Association between Macronutrient Intake and Excessive Daytime Sleepiness: An Iso-Caloric Substitution Analysis from the North West Adelaide Health Study

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
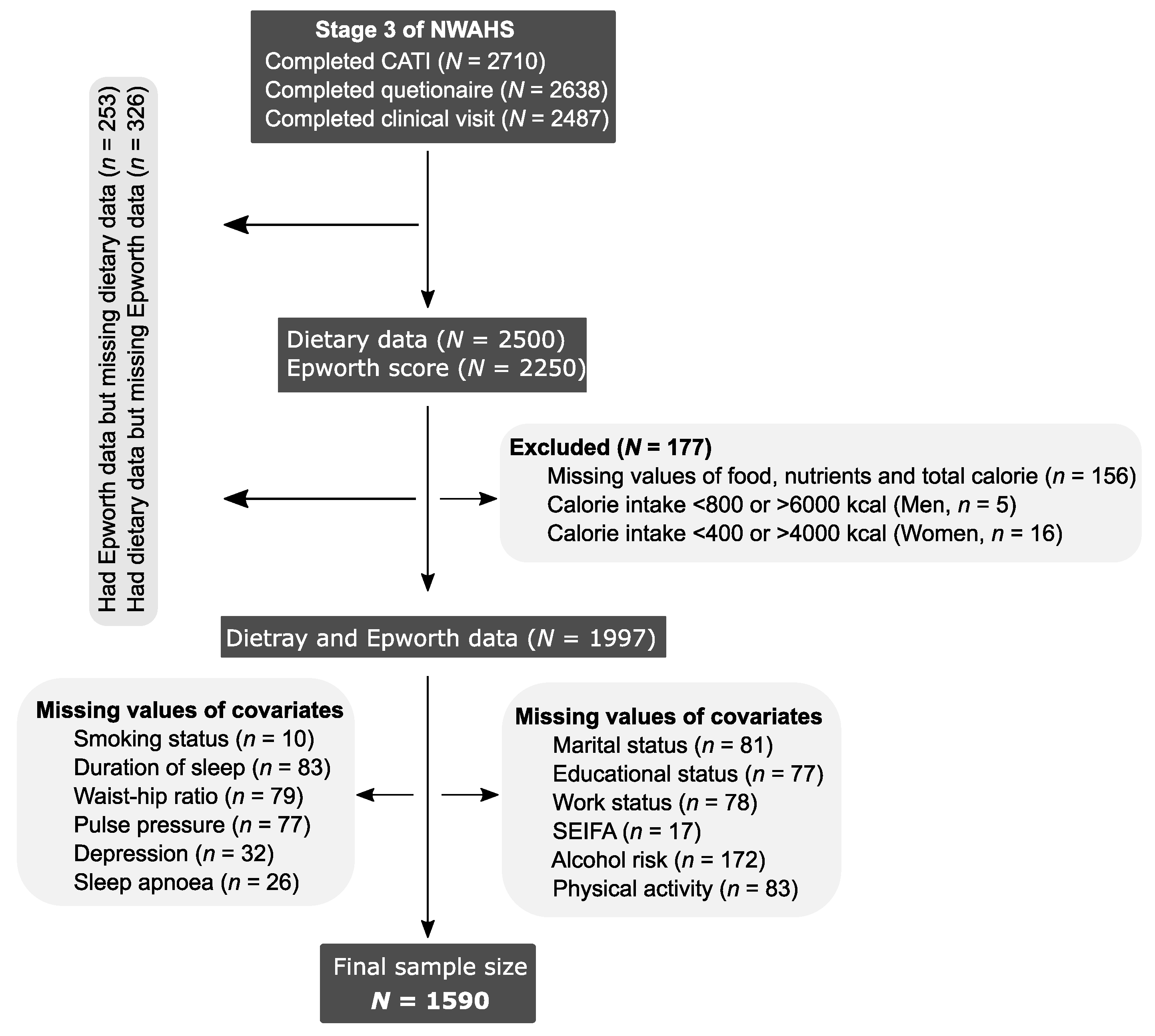
2.1. Study Design and Population
2.2. Assessment of Dietary and Nutrient Intakes
2.3. Outcome Variable
2.4. Covariates
2.5. Statistical Analysis
3. Results
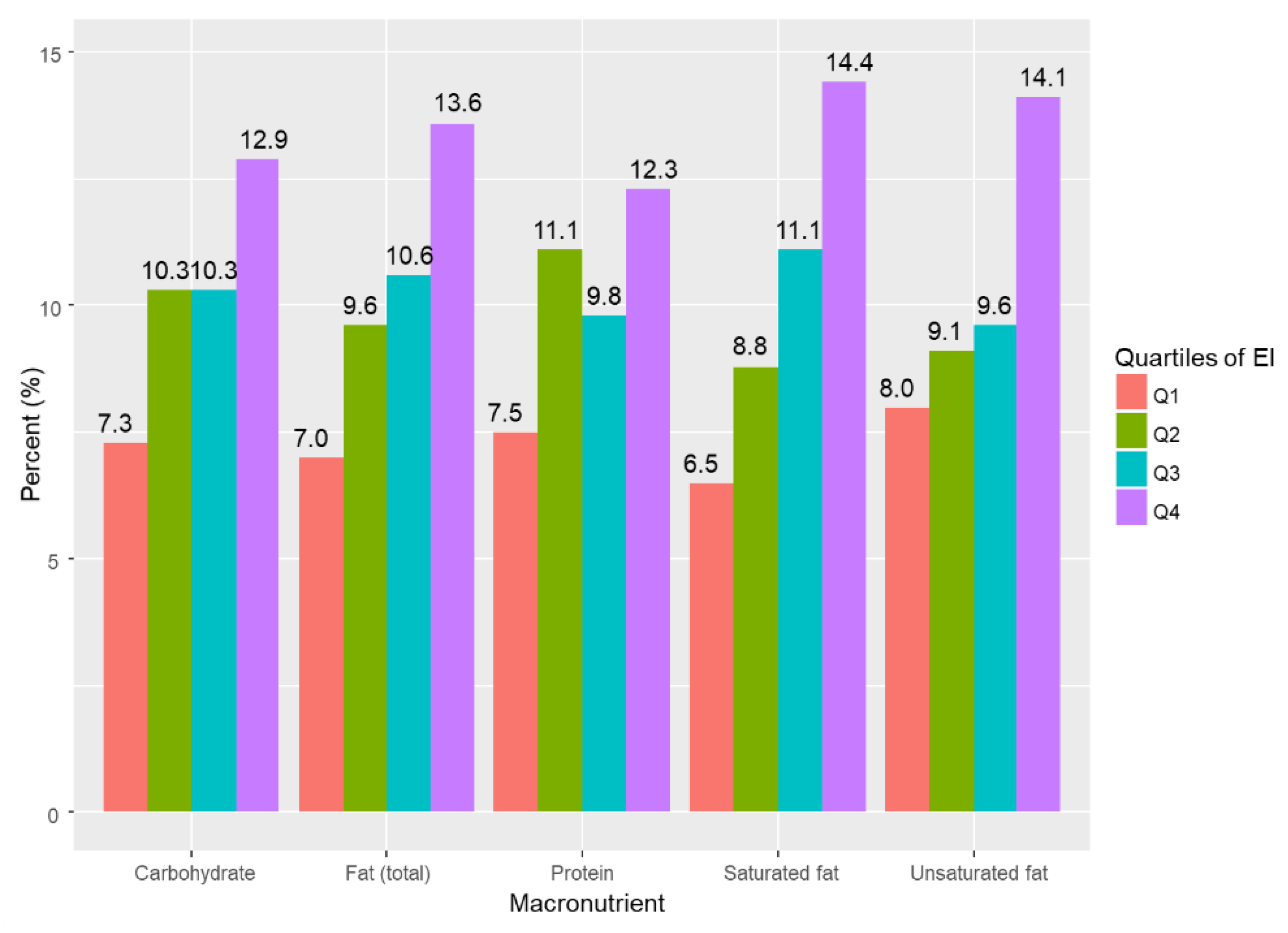
3.1. Participants’ Characteristics
3.2. Association between EI and EDS
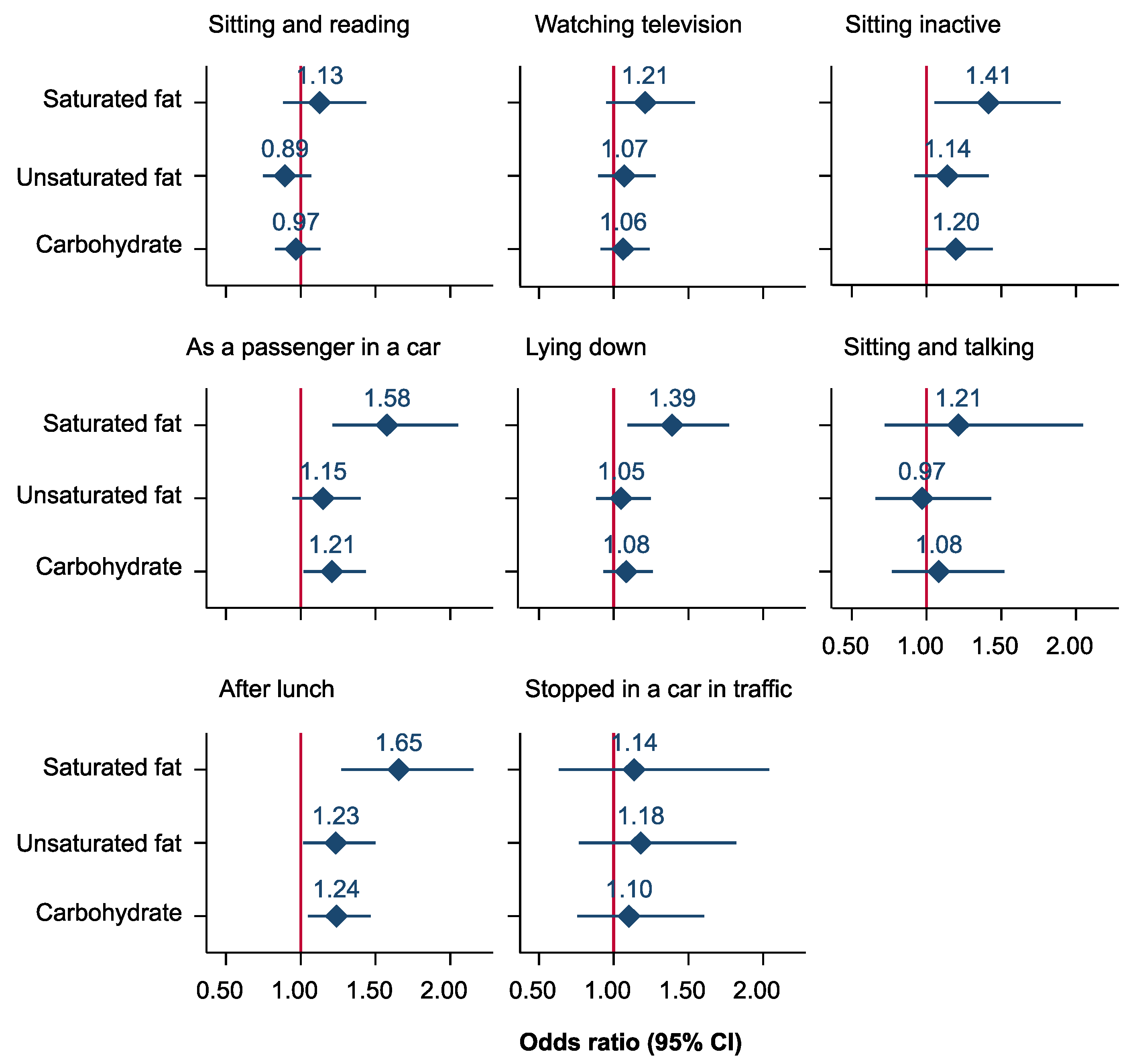
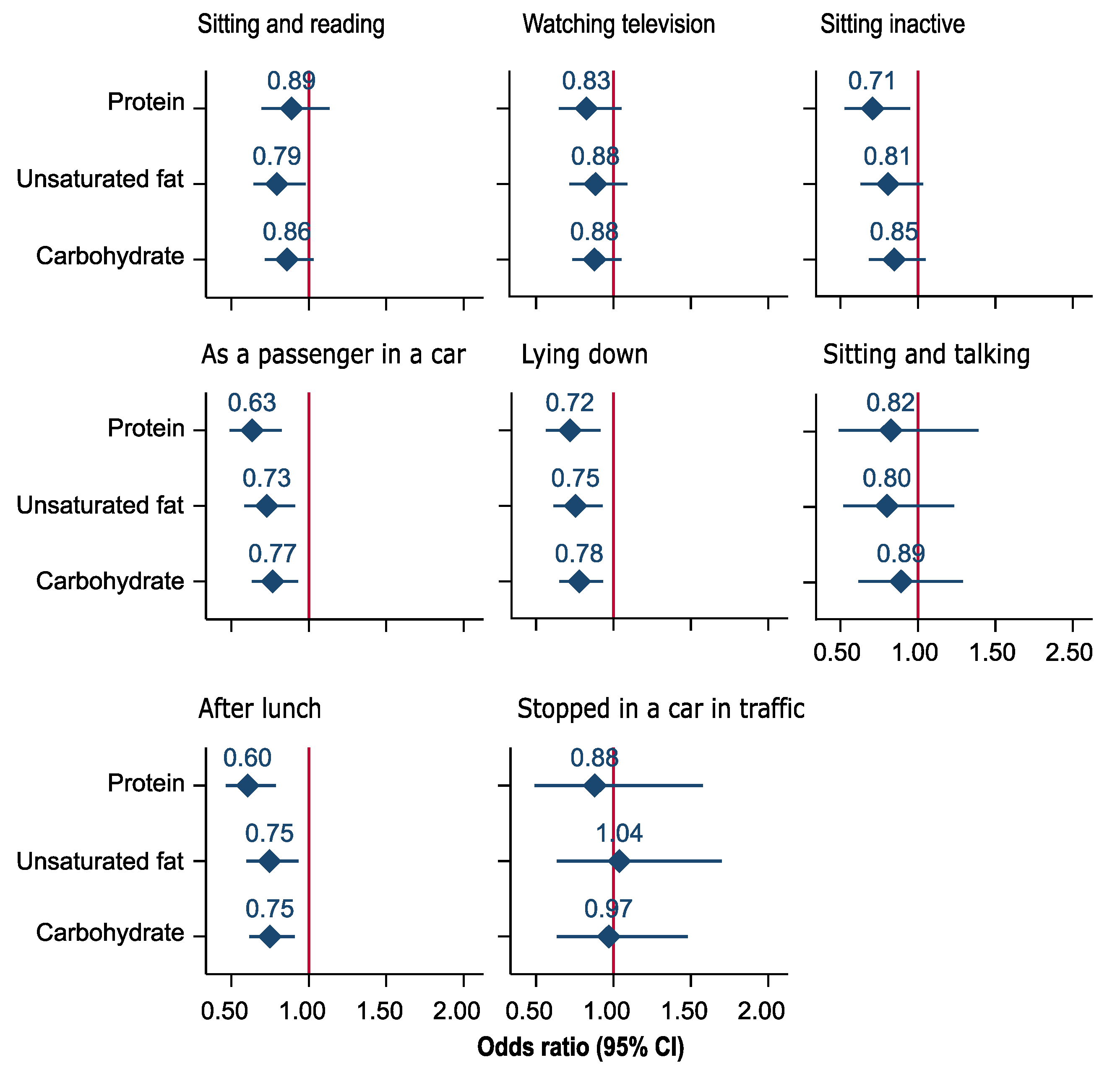
3.3. Substitution Models
4. Discussion
4.1. Comparison with Other Studies
4.2. Potential Mechanisms and Implications
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bittencourt, L.R.A.; Silva, R.S.; Santos, R.F.; Pires, M.L.N.; de Mello, M.T. Excessive daytime sleepiness. Braz. J. Psychiatry 2005, 27, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Cunningham, T.J.; Giles, W.H.; Croft, J.B. Trends in insomnia and excessive daytime sleepiness among U.S. adults from 2002 to 2012. Sleep Med. 2015, 16, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Lang, C.J.; Appleton, S.L.; Vakulin, A.; McEvoy, R.D.; Vincent, A.D.; Wittert, G.A.; Martin, S.A.; Grant, J.F.; Taylor, A.W.; Antic, N.; et al. Associations of Undiagnosed Obstructive Sleep Apnea and Excessive Daytime Sleepiness with Depression: An Australian Population Study. J. Clin. Sleep Med. 2017, 13, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Vashum, K.P.; McEvoy, M.A.; Hancock, S.J.; Islam, M.R.; Peel, R.; Attia, J.R.; Milton, A.H. Prevalence of and associations with excessive daytime sleepiness in an Australian older population. Asia Pac. J. 2015, 27, NP2275–NP2284. [Google Scholar] [CrossRef]
- Rakel, R.E. Clinical and societal consequences of obstructive sleep apnea and excessive daytime sleepiness. Postgrad Med. 2009, 121, 86–95. [Google Scholar] [CrossRef]
- Stevenson, M.R.; Elkington, J.; Sharwood, L.; Meuleners, L.; Ivers, R.; Boufous, S.; Williamson, A.; Haworth, N.; Quinlan, M.; Grunstein, R.; et al. The role of sleepiness, sleep disorders, and the work environment on heavy-vehicle crashes in 2 Australian states. Am. J. Epidemiol. 2014, 179, 594–601. [Google Scholar] [CrossRef]
- Ward, K.L.; Hillman, D.R.; James, A.; Bremner, A.P.; Simpson, L.; Cooper, M.N.; Palmer, L.J.; Fedson, A.C.; Mukherjee, S. Excessive daytime sleepiness increases the risk of motor vehicle crash in obstructive sleep apnea. J. Clin. Sleep Med. 2013, 9, 1013–1021. [Google Scholar] [CrossRef]
- Newman, A.B.; Spiekerman, C.F.; Enright, P.; Lefkowitz, D.; Manolio, T.; Reynolds, C.F.; Robbins, J. Daytime sleepiness predicts mortality and cardiovascular disease in older adults. The Cardiovascular Health Study Research Group. J. Am. Geriatr. Soc. 2000, 48, 115–123. [Google Scholar] [CrossRef]
- Fatani, A.; Al-Rouqi, K.; Al Towairky, J.; Ahmed, A.E.; Al-Jahdali, S.; Ali, Y.; Al-Shimemeri, A.; Al-Harbi, A.; Baharoon, S.; Khan, M.; et al. Effect of age and gender in the prevalence of excessive daytime sleepiness among a sample of the Saudi population. J. Epidemiol. Glob. Health 2015, 5 (Suppl. 1), S59–S66. [Google Scholar] [CrossRef] [Green Version]
- Dashti, H.S.; Scheer, F.A.; Jacques, P.F.; Lamon-Fava, S.; Ordovas, J.M. Short sleep duration and dietary intake: Epidemiologic evidence, mechanisms, and health implications. Adv. Nutr. 2015, 6, 648–659. [Google Scholar] [CrossRef]
- McClain, J.J.; Lewin, D.S.; Laposky, A.D.; Kahle, L.; Berrigan, D. Associations between physical activity, sedentary time, sleep duration and daytime sleepiness in US adults. Prev. Med. 2014, 66, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Panossian, L.A.; Veasey, S.C. Daytime sleepiness in obesity: Mechanisms beyond obstructive sleep apnea—A review. Sleep 2012, 35, 605–615. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.J.; Appleton, S.L.; Vakulin, A.; Lang, C.; Martin, S.A.; Taylor, A.W.; McEvoy, R.D.; Antic, N.A.; Catcheside, P.G.; Wittert, G.A. Association of daytime sleepiness with obstructive sleep apnoea and comorbidities varies by sleepiness definition in a population cohort of men. Respirology 2016, 21, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Bixler, E.O.; Vgontzas, A.N.; Lin, H.M.; Calhoun, S.L.; Vela-Bueno, A.; Kales, A. Excessive daytime sleepiness in a general population sample: The role of sleep apnea, age, obesity, diabetes, and depression. J. Clin. Endocrinol. Metab. 2005, 90, 4510–4515. [Google Scholar] [CrossRef]
- Maung, S.C.; El Sara, A.; Chapman, C.; Cohen, D.; Cukor, D. Sleep disorders and chronic kidney disease. World J. Nephrol. 2016, 5, 224–232. [Google Scholar] [CrossRef]
- Potter, G.D.M.; Cade, J.E.; Grant, P.J.; Hardie, L.J. Nutrition and the circadian system. Br. J. Nutr. 2016, 116, 434–442. [Google Scholar] [CrossRef] [Green Version]
- St-Onge, M.P.; Mikic, A.; Pietrolungo, C.E. Effects of Diet on Sleep Quality. Adv. Nutr. 2016, 7, 938–949. [Google Scholar] [CrossRef]
- Cao, Y.; Wittert, G.; Taylor, A.W.; Adams, R.; Shi, Z. Associations between Macronutrient Intake and Obstructive Sleep Apnoea as Well as Self-Reported Sleep Symptoms: Results from a Cohort of Community Dwelling Australian Men. Nutrients 2016, 8, 207. [Google Scholar] [CrossRef]
- Kwan, R.M.; Thomas, S.; Mir, M.A. Effects of a low carbohydrate isoenergetic diet on sleep behavior and pulmonary functions in healthy female adult humans. J. Nutr. 1986, 116, 2393–2402. [Google Scholar] [CrossRef]
- Wells, A.S.; Read, N.W.; Uvnas-Moberg, K.; Alster, P. Influences of fat and carbohydrate on postprandial sleepiness, mood, and hormones. Physiol. Behav. 1997, 61, 679–686. [Google Scholar] [CrossRef]
- St-Onge, M.-P.; Roberts, A.; Shechter, A.; Choudhury, A.R. Fiber and Saturated Fat Are Associated with Sleep Arousals and Slow Wave Sleep. J. Clin. Sleep Med. 2016, 12, 19–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satija, A.; Yu, E.; Willett, W.C.; Hu, F.B. Understanding nutritional epidemiology and its role in policy. Adv. Nutr. 2015, 6, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, E.; Yatsuya, H.; Uemura, M.; Murata, C.; Otsuka, R.; Toyoshima, H.; Tamakoshi, K.; Sasaki, S.; Kawaguchi, L.; Aoyama, A. Associations of protein, fat, and carbohydrate intakes with insomnia symptoms among middle-aged Japanese workers. Int. J. Epidemiol. 2013, 23, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Stampfer, M.J.; Rimm, E.; Ascherio, A.; Rosner, B.A.; Spiegelman, D.; Willett, W.C. Dietary fat and coronary heart disease: A comparison of approaches for adjusting for total energy intake and modeling repeated dietary measurements. Am. J. Epidemiol. 1999, 149, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.F.; Chittleborough, C.R.; Taylor, A.W.; Dal Grande, E.; Wilson, D.H.; Phillips, P.J.; Adams, R.J.; Cheek, J.; Price, K.; Gill, T.; et al. The North West Adelaide Health Study: Detailed methods and baseline segmentation of a cohort for selected chronic diseases. Epidemiol. Perspect. Innov. 2006, 3, 4. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.F.; Taylor, A.W.; Ruffin, R.E.; Wilson, D.H.; Phillips, P.J.; Adams, R.J.; Price, K. Cohort Profile: The North West Adelaide Health Study (NWAHS). Int. J. Epidemiol. 2009, 38, 1479–1486. [Google Scholar] [CrossRef] [PubMed]
- Hodge, A.; Patterson, A.J.; Brown, W.J.; Ireland, P.; Giles, G. The Anti Cancer Council of Victoria FFQ: Relative validity of nutrient intakes compared with weighed food records in young to middle-aged women in a study of iron supplementation. Aust. N. Z. J. Public Health 2000, 24, 576–583. [Google Scholar] [CrossRef]
- Hebden, L.; Kostan, E.; O’Leary, F.; Hodge, A.; Allman-Farinelli, M. Validity and reproducibility of a food frequency questionnaire as a measure of recent dietary intake in young adults. PLoS ONE 2013, 8, e75156. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef]
- Johns, M.; Hocking, B. Daytime sleepiness and sleep habits of Australian workers. Sleep 1997, 20, 844–849. [Google Scholar] [CrossRef]
- Johns, M.W. Reliability and factor analysis of the Epworth Sleepiness Scale. Sleep 1992, 15, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Lapin, B.R.; Bena, J.F.; Walia, H.K.; Moul, D.E. The Epworth Sleepiness Scale: Validation of One-Dimensional Factor Structure in a Large Clinical Sample. J. Clin. Sleep Med. 2018, 14, 1293–1301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Bureau of Statistics. Information Paper: An Introduction to Socio-Economic Indexes for Areas (SEIFA); Australian Bureau of Statistics: Canberra, Australia, 2006. Available online: http://www.abs.gov.au/ausstats/[email protected]/mf/2039.0/ (accessed on 5 April 2019).
- National Heart Foundation, Australian Institute of Health and Welfare. Risk Factor Prevalence Study: SURVEY No 3; NHF: Canberra, Australia, 1989.
- Australian Institute of Health and Welfare. The Active Australia Survey: A Guide and Manual for Implementation, Analysis and Reporting; Australian Institute of Health and Welfare: Canberra, Australia, 2003.
- Myint, P.K.; Kwok, C.S.; Luben, R.N.; Wareham, N.J.; Khaw, K.T. Body fat percentage, body mass index and waist-to-hip ratio as predictors of mortality and cardiovascular disease. Heart 2014, 100, 1613–1619. [Google Scholar] [CrossRef] [PubMed]
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Retrieved from the University of Minnesota Digital Conservancy. 1977. Available online: http://hdl.handle.net/11299/98561 (accessed on 22 June 2019).
- Ricci, C.; Baumgartner, J.; Zec, M.; Kruger, H.S.; Smuts, C.M. Type of dietary fat intakes in relation to all-cause and cause-specific mortality in US adults: An iso-energetic substitution analysis from the American National Health and Nutrition Examination Survey linked to the US mortality registry. Br. J. Nutr. 2018, 119, 456–463. [Google Scholar] [CrossRef]
- Oh, K.; Hu, F.B.; Manson, J.E.; Stampfer, M.J.; Willett, W.C. Dietary fat intake and risk of coronary heart disease in women: 20 years of follow-up of the nurses’ health study. Am. J. Epidemiol. 2005, 161, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Campmans-Kuijpers, M.J.; Sluijs, I.; Nothlings, U.; Freisling, H.; Overvad, K.; Weiderpass, E.; Fagherazzi, G.; Kühn, T.; Katzke, V.A.; Mattiello, A.; et al. Isocaloric substitution of carbohydrates with protein: The association with weight change and mortality among patients with type 2 diabetes. Cardiovasc. Diabetol. 2015, 14, 39. [Google Scholar] [CrossRef]
- Bernstein, A.M.; Sun, Q.; Hu, F.B.; Stampfer, M.J.; Manson, J.E.; Willett, W.C. Major dietary protein sources and risk of coronary heart disease in women. Circulation 2010, 122, 876–883. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Katagiri, R.; Asakura, K.; Kobayashi, S.; Suga, H.; Sasaki, S. Low intake of vegetables, high intake of confectionary, and unhealthy eating habits are associated with poor sleep quality among middle-aged female Japanese workers. Int. J. Occup. Med. Environ. Health 2014, 56, 359–368. [Google Scholar] [CrossRef]
- Tan, X.; Alen, M.; Cheng, S.M.; Mikkola, T.M.; Tenhunen, J.; Lyytikainen, A.; Wiklund, P.; Cong, F.; Saarinen, A.; Tarkka, I.; et al. Associations of disordered sleep with body fat distribution, physical activity and diet among overweight middle-aged men. J. Sleep Res. 2015, 24, 414–424. [Google Scholar] [CrossRef]
- Afaghi, A.; O’Connor, H.; Chow, C.M. High-glycemic-index carbohydrate meals shorten sleep onset. Am. J. Clin. Nutr. 2007, 85, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Lindseth, G.; Lindseth, P.; Thompson, M. Nutritional effects on sleep. West. J. Nurs. Res. 2013, 35, 497–513. [Google Scholar] [CrossRef] [PubMed]
- Kohsaka, A.; Laposky, A.D.; Ramsey, K.M.; Estrada, C.; Joshu, C.; Kobayashi, Y.; Turek, F.W.; Bass, J. High-fat diet disrupts behavioral and molecular circadian rhythms in mice. Cell Metab. 2007, 6, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Wells, A.S.; Read, N.W.; Craig, A. Influences of dietary and intraduodenal lipid on alertness, mood, and sustained concentration. Br. J. Nutr. 1995, 74, 115–123. [Google Scholar] [CrossRef] [Green Version]
- Lyons, P.M.; Truswell, A.S. Serotonin precursor influenced by type of carbohydrate meal in healthy adults. Am. J. Clin. Nutr. 1988, 47, 433–439. [Google Scholar] [CrossRef]
- Afaghi, A.; O’Connor, H.; Chow, C.M. Acute effects of the very low carbohydrate diet on sleep indices. Nutr. Neurosci. 2008, 11, 146–154. [Google Scholar] [CrossRef]
- Kapas, L.; Obal, F., Jr.; Alfoldi, P.; Rubicsek, G.; Penke, B.; Obal, F. Effects of nocturnal intraperitoneal administration of cholecystokinin in rats: Simultaneous increase in sleep, increase in EEG slow-wave activity, reduction of motor activity, suppression of eating, and decrease in brain temperature. Brain Res. 1988, 438, 155–164. [Google Scholar] [CrossRef]
- Crispim, C.A.; Zimberg, I.Z.; dos Reis, B.G.; Diniz, R.M.; Tufik, S.; de Mello, M.T. Relationship between food intake and sleep pattern in healthy individuals. J. Clin. Sleep Med. 2011, 7, 659–664. [Google Scholar] [CrossRef]
- Yajima, K.; Seya, T.; Iwayama, K.; Hibi, M.; Hari, S.; Nakashima, Y.; Ogata, H.; Omi, N.; Satoh, M.; Tokuyama, K. Effects of nutrient composition of dinner on sleep architecture and energy metabolism during sleep. J. Nutr. Sci. Vitaminol. 2014, 60, 114–121. [Google Scholar] [CrossRef]
- Phillips, F.; Chen, C.N.; Crisp, A.H.; Koval, J.; McGuinness, B.; Kalucy, R.S.; Lacey, J. Isocaloric diet changes and electroencephalographic sleep. Lancet 1975, 2, 723–725. [Google Scholar] [CrossRef]
- Hayley, A.C.; Williams, L.J.; Kennedy, G.A.; Berk, M.; Brennan, S.L.; Pasco, J.A. Excessive daytime sleepiness and body composition: A population-based study of adults. PLoS ONE 2014, 9, e112238. [Google Scholar] [CrossRef] [PubMed]
- Sweatt, S.K.; Gower, B.A.; Chieh, A.Y.; Liu, Y.; Li, L. Sleep quality is differentially related to adiposity in adults. Psychoneuroendocrinology 2018, 98, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Shochat, T.; Shefer-Hilel, G.; Zisberg, A. Relationships between body mass index and sleep quality and duration in adults 70 years and older. Sleep Health 2016, 2, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.N.; Zoumakis, E.; Lin, H.M.; Bixler, E.O.; Trakada, G.; Chrousos, G.P. Marked decrease in sleepiness in patients with sleep apnea by etanercept, a tumor necrosis factor-alpha antagonist. J. Clin. Endocrinol. Metab. 2004, 89, 4409–4413. [Google Scholar] [CrossRef] [PubMed]
- Blackburn, P.; Despres, J.P.; Lamarche, B.; Tremblay, A.; Bergeron, J.; Lemieux, I.; Couillard, C. Postprandial variations of plasma inflammatory markers in abdominally obese men. Obesity 2006, 14, 1747–1754. [Google Scholar] [CrossRef]
- Vgontzas, A.N.; Papanicolaou, D.A.; Bixler, E.O.; Hopper, K.; Lotsikas, A.; Lin, H.M.; Kales, A.; Chrousos, G.P. Sleep apnea and daytime sleepiness and fatigue: Relation to visceral obesity, insulin resistance, and hypercytokinemia. J. Clin. Endocrinol. Metab. 2000, 85, 1151–1158. [Google Scholar] [CrossRef]
- Stanaway, J.D.; Afshin, A.; Gakidou, E.; Lim, S.S.; Abate, D.; Abate, K.H.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar]
- Hooper, L.; Martin, N.; Abdelhamid, A.; Davey Smith, G. Reduction in saturated fat intake for cardiovascular disease. Cochrane Database Syst. Rev. 2015, 6, Cd011737. [Google Scholar] [CrossRef]
- Liu, S. Intake of refined carbohydrates and whole grain foods in relation to risk of type 2 diabetes mellitus and coronary heart disease. J. Am. Coll. Nutr. 2002, 21, 298–306. [Google Scholar] [CrossRef]
- Sanchez-Villegas, A.; Verberne, L.; De Irala, J.; Ruiz-Canela, M.; Toledo, E.; Serra-Majem, L.; Martínez-González, M. Dietary fat intake and the risk of depression: The SUN Project. PLoS ONE 2011, 6, e16268. [Google Scholar] [CrossRef]
- Vernet, C.; Redolfi, S.; Attali, V.; Konofal, E.; Brion, A.; Frija-Orvoen, E.; Pottier, M.; Similowski, T.; Arnulf, I. Residual sleepiness in obstructive sleep apnoea: Phenotype and related symptoms. Eur. Respir. J. 2011, 38, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Antic, N.A.; Catcheside, P.; Buchan, C.; Hensley, M.; Naughton, M.T.; Rowland, S.; Williamson, B.; Windler, S.; McEvoy, R.D. The effect of CPAP in normalizing daytime sleepiness, quality of life, and neurocognitive function in patients with moderate to severe OSA. Sleep 2011, 34, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Willett, W. Nutritional Epidemiology; OUP: New York, NY, USA, 2013. [Google Scholar]
- Crosby, P.; Hamnett, R.; Putker, M.; Hoyle, N.P.; Reed, M.; Karam, C.J.; Maywood, E.S.; Stangherlin, A.; Chesham, J.E.; Hayter, E.A.; et al. Insulin/IGF-1 Drives PERIOD Synthesis to Entrain Circadian Rhythms with Feeding Time. Cell 2019, 177, 896–909. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Category | N (%) |
|---|---|---|
| Sex | Male | 930 (46.6%) |
| Age (years) # | 56.3 (13.9) | |
| Marital status | Married or living with partner | 1332 (66.7%) |
| Separated/divorced | 256 (12.8%) | |
| Widowed | 164 (8.2%) | |
| Never married | 164 (8.2%) | |
| Missing | 81 (4.1%) | |
| Educational status | Did not complete school/high school level | 961 (48.1%) |
| Trade/certificate/diploma | 614 (30.7%) | |
| Degree or higher | 345 (17.3%) | |
| Missing | 77 (3.9%) | |
| Work status | Employed | 1103 (55.2%) |
| Unemployed | 29 (1.5%) | |
| Retired | 605 (30.3%) | |
| Other | 182 (9.1%) | |
| Missing | 78 (3.9%) | |
| SEIFA | Lowest quintile | 498 (24.9%) |
| Low quintile | 491 (24.6%) | |
| Middle quintile | 432 (21.6%) | |
| High quintile | 426 (21.3%) | |
| Highest quintile | 133 (6.7%) | |
| Missing | 17 (0.9%) | |
| Alcohol risk | Nondrinkers, no risk | 987 (49.4%) |
| Low risk | 744 (37.3%) | |
| Intermediate to very high risk | 94 (4.7%) | |
| Missing | 172 (8.6%) | |
| Physical activity level | No activity | 355 (17.8%) |
| Activity but not sufficient | 819 (41.0%) | |
| Sufficient activity | 740 (37.1%) | |
| Missing | 83 (4.2%) | |
| Smoking status | Non-smoker | 926 (46.4%) |
| Ex-smoker | 774 (38.8%) | |
| Current smoker | 287 (14.4%) | |
| Missing | 10 (0.5%) | |
| Sleeping duration (hours per day) # | 7.2 (1.2) | |
| Waist-to-hip ratio # | 0.89 (0.09) | |
| Pulse pressure (mmHg) # | 50.6 (14.3) | |
| Diabetes | Yes | 191 (9.6%) |
| Depression | Yes | 338 (16.9%) |
| Missing | 32 (1.6%) | |
| Sleep apnea | Yes | 119 (6.0%) |
| Missing | 26 (1.3%) | |
| Total energy in kcal # (fat, carbohydrate, and protein) | 1984.5 (591.4) | |
| Energy from unsaturated fat # (%) | 26.6 (5.4) | |
| Energy from saturated fat # (%) | 12.8 (2.7) | |
| Energy from carbohydrate # (%) | 41.3 (7.0) | |
| Energy from protein # (%) | 19.3 (3.3) | |
| Excessive daytime sleepiness | 211 (10.6%) |
| Model | Odds Ratio (95% CI) | ||||
|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | p Trend | |
| Total fat | |||||
| Model 1 | 1.00 | 1.32 (0.78–2.25) | 1.39 (0.78–2.49) | 1.72 (0.86–3.45) | 0.147 |
| Model 2 | 1.00 | 1.21 (0.69–2.12) | 1.11 (0.60–2.05) | 1.06 (0.49–2.28) | 0.975 |
| Saturated fat | |||||
| Model 1 | 1.00 | 1.37 (0.80–2.36) | 1.75 (0.99–3.10) | 2.33 (1.20–4.52) | 0.011 |
| Model 2 | 1.00 | 1.26 (0.71–2.23) | 1.52 (0.82–2.81) | 1.77 (0.87–3.64) | 0.106 |
| Unsaturated fat | |||||
| Model 1 | 1.00 | 1.07 (0.64–1.78) | 1.04 (0.60–1.81) | 1.47 (0.80–2.73) | 0.247 |
| Model 2 | 1.00 | 0.92 (0.53–1.58) | 0.86 (0.48–1.54) | 0.97 (0.49–1.92) | 0.899 |
| Carbohydrate | |||||
| Model 1 | 1.00 | 1.30 (0.77–2.20) | 1.17 (0.65–2.11) | 1.24 (0.57–2.66) | 0.695 |
| Model 2 | 1.00 | 1.33 (0.76–2.32) | 1.23 (0.65–2.32) | 1.42 (0.62–3.25) | 0.507 |
| Protein | |||||
| Model 1 | 1.00 | 1.32 (0.80–2.19) | 1.01 (0.57–1.78) | 1.06 (0.54–2.09) | 0.870 |
| Model 2 | 1.00 | 1.47 (0.86–2.53) | 1.04 (0.56–1.91) | 1.03 (0.48–2.19) | 0.761 |
| Model | Odds Ratio (95% CI) | |||
|---|---|---|---|---|
| Saturated Fat | Unsaturated Fat | Protein | Carbohydrate | |
| Substituting protein | ||||
| Partition model | ||||
| Absolute intake (10 g) | ||||
| Model 1 | 1.40 (1.08–1.81) | 1.11 (0.94–1.31) | 1.07 (0.96–1.19) | |
| Model 2 | 1.34 (1.00–1.78) | 1.06 (0.88–1.27) | 1.07 (0.96–1.19) | |
| Energy intake (100 kcal) | ||||
| Model 1 | 1.57 (1.07–2.30) | 1.22 (0.91–1.63) | 1.17 (0.92–1.50) | |
| Model 2 | 1.49 (0.98–2.26) | 1.14 (0.83–1.58) | 1.18 (0.90–1.53) | |
| Standard regression model (10 g) | ||||
| Model 1 | 1.50 (1.07–2.12) | 1.20 (0.92–1.55) | 1.07 (0.97–1.18) | |
| Model 2 | 1.43 (0.98–2.08) | 1.13 (0.85–1.50) | 1.07 (0.96–1.18) | |
| Nutrient density model (5% energy) | ||||
| Model 1 | 1.74 (1.16– 2.63) | 1.26 (0.92– 1.71) | 1.24 (0.94–1.62) | |
| Model 2 | 1.57 (1.00–2.45) | 1.16 (0.83–1.62) | 1.23 (0.92–1.65) | |
| Substituting carbohydrate | ||||
| Partition model | ||||
| Absolute intake (10 g) | ||||
| Model 1 | 1.31 (1.06–1.63) | 1.04 (0.93–1.17) | 0.94 (0.85–1.03) | |
| Model 2 | 1.25 (0.98–1.60) | 0.99 (0.87–1.13) | 0.94 (0.84–1.04) | |
| Energy intake (100 kcal) | ||||
| Model 1 | 1.34 (1.04–1.72) | 1.04 (0.90–1.19) | 0.85 (0.67–1.09) | |
| Model 2 | 1.27 (0.96–1.67) | 0.97 (0.84–1.13) | 0.85 (0.65–1.11) | |
| Standard regression model (10 g) | ||||
| Model 1 | 1.30 (1.04–1.63) | 1.03(0.92–1.17) | 0.94(0.85–1.03) | |
| Model 2 | 1.24 (0.96–1.59) | 0.98(0.85–1.12) | 0.94(0.84–1.04) | |
| Nutrient density model (5% energy) | ||||
| Model 1 | 1.41 (1.06–1.88) | 1.01 (0.87–1.19) | 0.80 (0.62–1.06) | |
| Model 2 | 1.27 (0.93–1.75) | 0.94 (0.79–1.12) | 0.81 (0.61–1.09) | |
| Substituting saturated fat | ||||
| Partition model | ||||
| Absolute intake (10 g) | ||||
| Model 1 | 0.80 (0.61–1.04) | 0.71 (0.55–0.93) | 0.76 (0.61–0.95) | |
| Model 2 | 0.79 (0.58–1.07) | 0.75 (0.56–1.00) | 0.80 (0.63–1.02) | |
| Energy intake (100 kcal) | ||||
| Model 1 | 0.78 (0.57–1.05) | 0.64 (0.43–0.93) | 0.75 (0.58–0.96) | |
| Model 2 | 0.77 (0.55–1.08) | 0.67 (0.44–1.02) | 0.79 (0.60–1.05) | |
| Standard regression model (10 g) | ||||
| Model 1 | 0.80 (0.61–1.04) | 0.83 (0.72–0.97) | 0.89 (0.80–0.98) | |
| Model 2 | 0.79 (0.58–1.07) | 0.85 (0.72–1.01) | 0.91 (0.81–1.02) | |
| Nutrient density model (5% energy) | ||||
| Model 1 | 0.72 (0.52–1.01) | 0.57 (0.38–0.86) | 0.71 (0.53–0.94) | |
| Model 2 | 0.74 (0.51–1.06) | 0.63 (0.41–0.99) | 0.79 (0.57–1.08) | |
| Substituting unsaturated fat | ||||
| Partition model | ||||
| Absolute intake (10 g) | ||||
| Model 1 | 1.26 (0.96–1.65) | 0.90 (0.76–1.06) | 0.96 (0.86–1.07) | |
| Model 2 | 1.27 (0.93–1.71) | 0.95 (0.79–1.14) | 1.01 (0.89–1.15) | |
| Energy intake (100 kcal) | ||||
| Model 1 | 1.29 (0.95–1.74) | 0.82 (0.61–1.10) | 0.96 (0.84–1.10) | |
| Model 2 | 1.30 (0.93–1.82) | 0.87 (0.64–1.20) | 1.03 (0.88–1.20) | |
| Standard regression model (10 g) | ||||
| Model 1 | 1.26 (0.96–1.65) | 0.92 (0.82–1.04) | 0.98 (0.93–1.04) | |
| Model 2 | 1.27 (0.93–1.71) | 0.95 (0.83–1.08) | 1.01 (0.95–1.07) | |
| Nutrient density model (5% energy) | ||||
| Model 1 | 1.38 (0.99–1.93) | 0.79 (0.58–1.08) | 0.98 (0.84–1.15) | |
| Model 2 | 1.36 (0.94–1.95) | 0.86 (0.62–1.21) | 1.06 (0.90–1.26) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melaku, Y.A.; Reynolds, A.C.; Gill, T.K.; Appleton, S.; Adams, R. Association between Macronutrient Intake and Excessive Daytime Sleepiness: An Iso-Caloric Substitution Analysis from the North West Adelaide Health Study. Nutrients 2019, 11, 2374. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102374
Melaku YA, Reynolds AC, Gill TK, Appleton S, Adams R. Association between Macronutrient Intake and Excessive Daytime Sleepiness: An Iso-Caloric Substitution Analysis from the North West Adelaide Health Study. Nutrients. 2019; 11(10):2374. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102374
Chicago/Turabian StyleMelaku, Yohannes Adama, Amy C. Reynolds, Tiffany K. Gill, Sarah Appleton, and Robert Adams. 2019. "Association between Macronutrient Intake and Excessive Daytime Sleepiness: An Iso-Caloric Substitution Analysis from the North West Adelaide Health Study" Nutrients 11, no. 10: 2374. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102374