A Novel Nutritional Index Serves as A Useful Prognostic Indicator in Cardiac Critical Patients Requiring Mechanical Circulatory Support

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Population and Follow-Up Period
2.2. Endpoints
2.3. Nutritional Indices, GNRI, and TCBI
(height (cm) − 100) − (height (cm) − 150)/2
2.4. Statistical Analysis
3. Results
3.1. Baseline Patient Demographics in Tertiles of TCBI
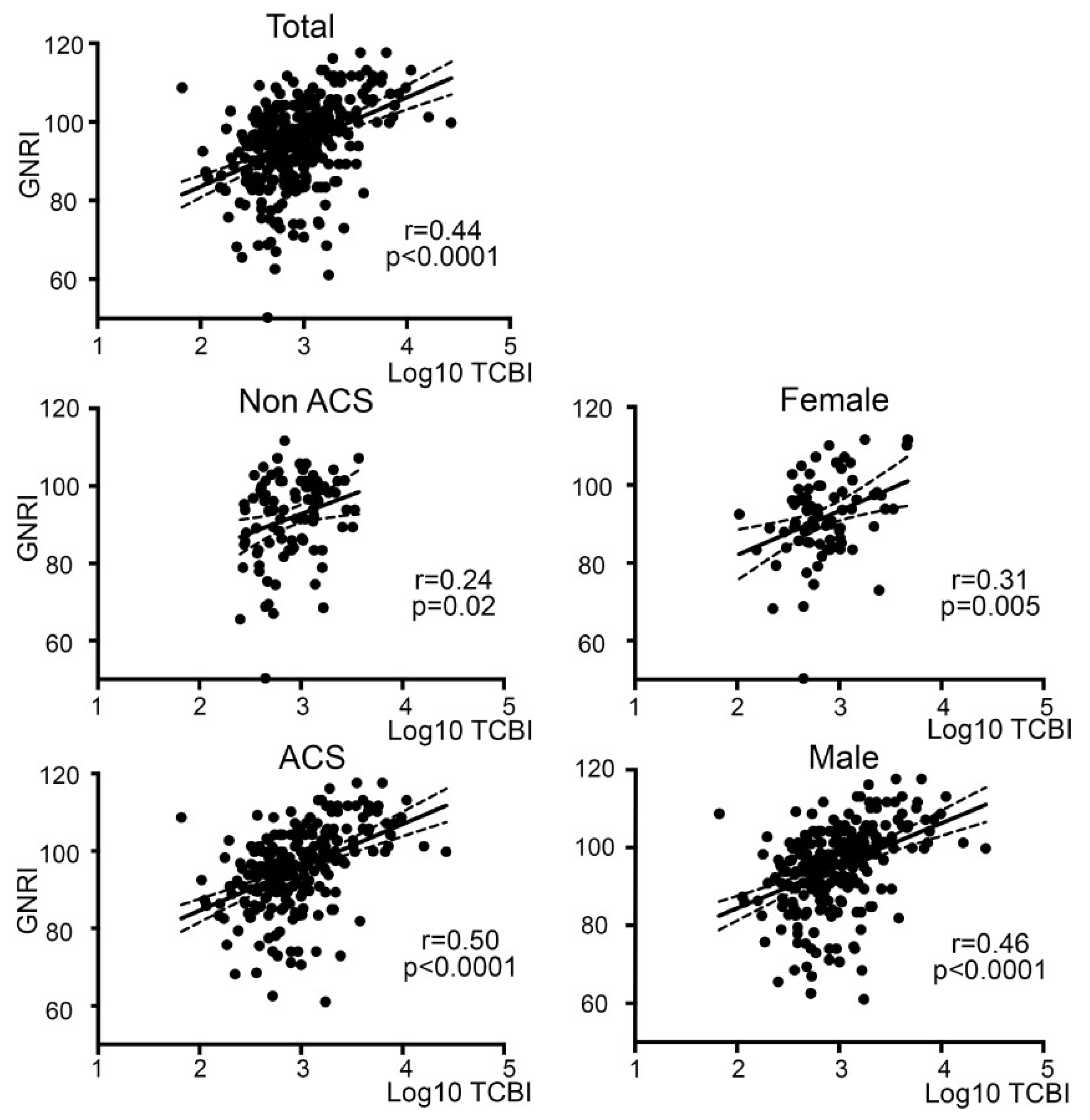
3.2. Linear Positive Correlation of TCBI with GNRI
3.3. Nutritional Status Was Poorer in the Patient Population with More Severe Cardiovascular Diseases
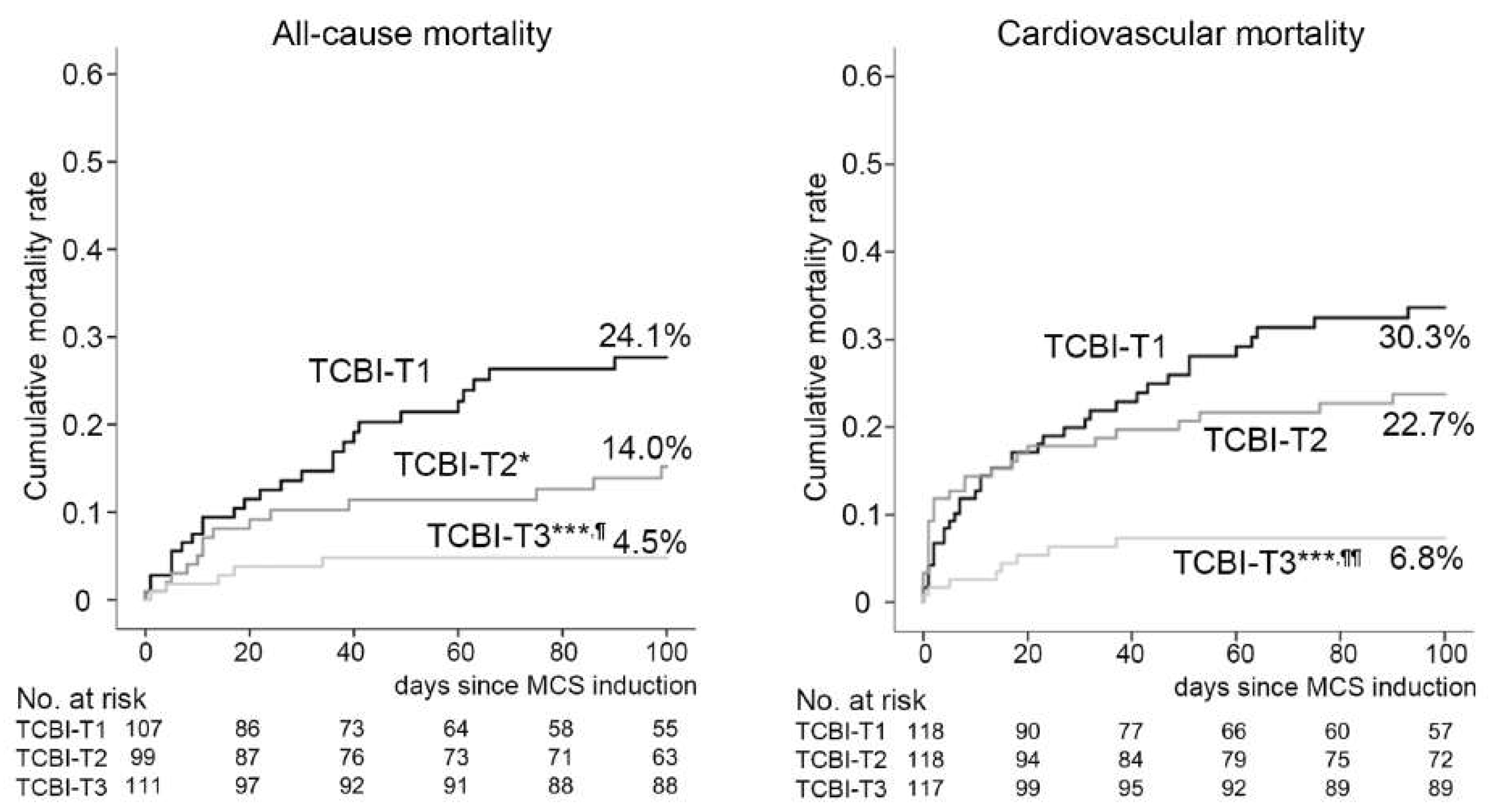
3.4. Higher TCBI Was Associated with Lower Incidences of All-Cause and Cardiovascular Mortalities in Unadjusted Kaplan–Meier Analyses
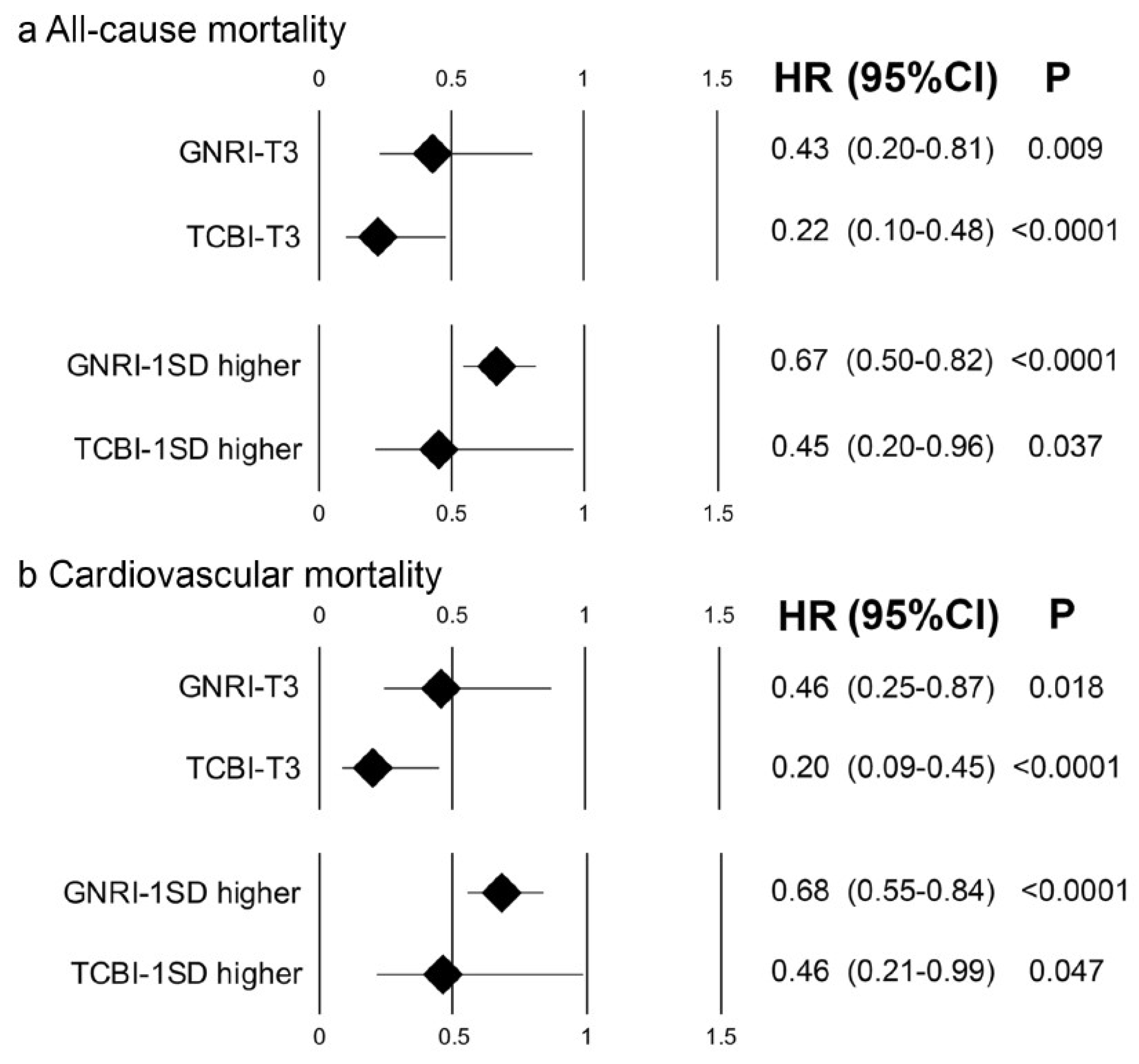
3.5. Lower Risk of All-Cause and Cardiovascular Mortality in Patients with Higher TCBI
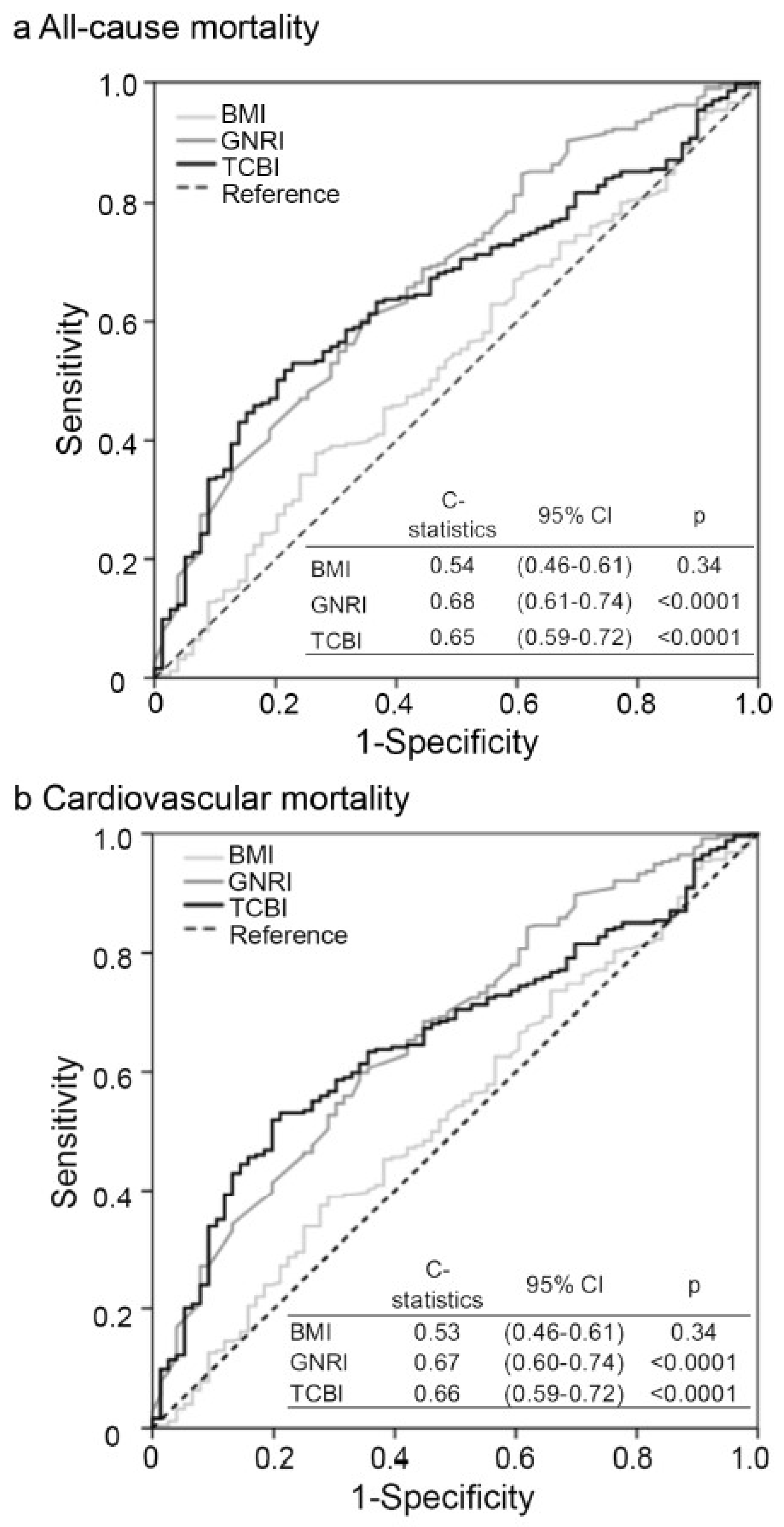
3.6. Comparable Prognostic Implication of TCBI for All-Cause and Cardiovascular Mortalities with GNRI
3.7. Higher TCBI Was Associated with Lower All-Cause Mortality after the Adjustment with Markers of Organ Function
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ICU | intensive care unit |
| MCS | mechanical circulatory support |
| IABP | intra-aortic balloon pumping |
| VA-ECMO | veno-arterial extracorporeal membrane oxygenation |
| TG | triglycerides |
| TC | total cholesterol |
| BW | body weight |
| TCBI | Triglycerides-total Cholesterol-Body weight-Index |
| GNRI | Geriatric nutritional risk index |
References
- Lew, C.C.H.; Yandell, R.; Fraser, R.J.L.; Chua, A.P.; Chong, M.F.F.; Miller, M. Association Between Malnutrition and Clinical Outcomes in the Intensive Care Unit: A Systematic Review. JPEN J. Parenter Enteral Nutr. 2017, 41, 744–758. [Google Scholar] [CrossRef] [PubMed]
- Mogensen, K.M.; Robinson, M.K.; Casey, J.D.; Gunasekera, N.S.; Moromizato, T.; Rawn, J.D.; Christopher, K.B. Nutritional Status and Mortality in the Critically Ill. Crit. Care Med. 2015, 43, 2605–2615. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.K.; Mogensen, K.M.; Casey, J.D.; McKane, C.K.; Moromizato, T.; Rawn, J.D.; Christopher, K.B. The relationship among obesity, nutritional status, and mortality in the critically ill. Crit. Care Med. 2015, 43, 87–100. [Google Scholar] [CrossRef] [PubMed]
- Lew, C.C.H.; Wong, G.J.Y.; Cheung, K.P.; Chua, A.P.; Chong, M.F.F.; Miller, M. Association between Malnutrition and 28-Day Mortality and Intensive Care Length-of-Stay in the Critically ill: A Prospective Cohort Study. Nutrients. 2017, 10, 10. [Google Scholar] [CrossRef] [PubMed]
- Kondrup, J.; Allison, S.P.; Elia, M.; Vellas, B.; Plauth, M. Educational, Clinical Practice Committee ESoP and Enteral, N. ESPEN guidelines for nutrition screening 2002. Clin. Nutr. 2003, 22, 415–421. [Google Scholar] [CrossRef]
- Detsky, A.S.; McLaughlin, J.R.; Baker, J.P.; Johnston, N.; Whittaker, S.; Mendelson, R.A.; Jeejeebhoy, K.N. What is subjective global assessment of nutritional status? JPEN J. Parenter Enteral Nutr. 1987, 11, 8–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canada-USA (CANUSA) Peritoneal Dialysis Study Group. Adequacy of dialysis and nutrition in continuous peritoneal dialysis: Association with clinical outcomes. J. Am. Soc. Nephrol. 1996, 7, 198–207. [Google Scholar]
- Stratton, R.J.; Hackston, A.; Longmore, D.; Dixon, R.; Price, S.; Stroud, M.; King, C.; Elia, M. Malnutrition in hospital outpatients and inpatients: Prevalence, concurrent validity and ease of use of the ‘malnutrition universal screening tool’ (‘MUST’) for adults. Br. J. Nutr. 2004, 92, 799–808. [Google Scholar] [CrossRef]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef]
- Ignacio de Ulibarri, J.; Gonzalez-Madrono, A.; de Villar, N.G.; Gonzalez, P.; Gonzalez, B.; Mancha, A.; Rodriguez, F.; Fernandez, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar]
- Alvares-da-Silva, M.R.; Reverbel da Silveira, T. Comparison between handgrip strength, subjective global assessment, and prognostic nutritional index in assessing malnutrition and predicting clinical outcome in cirrhotic outpatients. Nutrition 2005, 21, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Luo, L.; Zhao, X.; Ye, P. Controlling Nutritional Status (CONUT) score as a predictor of all-cause mortality in elderly hypertensive patients: A prospective follow-up study. BMJ 2017, 7, e015649. [Google Scholar] [CrossRef] [PubMed]
- Wada, H.; Dohi, T.; Miyauchi, K.; Doi, S.; Konishi, H.; Naito, R.; Tsuboi, S.; Ogita, M.; Kasai, T.; Okazaki, S.; et al. Prognostic impact of nutritional status assessed by the Controlling Nutritional Status score in patients with stable coronary artery disease undergoing percutaneous coronary intervention. Clin. Res. Cardiol. 2017, 106, 875–883. [Google Scholar] [CrossRef] [PubMed]
- Yoshihisa, A.; Kanno, Y.; Watanabe, S.; Yokokawa, T.; Abe, S.; Miyata, M.; Sato, T.; Suzuki, S.; Oikawa, M.; Kobayashi, A.; et al. Impact of nutritional indices on mortality in patients with heart failure. Open Heart 2018, 5, e000730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonca, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Heyland, D.K.; Dhaliwal, R.; Jiang, X.; Day, A.G. Identifying critically ill patients who benefit the most from nutrition therapy: The development and initial validation of a novel risk assessment tool. Crit. Care. 2011, 15, R268. [Google Scholar] [CrossRef] [PubMed]
- Doi, S.; Iwata, H.; Wada, H.; Funamizu, T.; Shitara, J.; Endo, H.; Naito, R.; Konishi, H.; Tsuboi, S.; Ogita, M.; et al. A novel and simply calculated nutritional index serves as a useful prognostic indicator in patients with coronary artery disease. Int. J. Cardiol. 2018, 262, 92–98. [Google Scholar] [CrossRef]
- Wada, H.; Dohi, T.; Miyauchi, K.; Doi, S.; Naito, R.; Konishi, H.; Tsuboi, S.; Ogita, M.; Kasai, T.; Hassan, A.; et al. Prognostic Impact of the Geriatric Nutritional Risk Index on Long-Term Outcomes in Patients Who Underwent Percutaneous Coronary Intervention. Am. J. Cardiol. 2017, 119, 1740–1745. [Google Scholar] [CrossRef]
- Cho, J.Y.; Kim, K.H.; Cho, H.J.; Lee, H.Y.; Choi, J.O.; Jeon, E.S.; Lee, S.E.; Kim, M.S.; Kim, J.J.; Hwang, K.K.; et al. Nutritional risk index as a predictor of mortality in acutely decompensated heart failure. PLoS ONE 2018, 13, e0209088. [Google Scholar] [CrossRef]
- Yokoyama, M.; Watanabe, T.; Otaki, Y.; Watanabe, K.; Toshima, T.; Sugai, T.; Takahashi, T.; Kinoshita, D.; Tamura, H.; Nishiyama, S.; et al. Impact of Objective Malnutrition Status on the Clinical Outcomes in Patients with Peripheral Artery Disease Following Endovascular Therapy. Circ. J. 2018, 82, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Farhangi, M.A.; Moradi, F.; Najafi, M.; Jafarabadi, M.A. 10-y survival in patients who underwent coronary artery bypass grafting surgery in Tehran Heart Center-Coronary Outcome Measurement Study: The powerful predicting ability of the dietary inflammatory index and dietary antioxidant quality. Nutrition 2019, 63, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Keskin, M.; Ipek, G.; Aldag, M.; Altay, S.; Hayiroglu, M.I.; Borklu, E.B.; Inan, D.; Kozan, O. Effect of nutritional status on mortality in patients undergoing coronary artery bypass grafting. Nutrition 2018, 48, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Wernio, E.; Malgorzewicz, S.; Dardzinska, J.A.; Jagielak, D.; Rogowski, J.; Gruszecka, A.; Klapkowski, A.; Bramlage, P. Association between Nutritional Status and Mortality after Aortic Valve Replacement Procedure in Elderly with Severe Aortic Stenosis. Nutrients 2019, 11, 446. [Google Scholar] [CrossRef] [PubMed]
- Shibata, K.; Yamamoto, M.; Kano, S.; Koyama, Y.; Shimura, T.; Kagase, A.; Yamada, S.; Kobayashi, T.; Tada, N.; Naganuma, T.; et al. Importance of Geriatric Nutritional Risk Index assessment in patients undergoing transcatheter aortic valve replacement. Am. Heart. J. 2018, 202, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Gurm, H.S.; Brennan, D.M.; Booth, J.; Tcheng, J.E.; Lincoff, A.M.; Topol, E.J. Impact of body mass index on outcome after percutaneous coronary intervention (the obesity paradox). Am. J. Cardiol. 2002, 90, 42–45. [Google Scholar] [CrossRef]
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Association of all-cause mortality with overweight and obesity using standard body mass index categories: A systematic review and meta-analysis. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Yang-Giuliano, X.; Osborn, E.A. Paradoxically simple: A new nutritional index for predicting coronary risk. Int. J. Cardiol. 2018, 262, 106–107. [Google Scholar] [CrossRef] [PubMed]
- Nazzari, H.; Chue, C.D.; Toma, M. Mechanical circulatory support in the heart failure population. Curr. Opin. Cardiol. 2019, 34, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Hajjar, L.A.; Teboul, J.L. Mechanical Circulatory Support Devices for Cardiogenic Shock: State of the Art. Crit. Care. 2019, 23, 76. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TCBI T1 (N = 119) | TCBI T2 (N = 119) | TCBI T3 (N = 119) | p-value | |
|---|---|---|---|---|
| Age | 74.9 ± 9.5 | 72.2 ± 10.0 | 64.7 ± 12.0 | <0.001 |
| Gender, male | 85, 71.4% | 88, 74.0% | 103, 86.6% | 0.010 |
| Body mass index, kg/m2 | 21.6 ± 3.2 | 22.7 ± 3.5 | 25.7 ± 4.2 | <0.001 |
| Systolic blood pressure, mm Hg | 96.7 ± 30.8 | 102.3 ± 32.1 | 110.7 ± 29.4 | 0.003 |
| Heart Rate, beats per minute | 86.5 ± 26.4 | 88.7 ± 23.6 | 88.0 ± 22.6 | 0.780 |
| Dyslipidemia | 42, 35.3% | 47, 39.5% | 99, 83.2% | <0.001 |
| Chronic kidney disease (Grade 3–5) | 71, 60.0% | 74, 62.2% | 46, 38.7% | <0.001 |
| eGFR, mL/min/1.732 | 49.5 ± 29.0 | 53 ± 28.4 | 66.8 ± 24.8 | <0.001 |
| Diabetes | 30, 25.9% | 28, 23.9% | 50, 42.0% | 0.005 |
| CRP, mg/dL | 0.50 (0.30–2.40) | 0.40 (0.30–1.65) | 0.30 (0.30–0.60) | 0.127 |
| Serum Albumin, g/dL | 3.4 ± 0.7 | 3.6 ± 0.5 | 3.9 ± 0.7 | <0.001 |
| GNRI | 89.6 ± 10.6 | 94 ± 8.4 | 99.6 ± 10.4 | <0.001 |
| Cause of MCS indication | ||||
| Acute coronary syndrome | 88, 74.0% | 87, 73.1% | 96, 80.1% | 0.347 |
| Cardiogenic shock | 15, 12.6% | 7, 5.9% | 17, 14.3% | 0.086 |
| IABP use | 119, 100% | 119, 100% | 119, 100% | 1 |
| V-A ECMO use | 20, 17.0% | 18, 15.3% | 17, 14.3% | 0.839 |
| Lipid parameters | ||||
| HDL-C, mg/dL | 46.6 ± 14.7 | 47.9 ± 15.5 | 43.2 ± 12.2 | 0.035 |
| LDL-C, mg/dL | 84.3 ± 30.9 | 111.0 ± 34.8 | 132.4 ± 43.4 | <0.001 |
| Total cholesterol, mg/dL | 142.5 ± 40.7 | 178.8 ± 36.3 | 209.8 ± 52.4 | <0.001 |
| Triglycerides, mg/dL | 48 (38–61) | 80 (68–100) | 151 (119–209) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minami-Takano, A.; Iwata, H.; Miyosawa, K.; Kubota, K.; Kimura, A.; Osawa, S.; Shitara, M.; Okazaki, S.; Suwa, S.; Miyauchi, K.; et al. A Novel Nutritional Index Serves as A Useful Prognostic Indicator in Cardiac Critical Patients Requiring Mechanical Circulatory Support. Nutrients 2019, 11, 1420. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11061420
Minami-Takano A, Iwata H, Miyosawa K, Kubota K, Kimura A, Osawa S, Shitara M, Okazaki S, Suwa S, Miyauchi K, et al. A Novel Nutritional Index Serves as A Useful Prognostic Indicator in Cardiac Critical Patients Requiring Mechanical Circulatory Support. Nutrients. 2019; 11(6):1420. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11061420
Chicago/Turabian StyleMinami-Takano, Asuka, Hiroshi Iwata, Katsutoshi Miyosawa, Kyoko Kubota, Atsushi Kimura, Shota Osawa, Minako Shitara, Shinya Okazaki, Satoru Suwa, Katsumi Miyauchi, and et al. 2019. "A Novel Nutritional Index Serves as A Useful Prognostic Indicator in Cardiac Critical Patients Requiring Mechanical Circulatory Support" Nutrients 11, no. 6: 1420. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11061420