Microencapsulated Pomegranate Reverts High-Density Lipoprotein (HDL)-Induced Endothelial Dysfunction and Reduces Postprandial Triglyceridemia in Women with Acute Coronary Syndrome

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Preparation of MiPo
2.3. Dietary Interventions
2.4. Laboratory Analysis
2.5. HDL Subclasses Assessment
2.6. Vascular Reactivity of Aorta Rings
2.7. Paraoxonase–1 (PON1) Activity
2.8. Data Analysis
3. Results
3.1. Study Population
3.2. Biochemical Parameter Profile
3.3. HDL Lipid Profile
3.4. HDL Size Distribution
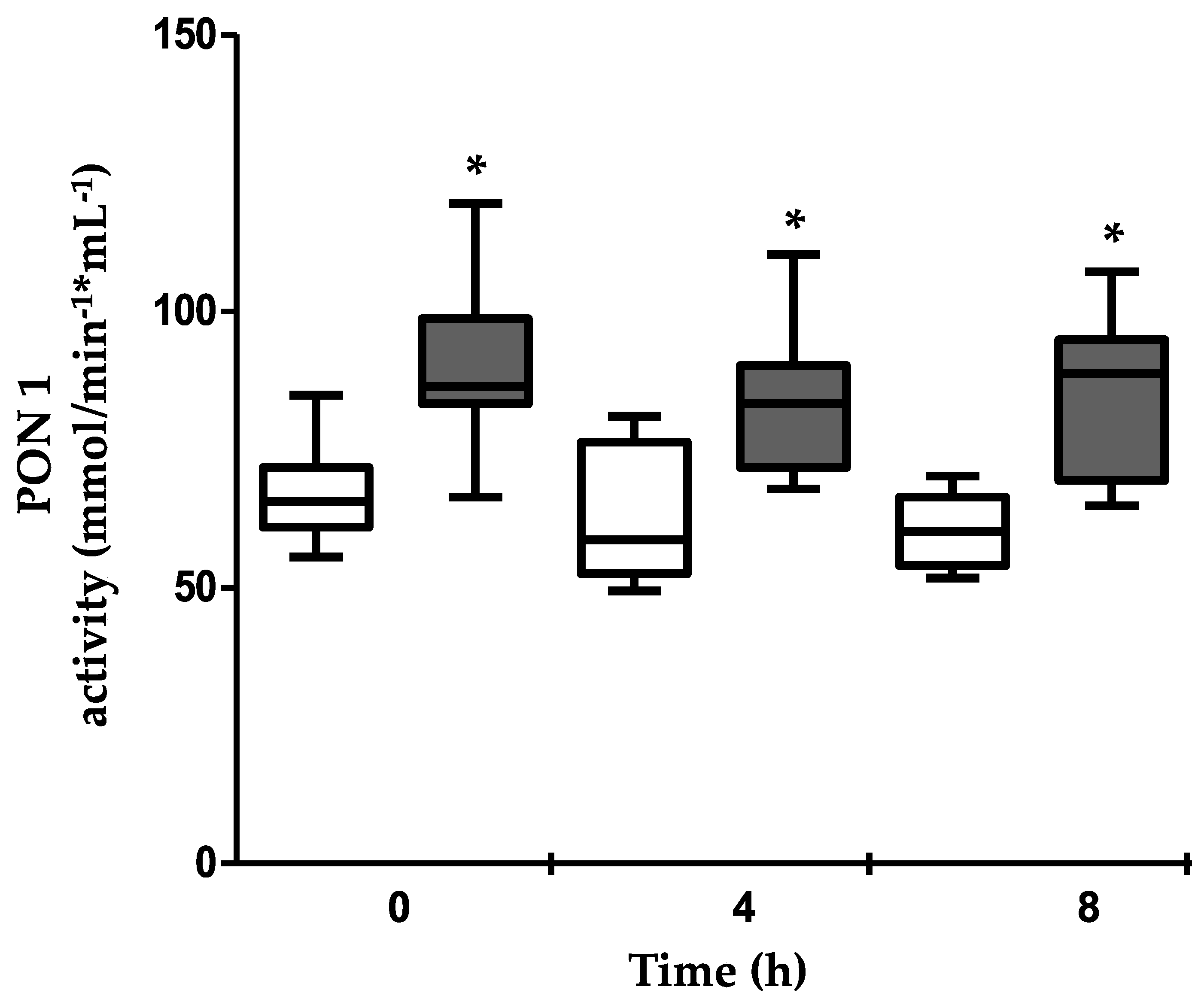
3.5. PON1 Activity
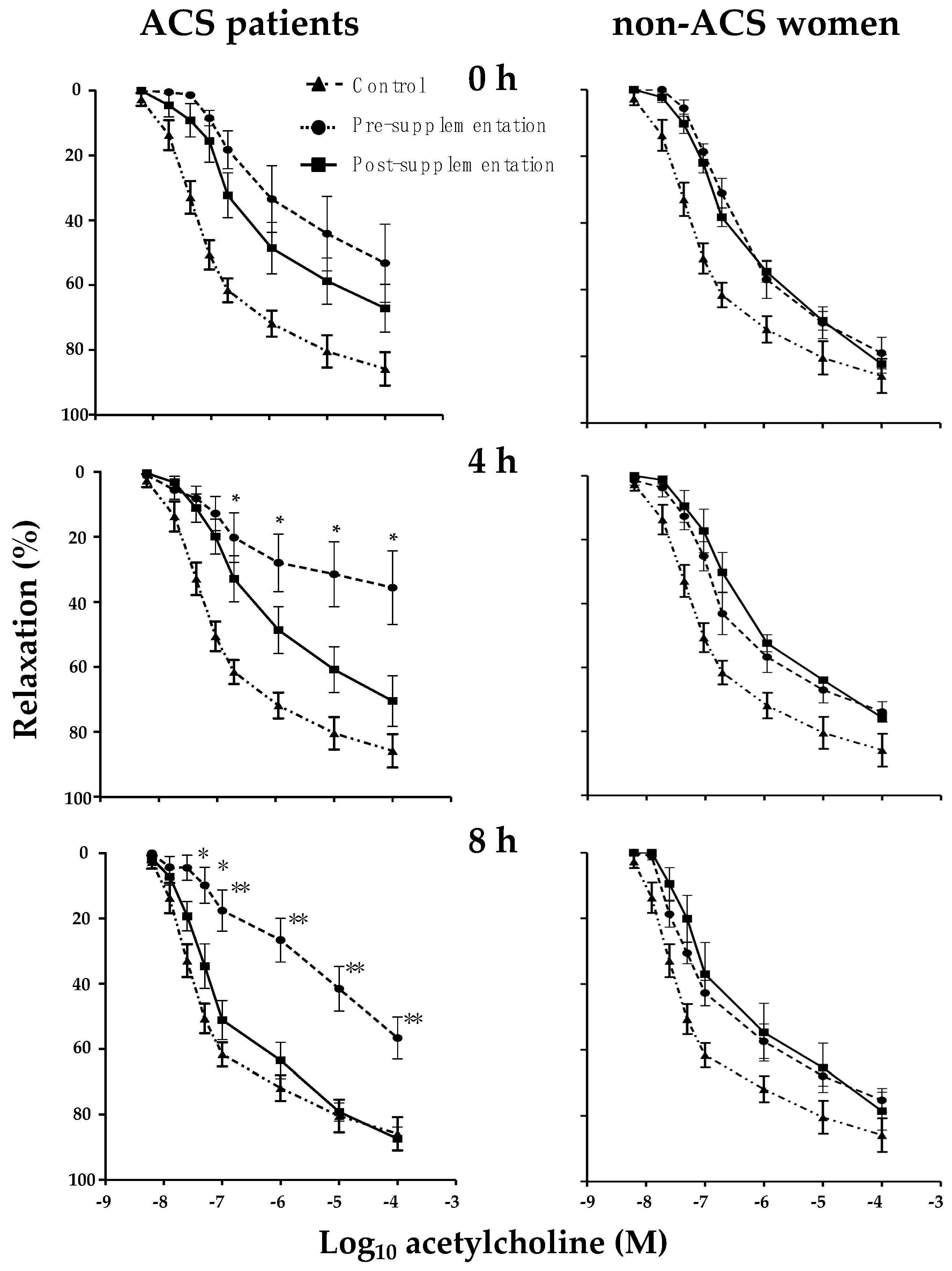
3.6. Effect of MiPo on Aortic Rings Incubated with HDL of ACS Women
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Estrada-Luna, D.; Ortiz-Rodriguez, M.A.; Medina-Briseno, L.; Carreon-Torres, E.; Izquierdo-Vega, J.A.; Sharma, A.; Cancino-Diaz, J.C.; Perez-Mendez, O.; Belefant-Miller, H.; Betanzos-Cabrera, G. Current therapies focused on high-density lipoproteins associated with cardiovascular disease. Molecules 2018, 23, 2730. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.H. Biomedicinal implications of high-density lipoprotein: Its composition, structure, functions, and clinical applications. BMB Rep. 2009, 42, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Méndez, Ó.; Pacheco, H.G.; Martínez-Sánchez, C.; Franco, M. HDL-cholesterol in coronary artery disease risk: function or structure? Clin. Chim. Acta 2014, 429, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Annema, W.; von Eckardstein, A. High-density lipoproteins. Multifunctional but vulnerable protections from atherosclerosis. Circ. J. 2013, 77, 2432–2448. [Google Scholar] [CrossRef] [PubMed]
- Camont, L.; Lhomme, M.; Rached, F.; Le Goff, W.; Nègre-Salvayre, A.; Salvayre, R.; Calzada, C.; Lagarde, M.; Chapman, M.J.; Kontush, A.; et al. Small, dense high-density lipoprotein–3 particles are enriched in negatively charged phospholipids: Relevance to cellular cholesterol efflux, antioxidative, antithrombotic, anti-inflammatory, and antiapoptotic functionalities. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 2715–2723. [Google Scholar] [CrossRef] [PubMed]
- Quintanilla-Cantú, A.; Peña-de-la-Sancha, P.; Flores-Castillo, C.; Mejía-Dominguez, A.M.; Posadas-Sánchez, R.; Pérez-Hernández, N.; Bautista-Pérez, R.; Enréquez-Calderón, R.E.; Juárez-Oropeza, M.A.; Fragoso, J.M.; et al. Small HDL subclasses become cholesterol-poor during postprandial period after a fat diet intake in subjects with high triglyceridemia increases. Clin. Chim. Acta 2017, 464, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Bellanger, N.; Julia, Z.; Villard, E.F.; El Khoury, P.; Duchene, E.; Chapman, M.J.; Fournier, N.; Le Goff, W.; Guerin, M. Functionality of postprandial larger HDL2 particles is enhanced following CETP inhibition therapy. Atherosclerosis 2012, 221, 160–168. [Google Scholar] [CrossRef]
- Beer, S.; Moren, X.; Ruiz, J.; James, R.W. Postprandial modulation of serum paraoxonase activity and concentration in diabetic and non-diabetic subjects. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 457–465. [Google Scholar] [CrossRef]
- Woodman, R.J.; Chew, G.T.; Watts, G.F. Mechanisms, significance and treatment of vascular dysfunction in type 2 diabetes mellitus: Focus on lipid-regulating therapy. Drugs 2005, 65, 31–74. [Google Scholar] [CrossRef]
- Pagidipati, N.J.; Peterson, E.D. Acute coronary syndromes in women and men. Nat. Rev. Cardiol. 2016, 13, 471–480. [Google Scholar] [CrossRef]
- Cattaneo, M.G.; Vanetti, C.; Decimo, I.; Di Chio, M.; Martano, G.; Garrone, G.; Bifari, F.; Vicentini, L.M. Sex-specific eNOS activity and function in human endothelial cells. Sci. Rep. 2017, 7, 9612. [Google Scholar] [CrossRef] [PubMed]
- Mineo, C.; Deguchi, H.; Griffin, J.H.; Shaul, P.W. Endothelial and antithrombotic actions of HDL. Circ. Res. 2006, 98, 1352–1364. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Vega, M.; Massó, F.; Páez, A.; Vargas-Alarcón, G.; Coral-Vázquez, R.; Mas-Oliva, J.; Carreón-Torres, E.; Pérez-Méndez, Ó. HDL-Mediated lipid influx to endothelial cells contributes to regulating Intercellular Adhesion Molecule (ICAM)—1 Expression and eNOS Phosphorylation. Int. J. Mol. Sci. 2018, 19, 3394. [Google Scholar] [CrossRef] [PubMed]
- Taheri Rouhi, S.Z.; Sarker, M.M.R.; Rahmat, A.; Alkahtani, S.A.; Othman, F. The effect of pomegranate fresh juice versus pomegranate seed powder on metabolic indices, lipid profile, inflammatory biomarkers, and the histopathology of pancreatic islets of Langerhans in streptozotocin-nicotinamide induced type 2 diabetic Sprague-Dawley rats. BMC Complement. Altern. Med. 2017, 17, 156. [Google Scholar]
- Estrada-Luna, D.; Martinez-Hinojosa, E.; Cancino-Diaz, J.C.; Belefant-Miller, H.; Lopez-Rodriguez, G.; Betanzos-Cabrera, G. Daily supplementation with fresh pomegranate juice increases paraoxonase 1 expression and activity in mice fed a high-fat diet. Eur. J. Nutr. 2018, 57, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Shishehbor, F.; Mohammad Shahi, M.; Zarei, M.; Saki, A.; Zakerkish, M.; Shirani, F.; Zare, M. Effects of concentrated pomegranate juice on subclinical inflammation and cardiometabolic risk factors for type 2 diabetes: A Quasi-Experimental Study. Int. J. Endocrinol. Metab. 2016, 14, e33835. [Google Scholar] [CrossRef] [PubMed]
- Rom, O.; Volkova, N.; Jeries, H.; Grajeda-Iglesias, C.; Aviram, M. Exogenous (pomegranate juice) or endogenous (paraoxonase–1) antioxidants decrease triacylglycerol accumulation in mouse cardiovascular disease-related tissues. Lipids 2018, 53, 1031–1041. [Google Scholar] [CrossRef]
- Wu, S.; Tian, L. Diverse phytochemicals and bioactivities in the ancient fruit and modern functional food pomegranate (Punica granatum). Molecules 2017, 22, 1606. [Google Scholar] [CrossRef]
- Huesca-Gomez, C.; Franco, M.; Luc, G.; Montano, L.F.; Masso, F.; Posadas-Romero, C.; Perez-Mendez, O. Chronic hypothyroidism induces abnormal structure of high-density lipoproteins and impaired kinetics of apolipoprotein A-I in the rat. Metabolism 2002, 51, 443–450. [Google Scholar] [CrossRef]
- Toledo-Ibelles, P.; Garcia-Sanchez, C.; Avila-Vazzini, N.; Carreon-Torres, E.; Posadas-Romero, C.; Vargas-Alarcon, G.; Perez-Mendez, O. Enzymatic assessment of cholesterol on electrophoresis gels for estimating HDL size distribution and plasma concentrations of HDL subclasses. J. Lipid. Res. 2010, 51, 1610–1617. [Google Scholar] [CrossRef] [Green Version]
- Bautista, R.; Carreon-Torres, E.; Luna-Luna, M.; Komera-Arenas, Y.; Franco, M.; Fragoso, J.M.; Lopez-Olmos, V.; Cruz-Robles, D.; Vargas-Barron, J.; Vargas-Alarcon, G.; et al. Early endothelial nitrosylation and increased abdominal adiposity in Wistar rats after long-term consumption of food fried in canola oil. Nutrition 2014, 30, 1055–1060. [Google Scholar] [CrossRef] [PubMed]
- Gan, K.N.; Smolen, A.; Eckerson, H.W.; La Du, B.N. Purification of human serum paraoxonase/arylesterase. Evidence for one esterase catalyzing both activities. Drug Metab. Dispos. 1991, 19, 100–106. [Google Scholar] [PubMed]
- García-Sánchez, C.; Posadas-Romero, C.; Posadas-Sánchez, R.; Carreón-Torres, E.; Rodríguez-Pérez, J.M.; Juárez-Rojas, J.G.; Martínez-Sánchez, C.; Fragoso, J.M.; González-Pacheco, H.; Vargas-Alarcón, G.; et al. Low concentrations of phospholipids and plasma HDL cholesterol subclasses in asymptomatic subjects with high coronary calcium scores. Atherosclerosis 2015, 238, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Manthou, E.; Georgakouli, K.; Deli, C.K.; Sotiropoulos, A.; Fatouros, I.G.; Kouretas, D.; Haroutounian, S.; Matthaiou, C.; Koutedakis, Y.; Jamurtas, A.Z. Effect of pomegranate juice consumption on biochemical parameters and complete blood count. Exp. Ther. Med. 2017, 14, 1756–1762. [Google Scholar] [CrossRef] [PubMed]
- Asgary, S.; Sahebkar, A.; Afshani, M.R.; Keshvari, M.; Haghjooyjavanmard, S.; Rafieian-Kopaei, M. Clinical evaluation of blood pressure lowering, endothelial function improving, hypolipidemic and anti-inflammatory effects of pomegranate juice in hypertensive subjects. Phytother. Res. 2014, 28, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Dana, N.; Javanmard, S.H.; Rafiee, L. Role of peroxisome proliferator-activated receptor alpha and gamma in antiangiogenic effect of pomegranate peel extract. Iran. J. Basic Med. Sci. 2016, 19, 106–110. [Google Scholar] [PubMed]
- Khateeb, J.; Gantman, A.; Kreitenberg, A.J.; Aviram, M.; Fuhrman, B. Paraoxonase 1 (PON1) expression in hepatocytes is upregulated by pomegranate polyphenols: A role for PPAR-gamma pathway. Atherosclerosis 2010, 208, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Hontecillas, R.; Diguardo, M.; Duran, E.; Orpi, M.; Bassaganya-Riera, J. Catalpic acid decreases abdominal fat deposition, improves glucose homeostasis and upregulates PPAR alpha expression in adipose tissue. Clin. Nutr. 2008, 27, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Hontecillas, R.; O’Shea, M.; Einerhand, A.; Diguardo, M.; Bassaganya-Riera, J. Activation of PPAR gamma and alpha by punicic acid ameliorates glucose tolerance and suppresses obesity-related inflammation. J. Am. Coll. Nutr. 2009, 28, 184–195. [Google Scholar] [CrossRef]
- Zilversmit, D.B. Atherogenesis: A postprandial phenomenon. Circulation 1979, 60, 473–485. [Google Scholar] [CrossRef]
- O’Keefe, J.H.; Bell, D.S. Postprandial hyperglycemia/hyperlipidemia (postprandial dysmetabolism) is a cardiovascular risk factor. Am. J. Cardiol. 2007, 100, 899–904. [Google Scholar] [CrossRef]
- Carstensen, M.; Thomsen, C.; Hermansen, K. Incremental area under response curve more accurately describes the triglyceride response to an oral fat load in both healthy and type 2 diabetic subjects. Metabolism 2003, 52, 1034–1037. [Google Scholar] [CrossRef]
- Persegol, L.; Darabi, M.; Dauteuille, C.; Lhomme, M.; Chantepie, S.; Rye, K.A.; Therond, P.; Chapman, M.J.; Salvayre, R.; Negre-Salvayre, A.; et al. Small dense HDLs display potent vasorelaxing activity, reflecting their elevated content of sphingosine–1-phosphate. J. Lipid Res. 2018, 59, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Rosenblat, M.; Aviram, M. Paraoxonases role in the prevention of cardiovascular diseases. Biofactors 2009, 35, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, J.; Boutjdir, M.; Rudel, L.L.; Hussain, M.M. Intestine-specific MTP and global ACAT2 deficiency lowers acute cholesterol absorption with chylomicrons and HDLs. J. Lipid Res. 2014, 55, 2261–2275. [Google Scholar] [CrossRef] [Green Version]
- Lv, O.; Wang, L.; Li, J.; Ma, Q.; Zhao, W. Effects of pomegranate peel polyphenols on lipid accumulation and cholesterol metabolic transformation in L–02 human hepatic cells via the PPARgamma-ABCA1/CYP7A1 pathway. Food Funct. 2016, 7, 4976–4983. [Google Scholar] [CrossRef]
- Niesor, E.J.; Chaput, E.; Mary, J.L.; Staempfli, A.; Topp, A.; Stauffer, A.; Wang, H.; Durrwell, A. Effect of compounds affecting ABCA1 expression and CETP activity on the HDL pathway involved in intestinal absorption of lutein and zeaxanthin. Lipids 2014, 49, 1233–1243. [Google Scholar] [CrossRef]
- Flores-Castillo, C.; Luna-Luna, M.; Carreón-Torres, E.; López-Olmos, V.; Frías, S.; Juárez-Oropeza, M.A.; Franco, M.; Fragoso, J.M.; Vargas-Alarcón, G.; Pérez-Méndez, Ó.; et al. Atorvastatin and fenofibrate increase the content of unsaturated acyl chains in HDL and modify in vivo kinetics of HDL-Cholesteryl esters in New Zealand white rabbits. Int. J. Mol. Sci. 2019, 20, 2521. [Google Scholar] [CrossRef]
- Martínez-Ramírez, M.; Madero, M.; Vargas-Alarcón, G.; Vargas-Barrón, J.; Fragoso, J.M.; Rodríguez-Pérez, J.M.; Martínez-Sánchez, C.; González-Pacheco, H.; Bautista-Pérez, R.; Carreón-Torres, E.; et al. HDL-sphingomyelin reduction after weight loss by an energy-restricted diet is associated with the improvement of lipid profile, blood pressure, and decrease of insulin resistance in overweight/obese patients. Clin. Chim. Acta 2016, 454, 77–81. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameters | Pre-Supplementation n = 11 | Post-Supplementation n = 11 | p Value * |
|---|---|---|---|
| Age (years) | 51.6 (41.2–60.98) | ||
| BMI (kg/m2) | 26.96 (24.61–29.32) | 26.37 (24.06–28.68) | 0.105 |
| Waist circumference (cm) | 92.45 (85.41–99.49) | 91.45 (84.36–98.58) | 0.009 |
| Systolic BP (mmHg) | 128.3 (113.5–143.1) | 121.5 (112.8–130.2) | 0.130 |
| Diastolic BP (mmHg) | 72.1 (62.1–82.1) | 72.4 (65.7–79.1) | 0.404 |
| Statins (n) | 8 | ||
| Beta blockers (n) | 6 | ||
| ACEI (n) | 3 | ||
| Nutrient intake: | |||
| Carbohydrates (%) | 51.4 (49.7–53.1) | 52.29 (50.65–53.94) | 0.640 |
| Lipids (%) | 20.27 (18.61–21.93) | 20.58 (19.1–22.07) | 0.705 |
| Protein (%) | 28.65 (27.88–29.42) | 28.47 (26.76–30.19) | 0.810 |
| Calories (kcal) | 1869.34 (1761.16–1977.52) | 1880.22 (1749.86–2010.58) | 0.705 |
| Parameter | Sample Time (n = 11) | |||
|---|---|---|---|---|
| 0 h | 4 h | 8 h | ||
| Glucose (mg/dL) | Pre | 88.3 (76.6–125.9) | 83.2 (67.9–113.9) | 88.9 (76.3–110.4) |
| Post | 79.7 (73.2–89.0) | 88.0 (78.7–95.3) | 89.2 (78.2–92.1) | |
| Total cholesterol (mg/dL) | Pre | 157.6 (146.5–219.8) | 150.9 (139.9–245.8) | 141.4 (130.2–254.4) |
| Post | 133.2 (87.1–140.7) a | 138.9 (127.2–149.0) b | 128.4 (103.3–148.6) c | |
| LDL-C (mg/dL) | Pre | 85.8 (69.1–161.1) | 73.4 (56.1–160.4) | 74.2 (52.1–180.0) |
| Post | 62.7 (34.1–88.5) a | 46.9 (40.6–63.6) b | 48.2 (34.2–65.3) c | |
| Triglycerides (mg/dL) | Pre | 125.4 (119.4–182.3) | 226.6 (190.0–344.2) a | 202.2 (156.6–322.9) a,b |
| Post | 105.1 (83.5–120.7) a | 207.5 (112.5–247.4) b,d | 117.2 (92.3–197.9) c,d,e | |
| iAUC (h × mg/dL) | Pre | 419.0 (315.3–1011.7) | ||
| Post | 382.8 (107.3–563.0) f | |||
| HDL-C (mg/dL) | Pre | 39.4 (35.7–56.7) | 38.0 (31.4–47) a | 36.6 (33.2–49.2) a |
| Post | 43.9 (40.2–62.6) a | 39.4 (35.8–53.3) d | 39.3 (36.8–49.3) c,d | |
| HDL-Tg (mg/dL) | Pre | 17.0 (14.6–25.5) | 20.1 (15.8–28.0) | 25.3 (16.3–30.8) |
| Post | 19.8 (19.4–31.4) | 22.9 (20.3–30.8) | 29.8 (23.9–36.7) c,d,e | |
| HDL-Pho (mg/dL) | Pre | 89.4 (75.4–115.4) | 93.2 (75.4–103.1) | 88.6 (72.1–122.0) |
| Post | 95.9 (80.8–113.0) | 90.2 (80.0–103.3) | 101.6 (91.2–129.3) c,d,e | |
| Ratios: | ||||
| HDL-C/HDL-Pho | Pre | 0.489 (0.399–0.559) | 0.433 (0.388–0.464) | 0.424 (0.388–0.464) |
| Post | 0.460 (0.421–0.595) | 0.429 (0.395–0.499) d | 0.363 (0.337–0.447) d,e | |
| HDL-Tg/HDL-Pho | Pre | 0.217 (0.146–0.287) | 0.232 (0.166–0.301) | 0.259 (0.201–0.339) |
| Post | 0.255 (0.194–0.288) | 0.234 (0.201–0.396) | 0.278 (0.208–0.375) | |
| HDL Subclasses (%) | Sample Time (n = 11) | |||
|---|---|---|---|---|
| 0 h | 4 h | 8 h | ||
| n = 11 | ||||
| HDL2b | Pre | 30.8 (15.9–35.0) | 31.5 (16.9–40.3) a | 38.6 (18.8–42.3) a |
| Post | 31.5 (17.3–40.3) a | 32.8 (19.3–40.7) b | 31.7 (18.2–42.1) | |
| HDL2a | Pre | 14.3 (10.9–16.4) | 15.0 (10.9–16.6) | 16.0 (12.5–18.7) |
| Post | 15.0 (12.3–17.9) | 14.6 (12.4–16.6) | 14.7 (10.6–16.9) | |
| HDL3a | Pre | 31.0 (27.8–35.9) | 29.2 (27.3–33.5) | 28.3 (25.9–32.8) a |
| Post | 27.7 (26.5–34.1) a | 29.5 (24.7–34.1) | 29.2 (26.0–33.3) | |
| HDL3b | Pre | 16.9 (12.5–21.8) | 14.1 (10.2–21.5) | 10.4 (7.8–21.2) a |
| Post | 14.7 (10.0–21.8) | 15.7 (8.2–25.6) | 15.3 (8.8–23.2) | |
| HDL3c | Pre | 6.2 (4.6–12.3) | 6.4 (3.4–19.3) | 4.4 (1.3–15.1) |
| Post | 5.1 (2.6–10.8) | 5.5 (2.3–16.8) | 7.9 (1.2–21.3) c | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Estrada-Luna, D.; Carreón-Torres, E.; Bautista-Pérez, R.; Betanzos-Cabrera, G.; Dorantes-Morales, A.; Luna-Luna, M.; Vargas-Barrón, J.; Mejía, A.M.; Fragoso, J.M.; Carvajal-Aguilera, K.; et al. Microencapsulated Pomegranate Reverts High-Density Lipoprotein (HDL)-Induced Endothelial Dysfunction and Reduces Postprandial Triglyceridemia in Women with Acute Coronary Syndrome. Nutrients 2019, 11, 1710. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11081710
Estrada-Luna D, Carreón-Torres E, Bautista-Pérez R, Betanzos-Cabrera G, Dorantes-Morales A, Luna-Luna M, Vargas-Barrón J, Mejía AM, Fragoso JM, Carvajal-Aguilera K, et al. Microencapsulated Pomegranate Reverts High-Density Lipoprotein (HDL)-Induced Endothelial Dysfunction and Reduces Postprandial Triglyceridemia in Women with Acute Coronary Syndrome. Nutrients. 2019; 11(8):1710. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11081710
Chicago/Turabian StyleEstrada-Luna, Diego, Elizabeth Carreón-Torres, Rocío Bautista-Pérez, Gabriel Betanzos-Cabrera, Alan Dorantes-Morales, María Luna-Luna, Jesús Vargas-Barrón, Ana María Mejía, José Manuel Fragoso, Karla Carvajal-Aguilera, and et al. 2019. "Microencapsulated Pomegranate Reverts High-Density Lipoprotein (HDL)-Induced Endothelial Dysfunction and Reduces Postprandial Triglyceridemia in Women with Acute Coronary Syndrome" Nutrients 11, no. 8: 1710. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11081710