Rectal Cancer: 20% Risk Reduction Thanks to Dietary Fibre Intake. Systematic Review and Meta-Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Inclusion/Exclusion Criteria
2.2. Data Extraction
2.3. Quality Evaluation
2.4. Statistical Analysis
2.5. Sub-Group and Sensitivity Analysis
2.6. Cumulative Analysis
2.7. Moderator Analysis
3. Results
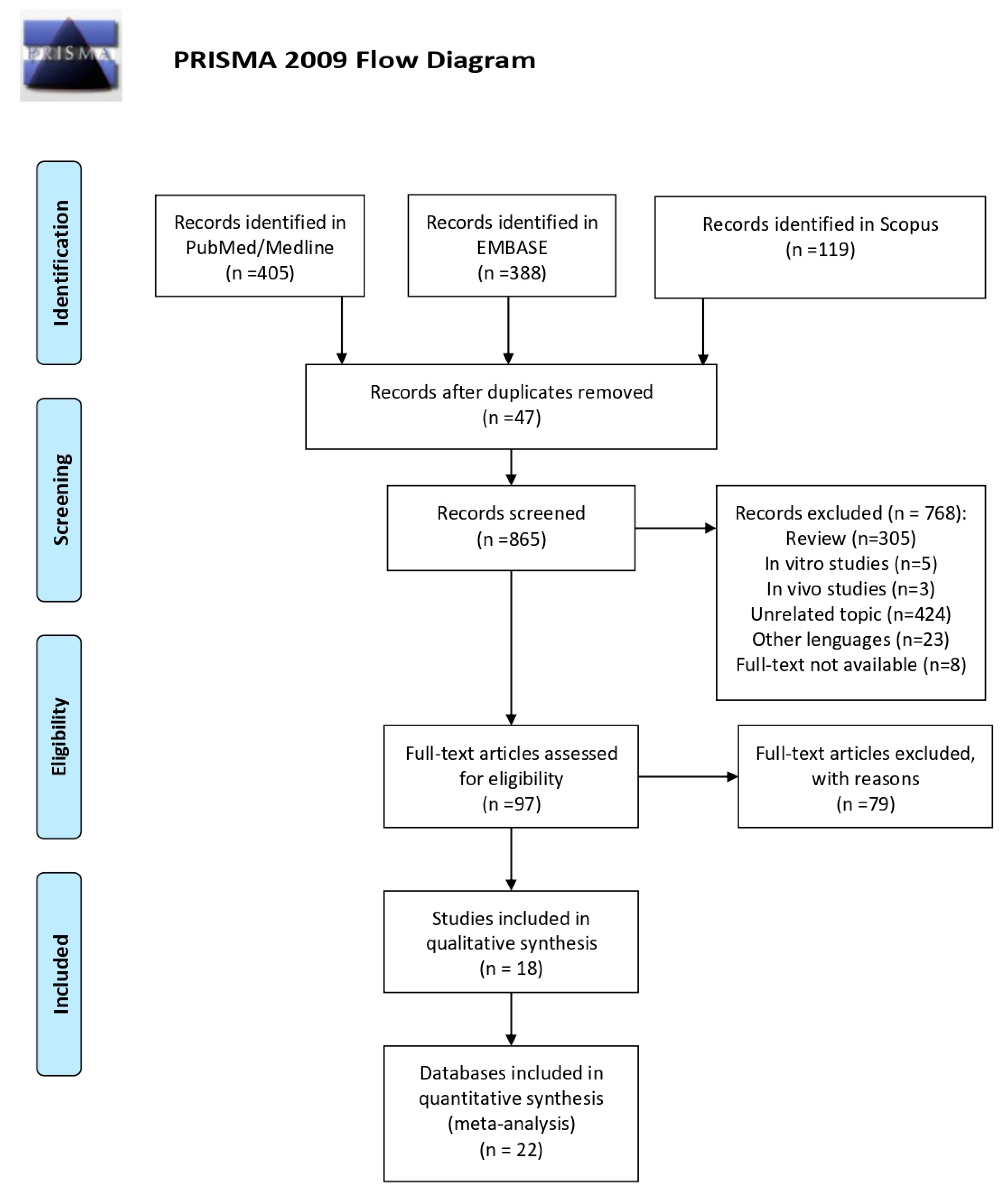
3.1. Literature Search
3.2. Characteristics of Included Studies
3.3. Sensitivity Analysis
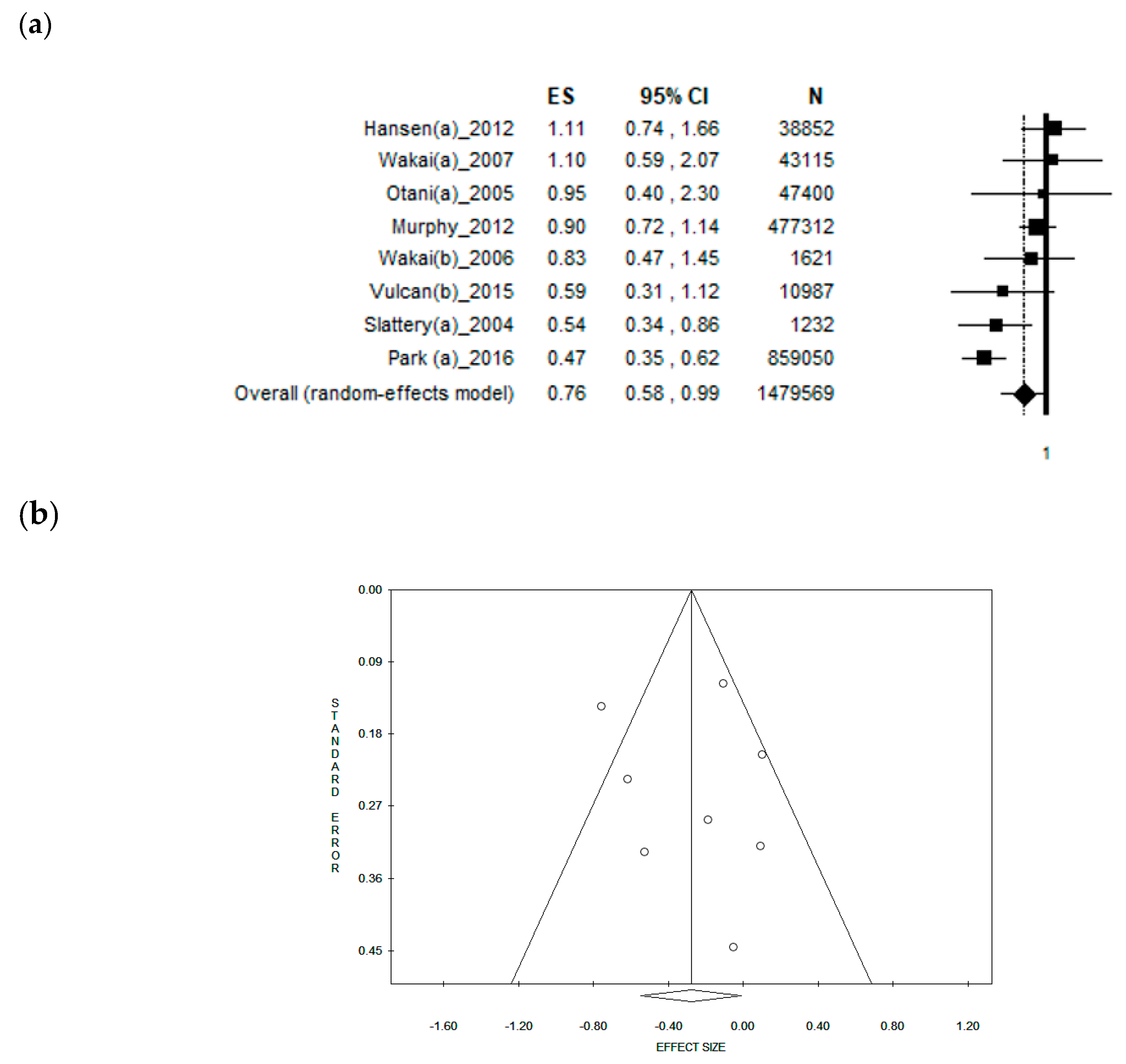
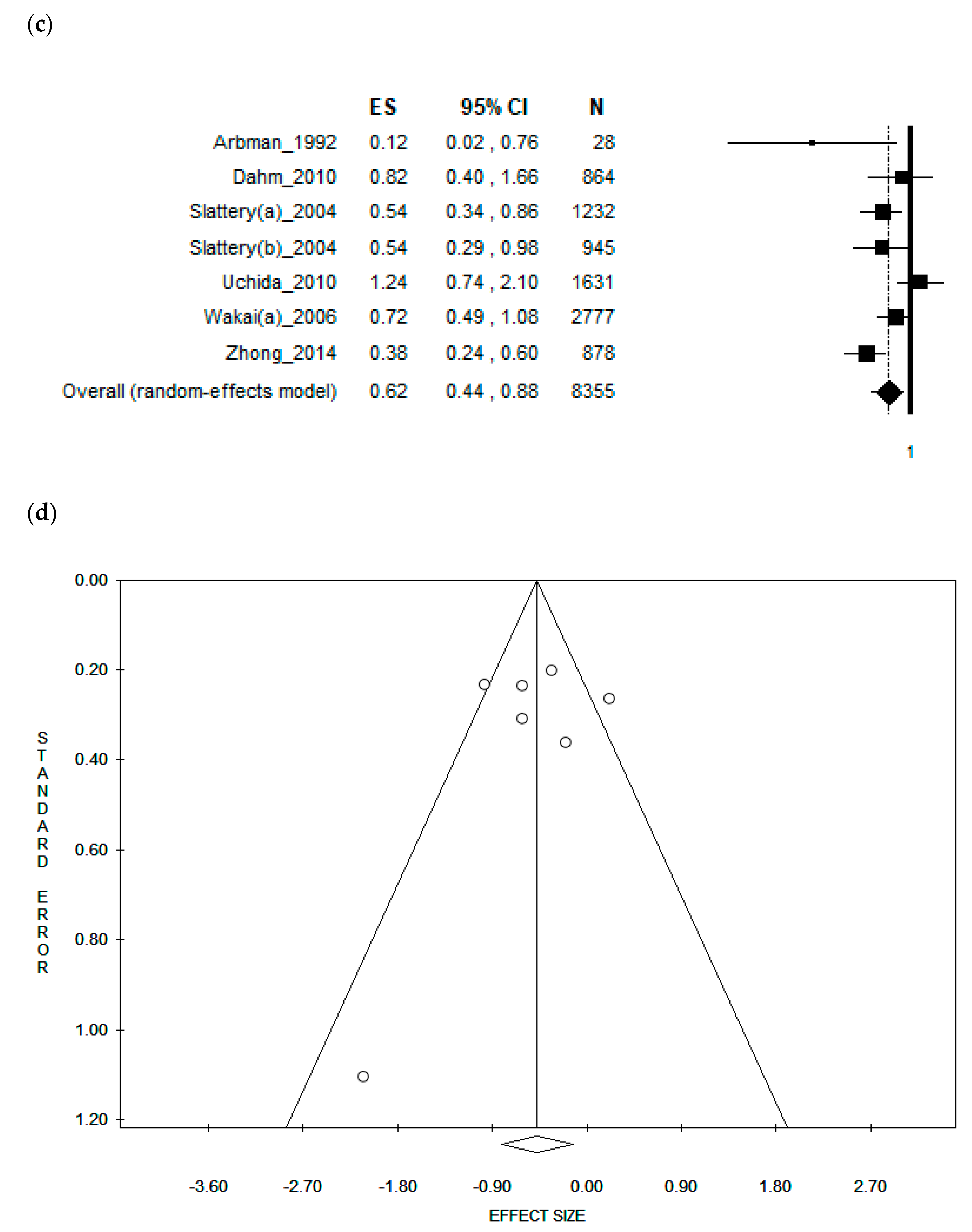
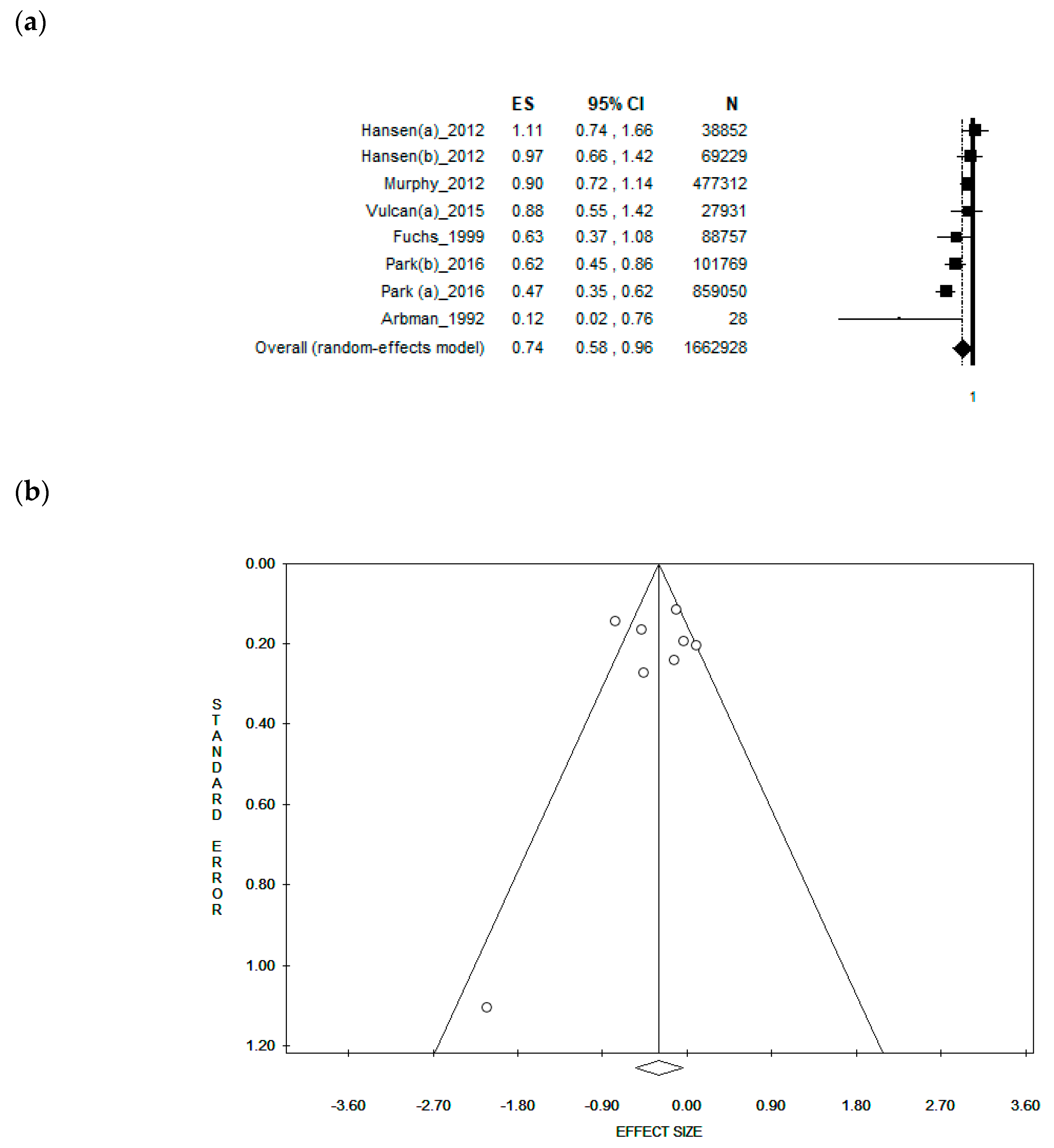
3.4. Sub-Group Analysis by Gender
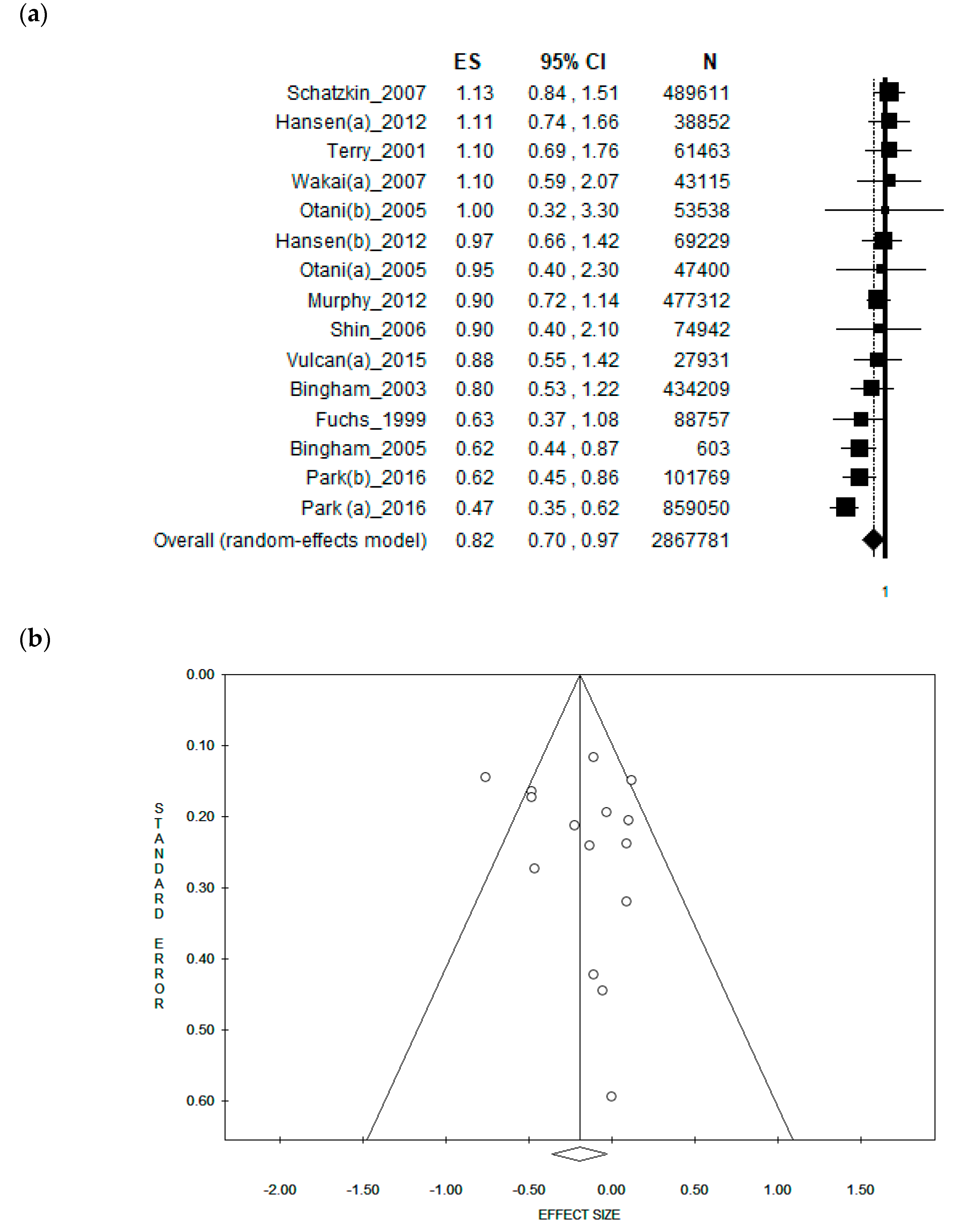
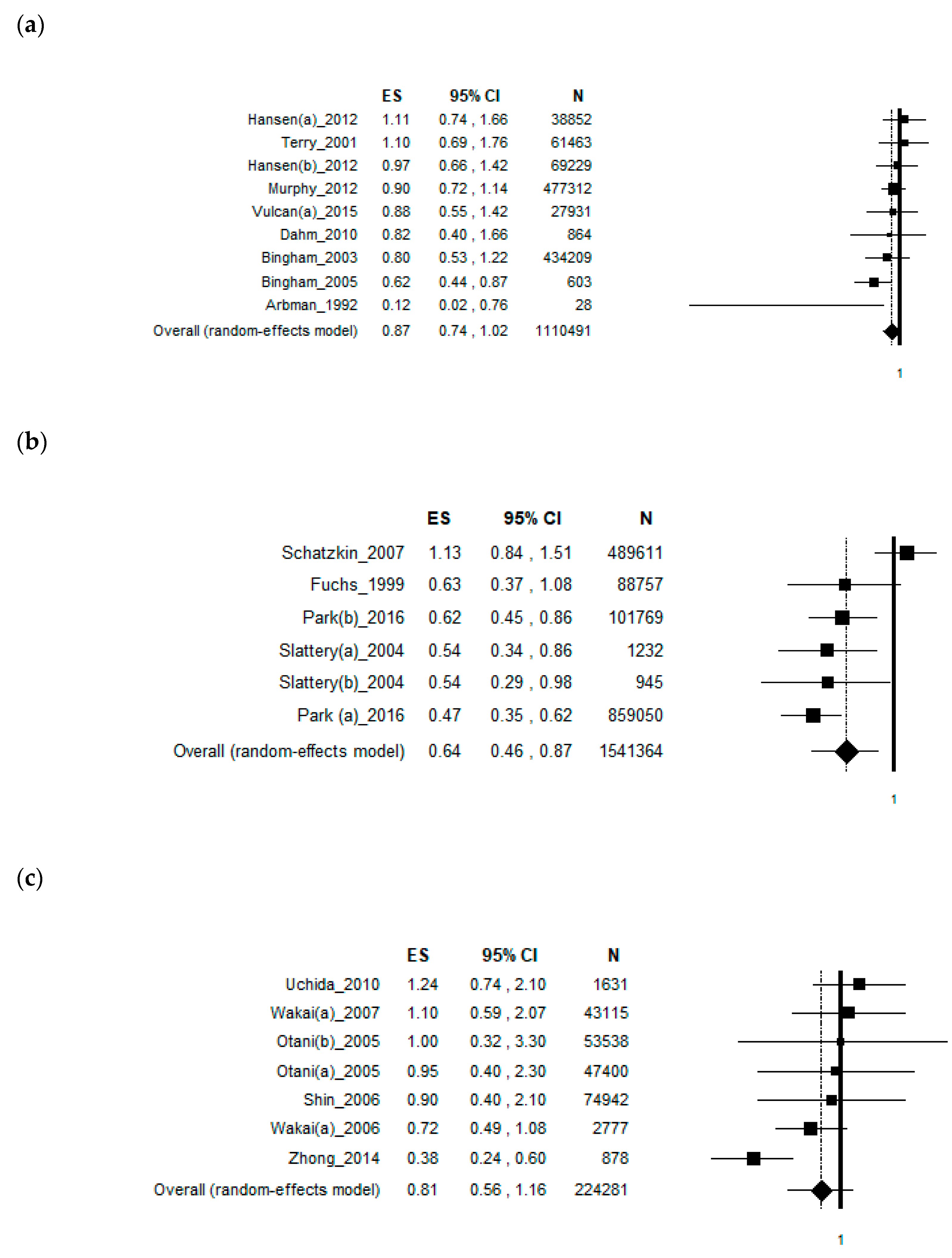
3.5. Sub-Group Analysis by Study Type
3.6. Sub-Group Analysis by Duration of the Studies
3.7. Sub-Group Analysis by Continent
3.8. Cumulative and Moderator Analysis
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Internation Agency for Reseach on Cancer. Colorectum: Factsheet. Available online: https://gco.iarc.fr/today/data/factsheets/populations/900-world-fact-sheets.pdf (accessed on 18 March 2019).
- World Cancer Research Fund International/American Institute for Cancer Research. Countinous Update Project Report: Diet, Nutrition, Physical Activity and Colorectal Cancer; World Cancer Research Fund International/American Institute for Cancer Research: London, UK, 2017. [Google Scholar]
- Moss, A.; Nalankilli, K. The association between diet and colorectal cancer risk: Moving beyond generalizations. Gastroenterology 2017, 152, 1821–1823. [Google Scholar] [CrossRef] [PubMed]
- Farinetti, A.; Zurlo, V.; Manenti, A.; Coppi, F.; Mattioli, A.V. Mediterranean diet and colorectal cancer: A systematic review. Nutrition 2017, 43, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Zamora-Ros, R.; Barupal, D.K.; Rothwell, J.A.; Jenab, M.; Fedirko, V.; Romieu, I.; Aleksandrova, K.; Overvad, K.; Kyro, C.; Tjonneland, A.; et al. Dietary flavonoid intake and colorectal cancer risk in the European prospective investigation into cancer and nutrition (EPIC) cohort. Int. J. Cancer 2017, 140, 1836–1844. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Salvatori, T.; Villarini, M.; Moretti, M.; Nucci, D.; Realdon, S. Is dietary fibre truly protective against colon cancer? A systematic review and meta-analysis. Int. J. Food Sci. Nutr. 2018, 69, 904–915. [Google Scholar] [CrossRef] [PubMed]
- Gaertner, W.B.; Kwaan, M.R.; Madoff, R.D.; Melton, G.B. Rectal cancer: An evidence-based update for primary care providers. World J. Gastroenterol. 2015, 21, 7659–7671. [Google Scholar] [CrossRef] [PubMed]
- Nogacka, A.M.; Gomez-Martin, M.; Suarez, A.; Gonzalez-Bernardo, O.; de Los Reyes-Gavilan, C.G.; Gonzalez, S. Xenobiotics formed during food processing: Their relation with the intestinal microbiota and colorectal cancer. Int. J. Mol. Sci. 2019, 20, 2051. [Google Scholar] [CrossRef] [PubMed]
- Bindels, L.B.; Delzenne, N.M.; Cani, P.D.; Walter, J. Towards a more comprehensive concept for prebiotics. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 303–310. [Google Scholar] [CrossRef]
- Slattery, M.L.; Curtin, K.P.; Edwards, S.L.; Schaffer, D.M. Plant foods, fiber, and rectal cancer. Am. J. Clin. Nutr. 2004, 79, 274–281. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.; Brunnhuber, K.; Chalkidou, K.; Chalmers, I.; Clarke, M.; Fenton, M.; Forbes, C.; Glanville, J.; Hicks, N.J.; Moody, J.; et al. How to formulate research recommendations. BMJ 2006, 333, 804–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0.; The Cochrane Collaboration: London, UK, 2013. [Google Scholar]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duval, S.; Tweedie, R. A nonparametric “Trim and Fill” method of accounting for publication bias in meta-analysis. J. Am. Stat. Assoc. 2000, 95, 89–98. [Google Scholar] [CrossRef]
- Leimu, R.; Koricheva, J. Cumulative meta-analysis: A new tool for detection of temporal trends and publication bias in ecology. Proc. Biol. Sci. 2004, 271, 1961–1966. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Wilkens, L.R.; Kolonel, L.N.; Henderson, B.E.; Le Marchand, L. Inverse associations of dietary fiber and menopausal hormone therapy with colorectal cancer risk in the multiethnic cohort study. Int. J. Cancer 2016, 139, 1241–1250. [Google Scholar] [CrossRef] [PubMed]
- Otani, T.; Iwasaki, M.; Hanaoka, T.; Kobayashi, M.; Ishihara, J.; Natsukawa, S.; Shaura, K.; Koizumi, Y.; Kasuga, Y.; Yoshimura, K.; et al. Folate, vitamin B6, vitamin B12, and vitamin B2 intake, genetic polymorphisms of related enzymes, and risk of colorectal cancer in a hospital-based case-control study in Japan. Nutr. Cancer 2005, 53, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Hansen, L.; Skeie, G.; Landberg, R.; Lund, E.; Palmqvist, R.; Johansson, I.; Dragsted, L.O.; Egeberg, R.; Johnsen, N.F.; Christensen, J.; et al. Intake of dietary fiber, especially from cereal foods, is associated with lower incidence of colon cancer in the HELGA cohort. Int. J. Cancer 2012, 131, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Dahm, C.C.; Keogh, R.H.; Spencer, E.A.; Greenwood, D.C.; Key, T.J.; Fentiman, I.S.; Shipley, M.J.; Brunner, E.J.; Cade, J.E.; Burley, V.J.; et al. Dietary fiber and colorectal cancer risk: A nested case-control study using food diaries. J. Nat. Cancer Inst. 2010, 102, 614–626. [Google Scholar] [CrossRef]
- Arbman, G.; Axelson, O.; Ericsson-Begodzki, A.B.; Fredriksson, M.; Nilsson, E.; Sjodahl, R. Cereal fiber, calcium, and colorectal cancer. Cancer 1992, 69, 2042–2048. [Google Scholar] [CrossRef]
- Terry, P.; Giovannucci, E.; Michels, K.B.; Bergkvist, L.; Hansen, H.; Holmberg, L.; Wolk, A. Fruit, vegetables, dietary fiber, and risk of colorectal cancer. J. Nat. Cancer Inst. 2001, 93, 525–533. [Google Scholar] [CrossRef]
- Vulcan, A.; Brandstedt, J.; Manjer, J.; Jirstrom, K.; Ohlsson, B.; Ericson, U. Fibre intake and incident colorectal cancer depending on fibre source, sex, tumour location and tumour, node, metastasis stage. Br. J. Nutr. 2015, 114, 959–969. [Google Scholar] [CrossRef]
- Bingham, S.A.; Day, N.E.; Luben, R.; Ferrari, P.; Slimani, N.; Norat, T.; Clavel-Chapelon, F.; Kesse, E.; Nieters, A.; Boeing, H.; et al. Dietary fibre in food and protection against colorectal cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC): An observational study. Lancet 2003, 361, 1496–1501. [Google Scholar] [CrossRef]
- Bingham, S.A.; Norat, T.; Moskal, A.; Ferrari, P.; Slimani, N.; Clavel-Chapelon, F.; Kesse, E.; Nieters, A.; Boeing, H.; Tjonneland, A.; et al. Is the association with fiber from foods in colorectal cancer confounded by folate intake? Cancer Epidemiol. Biomark. Prev. 2005, 14, 1552–1556. [Google Scholar] [CrossRef] [PubMed]
- Murphy, N.; Norat, T.; Ferrari, P.; Jenab, M.; Bueno-de-Mesquita, B.; Skeie, G.; Dahm, C.C.; Overvad, K.; Olsen, A.; Tjonneland, A.; et al. Dietary fibre intake and risks of cancers of the colon and rectum in the European prospective investigation into cancer and nutrition (EPIC). PLoS ONE 2012, 7, e39361. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, C.S.; Giovannucci, E.L.; Colditz, G.A.; Hunter, D.J.; Stampfer, M.J.; Rosner, B.; Speizer, F.E.; Willett, W.C. Dietary fiber and the risk of colorectal cancer and adenoma in women. N. Engl. J. Med. 1999, 340, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Schatzkin, A.; Mouw, T.; Park, Y.; Subar, A.F.; Kipnis, V.; Hollenbeck, A.; Leitzmann, M.F.; Thompson, F.E. Dietary fiber and whole-grain consumption in relation to colorectal cancer in the NIH-AARP Diet and Health Study. Am. J. Clin. Nutr. 2007, 85, 1353–1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchida, K.; Kono, S.; Yin, G.; Toyomura, K.; Nagano, J.; Mizoue, T.; Mibu, R.; Tanaka, M.; Kakeji, Y.; Maehara, Y.; et al. Dietary fiber, source foods and colorectal cancer risk: The fukuoka colorectal cancer study. Scand. J. Gastroenterol. 2010, 45, 1223–1231. [Google Scholar] [CrossRef]
- Wakai, K.; Date, C.; Fukui, M.; Tamakoshi, K.; Watanabe, Y.; Hayakawa, N.; Kojima, M.; Kawado, M.; Suzuki, K.; Hashimoto, S.; et al. Dietary fiber and risk of colorectal cancer in the Japan collaborative cohort study. Cancer Epidemiol. Biomark. Prev. 2007, 16, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Wakai, K.; Hirose, K.; Matsuo, K.; Ito, H.; Kuriki, K.; Suzuki, T.; Kato, T.; Hirai, T.; Kanemitsu, Y.; Tajima, K. Dietary risk factors for colon and rectal cancers: A comparative case-control study. J. Epidemiol. 2006, 16, 125–135. [Google Scholar] [CrossRef]
- Shin, A.; Li, H.; Shu, X.O.; Yang, G.; Gao, Y.T.; Zheng, W. Dietary intake of calcium, fiber and other micronutrients in relation to colorectal cancer risk: Results from the Shanghai women’s health study. Int. J. Cancer 2006, 119, 2938–2942. [Google Scholar] [CrossRef]
- Zhong, X.; Fang, Y.J.; Pan, Z.Z.; Lu, M.S.; Zheng, M.C.; Chen, Y.M.; Zhang, C.X. Dietary fiber and fiber fraction intakes and colorectal cancer risk in Chinese adults. Nutr. Cancer 2014, 66, 351–361. [Google Scholar] [CrossRef]
- Song, J.W.; Chung, K.C. Observational studies: Cohort and case-control studies. Plast. Reconstr. Surg. 2010, 126, 2234–2242. [Google Scholar] [CrossRef] [PubMed]
- Tuncil, Y.E.; Nakatsu, C.H.; Kazem, A.E.; Arioglu-Tuncil, S.; Reuhs, B.; Martens, E.C.; Hamaker, B.R. Delayed utilization of some fast-fermenting soluble dietary fibers by human gut microbiota when presented in a mixture. J. Funct. Foods 2017, 32, 347–357. [Google Scholar] [CrossRef]
- Chen, T.; Long, W.; Zhang, C.; Liu, S.; Zhao, L.; Hamaker, B.R. Fiber-utilizing capacity varies in Prevotella-versus Bacteroides-dominated gut microbiota. Sci. Rep. 2017, 7, 2594. [Google Scholar] [CrossRef] [PubMed]
- Prado, S.B.R.d.; Castro-Alves, V.C.; Ferreira, G.F.; Fabi, J.P. Ingestion of non-digestible carbohydrates from plant-source foods and decreased risk of colorectal cancer: A review on the biological effects and the mechanisms of action. Front. Nutr. 2019, 6, 72. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.C.; Ferguson, L.R.; Tannock, G.W. Dietary fibres as “prebiotics”: Implications for colorectal cancer. Mol. Nutr. Food Res. 2005, 49, 609–619. [Google Scholar] [CrossRef]
- Duvallet, C.; Gibbons, S.M.; Gurry, T.; Irizarry, R.A.; Alm, E.J. Meta-analysis of gut microbiome studies identifies disease-specific and shared responses. Nat. Commun. 2017, 8, 1784. [Google Scholar] [CrossRef]
- Ahn, J.; Sinha, R.; Pei, Z.; Dominianni, C.; Wu, J.; Shi, J.; Goedert, J.J.; Hayes, R.B.; Yang, L. Human gut microbiome and risk for colorectal cancer. J. Nat. Cancer Inst. 2013, 105, 1907–1911. [Google Scholar] [CrossRef]
- Youssef, O.; Lahti, L.; Kokkola, A.; Karla, T.; Tikkanen, M.; Ehsan, H.; Carpelan-Holmstrom, M.; Koskensalo, S.; Bohling, T.; Rautelin, H.; et al. stool microbiota composition differs in patients with stomach, colon, and rectal neoplasms. Dig. Dis. Sci. 2018, 63, 2950–2958. [Google Scholar] [CrossRef]
- Flemer, B.; Lynch, D.B.; Brown, J.M.; Jeffery, I.B.; Ryan, F.J.; Claesson, M.J.; O’Riordain, M.; Shanahan, F.; O’Toole, P.W. Tumour-associated and non-tumour-associated microbiota in colorectal cancer. Gut 2017, 66, 633–643. [Google Scholar] [CrossRef]
- O’Callaghan, A.; van Sinderen, D. Bifidobacteria and their role as members of the human gut microbiota. Front. Microbiol. 2016, 7, 925. [Google Scholar] [CrossRef]
- Cianci, R.; Franza, L.; Schinzari, G.; Rossi, E.; Ianiro, G.; Tortora, G.; Gasbarrini, A.; Gambassi, G.; Cammarota, G. The interplay between immunity and microbiota at intestinal immunological niche: The case of cancer. Int. J. Mol. Sci. 2019, 20, 501. [Google Scholar] [CrossRef] [PubMed]
- Federici, E.; Prete, R.; Lazzi, C.; Pellegrini, N.; Moretti, M.; Corsetti, A.; Cenci, G. Bacterial composition, genotoxicity, and cytotoxicity of fecal samples from individuals consuming omnivorous or vegetarian diets. Front. Microbiol. 2017, 8, 300. [Google Scholar] [CrossRef] [PubMed]
- Yu, G.; Bei, J.; Zhao, J.; Li, Q.; Cheng, C. Modification of carrot (Daucus carota Linn. var. Sativa Hoffm.) pomace insoluble dietary fiber with complex enzyme method, ultrafine comminution, and high hydrostatic pressure. Food Chem. 2018, 257, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Sun, P.; Li, H.; Adhikari, B.P.; Li, D. Rheological behavior of tomato fiber suspensions produced by high shear and high pressure homogenization and their application in tomato products. Int. J. Anal. Chem. 2018, 2018, 5081938. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author and Year | Country | Sample Size | Gender and Age | Population Characteristics | Duration of Study | Dietary Fibre Intake * ± SD | Tool | Effect Size | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Case-control studies | |||||||||
| Arbman, 1992 | Sweden | 28 | M,F 49–77 y | Patients surgically treated for rectal cancer | 15 y | Cases: 21.23 ± 1.26 g/10 MJ (SEM) | dietary history protocol (interview) | RR: 0.12 (90% CI 0.02–0.76) | n.s. |
| Control: 21.18 ± 1.15 g/10 MJ (SEM) | |||||||||
| Dahm, 2010 | UK | 864 | M,F mean 56.97 y | Seven established UK cohorts: EPIC-Norfolk, EPIC-Oxford, the Guernsey Study, MRCNSHD, the OVS, the UKWCS and Whitehall II | 21 y | Cases: 8.9 ± 1.6 g/MJ | validated Food diary | OR (95%CI) 0.82(0.40–1.66) | p = 0.7 |
| Control: 24.1 ± 5.4 g/MJ | |||||||||
| Slattery (a), 2004 | USA | 1232 | M 30–79 y | KPMCP | 4 y | Cases: ≤16 g/d | CARDIA diet history | OR (95%CI): 0.54(0.34–0.86) | p < 0.01 |
| Control: >34 g/d | |||||||||
| Slattery (b), 2004 | USA | 945 | F 30–79 y | KPMCP | 4 y | Cases: ≤16 g/d | CARDIA diet history | OR (95%CI): 0.54(0.29–0.98) | p < 0.01 |
| Control: >34 g/d | |||||||||
| Uchida, 2010 | Japan | 1631 | M, F 20–74 y | Fukuka Colorectal Cancer Study, patients with histologically confirmed incident adenocarcinomas | 3 y | Cases: 9.2 g/d | validated computer-assisted interview | OR (95%CI): 1.24(0.74–2.10) | p = 0.41 |
| Control: 19.8 g/d | |||||||||
| Wakai (a), 2006 | Japan | 2777 | M, F 20–79 y | HERPACC included patients with cancer of colon or rectum and controls free of cancer | 3 y | n.a. | validated FFQ | OR (95%CI): 0.72 (0.49–1.08) | p = 0.64 |
| Wakai (b), 2006 | Japan | 1621 | M 20–79 y | HERPACC included patients with cancer of colon or rectum and controls free of cancer | 3 y | n.a. | validated FFQ | OR (95%CI): 0.83(0.47–1.45) | p = 0.68 |
| Wakai (c), 2006 | Japan | 1156 | F 20–79 y | HERPACC included patients with cancer of colon or rectum and controls free of cancer | 3 y | n.a. | validated FFQ | OR (95%CI): 0.78(0.40–1.51) | p = 0.64 |
| Zhong, 2014 | China | 878 | M, F mean age cases: 56.7 ± 10.6 (SD); age controls: 56.4 ±10.5 y | Colorectal cancer patients diagnosed no more than 3 months before interview. | 2 y | M/F cases: 7.13/13.79 g/d | validated FFQ | OR (95%CI): 0.38 (0.24–0.60) | p < 0.01 |
| M/F control: 14.92 /12.65 g/d | |||||||||
| Cohort studies | |||||||||
| Bingham, 2003 | Europe | 434,209 | M,F 25–70 y | EPIC | 6 y | Quintile 1: 12.71 g/d Quintile 5: 33.76 g/d | country-specific dietary questionnaire | HR (95% CI): 0.80 (0.53–1.22) | p = 0.319 |
| Bingham, 2005 | Europe | 603 | M, F 25–70 y | EPIC | 6.2 y | Quintile 1: 17.1 g/d Quintile 5: 27.2 g/d | self-administered dietary questionnaire | HR (95% CI): 0.62 (0.44–0.87) | p = 0.01 |
| Fuchs, 1999 | USA | 88,757 | F 34–59 y | Women, participants of the Nurses’ Health Study without history of cancer, inflammatory bowel disease, or familial polyposis | 16 y | Quintile 1: 9,8 ± 1,7 g/d | validated FFQ | RR (95%CI): 0.63(0.37–1.08) | p = 0.37 |
| Quintile 5: 24.9 ± 5.5 g/d | |||||||||
| Hansen (a), 2012 | Scandinavia | 38,852 | M 30–64 y | HELGA | 11.3 y | Quartile 1: >16.8–≤22.1 g/d | validated FFQ | RR (95%CI): 1.11(0.74–1.66) | n.s. |
| Quartile 4: >28.1 g/d | |||||||||
| Hansen (b), 2012 | Scandinavia | 69,229 | F 30–64 y | HELGA | 11.3 y | Quartile 1: >15.4–≤19.6 g/d | validated FFQ | RR (95%CI): 0.97(0.66–1.42) | n.s. |
| Quartile 4: >24.5 g/d | |||||||||
| Murphy, 2012 | Europe | 477,312 | M, ≥35 y | EPIC | mean follow-up: 11.0 y | Quintile 1: <16.4 g/d | validated FFQ | HR (95%CI): 0.90(0.72–1.14) | p = 0.34 |
| Quintile 5: ≥28.5 g/d | |||||||||
| Otani (a), 2005 | Japan | 47,400 | M 40–69 y | Cohort I of JPHC study started in 1990, the Cohort II started in 1993 | 5.8 y follow-up | Quintile 1: 6.4 g/d | validated FFQ self-administered | HR (95%CI): Highest 0.95(0.40–2.3) | p = 0.99 |
| Quintile 5: 18.7 g/d | |||||||||
| Otani (b), 2005 | Japan | 53,538 | F 40–69 y | Cohort I of JPHC study started in 1990, the Cohort II started in 1993 | 5.8 y follow-up | Quintile 1: 8.3 g/d Quintile 5: 20.0 g/d | validated FFQ self-administered | HR (95%CI): Highest 1.0(0.32–3.3) | p = 0.82 |
| Park 2016 (a) | USA | 85,905 | M 45–75 y | African American, Native Hawaiian, Japanese American, Latino, and white | 19 y | Quintile 1: <8.1 g/1000 kcal | self-administered quantitative FFQ | HR (95%CI): Highest 0.47 (0.35–0.62) | p < 0.0001 |
| Quintile 5: >15.3 g/1000 kcal | |||||||||
| Park 2016 (b) | USA | 101,769 | F 45–75 | African American, Native Hawaiian, Japanese American, Latino, and white cancer registries | 19 y | Quintile 1: <8.1 g/1000 kcal | self-administered mailed questionnaire | HR (95%CI): Highest 0.62 (0.45–0.86) | p = 0.004 |
| Quintile 5: >15.3 g/1000 kcal | |||||||||
| Schatzkin, 2007 | USA | 489,611 | M,F 50–71 years | NIH-AARP Diet and Health Study | 5 y follow-up | Quintile 1: 6.6 g/1000 kcal | validated FFQ self-administered | RR (95%CI): 1.13(0.84–1.51) | p = 0.39 |
| Quintile 5: 15.9 g/1000 kcal | |||||||||
| Shin, 2006 | China | 74,942 | F 40–72 years | SWHS | 3 y | Quintile 1: 7.3 g/d Quintile 5: >13.45 g/d | validated FFQ | RR (95%CI): 0.9(0.4–2.1) | p = 0.335 |
| Terry, 2001 | Sweden | 61,463 | F 40–74 years | SMSC | 9.6 y follow-up | Quartile 1: 5.7 ± 1.4 g/d | validate FFQ (self-administered) | RR (95%CI): 1.10(0.69–1.76) | p = 0.15 |
| Quartile 4: 13.6 ± 2.7 g/d | |||||||||
| Vulcan (a), 2015 | Sweden | 27,931 | M, F 66-93 years | MDCS | 15.4 follow-up y | Quintile 1: 0–1.7 g/MJ | 7-d menu book | HR (95% CI): 0.88(0.55–1.42) | p = 0.525 |
| Quintile 5: 2.7–8 g/MJ | |||||||||
| Vulcan (b), 2015 | Sweden | 10,987 | M 66–93 years | MDCS | 15.4 follow-up y | Quintile 1: 0–1.7 g/MJ | 7-d menu book | HR (95% CI): 0.59(0.31–1.12) | p = 0.263 |
| Quintile 5: 2.7–8 g/MJ | |||||||||
| Vulcan (c), 2015 | Sweden | 16,944 | F 66–93 years | MDCS | 15.4 follow-up y | Quintile 1: 0–1.7 g/MJ | 7-d menu book | HR (95% CI): 1.36(0.67–2.78) | p = 0.660 |
| Quintile 5: 2.7–8 g/MJ | |||||||||
| Wakai (a), 2007 | Japan | 43,115 | M,F 40–79 y | JACC | 7.6 y | Quartile 1: 7.1 ±2.0 g/d | validated FFQ | RR (95%CI): 1.10 (0.59–2.07) | p = 0.67 |
| Quartile 4: 13.4 ± 2.9 g/d | |||||||||
| Wakai (b), 2007 | Japan | 16,636 | M, 40–79 y | JACC | 7.6 y | Quartile 1: 6.7 ± 2.0 g/d | validated FFQ | RR (95%CI): 0.95 (0.45–2.02) | p = 0.89 |
| Quartile 4: 13.4 ± 3.0 g/d | |||||||||
| Wakai (c), 2007 | Japan | 26,479 | F, 40–79 y | JACC | 7.6 y | Quartile 1: 7.4 ± 2.1 g/d | validated FFQ | RR (95%CI): 1.82 (0.59–5.65) | p = 0.19 |
| Quartile 4: 13.4 ± 2.8 g/d | |||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gianfredi, V.; Nucci, D.; Salvatori, T.; Dallagiacoma, G.; Fatigoni, C.; Moretti, M.; Realdon, S. Rectal Cancer: 20% Risk Reduction Thanks to Dietary Fibre Intake. Systematic Review and Meta-Analysis. Nutrients 2019, 11, 1579. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071579
Gianfredi V, Nucci D, Salvatori T, Dallagiacoma G, Fatigoni C, Moretti M, Realdon S. Rectal Cancer: 20% Risk Reduction Thanks to Dietary Fibre Intake. Systematic Review and Meta-Analysis. Nutrients. 2019; 11(7):1579. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071579
Chicago/Turabian StyleGianfredi, Vincenza, Daniele Nucci, Tania Salvatori, Giulia Dallagiacoma, Cristina Fatigoni, Massimo Moretti, and Stefano Realdon. 2019. "Rectal Cancer: 20% Risk Reduction Thanks to Dietary Fibre Intake. Systematic Review and Meta-Analysis" Nutrients 11, no. 7: 1579. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071579