Association of Diet Quality and Vegetable Variety with the Risk of Cognitive Decline in Chinese Older Adults

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Assessment of Diet, Diet Quality, and Vegetable Variety
2.3. Assessment of Cognition
2.4. Covariates
2.5. Laboratory Assay
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Association between Diet Quality, Quantity-Adjusted Vegetable Variety, and Risk of Cognitive Decline
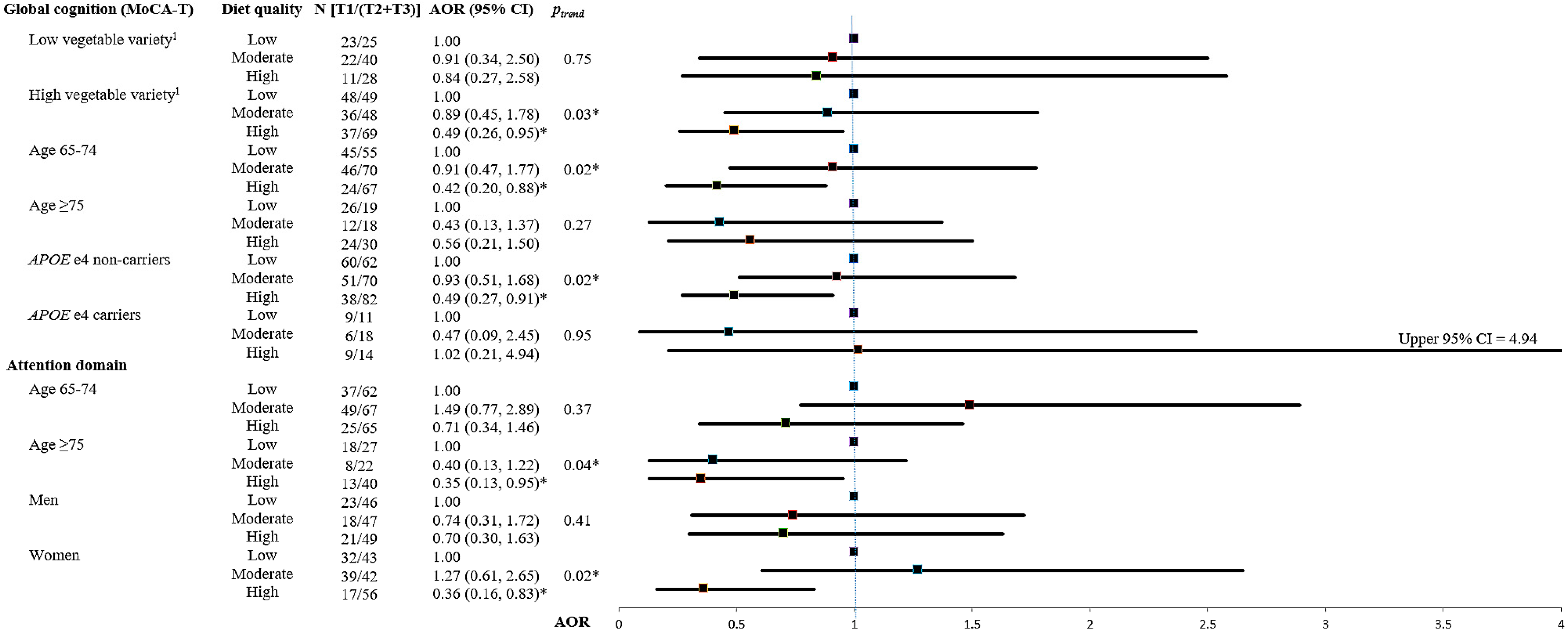
3.3. Interactions between Diet Quality and Important Covariates
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sachdev, P.S.; Blacker, D.; Blazer, D.G.; Ganguli, M.; Jeste, D.V.; Paulsen, J.S.; Petersen, R.C. Classifying neurocognitive disorders: The DSM-5 approach. Nat. Rev. Neurol. 2014, 10, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C. Clinical practice. Mild cognitive impairment. N. Engl. J. Med. 2011, 364, 2227–2234. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Association. 2018 Alzheimer’s disease facts and figures. Alzheimers Dement. 2018, 14, 367–429. [Google Scholar] [CrossRef]
- Guerchet, M.; Ali, G.C.; Prince, M.; Wu, Y.T. Chapter 3. The incidence of dementia. In World Alzheimer Report 2015. The Global Impact of Dementia and Analysis of Prevalence, Incidence, Cost and Trends; Prince, M., Wimo, A., Guerchet, M., Ali, G.C., Wu, Y.T., Prina, M., Eds.; Alzheimer’s Disease International: London, UK, 2015; pp. 30–35. [Google Scholar]
- Sun, Y.; Lee, H.J.; Yang, S.C.; Chen, T.F.; Lin, K.N.; Lin, C.C.; Wang, P.N.; Tang, L.Y.; Chiu, M.J. A nationwide survey of mild cognitive impairment and dementia, including very mild dementia, in Taiwan. PLoS ONE 2014, 9, e100303. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.; Tang, E.; Taylor, J.P. Dementia: Timely diagnosis and early intervention. BMJ 2015, 350, h3029. [Google Scholar] [CrossRef] [PubMed]
- Saunders, A.M.; Strittmatter, W.J.; Schmechel, D.; George-Hyslop, P.H.; Pericak-Vance, M.A.; Joo, S.H.; Rosi, B.L.; Gusella, J.F.; Crapper-MacLachlan, D.R.; Alberts, M.J.; et al. Association of apolipoprotein e allele epsilon 4 with late-onset familial and sporadic alzheimer’s disease. Neurology 1993, 43, 1467–1472. [Google Scholar] [CrossRef] [PubMed]
- Farrer, L.A.; Cupples, L.A.; Haines, J.L.; Hyman, B.; Kukull, W.A.; Mayeux, R.; Myers, R.H.; Pericak-Vance, M.A.; Risch, N.; van Duijn, C.M. Effects of age, sex, and ethnicity on the association between apolipoprotein e genotype and alzheimer disease: A meta-analysis. JAMA 1997, 278, 1349–1356. [Google Scholar] [CrossRef]
- Plassman, B.L.; Williams, J.W., Jr.; Burke, J.R.; Holsinger, T.; Benjamin, S. Systematic review: Factors associated with risk for and possible prevention of cognitive decline in later life. Ann. Intern. Med. 2010, 153, 182–193. [Google Scholar] [CrossRef]
- Griñán-Ferré, C.; Corpas, R.; Puigoriol-Illamola, D.; Palomera-Ávalos, V.; Sanfeliu, C.; Pallàs, M. Understanding epigenetics in the neurodegeneration of alzheimer’s disease: Samp8 mouse model. J. Alzheimers Dis. 2018, 62, 943–963. [Google Scholar] [CrossRef]
- Kamphuis, P.J.; Scheltens, P. Can nutrients prevent or delay onset of Alzheimer’s disease? J. Alzheimers Dis. 2010, 20, 765–775. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Kourlaba, G.; Panagiotakos, D.B. Dietary quality indices and human health: A review. Maturitas 2009, 62, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kritchevsky, S.B.; Houston, D.K. Chapter 15. Nutritional Epidemiology in Aging. In The Epidemiology of Aging; Newman, A.B., Cauley, J.A., Eds.; Springer: Dordrecht, The Netherlands, 2012; pp. 255–272. [Google Scholar]
- Waijers, P.M.; Feskens, E.J.; Ocke, M.C. A critical review of predefined diet quality scores. Br. J. Nutr. 2007, 97, 219–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- US Department of Health and Human Services and US Department of Agriculture. 2015–2020 Dietary Guidelines for Americans. Available online: http://health.Gov/dietaryguidelines/2015/guidelines/ (accessed on 30 December 2018).
- Binns, C.W.; Lee, M.K.; Kagawa, M.; Low, W.Y.; Liqian, Q.; Guldan, G.S.; Hokama, T.; Nanishi, K.; Oy, S.; Tang, L.; et al. Dietary guidelines for the Asia pacific region. Asia Pac. J. Public Health 2017, 29, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Health Promotion Administration, Ministry of Health and Welfare. Daily Food Guide for Taiwanese. Available online: http://www.Hpa.Gov.Tw/home/index.Aspx (accessed on 30 December 2018).
- Solfrizzi, V.; Panza, F.; Frisardi, V.; Seripa, D.; Logroscino, G.; Imbimbo, B.P.; Pilotto, A. Diet and alzheimer’s disease risk factors or prevention: The current evidence. Expert Rev. Neurother. 2011, 11, 677–708. [Google Scholar] [CrossRef] [PubMed]
- Loef, M.; Walach, H. Fruit, vegetables and prevention of cognitive decline or dementia: A systematic review of cohort studies. J. Nutr. Health Aging 2012, 16, 626–630. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.H.; Ascherio, A.; Grodstein, F. Fruit and vegetable consumption and cognitive decline in aging women. Ann. Neurol. 2005, 57, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Jung, C.C.; Chen, J.H.; Chiou, J.M.; Chen, T.F.; Chen, Y.F.; Tang, S.C.; Yeh, S.J.; Lee, M.S. Association of dietary patterns with global and domain-specific cognitive decline in Chinese elderly. J. Am. Geriatr. Soc. 2017, 65, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Huijbregts, P.P.; Feskens, E.J.; Rasanen, L.; Fidanza, F.; Alberti-Fidanza, A.; Nissinen, A.; Giampaoli, S.; Kromhout, D. Dietary patterns and cognitive function in elderly men in Finland, Italy and the Netherlands. Eur. J. Clin. Nutr. 1998, 52, 826–831. [Google Scholar] [CrossRef] [Green Version]
- Correa Leite, M.L.; Nicolosi, A.; Cristina, S.; Hauser, W.A.; Nappi, G. Nutrition and cognitive deficit in the elderly: A population study. Eur. J. Clin. Nutr. 2001, 55, 1053–1058. [Google Scholar] [CrossRef]
- Tangney, C.C.; Kwasny, M.J.; Li, H.; Wilson, R.S.; Evans, D.A.; Morris, M.C. Adherence to a mediterranean-type dietary pattern and cognitive decline in a community population. Am. J. Clin. Nutr. 2011, 93, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Shatenstein, B.; Ferland, G.; Belleville, S.; Gray-Donald, K.; Kergoat, M.J.; Morais, J.; Gaudreau, P.; Payette, H.; Greenwood, C. Diet quality and cognition among older adults from the NuAge study. Exp. Gerontol. 2012, 47, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Olsson, E.; Karlstrom, B.; Kilander, L.; Byberg, L.; Cederholm, T.; Sjogren, P. Dietary patterns and cognitive dysfunction in a 12-year follow-up study of 70 year old men. J. Alzheimers Dis. 2015, 43, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Haring, B.; Wu, C.; Mossavar-Rahmani, Y.; Snetselaar, L.; Brunner, R.; Wallace, R.B.; Neuhouser, M.L.; Wassertheil-Smoller, S. No association between dietary patterns and risk for cognitive decline in older women with 9-year follow-up: Data from the women’s health initiative memory study. J. Acad. Nutr. Diet. 2016, 116, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Sasaki, S.; Horiguchi, H.; Oguma, E.; Miyamoto, K.; Hosoi, Y.; Kim, M.K.; Kayama, F. Dietary patterns associated with bone mineral density in premenopausal Japanese farmwomen. Am. J. Clin. Nutr. 2006, 83, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Pan, W.H.; Liu, K.L.; Yu, M.S. Reproducibility and validity of a Chinese food frequency questionnaire used in Taiwan. Asia Pac. J. Clin. Nutr. 2006, 15, 161–169. [Google Scholar] [PubMed]
- Bowman, S.A.; Clemens, J.C.; Thoerig, R.C.; Friday, J.E.; Shimizu, M.; Moshfegh, A.J. Food Patterns Equivalents Database 2009–2010: Methodology and User Guide. Worldwide Web Site: Food Surveys Research Group. Available online: www.ars.usda.gov/Services/docs.htm?docid=23594 (accessed on 30 December 2018).
- Taiwan’s Food and Drug Administration Database. Available online: https://consumer.Fda.Gov.Tw/food/tfnd.Aspx?Nodeid=178# (accessed on 30 December 2018).
- Dehghan, M.; Mente, A.; Teo, K.K.; Gao, P.; Sleight, P.; Dagenais, G.; Avezum, A.; Probstfield, J.L.; Dans, T.; Yusuf, S.; et al. Relationship between healthy diet and risk of cardiovascular disease among patients on drug therapies for secondary prevention: A prospective cohort study of 31,546 high-risk individuals from 40 countries. Circulation 2012, 126, 2705–2712. [Google Scholar] [CrossRef]
- Leenders, M.; Siersema, P.D.; Overvad, K.; Tjonneland, A.; Olsen, A.; Boutron-Ruault, M.C.; Bastide, N.; Fagherazzi, G.; Katzke, V.; Kuhn, T.; et al. Subtypes of fruit and vegetables, variety in consumption and risk of colon and rectal cancer in the european prospective investigation into cancer and nutrition. Int. J. Cancer 2015, 137, 2705–2714. [Google Scholar] [CrossRef]
- Tsai, C.F.; Lee, W.J.; Wang, S.J.; Shia, B.C.; Nasreddine, Z.; Fuh, J.L. Psychometrics of the montreal cognitive assessment (MoCA) and its subscales: Validation of the taiwanese version of the moca and an item response theory analysis. Int. Psychogeriatr. 2012, 24, 651–658. [Google Scholar] [CrossRef]
- Wechsler, D.A. Wechsler Memory Scale for Adults, 3rd ed.; The Psychological Corporation: San Antonio, TX, USA, 1997. [Google Scholar]
- Sink, K.M.; Espeland, M.A.; Castro, C.M.; Church, T.; Cohen, R.; Dodson, J.A.; Guralnik, J.; Hendrie, H.C.; Jennings, J.; Katula, J.; et al. Effect of a 24-month physical activity intervention vs health education on cognitive outcomes in sedentary older adults: The life randomized trial. JAMA 2015, 314, 781–790. [Google Scholar] [CrossRef]
- Liou, Y.M.; Jwo, C.J.; Yao, K.G.; Chiang, L.C.; Huang, L.H. Selection of appropriate Chinese terms to represent intensity and types of physical activity terms for use in the Taiwan version of IPAQ. J. Nurs. Res. 2008, 16, 252–263. [Google Scholar] [CrossRef] [PubMed]
- Radloff, L.S. The ces-d scale:A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Bhupathiraju, S.N.; Wedick, N.M.; Pan, A.; Manson, J.E.; Rexrode, K.M.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Quantity and variety in fruit and vegetable intake and risk of coronary heart disease. Am. J. Clin. Nutr. 2013, 98, 1514–1523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richard, E.L.; Laughlin, G.A.; Kritz-Silverstein, D.; Reas, E.T.; Barrett-Connor, E.; McEvoy, L.K. Dietary patterns and cognitive function among older community-dwelling adults. Nutrients 2018, 10, 1088. [Google Scholar] [CrossRef] [PubMed]
- Soni, M.; Rahardjo, T.B.; Soekardi, R.; Sulistyowati, Y.; Lestariningsih; Yesufu-Udechuku, A.; Irsan, A.; Hogervorst, E. Phytoestrogens and cognitive function: A review. Maturitas 2014, 77, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, G.; Baroni, L. Soy, soy foods and their role in vegetarian diets. Nutrients 2018, 10, 43. [Google Scholar] [CrossRef] [PubMed]
- Keinan-Boker, L.; Peeters, P.H.M.; Mulligan, A.A.; Navarro, C.; Slimani, N.; Mattisson, I.; Lundin, E.; McTaggart, A.; Allen, N.E.; Overvad, K.; et al. Soy product consumption in 10 european countries: The european prospective investigation into cancer and nutrition (epic) study. Public Health Nutr. 2007, 5, 1217–1226. [Google Scholar] [CrossRef] [PubMed]
- Messina, M. Soy and health update: Evaluation of the clinical and epidemiologic literature. Nutrients 2016, 8, 754. [Google Scholar] [CrossRef]
- Berr, C.; Portet, F.; Carriere, I.; Akbaraly, T.N.; Feart, C.; Gourlet, V.; Combe, N.; Barberger-Gateau, P.; Ritchie, K. Olive oil and cognition: Results from the three-city study. Dement. Geriatr. Cogn. Disord. 2009, 28, 357–364. [Google Scholar] [CrossRef]
- Naqvi, A.Z.; Harty, B.; Mukamal, K.J.; Stoddard, A.M.; Vitolins, M.; Dunn, J.E. Monounsaturated, trans, and saturated fatty acids and cognitive decline in women. J. Am. Geriatr. Soc. 2011, 59, 837–843. [Google Scholar] [CrossRef]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Stampfer, M.J.; Willett, W.C. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Guenther, P.M.; Reedy, J.; Krebs-Smith, S.M. Development of the healthy eating index-2005. J. Am. Diet. Assoc. 2008, 108, 1896–1901. [Google Scholar] [CrossRef] [PubMed]
- Shatenstein, B.; Nadon, S.; Godin, C.; Ferland, G. Diet quality of montreal-area adults needs improvement: Estimates from a self-administered food frequency questionnaire furnishing a dietary indicator score. J. Am. Diet. Assoc. 2005, 105, 1251–1260. [Google Scholar] [CrossRef] [PubMed]
- Smyth, A.; Dehghan, M.; O’Donnell, M.; Anderson, C.; Teo, K.; Gao, P.; Sleight, P.; Dagenais, G.; Probstfield, J.L.; Mente, A.; et al. Healthy eating and reduced risk of cognitive decline: A cohort from 40 countries. Neurology 2015, 84, 2258–2265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kesse-Guyot, E.; Amieva, H.; Castetbon, K.; Henegar, A.; Ferry, M.; Jeandel, C.; Hercberg, S.; Galan, P.; Group, S.V.M.R. Adherence to nutritional recommendations and subsequent cognitive performance: Findings from the prospective supplementation with antioxidant vitamins and minerals 2 (su.Vi.Max 2) study. Am. J. Clin. Nutr. 2011, 93, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Frisardi, V.; Panza, F.; Seripa, D.; Imbimbo, B.P.; Vendemiale, G.; Pilotto, A.; Solfrizzi, V. Nutraceutical properties of mediterranean diet and cognitive decline: Possible underlying mechanisms. J. Alzheimers Dis. 2010, 22, 715–740. [Google Scholar] [CrossRef] [PubMed]
- Steele, M.; Stuchbury, G.; Munch, G. The molecular basis of the prevention of alzheimer’s disease through healthy nutrition. Exp. Gerontol. 2007, 42, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Caracciolo, B.; Xu, W.; Collins, S.; Fratiglioni, L. Cognitive decline, dietary factors and gut-brain interactions. Mech. Ageing Dev. 2014, 136, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Justin, B.N.; Turek, M.; Hakim, A.M. Heart disease as a risk factor for dementia. Clin. Epidemiol. 2013, 5, 135–145. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, J.T.; Erkinjuntti, T.; Reisberg, B.; Roman, G.; Sawada, T.; Pantoni, L.; Bowler, J.V.; Ballard, C.; DeCarli, C.; Gorelick, P.B.; et al. Vascular cognitive impairment. Lancet Neurol. 2003, 2, 89–98. [Google Scholar] [CrossRef]
- Ye, X.; Bhupathiraju, S.N.; Tucker, K.L. Variety in fruit and vegetable intake and cognitive function in middle-aged and older Puerto Rican adults. Br. J. Nutr. 2013, 109, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Chu, Y.F.; Sun, J.; Wu, X.; Liu, R.H. Antioxidant and antiproliferative activities of common vegetables. J. Agric. Food Chem. 2002, 50, 6910–6916. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C.; Evans, D.A.; Tangney, C.C.; Bienias, J.L.; Wilson, R.S. Associations of vegetable and fruit consumption with age-related cognitive change. Neurology 2006, 67, 1370–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCrory, M.A.; Fuss, P.J.; McCallum, J.E.; Yao, M.; Vinken, A.G.; Hays, N.P.; Roberts, S.B. Dietary variety within food groups: Association with energy intake and body fatness in men and women. Am. J. Clin. Nutr. 1999, 69, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Fulton, S.L.; McKinley, M.C.; Young, I.S.; Cardwell, C.R.; Woodside, J.V. The effect of increasing fruit and vegetable consumption on overall diet: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2016, 56, 802–816. [Google Scholar] [CrossRef] [PubMed]
- Foote, J.A.; Murphy, S.P.; Wilkens, L.R.; Basiotis, P.P.; Carlson, A. Dietary variety increases the probability of nutrient adequacy among adults. J. Nutr. 2004, 134, 1779–1785. [Google Scholar] [CrossRef] [PubMed]
- Berkowitz, C.L.; Mosconi, L.; Rahman, A.; Scheyer, O.; Hristov, H.; Isaacson, R.S. Clinical application of APOE in Alzheimer’s prevention: A precision medicine approach. J. Prev. Alzheimers Dis. 2018, 5, 245–252. [Google Scholar]
- Alles, B.; Samieri, C.; Feart, C.; Jutand, M.A.; Laurin, D.; Barberger-Gateau, P. Dietary patterns: A novel approach to examine the link between nutrition and cognitive function in older individuals. Nutr. Res. Rev. 2012, 25, 207–222. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Diet Quality (mAHEI) | p-Value | |||
|---|---|---|---|---|---|
| Overall | Low (T1) | Moderate (T2) | High (T3) | ||
| (n = 436) | (n = 145) | (n = 146) | (n = 145) | ||
| Mean, SD | |||||
| mAHEI | 36.5, 7.6 | 28.1, 4.1 | 36.6, 2.0 | 44.9, 3.6 | <0.0001 |
| Vegetable variety 1 | 3.4, 1.0 | 3.1, 1.1 | 3.3, 0.9 | 3.9, 0.8 | <0.0001 |
| Age (years) | 72.5, 5.2 | 72.8, 5.2 | 71.4, 4.7 | 73.1, 5.6 | 0.01 |
| Years of education (years) | 14.0, 3.4 | 13.5, 3.4 | 14.1, 3.3 | 14.4, 3.6 | 0.08 |
| BMI (kg/m2) | 23.8, 2.9 | 24.1, 2.8 | 23.9, 3.1 | 23.5, 2.9 | 0.26 |
| Physical activity (MET-min/week) | 1747.5, 1444.0 | 1494.5, 1418.4 | 1821.7, 1506.7 | 1925.9, 1377.6 | 0.03 |
| Gait speed (m/s) | 0.8, 0.2 | 0.8, 0.2 | 0.9, 0.2 | 0.9, 0.3 | 0.04 |
| Total energy intake (kcal/day) | 1683.0, 395.1 | 1632.8, 415.6 | 1684.5, 377.4 | 1731.6, 387.9 | 0.10 |
| MoCA-T | 27.0, 2.1 | 27.0, 2.1 | 27.1, 2.1 | 27.0, 2.2 | 0.86 |
| N (%) | |||||
| Women | 231 (53) | 75 (52) | 81 (55) | 75 (52) | 0.76 |
| Annual disposable income (TWD per year) | <0.0001 | ||||
| <300 K | 68 (16) | 30 (23) | 18 (13) | 20 (14) | |
| 300–800 K | 106 (26) | 47 (35) | 31 (22) | 28 (20) | |
| 800–1000 K | 61 (15) | 18 (13) | 10 (7) | 33 (24) | |
| >1000 K | 177 (43) | 38 (29) | 81 (58) | 58 (42) | |
| Supplement use | 346 (79) | 113 (78) | 124 (85) | 109 (75) | 0.11 |
| Depressive symptoms 2 | 43 (10) | 18 (12) | 14 (10) | 11 (8) | 0.38 |
| Hypertension | 280 (65) | 106 (74) | 89 (61) | 85 (60) | 0.02 |
| Diabetes mellitus | 68 (16) | 24 (17) | 27 (18) | 17 (12) | 0.26 |
| APOE e4 carriers | 67 (16) | 20 (14) | 24 (17) | 23 (16) | 0.83 |
| Cognitive Function | Diet Quality | β (95% CI) 1,3 | N (Decliners/Non-Decliners) | AOR (95% CI) 2,3 |
|---|---|---|---|---|
| Global cognition | ||||
| MoCA-T | Low (T1) | Ref. | 71/74 | 1.00 |
| Moderate (T2) | 0.02 (−0.45, 0.50) | 58/88 | 0.87 (0.50, 1.51) | |
| High (T3) | 0.54 (0.06, 1.02) | 48/97 | 0.54 (0.31, 0.95) | |
| ptrend4 = 0.02 | ptrend4 = 0.03 | |||
| Cognitive domains (composite Z score for each domain) | ||||
| Logical memory | Low (T1) | Ref. | 55/90 | 1.00 |
| Moderate (T2) | 0.08 (−0.08, 0.23) | 42/104 | 1.13 (0.62, 2.07) | |
| High (T3) | 0.09 (−0.06, 0.24) | 48/97 | 0.76 (0.42, 1.38) | |
| ptrend4 = 0.23 | ptrend4 = 0.38 | |||
| Verbal fluency | Low (T1) | Ref. | 55/90 | 1.00 |
| Moderate (T2) | −0.004 (−0.12, 0.11) | 42/104 | 1.18 (0.69, 2.03) | |
| High (T3) | 0.07 (−0.05, 0.19) | 48/97 | 0.94 (0.53, 1.64) | |
| ptrend4 = 0.23 | ptrend4 = 0.84 | |||
| Executive function | Low (T1) | Ref. | 43/101 | 1.00 |
| Moderate (T2) | −0.06 (−0.22, 0.10) | 55/91 | 1.27 (0.75, 2.13) | |
| High (T3) | −0.07 (−0.23, 0.09) | 46/97 | 1.12 (0.65, 1.91) | |
| ptrend4 = 0.38 | ptrend4 =0.68 | |||
| Attention | Low (T1) | Ref. | 55/89 | 1.00 |
| Moderate (T2) | −0.008 (−0.13, 0.11) | 57/89 | 1.03 (0.60, 1.76) | |
| High (T3) | 0.12 (0.0003, 0.25) | 38/105 | 0.56 (0.32, 0.99) | |
| ptrend4 = 0.05 | ptrend4 = 0.049 | |||
| Cognitive Function | Quantity-Adjusted Vegetable Variety | β (95% CI) 1,3 | N (Decliners/Non-Decliners) | AOR (95% CI) 2,3 |
|---|---|---|---|---|
| Global cognition | ||||
| MoCA-T | Low (T1) | Ref. | 56/93 | 1.00 |
| Moderate (T2) | −0.15 (−0.62, 0.32) | 63/80 | 1.11 (0.64, 1.95) | |
| High (T3) | −0.07 (−0.54, 0.40) | 58/86 | 0.87 (0.50, 1.52) | |
| ptrend4 = 0.77 | ptrend4 = 0.61 | |||
| Cognitive domains (composite Z score for each domain) | ||||
| Logical memory | Low (T1) | Ref. | 42/107 | 1.00 |
| Moderate (T2) | 0.02 (−0.13, 0.17) | 49/94 | 1.04 (0.57, 1.91) | |
| High (T3) | −0.12 (−0.27, 0.03) | 54/90 | 1.21 (0.67, 2.20) | |
| ptrend4 = 0.12 | ptrend4 = 0.52 | |||
| Verbal fluency | Low (T1) | Ref. | 42/107 | 1.00 |
| Moderate (T2) | −0.04 (−0.16, 0.07) | 49/94 | 1.34 (0.77, 2.33) | |
| High (T3) | −0.03 (−0.14, 0.09) | 54/90 | 1.32 (0.76, 2.29) | |
| ptrend4 = 0.67 | ptrend4 = 0.32 | |||
| Executive function | Low (T1) | Ref. | 55/91 | 1.00 |
| Moderate (T2) | 0.10 (−0.06, 0.25) | 46/97 | 0.73 (0.43, 1.22) | |
| High (T3) | 0.08 (−0.08, 0.24) | 43/101 | 0.62 (0.37, 1.04) | |
| ptrend4 = 0.32 | ptrend4 = 0.07 | |||
| Attention | Low (T1) | Ref. | 55/91 | 1.00 |
| Moderate (T2) | 0.08 (−0.04, 0.20) | 46/97 | 0.82 (0.48, 1.42) | |
| High (T3) | 0.08 (−0.04, 0.20) | 49/95 | 0.79 (0.46, 1.36) | |
| ptrend4 = 0.20 | ptrend4 = 0.39 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, Y.-C.; Lee, M.-S.; Chiou, J.-M.; Chen, T.-F.; Chen, Y.-C.; Chen, J.-H. Association of Diet Quality and Vegetable Variety with the Risk of Cognitive Decline in Chinese Older Adults. Nutrients 2019, 11, 1666. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071666
Chou Y-C, Lee M-S, Chiou J-M, Chen T-F, Chen Y-C, Chen J-H. Association of Diet Quality and Vegetable Variety with the Risk of Cognitive Decline in Chinese Older Adults. Nutrients. 2019; 11(7):1666. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071666
Chicago/Turabian StyleChou, Yi-Chun, Meei-Shyuan Lee, Jeng-Min Chiou, Ta-Fu Chen, Yen-Ching Chen, and Jen-Hau Chen. 2019. "Association of Diet Quality and Vegetable Variety with the Risk of Cognitive Decline in Chinese Older Adults" Nutrients 11, no. 7: 1666. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071666