Effects of Anserine/Carnosine Supplementation on Mild Cognitive Impairment with APOE4

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Inventory of Anserine and Carnosine in the Normal Diet
2.3. Blood Analysis, APOE4 Genotyping and ELISA for Amyloid Beta 42
2.4. Test Formulae
2.5. Cognitive Testing
2.6. EEG Recording
2.7. Adverse Events and Safety
2.8. Statistical Analysis
3. Results
3.1. Characteristics of the Subjects
3.2. Anserine and Carnosine Intake from the Usual Diet in the Study Population
3.3. Primary Analysis
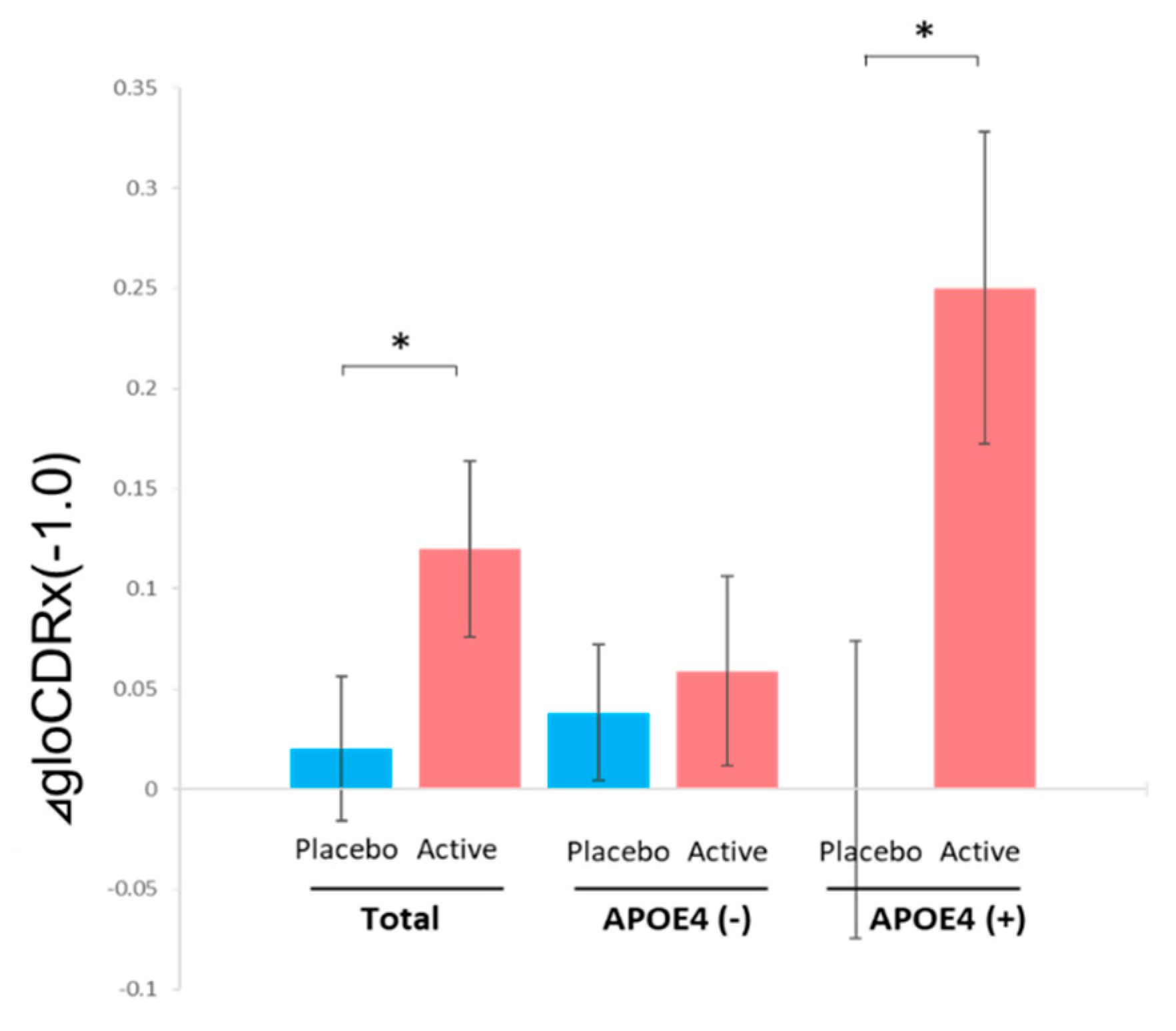
3.4. Analysis for Subgroups of Subjects with or without APOE4
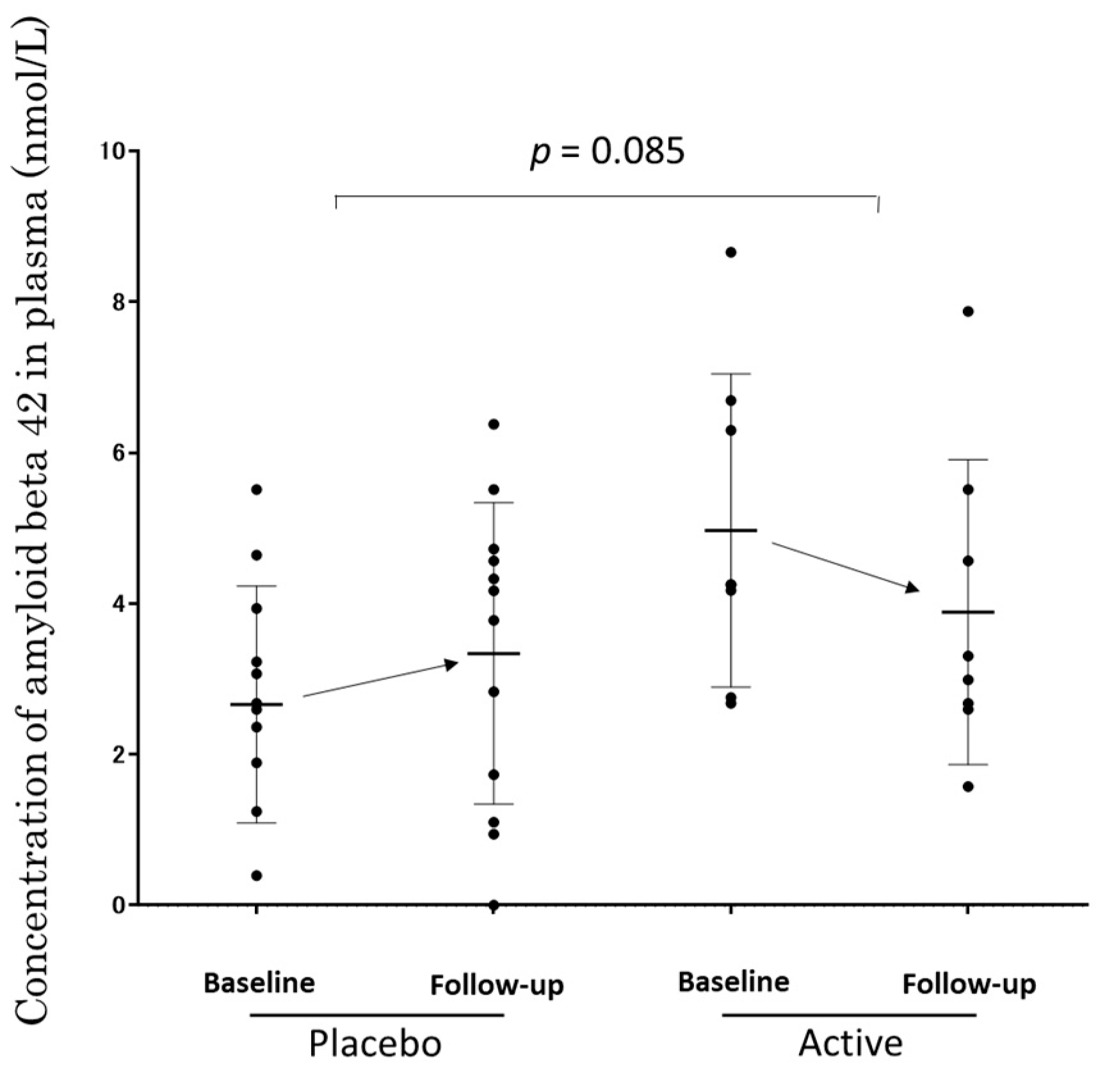
3.5. The Concentration of Aβ1-42 in Plasma of APOE4 (+) Subjects
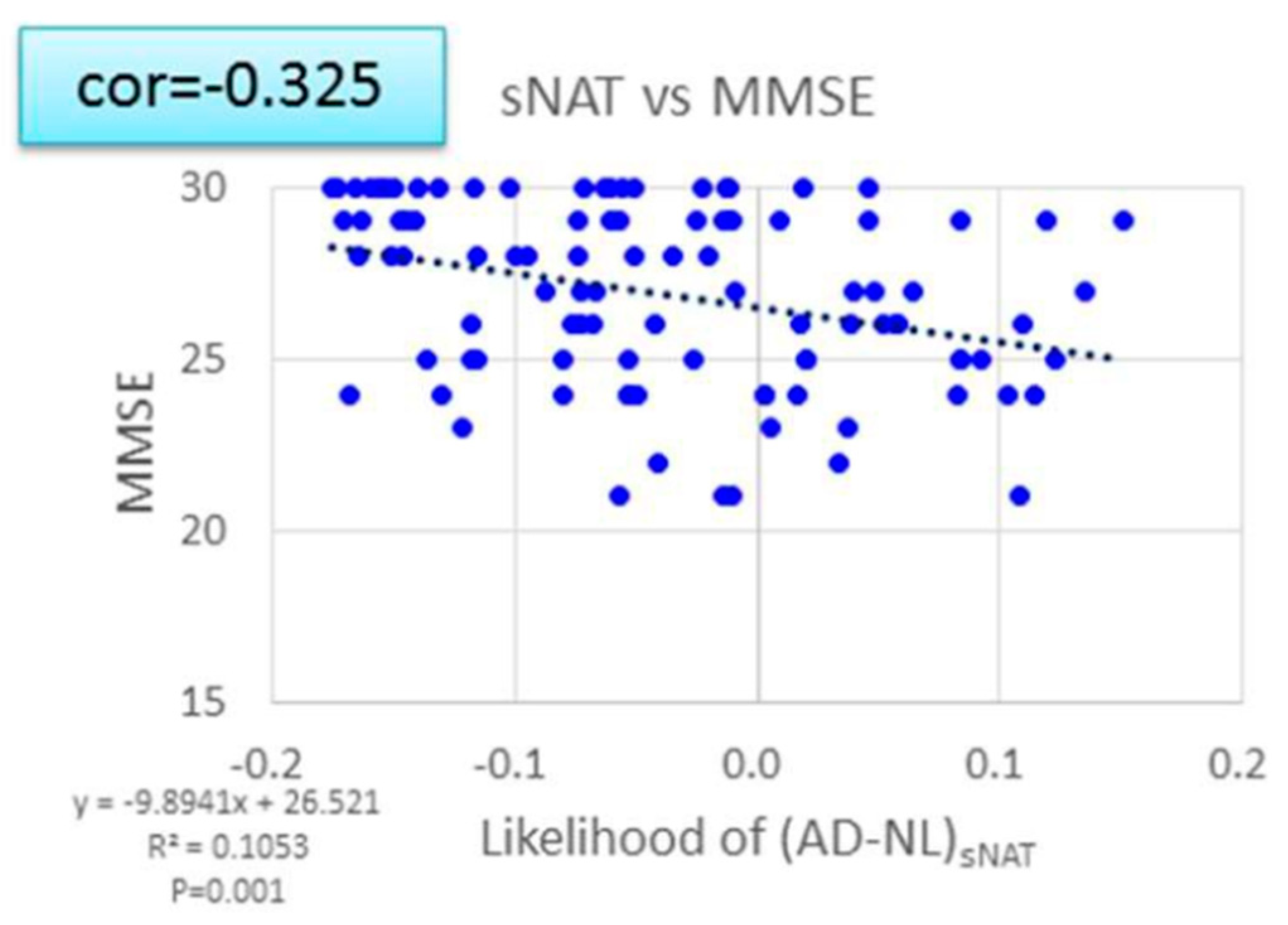
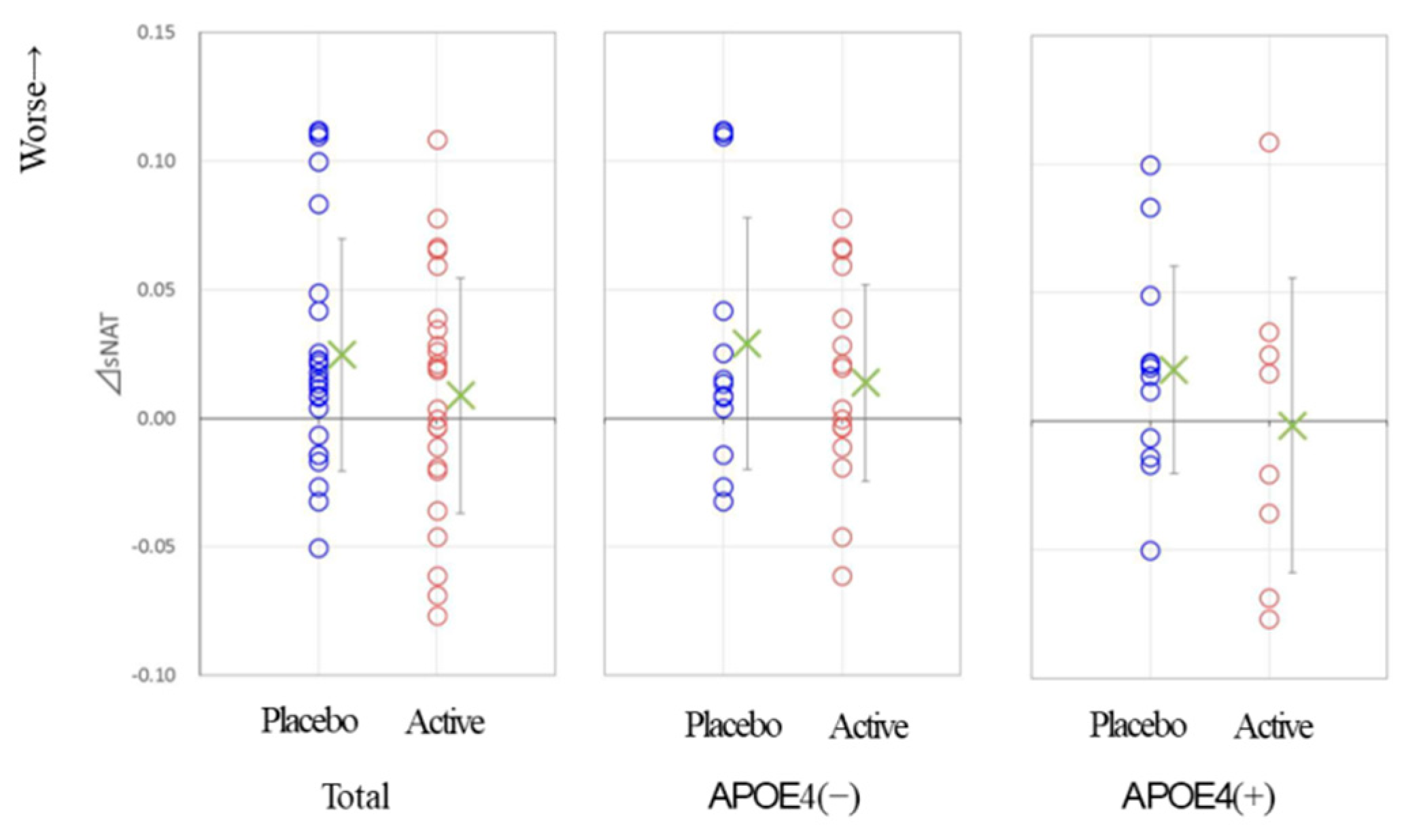
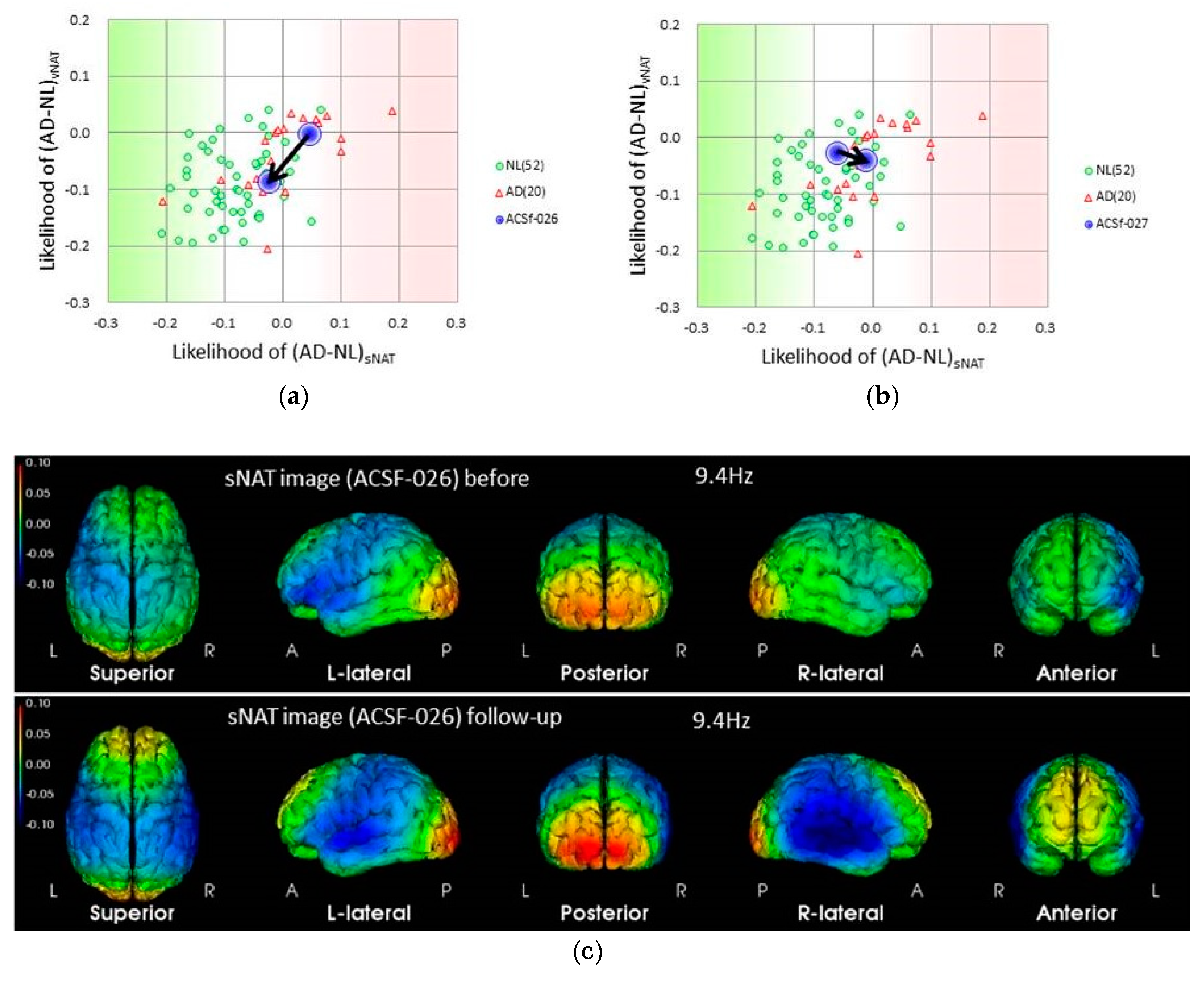
3.6. EEG Data
3.7. Clinical Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Towards a Dementia Plan: A WHO Guide; WHO: Geneva, Switzerland, 2018; Available online: https://apps.who.int/iris/bitstream/handle/10665/272642/9789241514132-eng.pdf (accessed on 16 July 2019).
- World Health Organization. The Epidemiology and Impact of Dementia: Current State and Future Trends; WHO: Geneva, Switzerland, 2015; Available online: http://www.who.int/mental_health/neurology/dementia/dementia_thematicbrief_epidemiology.pdf (accessed on 16 July 2019).
- GBD 2016 Dementia Collaborators (2007). Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2016, 18, 88–106. [Google Scholar]
- Plassman, B.L.; Langa, K.M.; Fisher, G.G.; Heeringa, S.G.; Weir, D.R.; Ofstedal, M.B.; Burke, J.R.; Hurd, M.D.; Potter, G.G.; Rodgers, W.L.; et al. Prevalence of dementia in the United States: The aging, demographics, and memory study. Neuroepidemiology 2007, 29, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Corder, E.H.; Saunders, A.M.; Strittmatter, W.J.; Schmechel, D.E.; Gaskell, P.C.; Small, G.W.; Roses, A.D.; Haines, J.L.; Pericak-Vance, M.A. Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer’s disease in late onset families. Science 1993, 261, 921–923. [Google Scholar] [CrossRef] [PubMed]
- Farrer, L.A.; Cupples, L.A.; Haines, J.L.; Hyman, B.; Kukull, W.A.; Mayeux, R.; Myers, R.H.; Pericak-Vance, M.A.; Risch, N.; van Duijn, C.M. Effects of Age, Sex, and Ethnicity on the Association between Apolipoprotein E Genotype and Alzheimer Disease. A Meta-analysis. JAMA 1997, 278, 1349–1356. [Google Scholar] [CrossRef] [PubMed]
- Giri, M.; Zhang, M.; Lü, Y. Genes associated with Alzheimer’s disease: An overview and current status. Clin. Interv. Aging 2016, 11, 665–681. [Google Scholar] [CrossRef] [PubMed]
- Tai, L.M.; Thomas, R.; Marottoli, F.M.; Koster, K.P.; Kanekiyo, T.; Morris, A.W.J.; Bu, G. The role of APOE in cerebrovascular dysfunction. Acta. Neuropathol. 2016, 131, 709–723. [Google Scholar] [CrossRef] [Green Version]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild cognitive impairment: Clinical characterization and outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef]
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef]
- Fink, H.A.; Jutkowitz, E.; McCarten, J.R.; Hemmy, L.S.; Butler, M.; Davila, H.; Ratner, E.; Calvert, C.; Barclay, T.R.; Brasure, M.; et al. Pharmacologic Interventions to Prevent Cognitive Decline, Mild Cognitive Impairment, and Clinical Alzheimer-Type Dementia: A Systematic Review. Ann. Intern. Med. 2018, 168, 39–51. [Google Scholar] [CrossRef]
- Lindenberger, U. Human cognitive aging: Corriger la fortune? Science 2014, 346, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Gutchess, A. Plasticity of the aging brain: New directions in cognitive neuroscience. Science 2014, 346, 579–582. [Google Scholar] [CrossRef] [PubMed]
- Pistollato, F.; Iglesias, R.C.; Ruiz, R.; Aparicio, S.; Crespo, J.; Lopez, L.D.; Manna, P.P.; Giampieri, F.; Battino, M. Nutritional patterns associated with the maintenance of neurocognitive functions and the risk of dementia and Alzheimer’s disease: A focus on human studies. Pharmacol. Res. 2018, 131, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Rokicki, J.; Li, L.; Imabayashi, E.; Kaneko, J.; Hisatsune, T.; Matsuda, H. Daily Carnosine and Anserine Supplementation Alters Verbal Episodic Memory and Resting State Network Connectivity in Healthy Elderly Adults. Front. Aging Neurosci. 2015, 7, 219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hisatsune, T.; Kaneko, J.; Kurashige, H.; Cao, Y.; Satsu, H.; Totsuka, M.; Katakura, Y.; Imabayashi, E.; Matsuda, H. Effect of Anserine/Carnosine Supplementation on Verbal Episodic Memory in Elderly People. J. Alzheimers Dis. 2016, 50, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Szcześniak, D.; Budzen, S.; Kopec, W.; Rymaszewska, J. Anserine and carnosine supplementation in the elderly: Effects on cognitive functioning and physical capacity. Arch. Gerontol. Geriatr. 2014, 59, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Ding, Q.; Tanigawa, K.; Kaneko, J.; Totsuka, M.; Katakura, Y.; Imabayashi, E.; Matsuda, H.; Hisatsune, T. Anserine/carnosine supplementation preserves blood flow in the prefrontal brain of elderly people carrying APOE e4. Aging Dis. 2018, 9, 334–345. [Google Scholar] [CrossRef] [PubMed]
- Boldyrev, A.A.; Aldini, G.; Derave, W. Physiology and pathology of carnosine. Physiol. Rev. 2013, 93, 1803–1845. [Google Scholar] [CrossRef]
- Kubomura, D.; Matahira, Y.; Masui, A.; Matsuda, H. Intestinal Absorption and Blood Clearance of L-Histidine-Related Compounds after Ingestion of Anserine in Humans and Comparison to Anserine-Containing Diets. J. Agric. Food Chem. 2009, 57, 1781–1785. [Google Scholar] [CrossRef]
- Yeum, K.-J.; Orioli, M.; Regazzoni, L.; Carini, M.; Rasmussen, H.; Russell, R.M.; Aldini, G. Profiling histidine dipeptides in plasma and urine after ingesting beef, chicken or chicken broth in humans. Amino Acids 2010, 38, 847–858. [Google Scholar] [CrossRef]
- Musha, T.; Matsuzaki, H.; Kobayashi, Y.; Okamoto, Y.; Tanaka, M.; Asada, T. EEG Markers for Characterizing Anomalous Activities of Cerebral Neurons in NAT (Neuronal Activity Topography) Method. IEEE Trans. Biomed. Eng. 2013, 60, 2332–2338. [Google Scholar] [CrossRef] [PubMed]
- Musha, T.; Asada, T.; Yamashita, F.; Kinoshita, T.; Chen, Z.; Matsuda, H.; Uno, M.; Shankle, W.R. A new EEG method for estimating cortical neuronal impairment that is sensitive to early stage Alzheimer’s disease. Clin. Neurophysiol. 2002, 113, 1052–1058. [Google Scholar] [CrossRef]
- Cichocki, A.; Shishkin, S.L.; Musha, T.; Leonowicz, Z.; Asada, T.; Kurachi, T. EEG filtering based on blind source separation (BSS) for early detection of Alzheimer’s disease. Clin. Neurophysiol. 2005, 116, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Osone, A.; Arai, R.; Hakamada, R.; Shimoda, K. Cognitive and brain reserve in conversion and reversion in patients with mild cognitive impairment over 12 months of follow-up. J. Clin. Exp. Neuropsychol. 2016, 38, 1084–1093. [Google Scholar] [CrossRef] [PubMed]
- Kuroki, T.; Ishitobi, M.; Kamio, Y.; Sugihara, G.; Murai, T.; Motomura, K.; Ogasawara, K.; Kimura, H.; Aleksic, B.; Ozaki, N.; et al. Current viewpoints on DSM-5 in Japan. Psychiatry Clin. Neurosci. 2016, 70, 371–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujino, T.; Yamada, T.; Asada, T.; Tsuboi, Y.; Wakana, C.; Mawatari, S.; Kono, S. Efficacy and Blood Plasmalogen Changes by Oral Administration of Plasmalogen in Patients with Mild Alzheimer’s Disease and Mild Cognitive Impairment: A Multicenter, Randomized, Double-blind, Placebo-controlled Trial. EBioMedicine 2017, 17, 199–205. [Google Scholar] [CrossRef]
- Kiyohara, Y.; Shinohara, A.; Kato, I.; Shirota, T.; Kubo, M.; Tanizaki, Y.; Fujishima, M.; Iida, M. Dietary factors and development of impaired glucose tolerance and diabetes in a general Japanese population: The Hisayama Study. J. Epidemiol. 2003, 13, 251–258. [Google Scholar] [CrossRef]
- Asada, T.; Kariya, T.; Yamagata, Z.; Kinoshita, T.; Asaka, A. ApoE epsilon 4 allele and cognitive decline in patients with Alzheimer’s disease. Neurology 1996, 47, 603. [Google Scholar] [CrossRef]
- Yasuno, F.; Tanimukai, S.; Sasaki, M.; Ikejima, C.; Yamashita, F.; Kodama, C.; Hidaka, S.; Mizukami, K.; Asada, T. Effect of plasma lipids, hypertension and APOE genotype on cognitive decline. Neurobiol. Aging 2012, 33, 2633–2640. [Google Scholar] [CrossRef] [Green Version]
- Ikejima, C.; Hisanaga, A.; Meguro, K.; Yamada, T.; Ouma, S.; Kawamuro, Y.; Hyouki, K.; Nakashima, K.; Wada, K.; Yamada, S.; et al. Multicentre population-based dementia prevalence survey in Japan: A preliminary report. Psychogeriatrics 2012, 12, 120–123. [Google Scholar] [CrossRef]
- Malek-Ahmadi, M. Reversion from mild cognitive impairment to normal cognition: A Meta-Analysis. Alzheimer Dis. Assoc. Disord. 2016, 30, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Aerts, L.; Heffernan, M.; Kochan, N.A.; Crawford, J.D.; Draper, B.; Trollor, J.N.; Sachdev, P.S.; Brodaty, H. Effects of MCI subtype and reversion on progression to dementia in a community sample. Neurology 2017, 88, 2225–2232. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.O.; Knopman, D.S.; Mielke, M.M.; Cha, R.H.; Pankratz, V.S.; Christianson, T.J.; Geda, Y.E.; Boeve, B.F.; Ivnik, R.J.; Tangalos, E.G.; et al. Higher risk of progression to dementia in mild cognitive impairment cases who revert to normal. Neurology 2014, 82, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- McKhan, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group* under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984, 34, 939–944. [Google Scholar] [CrossRef] [PubMed]
- Janelidze, S.; Stomrud, E.; Palmqvist, S.; Zetterberg, H.; van Westen, D.; Jeromin, A.; Song, L.; Hanlon, D.; Tan Hehir, C.A.; Baker, D.; et al. Plasma β-amyloid in Alzheimer’s disease and vascular disease. Sci. Rep. 2016, 6, 26801. [Google Scholar] [CrossRef]
- Hsu, J.L.; Lee, W.J.; Liao, Y.C.; Wang, S.J.; Fuh, J.L. The clinical significance of plasma clusterin and Aβ in the longitudinal follow-up of patients with Alzheimer’s disease. Alzheimer’s Res. Ther. 2017, 9, 91. [Google Scholar] [CrossRef]
- Herculano, B.; Tamura, M.; Ohba, A.; Shimatani, M.; Kutsuna, N.; Hisatsune, T. β-alanyl-L-histidine rescues cognitive deficits caused by feeding a high fat diet in a transgenic mouse model of Alzheimer’s disease. J. Alzheimer’s Dis. 2013, 33, 983–997. [Google Scholar] [CrossRef]
- Kaneko, J.; Enya, A.; Enomoto, K.; Ding, Q.; Hisatsune, T. Anserine (beta-alanyl-3-methyl-L-histidine) improves neurovascular-unit dysfunction and spatial memory in aged AβPPswe/PSEN1dE9 Alzheimer’s-model mice. Sci. Rep. 2017, 7, 12571. [Google Scholar] [CrossRef]
- Bell, R.D.; Zlokovic, B.V. Neurovascular mechanisms and blood-brain barrier disorder in Alzheimer’s disease. Acta Neuropathol. 2009, 118, 103–113. [Google Scholar] [CrossRef]
- Bell, R.D.; Winkler, E.A.; Singh, I.; Sagare, A.P.; Deane, R.; Wu, Z.; Holtzman, D.M.; Betsholtz, C.; Armulik, A.; Sallstrom, J.; et al. Apolipoprotein E controls cerebrovascular integrity via cyclophilin A. Nature 2012, 485, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Halliday, M.R.; Rege, S.V.; Ma, Q.; Zhao, Z.; Miller, C.A.; Winkler, E.A.; Zlokovic, B.V. Accelerated pericyte degeneration and blood-brain barrier breakdown in apolipoprotein E4 carriers with Alzheimer’s disease. J. Cereb. Blood Flow Metab. 2016, 36, 216–227. [Google Scholar] [CrossRef] [PubMed]
- Zlokovic, B.V. Neurovascular pathways to neurodegeneration in Alzheimer’s disease and other disorders. Nat. Rev. Neurosci. 2011, 12, 723–738. [Google Scholar] [CrossRef] [PubMed]
- Katakura, Y.; Totsuka, M.; Imabayashi, E.; Matsuda, H.; Hisatsune, T. Anserine/Carnosine Supplementation Suppresses the Expression of the Inflammatory Chemokine CCL24 in Peripheral Blood Mononuclear Cells from Elderly People. Nutrients 2017, 9, 1199. [Google Scholar] [CrossRef] [PubMed]
- Vitek, M.P.; Brown, C.M.; Colton, C.A. APOE genotype-specific differences in the innate immune response. Neurobiol. Aging 2009, 30, 1350–1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jofre-Monseny, L.; Loboda, A.; Wagner, A.E.; Huebbe, P.; Boesch-Saadatmandi, C.; Jozkowicz, A.; Minihane, A.M.; Dulak, J.; Rimbach, G. Effects of apoE genotype on macrophage inflammation and heme oxygenase-1 expression. Biochem. Biophys. Res. Commun. 2007, 357, 319–324. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Active Group | Placebo Group | p Value | |
|---|---|---|---|
| Age | 72.9 ± 8.8 b | 73.6 ± 6.1 | 0.75 c |
| Gender (M/F) | 12/13 | 12/13 | |
| BMI | 22.2 ± 2.8 | 21.5 ± 2.6 | 0.46 c |
| Years of education | 13.9 ± 2.5 | 14.1 ± 2.8 | 0.83 c |
| APOE4 positive/negative | 8/17 | 12/13 | 0.25 d |
| Startup | Follow-Up | Treatment × Time Interaction b | |||||
|---|---|---|---|---|---|---|---|
| Active | Placebo | Active | Placebo | Active | Placebo | p Value | |
| MMSE | 27.5 ± 2.2 | 27.0 ± 2.1 | 27.1 ± 2.5 | 26.0 ± 3.4 | −0.4 ± 1.6 | −1.0 ± 1.8 | 0.252 |
| gloCDR | 0.5 | 0.5 | 0.38 ± 0.2 | 0.48 ± 0.2 | −0.12 ± 0.22 | −0.02 ± 0.18 | 0.0231 |
| CDRsob | 0.82 ± 0.45 | 1.04 ± 0.53 | 0.80 ± 0.5 | 1.12 ± 0.77 | −0.02 ± 0.51 | 0.12 ± 0.79 | 0.583 |
| WMS-1 | 7.8 ± 4.4 | 7.0 ± 4.5 | 9.1 ± 4.4 | 8.2 ± 5.7 | 1.2 ± 2.8 | 1.2 ± 3.1 | 0.591 |
| WMS-2 | 5.3 ± 4.4 | 5.6 ± 4.6 | 6.7 ± 5.2 | 6.4 ± 6.1 | 1.4 ± 3.0 | 0.7 ± 3.0 | 0.975 |
| ADAS | 12.3 ± 7.4 | 15.5 ± 7.6 | 13.0 ± 8.5 | 15.4 ± 8.6 | 0.8 ± 4.4 | −0.2 ± 4.7 | 0.320 |
| GDS | 2.5 ± 1.9 | 2.5 ± 2.4 | 2.6 ± 2.9 | 2.6 ± 2.1 | 0.1 ± 2.7 | 0.1 ± 2.0 | 0.943 |
| Startup | Follow-Up | Treatment × Time Interaction b | |||||
|---|---|---|---|---|---|---|---|
| Active | Placebo | Active | Placebo | Active | Placebo | p Value | |
| MMSE | 27.1 ± 2.4 | 26.7 ± 2.3 | 26.9 ± 2.3 | 25.1 ± 3.6 | −0.25 ± 1.4 | −1.6 ± 1.5 | 0.0253 |
| gloCDR | 0.5 | 0.5 | 0.25 ± 0.27 | 0.50 ± 0.21 | −0.25 ± 0.27 | 0 ± 0.21 | 0.0261 |
| CDRsob | 0.69 ± 0.37 | 1.25 ± 0.50 | 0.75 ± 0.65 | 1.33 ± 0.86 | 0.06 ± 0.68 | 0.08 ± 0.82 | 0.406 |
| WMS-1 | 9.3 ± 3.4 | 6.5 ± 4.9 | 8.4 ± 3.1 | 6.8 ± 5.2 | −0.88 ± 2.9 | 0.25 ± 2.5 | 0.592 |
| WMS-2 | 5.8 ± 3.7 | 4.9 ± 4.5 | 6.4 ± 4.4 | 4.6 ± 5.5 | 0.63 ± 3.2 | −0.33 ± 2.4 | 0.670 |
| ADAS | 10.9 ± 5.8 | 17.6 ± 8.9 | 12.2 ± 9.4 | 17.5 ± 9.9 | 1.3 ± 6.4 | −0.13 ± 5.3 | 0.207 |
| GDS | 1.6 ± 1.1 | 2.1 ± 1.4 | 1.4 ± 2.0 | 2.6 ± 2.2 | −0.25 ± 2.7 | 0.5 ± 1.9 | 0.165 |
| GDS | 2.5 ± 1.9 | 2.5 ± 2.4 | 2.6 ± 2.9 | 2.6 ± 2.1 | 0.1 ± 2.7 | 0.1 ± 2.0 | 0.943 |
| Startup | Follow-Up | Treatment × Time Interaction b | |||||
|---|---|---|---|---|---|---|---|
| Active | Placebo | Active | Placebo | Active | Placebo | p Value | |
| MMSE | 27.6 ± 2.1 | 27.3 ± 2.0 | 27.2 ± 2.6 | 26.8 ± 3.1 | −0.41 ± 1.7 | −0.46 ± 1.9 | 0.840 |
| gloCDR | 0.5 | 0.5 | 0.44 ± 0.17 | 0.46 ± 0.14 | −0.059 ± 0.17 | −0.038 ± 0.14 | 0.477 |
| CDRsob | 0.88 ± 0.49 | 0.85 ± 0.47 | 0.82 ± 0.43 | 0.92 ± 0.64 | −0.059 ± 0.43 | 0.077 ± 0.76 | 0.602 |
| WMS-1 | 7.2 ± 4.8 | 7.5 ± 4.2 | 9.4 ± 4.9 | 9.5 ± 6.1 | 2.2 ± 2.3 | 2.0 ± 3.5 | 0.993 |
| WMS-2 | 5.1 ± 4.8 | 6.3 ± 4.6 | 6.8 ± 5.6 | 8.0 ± 6.5 | 1.7 ± 2.9 | 1.7 ± 3.3 | 0.997 |
| ADAS | 12.9 ± 8.2 | 13.6 ± 5.9 | 13.5 ± 8.2 | 13.4 ± 7.1 | 0.54 ± 3.3 | −0.20 ± 4.3 | 0.697 |
| GDS | 2.9 ± 2.0 | 2.8 ± 3.1 | 3.2 ± 3.1 | 2.5 ± 2.1 | 0.29 ± 2.8 | −0.30 ± 2.0 | 0.676 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masuoka, N.; Yoshimine, C.; Hori, M.; Tanaka, M.; Asada, T.; Abe, K.; Hisatsune, T. Effects of Anserine/Carnosine Supplementation on Mild Cognitive Impairment with APOE4. Nutrients 2019, 11, 1626. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071626
Masuoka N, Yoshimine C, Hori M, Tanaka M, Asada T, Abe K, Hisatsune T. Effects of Anserine/Carnosine Supplementation on Mild Cognitive Impairment with APOE4. Nutrients. 2019; 11(7):1626. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071626
Chicago/Turabian StyleMasuoka, Nobutaka, Chitose Yoshimine, Marie Hori, Mieko Tanaka, Takashi Asada, Keiichi Abe, and Tatsuhiro Hisatsune. 2019. "Effects of Anserine/Carnosine Supplementation on Mild Cognitive Impairment with APOE4" Nutrients 11, no. 7: 1626. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071626