRef]
- Iggman, D.; Arnlov, J.; Vessby, B.; Cederholm, T.; Sjogren, P.; Riserus, U. Adipose Tissue Fatty Acids and Insulin Sensitivity in Elderly Men. Diabetologia 2010, 53, 850–857. [Google Scholar] [CrossRef]
- Brouwer-Brolsma, E.M.; Sluik, D.; Singh-Povel, C.M.; Feskens, E.J.M. Dairy Product Consumption is Associated with Pre-Diabetes and Newly Diagnosed Type 2 Diabetes in the Lifelines Cohort Study. Br. J. Nutr. 2018, 119, 442–455. [Google Scholar] [CrossRef]
- Wang, H.; Steffen, L.M.; Vessby, B.; Basu, S.; Steinberger, J.; Moran, A.; Jacobs, D.R., Jr.; Hong, C.P.; Sinaiko, A.R. Obesity Modifies the Relations between Serum Markers of Dairy Fats and Inflammation and Oxidative Stress among Adolescents. Obesity (Silver Spring) 2011, 19, 2404–2410. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Cao, H.; King, I.B.; Lemaitre, R.N.; Song, X.; Siscovick, D.S.; Hotamisligil, G.S. Trans-Palmitoleic Acid, Metabolic Risk Factors, and New-Onset Diabetes in U.S. Adults: A Cohort Study. Ann. Intern. Med. 2010, 153, 790–799. [Google Scholar] [CrossRef]
- Mathieu, P.; Lemieux, I.; Després, J. Obesity, Inflammation, and Cardiovascular Risk. Clin. Pharmacol. Ther. 2010, 87, 407–416. [Google Scholar] [CrossRef]
- Ridker, P.M. High-Sensitivity C-Reactive Protein, Inflammation, and Cardiovascular Risk: From Concept to Clinical Practice to Clinical Benefit. Am. Heart J. 2004, 148, S19–S26. [Google Scholar] [CrossRef]
- Li, Y.; Zhong, X.; Cheng, G.; Zhao, C.; Zhang, L.; Hong, Y.; Wan, Q.; He, R.; Wang, Z. Hs-CRP and all-Cause, Cardiovascular, and Cancer Mortality Risk: A Meta-Analysis. Atherosclerosis 2017, 259, 75–82. [Google Scholar] [CrossRef]
- Choi, H.K.; Liu, S.; Curhan, G. Intake of Purine-Rich Foods, Protein, and Dairy Products and Relationship to Serum Levels of Uric Acid: The Third National Health and Nutrition Examination Survey. Arthritis Rheum. 2005, 52, 283–289. [Google Scholar] [CrossRef]
- Chen, J.H.; Chuang, S.Y.; Chen, H.J.; Yeh, W.T.; Pan, W.H. Serum Uric Acid Level as an Independent Risk Factor for all-Cause, Cardiovascular, and Ischemic Stroke Mortality: A Chinese Cohort Study. Arthritis Rheum. 2009, 61, 225–232. [Google Scholar] [CrossRef]
- Niskanen, L.K.; Laaksonen, D.E.; Nyyssonen, K.; Alfthan, G.; Lakka, H.M.; Lakka, T.A.; Salonen, J.T. Uric Acid Level as a Risk Factor for Cardiovascular and all-Cause Mortality in Middle-Aged Men: A Prospective Cohort Study. Arch. Intern. Med. 2004, 164, 1546–1551. [Google Scholar] [CrossRef]
- Ruggiero, C.; Cherubini, A.; Ble, A.; Bos, A.J.; Maggio, M.; Dixit, V.D.; Lauretani, F.; Bandinelli, S.; Senin, U.; Ferrucci, L. Uric Acid and Inflammatory Markers. Eur. Heart J. 2006, 27, 1174–1181. [Google Scholar] [CrossRef] [PubMed]
- Frohlich, M.; Imhof, A.; Berg, G.; Hutchinson, W.L.; Pepys, M.B.; Boeing, H.; Muche, R.; Brenner, H.; Koenig, W. Association between C-Reactive Protein and Features of the Metabolic Syndrome: A Population-Based Study. Diabetes Care 2000, 23, 1835–1839. [Google Scholar] [CrossRef] [PubMed]
- Hodge, A.M.; English, D.R.; O’Dea, K.; Sinclair, A.J.; Makrides, M.; Gibson, R.A.; Giles, G.G. Plasma Phospholipid and Dietary Fatty Acids as Predictors of Type 2 Diabetes: Interpreting the Role of Linoleic Acid. Am. J. Clin. Nutr. 2007, 86, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Sluik, D.; Geelen, A.; de Vries, J.H.; Eussen, S.J.; Brants, H.A.; Meijboom, S.; van Dongen, M.C.; Bueno-de-Mesquita, H.B.; Wijckmans-Duysens, N.E.; van’t Veer, P.; et al. A National FFQ for the Netherlands (the FFQ-NL 1.0): Validation of a Comprehensive FFQ for Adults. Br. J. Nutr. 2016, 116, 913–923. [Google Scholar] [CrossRef] [PubMed]
- Brouwer-Brolsma, E.M.; Streppel, M.T.; van Lee, L.; Geelen, A.; Sluik, D.; van de Wiel, A.M.; de Vries, J.H.M.; van’t Veer, P.; Feskens, E.J.M. A National Dietary Assessment Reference Database (NDARD) for the Dutch Population: Rationale Behind the Design. Nutrients 2017, 9, 1136. [Google Scholar] [CrossRef] [PubMed]
- Glaser, C.; Demmelmair, H.; Koletzko, B. High-Throughput Analysis of Fatty Acid Composition of Plasma Glycerophospholipids. J. Lipid Res. 2010, 51, 216–221. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline Characteristics | Total N = 769 | Males N = 404 | Females N = 365 | p-value |
|---|---|---|---|---|
| General | ||||
| Age visit 1, years | 53.0 ± 15.5 | 53.3 ± 15.2 | 52.7 ± 16.0 | 0.60 |
| Weight, kg | 79.3 ± 14.2 | 85.7 ± 11.9 | 72.3 ± 13.2 | <0.001 |
| BMI, kg/m2 | 26.0 ± 4.0 | 26.3 ± 3.4 | 25.8 ± 4.6 | 0.08 |
| Smoking, yes (%) | 115 (15.0%) | 68 (16.8%) | 47 (12.9%) | 0.13 |
| SBP, mmHg | 126.5 ± 17.0 | 129.5 ± 15.1 | 123.1 ± 18.2 | <0.001 |
| DBP, mmHg | 73.7 ± 9.7 | 76.6 ± 9.8 | 70.5 ± 8.4 | <0.001 |
| Laboratory measurements | ||||
| Total Cholesterol, mmol/L | 5.2 ± 1.0 | 5.1 ± 1.0 | 5.3 ± 1.1 | 0.03 |
| HDL cholesterol, mmol/L | 1.5 ± 0.4 | 1.3 ± 0.3 | 1.7 ± 0.4 | <0.001 |
| LDL cholesterol, mmol/L | 3.3 ± 0.9 | 3.3 ± 0.9 | 3.3 ± 1.0 | 0.27 |
| Total Triglycerides, mmol/L | 1.0 (0.8–1.5) | 1.2 (0.9–1.6) | 1.0 (0.7–1.3) | <0.001 |
| Total TG/HDL-c ratio | 0.72 (0.45–1.17) | 0.92 (0.60–1.43) | 0.56 (0.38–0.88) | <0.001 |
| Glucose, mmol/L | 5.1 ± 0.7 | 5.2 ± 0.6 | 5.0 ± 0.7 | 0.003 |
| HbA1c, % | 5.6 ± 0.4 | 5.6 ± 0.4 | 5.6 ± 0.4 | 0.99 |
| Creatinine, umol/L | 76.0 ± 13.6 | 83.6 ± 12.3 | 67.6 ± 9.3 | <0.001 |
| Hs-CRP, mg/L 1 | 1.0 (0.5–2.2) | 0.9 (0.4–1.9) | 1.1 (0.5–2.9) | 0.05 |
| Uric acid, mmol/L 1 | 0.31 ± 0.1 | 0.34 ± 0.1 | 0.28 ± 0.1 | <0.001 |
| Dietary intake (FFQ) | ||||
| Energy intake, Kcal/day | 1971 ± 624 | 2206 ± 665 | 1711 ± 449 | <0.001 |
| Total carbohydrates, g/day | 228.8 ± 76.7 | 254.4 ± 80.7 | 200.4 ± 60.6 | <0.001 |
| Total carbohydrates, En% | 46.4 ± 6.0 | 46.2 ± 5.7 | 46.7 ± 6.2 | 0.08 |
| Total protein, g/day | 74.8 ± 20.9 | 81.5 ± 22.6 | 67.3 ± 15.8 | <0.001 |
| Total protein, En% | 15.5 ± 2.4 | 15.0 ± 2.1 | 16.0 ± 2.6 | 0.05 |
| Total fat, g/day | 77.2 ± 30.0 | 87.1 ± 32.7 | 66.2 ± 22.0 | <0.001 |
| Total fat, En% | 34.9 ± 5.1 | 35.1 ± 5.0 | 34.6 ± 5.1 | 0.82 |
| Total Dairy intake, g/day | 322 (209–447) | 315 (202–444) | 324 (216–447) | 0.99 |
| Total Dairy fat intake, g/day | 12.3 (8.4–17.4) | 13.5 (9.0–18.3) | 11.3 (8.0–15.6) | <0.001 |
| Total Dairy fat intake (En%) | 6.0 (4.3–7.8) | 5.7 (3.4–7.4) | 6.2 (4.5–8.1) | 0.90 |
| Total Fish intake, g/day | 11.7 (5.6–17.5) | 12.0 (6.8–17.4) | 11.6 (5.2–17.5) | 0.87 |
| Total Fish fat intake, g/day | 1.14 (0.53–1.75) | 1.16 (0.58–1.74) | 1.10 (0.48–1.77) | 0.50 |
| Total Fish fat intake (En%) | 0.52 (0.24–0.88) | 0.49 (0.23–0.77) | 0.57 (0.26–1.01) | 0.01 |
| Fatty acid status in plasma TG | ||||
| Myristic acid, mol% | 1.87 (1.40–2.48) | 1.98 (1.49–2.68) | 1.74 (1.35–2.35) | <0.001 |
| Pentadecanoic acid, mol% | 0.30 (0.25–0.35) | 0.29 (0.24–0.35) | 0.30 (0.25–0.35) | 0.27 |
| Heptadecanoic acid, mol% | 0.49 (0.41–0.59) | 0.48 (0.39–0.58) | 0.52 (0.44–0.62) | <0.001 |
| Trans-Palmitoleic acid, mol% | 0.03 (0.02–0.04) | 0.03 (0.02–0.04) | 0.03 (0.02–0.04) | 0.05 |
| Vaccenic acid, mol% | 0.10 (0.06–0.14) | 0.10 (0.07–0.15) | 0.10 (0.07–0.14) | 0.30 |
| Conjugated Linoleic acid, mol% | 0.08 (0.05–0.10) | 0.07 (0.05–0.10) | 0.07 (0.05–0.10) | 0.24 |
| Fatty acid status in plasma PL | ||||
| Myristic acid, mol% | 0.49 (0.41–0.57) | 0.47 (0.40–0.55) | 0.50 (0.43–0.58) | <0.001 |
| Pentadecanoic acid, mol% | 0.28 (0.24–0.33) | 0.28 (0.24–0.33) | 0.29 (0.25–0.33) | 0.09 |
| Heptadecanoic acid, mol% | 0.40 (0.36–0.44) | 0.39 (0.35–0.44) | 0.40 (0.36–0.45) | 0.08 |
| Trans-Palmitoleic acid, mol% | 0.02 (0.01–0.03) | 0.02 (0.01–0.02) | 0.02 (0.02–0.03) | 0.002 |
| Vaccenic acid, mol% | 0.09 (0.07–0.12) | 0.09 (0.06–0.11) | 0.09 (0.07–0.12) | 0.002 |
| Conjugated Linoleic acid, mol% | 0.03 (0.02–0.04) | 0.03 (0.02–0.04) | 0.03 (0.02–0.04) | 0.01 |
| Dependent Variable | C14:0 | C15:0 | C17:0 | Trans-C16:1 (n-7) | Trans-C18:1 (n-7) | CLA | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | |
| Age (years) | 0.063 | 0.071 * | −0.027 | 0.022 | 0.088 * | 0.047 | ||||||
| Sex | −0.129 *** | 0.023 | 0.152 *** | 0.066 | −0.058 | 0.037 | ||||||
| Weight (kg) | 0.132 *** | 0.070 * | −0.091 * | −0.083 * | −0.187 *** | −0.117 *** | −0.073 | −0.043 | 0.030 | 0.000 | −0.024 | −0.008 |
| Waist circumference | 0.146 *** | 0.084 * | −0.096 * | −0.112 *** | −0.201 *** | −0.144 *** | −0.076 | −0.061 | 0.048 | 0.000 | −0.020 | −0.022 |
| BMI (kg/m2) | 0.091 * | 0.071 * | −0.117 ** | −0.132 *** | −0.181 *** | −0.170 *** | −0.073 | −0.075 | −0.008 | −0.031 | −0.022 | −0.030 |
| SBP (mmHg) | 0.075 * | 0.024 | −0.042 | −0.069 * | −0.103 * | −0.064 * | −0.049 | −0.047 | 0.019 | −0.031 | −0.043 | −0.057 |
| DBP (mmHg) | 0.128 *** | 0.068 * | −0.053 | −0.070 * | −0.147 *** | −0.093 * | −0.028 | −0.015 | 0.054 | 0.005 | 0.014 | 0.010 |
| Total C (mmol/L) | 0.152 *** | 0.147 *** | 0.000 | −0.024 | −0.296 *** | −0.308 *** | 0.051 | 0.039 | 0.128 *** | 0.108 ** | 0.079 * | 0.062 |
| HDL-c (mmol/L) | −0.262 *** | −0.213 *** | −0.035 | −0.052 | 0.220 *** | 0.157 *** | 0.051 | 0.019 | −0.060 | −0.041 | −0.057 | −0.078 * |
| LDL-c (mmol/L) | 0.172 *** | 0.154 *** | 0.017 | −0.001 | −0.277 *** | −0.270 *** | 0.029 | 0.025 | 0.119 ** | 0.095 * | 0.070 * | 0.059 |
| Total TG | 0.401 *** | 0.370 *** | −0.012 | −0.018 | −0.563 *** | −0.537 *** | −0.077 | −0.066 | 0.127 *** | 0.103 ** | 0.124 ** | 0.126 *** |
| TG/HDL-c ratio | 0.396 *** | 0.354 *** | 0.003 | 0.005 | −0.503 *** | −0.459 *** | −0.076 | −0.055 | 0.120 ** | 0.095 ** | 0.114 ** | 0.123 *** |
| Glucose (mmol/L) | 0.136 *** | 0.104 ** | −0.031 | −0.054 | −0.128 ** | −0.105 ** | −0.031 | −0.033 | 0.063 | 0.026 | 0.019 | 0.006 |
| HbA1c (%) | 0.119** | 0.088 * | −0.002 | −0.041 | −0.040 | −0.027 | −0.018 | −0.031 | 0.041 | −0.006 | −0.014 | −0.040 |
| Hs-CRP (mg/L) 1 | 0.021 | 0.039 | −0.109 * | −0.118 * | −0.168 ** | −0.203 *** | −0.057 | −0.076 | −0.063 | −0.057 | −0.019 | −0.027 |
| Creatinine (umol/L) | 0.100 * | 0.016 | −0.029 | −0.025 | −0.147 *** | −0.055 | −0.016 | 0.020 | 0.052 | 0.005 | −0.011 | 0.005 |
| Uric acid (mmol/L) 1 | 0.131 * | 0.082 | −0.139 * | −0.160 *** | −0.249 *** | −0.233 *** | −0.096 | −0.123 * | −0.087 | −0.108 * | −0.042 | −0.038 |
| Ureum (mmol/L) 1 | 0.031 | 0.007 | 0.146 ** | 0.122 * | 0.090 | 0.086 | 0.113 | 0.096 | 0.150 ** | 0.137 ** | 0.105 * | 0.080 |
| Dependent Variable | C14:0 | C15:0 | C17:0 | Trans-C16:1 (n-7) | Trans-C18:1 (n-7) | CLA | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | |
| Age (years) | 0.071 * | 0.070 * | 0.078 * | 0.008 | 0.071 * | 0.061 | ||||||
| Sex | 0.141 *** | 0.066 | 0.063 | 0.110 ** | 0.102 * | 0.103 ** | ||||||
| Weight (kg) | −0.071 * | −0.008 | −0.084 * | −0.056 | −0.173 *** | −0.148 *** | −0.071 * | −0.020 | −0.114 ** | −0.069 * | −0.046 | 0.000 |
| Waist circumference | −0.037 | −0.012 | −0.092 * | −0.094 ** | −0.176 *** | −0.182 *** | −0.102 ** | −0.068 * | −0.102 * | −0.092 ** | −0.040 | −0.025 |
| BMI (kg/m2) | −0.022 | −0.030 | −0.057 | −0.069 * | −0.170 *** | −0.185 *** | −0.069 | −0.065 | −0.107 ** | −0.119 ** | −0.037 | −0.044 |
| SBP (mmHg) | −0.029 | −0.036 | −0.024 | −0.044 | −0.045 | −0.069 * | −0.078 * | −0.062 * | −0.081 * | −0.095 ** | 0.055 | −0.064 * |
| DBP (mmHg) | −0.029 | −0.010 | −0.063 | −0.068 * | −0.121 ** | −0.130 *** | −0.075 * | −0.044 | −0.072 * | −0.066 * | −0.003 | 0.008 |
| Total C (mmol/L) | 0.153 *** | 0.123 *** | −0.058 | −0.085 * | −0.212 *** | −0.243 *** | −0.034 | −0.047 | 0.047 | 0.017 | 0.173 *** | 0.148 *** |
| HDL-c (mmol/L) | 0.068 | −0.001 | 0.072 * | 0.036 | −0.015 | −0.050 | 0.053 | 0.003 | 0.093 * | 0.042 | 0.084 * | 0.033 |
| LDL-c (mmol/L) | 0.137 *** | 0.127 *** | −0.054 | −0.071 * | −0.157 *** | −0.178 *** | −0.022 | −0.021 | 0.033 | 0.018 | 0.121 ** | 0.110 ** |
| Total TG | 0.018 | 0.040 | −0.155 *** | −0.153 *** | −0.235 *** | −0.235 *** | −0.151 *** | −0.130 *** | −0.098 * | −0.088 * | 0.091 * | 0.106 ** |
| TG/HDL-c ratio | −0.015 | 0.028 | −0.142 *** | −0.127 *** | −0.169 *** | −0.135 *** | −0.131 *** | −0.095 ** | −0.108 ** | −0.080 * | 0.033 | 0.064 |
| Glucose (mmol/L) | 0.033 | 0.025 | −0.048 | −0.065 | −0.100 * | −0.121 *** | −0.035 | −0.027 | −0.077 * | −0.095 * | −0.036 | −0.048 |
| HbA1c (%) | 0.014 | −0.027 | −0.001 | −0.040 | −0.008 | −0.052 | −0.023 | −0.029 | −0.057 | −0.099 ** | 0.006 | −0.029 |
| Hs-CRP (mg/L) 1 | −0.030 | −0.055 | −0.074 | −0.087 | −0.223 *** | −0.233 *** | −0.089 | −0.117 * | −0.160 ** | −0.179 *** | 0.023 | 0.005 |
| Creatinine (umol/L) | −0.112 ** | −0.040 | −0.029 | 0.000 | −0.107 ** | −0.082 * | −0.059 | 0.005 | −0.093 * | −0.044 | −0.062 | −0.010 |
| Uric acid (mmol/L) 1 | −0.140 * | −0.096 | −0.157 ** | −0.130 * | −0.270 *** | −0.258 *** | −0.140 * | −0.131 * | −0.243 *** | −0.208 *** | −0.029 | −0.065 |
| Ureum (mmol/L) 1 | 0.021 | 0.007 | 0.188 *** | 0.186 | 0.109 * | 0.089 | 0.097 | 0.096 | 0.105 * | 0.099 | 0.032 | 0.026 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pranger, I.G.; Muskiet, F.A.J.; Kema, I.P.; Singh-Povel, C.; Bakker, S.J.L. Potential Biomarkers for Fat from Dairy and Fish and Their Association with Cardiovascular Risk Factors: Cross-sectional Data from the LifeLines Biobank and Cohort Study. Nutrients 2019, 11, 1099. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11051099
Pranger IG, Muskiet FAJ, Kema IP, Singh-Povel C, Bakker SJL. Potential Biomarkers for Fat from Dairy and Fish and Their Association with Cardiovascular Risk Factors: Cross-sectional Data from the LifeLines Biobank and Cohort Study. Nutrients. 2019; 11(5):1099. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11051099
Chicago/Turabian StylePranger, Ilse G., Frits A. J. Muskiet, Ido P. Kema, Cécile Singh-Povel, and Stephan J. L. Bakker. 2019. "Potential Biomarkers for Fat from Dairy and Fish and Their Association with Cardiovascular Risk Factors: Cross-sectional Data from the LifeLines Biobank and Cohort Study" Nutrients 11, no. 5: 1099. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11051099