Relation of Fruits and Vegetables with Major Cardiometabolic Risk Factors, Markers of Oxidation, and Inflammation


Abstract
:1. Introduction
2. Dietary Polyphenol and Carotenoid Intake
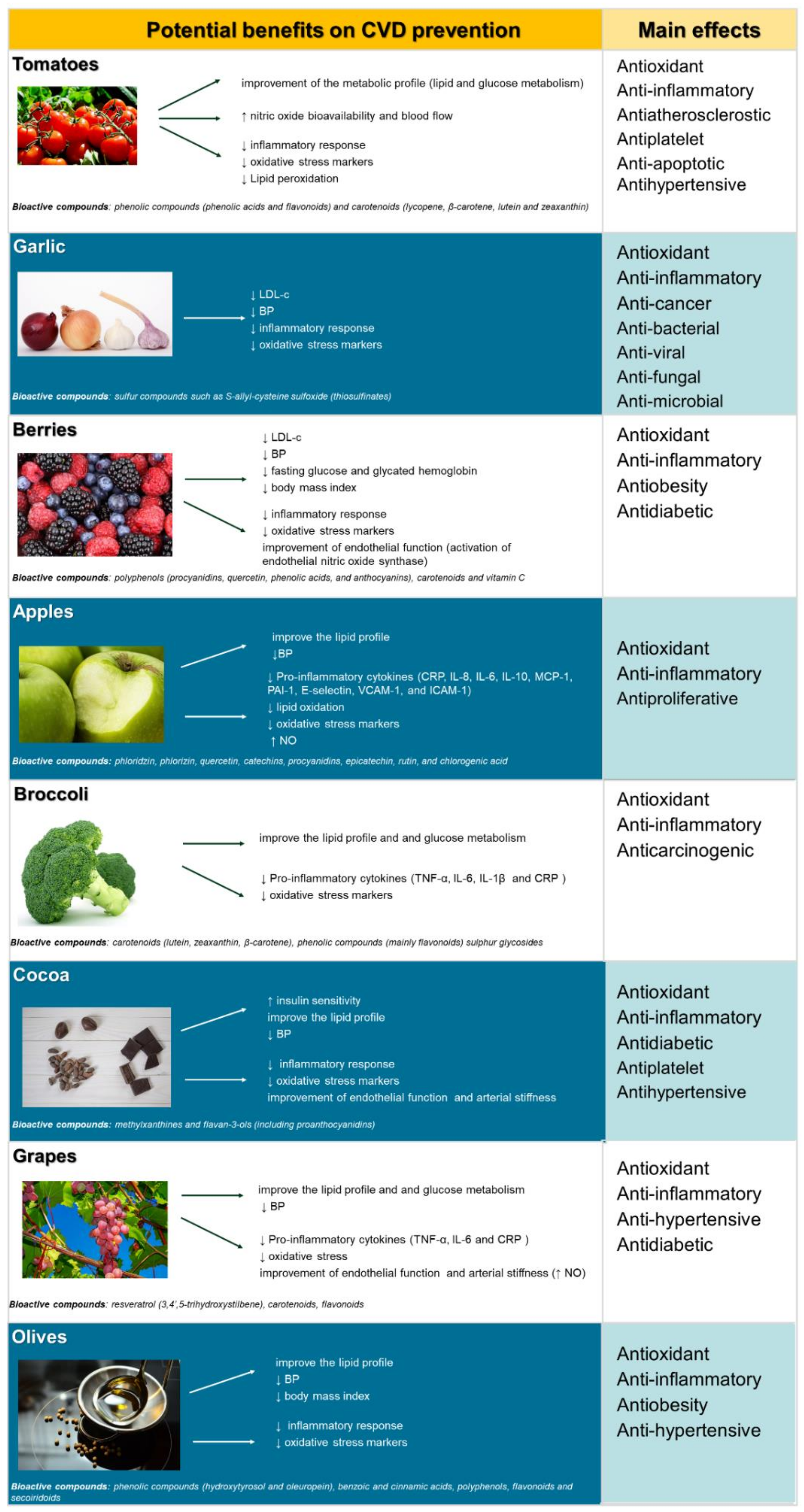
3. Health Potential of Selected Fruits and Vegetables
3.1. Tomatoes
3.2. Garlic
3.3. Berries
3.4. Apples
3.5. Broccoli
3.6. Cocoa
3.7. Grapes
3.8. Olives
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report from the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- WHO Cardiovascular Diseases (CVDs). Available online: http://www.who.int/cardiovascular_diseases/ (accessed on 24 July 2019).
- Frostegård, J. Immunity, atherosclerosis and cardiovascular disease. BMC Med. 2013, 11, 117. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D. Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity—A Comprehensive Review. Circulation 2016, 33, 187–225. [Google Scholar] [CrossRef] [PubMed]
- Chatzianagnostou, K.; Del Turco, S.; Pingitore, A.; Sabatino, L.; Vassalle, C. The Mediterranean Lifestyle as a Non-Pharmacological and Natural Antioxidant for Healthy Aging. Antioxidants 2015, 4, 719–736. [Google Scholar] [CrossRef] [PubMed]
- Latifovic, L.; Peacock, S.D.; Massey, T.E.; King, W.D. The Influence of Alcohol Consumption, Cigarette Smoking, and Physical Activity on Leukocyte Telomere Length. Cancer Epidemiol. Biomarkers Prev. 2016, 25, 374–380. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Increasing Fruit and Vegetable Consumption to Reduce the Risk of Noncommunicable Diseases. Available online: https://www.who.int/elena/titles/fruit_vegetables_ncds/en/ (accessed on 24 July 2019).
- World Health Organization. Ten Threats to Global Health in 2019. Available online: https://www.who.int/emergencies/ten-threats-to-global-health-in-2019 (accessed on 24 July 2019).
- Zhou, Y.; Zheng, J.; Li, S.; Zhou, T.; Zhang, P.; Li, H.B. Alcoholic beverage consumption and chronic diseases. Int. J. Environ. Res. Public Health 2016, 13, 522. [Google Scholar] [CrossRef] [PubMed]
- Casas, R.; Ruiz-León, A.M.; Estruch, R. Circulating immune cell activation and diet: A review on human trials. J. Allergy Immunol. 2017, 1, 1–9. [Google Scholar] [CrossRef]
- Tang, G.Y.; Meng, X.; Li, Y.; Zhao, C.N.; Liu, Q.; Li, H.B. Effects of Vegetables on Cardiovascular Diseases and Related Mechanisms. Nutrients 2017, 9, 857. [Google Scholar] [CrossRef]
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality—a systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiol. 2016, 46, 1029–1056. [Google Scholar] [CrossRef]
- Crowe, F.L. Fruit and vegetable consumption is associated with reduced all-cause and cardiovascular mortality. Evid. Based. Med. 2014, 20, 14. [Google Scholar] [CrossRef]
- Hu, D.; Huang, J.; Wang, Y.; Zhang, D.; Qu, Y. Fruits and vegetables consumption and risk of stroke: A meta-analysis of prospective cohort studies. Stroke 2014, 45, 1613–1619. [Google Scholar] [CrossRef] [PubMed]
- Scicchitano, P.; Cameli, M.; Maiello, M.; Modesti, P.A.; Muiesan, M.L.; Novo, S.; Palmiero, P.; Saba, P.S.; Pedrinelli, R.; Ciccone, M.M.; et al. Nutraceuticals and dyslipidaemia: Beyond the common therapeutics. J. Funct. Foods 2014, 6, 11–32. [Google Scholar] [CrossRef]
- Bubols, G.B.; ViannaDda, R.; Medina-Remon, A.; von Poser, G.; Lamuela-Raventos, R.M.; Eifler-Lima, V.L.; Garcia, S.C. The antioxidant activity of coumarins and flavonoids. Mini Rev. Med. Chem. 2013, 13, 318–334. [Google Scholar] [CrossRef] [PubMed]
- Tsui, P.F.; Lin, C.S.; Ho, L.J.; Lai, J.H. Spices and Atherosclerosis. Nutrients 2018, 10, 1724. [Google Scholar] [CrossRef] [PubMed]
- Hoek-van den Hil, E.F.; van Schothorst, E.M.; van der Stelt, I.; Swarts, H.J.M.; van Vliet, M.; Amolo, T.; Vervoort, J.J.M.; Venema, D.; Hollman, P.C.H.; Rietjens, I.M.; et al. Direct comparison of metabolic health effects of the flavonoids quercetin, hesperetin, epicatechin, apigenin and anthocyanins in high-fat-diet-fed mice. Genes Nutr. 2015, 10, 469. [Google Scholar] [CrossRef] [PubMed]
- Berman, A.Y.; Motechin, R.A.; Wiesenfeld, M.Y.; Holz, M.K. The therapeutic potential of resveratrol: A review of clinical trials. NPJ Precis. Oncol. 2017, 1, 35. [Google Scholar] [CrossRef] [PubMed]
- Castro-Barquero, S.; Lamuela-Raventós, R.M.; Doménech, M.; Estruch, R. Relationship between Mediterranean Dietary Polyphenol Intake and Obesity. Nutrients 2018, 10, 1523. [Google Scholar] [CrossRef] [PubMed]
- Zamora-Ros, R.; Knaze, V.; Rothwell, J.A.; Hémon, B.; Moskal, A.; Overvad, K.; Tjønneland, A.; Kyrø, C.; Fagherazzi, G.; Boutron-Ruault, M.C.; et al. Dietary polyphenol intake in Europe: The European Prospective Investigation into Cancer and Nutrition (EPIC) study. Eur. J. Nutr. 2016, 55, 1359–1375. [Google Scholar] [CrossRef]
- Kim, J.H.; Lee, J.; Choi, I.J.; Kim, Y.I.; Kwon, O.; Kim, H.; Kim, J. Dietary Carotenoids Intake and the Risk of Gastric Cancer: A Case-Control Study in Korea. Nutrients 2018, 10, 1031. [Google Scholar] [CrossRef]
- Wallace, T.C.; Giusti, M.M. Anthocyanins. Adv. Nutr. 2015, 6, 620–622. [Google Scholar] [CrossRef]
- Vogiatzoglou, A.; Mulligan, A.A.; Luben, R.N.; Lentjes, M.A.; Heiss, C.; Kelm, M.; Merx, M.W.; Spencer, J.P.; Schroeter, H.; Kuhnle, G.G. Assessment of the dietary intake of total flavan-3-ols, monomeric flavan-3-ols, proanthocyanidins and theaflavins in the European Union. Br. J. Nutr. 2014, 111, 1463–1473. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chung, S.J.; Song, W.O.; Chun, O.K. Estimation of daily proanthocyanidin intake and major food sources in the U. S. diet. J. Nutr. 2011, 141, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Vang, O.; Ahmad, N.; Baile, C.A.; Baur, J.A.; Brown, K.; Csiszar, A.; Das, D.K.; Delmas, D.; Gottfried, C.; Lin, H.Y.; et al. What is new for an old molecule? Systematic review and recommendations on the use of resveratrol. PLoS ONE 2011, 6, e19881. [Google Scholar] [CrossRef] [PubMed]
- Martínez, L.; Ros, G.; Nieto, G. Hydroxytyrosol: Health Benefits and Use as Functional Ingredient in Meat. Medicines 2018, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Burrows, T.L.; Williams, R.; Rollo, M.; Wood, L.; Garg, M.L.; Jensen, M.; Collins, C.E. Plasma carotenoid levels as biomarkers of dietary carotenoid consumption: A systematic review of the validation studies. J. Nutr. Intermed. Metab. 2015, 2, 15–64. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.S. Allicin and other functional active components in garlic: Health benefits and bioavailability. Int. J. Food Prop. 2007, 10, 245–268. [Google Scholar] [CrossRef]
- Sones, K.; Heaney, R.K.; Fenwick, G.R. An estimate of the mean daily intake of glucosinolates from cruciferous vegetables in the UK. J. Sci. Food Agric. 1984, 35, 712–720. [Google Scholar] [CrossRef]
- Gebhardt, C. The historical role of species from the Solanaceae plant family in genetic research. Theor. Appl. Genet. 2016, 129, 2281–2294. [Google Scholar] [CrossRef] [Green Version]
- Raiola, A.; Rigano, M.M.; Calafiore, R.; Frusciante, L.; Barone, A. Enhancing the health-promoting effects of tomato fruit for biofortified food. Mediat. Inflamm. 2014, 2014, 139873. [Google Scholar] [CrossRef]
- Salehi, B.; Sharifi-Rad, R.; Sharopov, F.; Namiesnik, J.; Roointan, A.; Kamle, M.; Kumar, P.; Martins, N.; Sharifi-Rad, J. Beneficial effects and potential risks of tomato consumption for human health: An overview. Nutrition 2019, 62, 201–208. [Google Scholar] [CrossRef]
- Nasir, M.U.; Hussain, S.; Jabbar, S. Tomato processing, lycopene and health benefits: A review. Sci. Lett. 2015, 3, 1–5. [Google Scholar]
- Martí, R.; Roselló, S.; Cebolla-Cornejo, J. Tomato as a Source of Carotenoids and Polyphenols Targeted to Cancer Prevention. Cancers 2016, 8, 58. [Google Scholar] [CrossRef] [PubMed]
- Kotíková, Z.; Lachman, J.; Hejtmánková, A.; Hejtmánková, K. Determination of antioxidant activity and antioxidant content in tomato varieties and evaluation of mutual interactions between antioxidants. LWT Food Sci. Technol. 2011, 44, 1703–1710. [Google Scholar] [CrossRef]
- Reimers, K.; Andon, M.; Jacobson, M.; Nguyen, V.; Cooper, L.; Rippe, J. Increasing tomato intake to MyPlate recommended amount: Effect on serum lycopene. FASEB J. 2013, 27, 624–628. [Google Scholar]
- Torres, N.; Guevara-Cruz, M.; Velázquez-Villegas, L.A.; Tovar, A.R. Nutrition and Atherosclerosis. Arch. Med. Res. 2015, 46, 408–426. [Google Scholar] [CrossRef] [PubMed]
- Pennathur, S.; Maitra, D.; Byun, J.; Sliskovic, I.; Abdulhamid, I.; Saed, G.M.; Diamond, M.P.; Abu-Soud, H.M. Potent antioxidative activity of lycopene: A potential role in scavenging hypochlorous acid. Free Radic. Biol. Med. 2010, 49, 205–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khachik, F.; Carvalho, L.; Bernstein, P.S.; Muir, G.J.; Zhao, D.Y.; Katz, N.B. Chemistry, distribution, and metabolism of tomato carotenoids and their impact on human health. Exp. Biol. Med. 2002, 227, 845–851. [Google Scholar] [CrossRef]
- Mordente, A.; Guantario, B.; Meucci, E.; Silvestrini, A.; Lombardi, E.; Martorana, G.E.; Giardina, B.; Böhm, V. Lycopene and cardiovascular diseases: An update. Curr. Med. Chem. 2011, 18, 1146–1163. [Google Scholar] [CrossRef]
- Song, B.; Liu, K.; Gao, Y.; Zhao, L.; Fang, H.; Li, Y.; Pei, L.; Xu, Y. Lycopene and risk of cardiovascular diseases: A meta-analysis of observational studies. Mol. Nutr. Food Res. 2017, 61, 1601009. [Google Scholar] [CrossRef]
- Cheng, H.M.; Koutsidis, G.; Lodge, J.K.; Ashor, A.W.; Siervo, M.; Lara, J. Lycopene and tomato and risk of cardiovascular diseases: A systematic review and meta-analysis of epidemiological evidence. Crit. Rev. Food Sci. Nutr. 2019, 59, 141–158. [Google Scholar] [CrossRef]
- Li, X.; Xu, J. Dietary and circulating lycopene and stroke risk: A meta-analysis of prospective studies. Sci. Rep. 2014, 4, 5031. [Google Scholar] [CrossRef]
- Li, X.; Xu, J. Lycopene supplement and blood pressure: An updated meta-analysis of intervention trials. Nutrients 2013, 5, 3696–3712. [Google Scholar] [CrossRef] [PubMed]
- Mozos, I.; Stoian, D.; Caraba, A.; Malainer, C.; Horbańczuk, J.O.; Atanasov, A.G. Lycopene and Vascular Health. Front. Pharmacol. 2018, 9, 521. [Google Scholar] [CrossRef] [PubMed]
- Hidekatsu, Y. The anti-atherosclerotic effects of tomatoes. Funct. Foods Health Dis. 2017, 7, 411–428. [Google Scholar] [CrossRef]
- Montesano, D.; Blasi, F.; Cossignani, L. Lycopene and Cardiovascular Disease: An Overview. Ann. Short Rep. 2019, 2, 1033. [Google Scholar]
- Cheng, H.M.; Koutsidis, G.; Lodge, J.K.; Ashor, A.; Siervo, M.; Lara, J. Tomato and lycopene supplementation and cardiovascular risk factors: A systematic review and meta-analysis. Atherosclerosis 2017, 257, 100–108. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.F.; Chang, Y.Y.; Huang, H.C.; Wu, Y.C.; Yang, M.D.; Chao, P.M. Tomato juice supplementation in young women reduces inflammatory adipokine levels independently of body fat reduction. Nutrition 2015, 31, 691–696. [Google Scholar] [CrossRef]
- García-Alonso, F.J.; Jorge-Vidal, V.; Ros, G.; Periago, M.J. Effect of consumption of tomato juice enriched with n-3 polyunsaturated fatty acids on the lipid profile, antioxidant biomarker status, and cardiovascular disease risk in healthy women. Eur. J. Nutr. 2012, 51, 415–424. [Google Scholar] [CrossRef]
- De Roos, B.; Mavrommatis, Y.; Brouwer, I.A. Long-chain n-3 polyunsaturated fatty acids: New insights into mechanisms relating to inflammation and coronary heart disease. Br. J. Pharmacol. 2009, 158, 413–428. [Google Scholar] [CrossRef]
- Valderas-Martinez, P.; Chiva-Blanch, G.; Casas, R.; Arranz, S.; Martínez-Huélamo, M.; Urpi-Sarda, M.; Torrado, X.; Corella, D.; Lamuela-Raventós, R.M.; Estruch, R. Tomato Sauce Enriched with Olive Oil Exerts Greater Effects on Cardiovascular Disease Risk Factors than Raw Tomato and Tomato Sauce: A Randomized Trial. Nutrients 2016, 8, 170. [Google Scholar] [CrossRef]
- Thies, F.; Masson, L.F.; Rudd, A.; Vaughan, N.; Tsang, C.; Brittenden, J.; Simpson, W.G.; Duthie, S.; Horgan, G.W.; Duthie, G. Effect of a tomato-rich diet on markers of cardiovascular disease risk in moderately overweight, disease-free, middle-aged adults: A randomized controlled trial. Am. J. Clin. Nutr. 2012, 95, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Burton-Freeman, B.; Talbot, J.; Park, E.; Krishnankutty, S.; Edirisinghe, I. Protective activity of processed tomato products on postprandial oxidation and inflammation: A clinical trial in healthy weight men and women. Mol. Nutr. Food Res. 2012, 56, 622–631. [Google Scholar] [CrossRef] [PubMed]
- Deplanque, X.; Muscente-Paque, D.; Chappuis, E. Proprietary tomato extract improves metabolic response to high-fat meal in healthy normal weight subjects. Food Nutr. Res. 2016, 60, 32537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghavipour, M.; Sotoudeh, G.; Ghorbani, M. Tomato juice consumption improves blood antioxidative biomarkers in overweight and obese females. Clin. Nutr. 2015, 34, 805–809. [Google Scholar] [CrossRef] [PubMed]
- Pourahmadi, Z.; Mahboob, S.; Saedisomeolia, A.; Reykandeh, M.T. The Effect of Tomato Juice Consumption on Antioxidant Status in Overweight and Obese Females. Women Health 2015, 55, 795–804. [Google Scholar] [CrossRef] [PubMed]
- O’Kennedy, N.; Crosbie, L.; Song, H.J.; Zhang, X.; Horgan, G.; Duttaroy, A.K. A randomised controlled trial comparing a dietary antiplatelet, the water-soluble tomato extract Fruitflow, with 75 mg aspirin in healthy subjects. Eur. J. Clin. Nutr. 2017, 71, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Krasinska, B.; Osińska, A.; Osinski, M.; Krasinska, A.; Rzymski, P.; Tykarski, A.; Krasiński, Z. Standardised tomato extract as an alternative to acetylsalicylic acid in patients with primary hypertension and high cardiovascular risk—A randomised, controlled trial. Arch. Med. Sci. 2018, 14, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, S.A.; Bowen, K.; Garg, M.L. Tomato juice and platelet aggregation in type 2 diabetes. JAMA 2004, 292, 805–806. [Google Scholar] [CrossRef]
- Xaplanteris, P.; Vlachopoulos, C.; Pietri, P.; Terentes-Printzios, D.; Kardara, D.; Alexopoulos, N.; Aznaouridis, K.; Miliou, A.; Stefanadis, C. Tomato paste supplementation improves endothelial dynamics and reduces plasma total oxidative status in healthy subjects. Nutr. Res. 2012, 32, 390–394. [Google Scholar] [CrossRef]
- Stangl, V.; Kuhn, C.; Hentschel, S.; Jochmann, N.; Jacob, C.; Böhm, V.; Fröhlich, K.; Müller, L.; Gericke, C.; Lorenz, M. Lack of effects of tomato products on endothelial function in human subjects: Results of a randomised, placebo-controlled cross-over study. Br. J. Nutr. 2011, 105, 263–267. [Google Scholar] [CrossRef]
- Dalbeni, A.; Treggiari, D.; Tagetti, A.; Bevilaqua, M.; Bonafini, S.; Montagnana, M.; Scaturro, G.; Minuz, P.; Fava, C. Positive Effects of Tomato Paste on Vascular Function After a Fat Meal in Male Healthy Subjects. Nutrients 2018, 10, 1310. [Google Scholar] [CrossRef] [PubMed]
- Thies, F.; Mills, L.M.; Moir, S.; Masson, L.F. Cardiovascular benefits of lycopene: Fantasy or reality? Proc. Nutr. Soc. 2017, 76, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Block, E. Garlic and Other Alliums. The Lore and the Science; Royal Society of Chemistry: Albany, NY, USA, 2010; p. 7162. [Google Scholar]
- Zeng, T.; Zhang, C.L.; Zhao, X.L.; Xie, K.Q. The roles of garlic on the lipid parameters: A systematic review of the literature. Crit. Rev. Food Sci. Nutr. 2013, 53, 215–230. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Casado, A. The Health Potential of Fruits and Vegetables Phytochemicals: Notable Examples. Crit. Rev. Food Sci. Nutr. 2016, 56, 1097–1107. [Google Scholar] [CrossRef] [PubMed]
- Qidwai, W.; Ashfa, T. Role of garlic usage in cardiovascular disease prevention: An evidence-based approach. Evid. Based Complement Alternat. Med. 2013, 2013, 125649. [Google Scholar] [CrossRef] [PubMed]
- Ried, K.; Travica, N.; Sali, A. The Effect of Kyolic Aged Garlic Extract on Gut Microbiota, Inflammation, and Cardiovascular Markers in Hypertensives: The GarGIC Trial. Front. Nutr. 2018, 5, 122. [Google Scholar] [CrossRef]
- Bayan, L.; Koulivand, P.H.; Gorji, A. Garlic: A review of potential therapeutic effects. Avicenna J. Phytomed. 2014, 4, 1–14. [Google Scholar] [PubMed]
- Sohn, D.W.; Han, C.H.; Jung, Y.S.; Kim, S.I.; Kim, S.W.; Cho, Y.H. Anti-inflammatory and antimicrobial effects of garlic and synergistic effect between garlic and ciprofloxacin in a chronic bacterial prostatitis rat model. Int. J. Antimicrob. Agents 2009, 34, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Varshney, R.; Budoff, M.J. Garlic and Heart Disease. J. Nutr. 2016, 146, 416S–421S. [Google Scholar] [CrossRef]
- Stabler, S.N.; Tejani, A.M.; Huynh, F.; Fowkes, C. Garlic for the prevention of cardiovascular morbidity and mortality in hypertensive patients. Cochrane Database Syst. Rev. 2012, 15, CD007653. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Anand, R.; Geng, X.; Ding, Y. A mini review: Garlic extract and vascular diseases. Neurol. Res. 2018, 40, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Antony, M.L.; Singh, S.V. Molecular mechanisms and targets of cancer chemoprevention by garlic-derived bioactive compound diallyl trisulfide. Indian J. Exp. Biol. 2011, 49, 805–816. [Google Scholar] [PubMed]
- Sun, Y.E.; Wang, W.; Qin, J. Anti-hyperlipidemia of garlic by reducing the level of total cholesterol and low-density lipoprotein: A meta-analysis. Medicine 2018, 97, e0255. [Google Scholar] [CrossRef] [PubMed]
- Zeng, T.; Guo, F.F.; Zhang, C.L.; Song, F.Y.; Zhao, X.L.; Xie, K.Q. A meta-analysis of randomized, double-blind, placebo-controlled trials for the effects of garlic on serum lipid profiles. J. Sci. Food Agric. 2012, 92, 1892–1902. [Google Scholar] [CrossRef] [PubMed]
- Shabani, E.; Sayemiri, K.; Mohammadpour, M. The effect of garlic on lipid profile and glucose parameters in diabetic patients: A systematic review and meta-analysis. Prim. Care Diabetes 2019, 13, 28–42. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, X.; Lan, H.; Wang, W. Effect of garlic supplement in the management of type 2 diabetes mellitus (T2DM): A meta-analysis of randomized controlled trials. Food Nutr. Res. 2017, 61, 1377571. [Google Scholar] [CrossRef]
- Ried, K. Garlic Lowers Blood Pressure in Hypertensive Individuals, Regulates Serum Cholesterol, and Stimulates Immunity: An Updated Meta-analysis and Review. J. Nutr. 2016, 146, 389S–396S. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.P.; Yang, J.; Qin, L.Q.; Yang, X.J. Effect of garlic on blood pressure: A meta-analysis. J. Clin. Hypertens. 2015, 17, 223–231. [Google Scholar] [CrossRef]
- Rohner, A.; Ried, K.; Sobenin, I.A.; Bucher, H.C.; Nordmann, A.J. A systematic review and metaanalysis on the effects of garlic preparations on blood pressure in individuals with hypertension. Am. J. Hypertens. 2015, 28, 414–423. [Google Scholar] [CrossRef]
- Taghizadeh, M.; Hamedifard, Z.; Jafarnejad, S. Effect of garlic supplementation on serum C-reactive protein level: A systematic review and meta-analysis of randomized controlled trials. Phytother. Res. 2019, 33, 243–252. [Google Scholar] [CrossRef]
- Darooghegi Mofrad, M.; Milajerdi, A.; Koohdani, F.; Surkan, P.J.; Azadbakht, L. Garlic Supplementation Reduces Circulating C-reactive Protein, Tumor Necrosis Factor, and Interleukin-6 in Adults: A Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Nutr. 2019, 149, 605–618. [Google Scholar] [CrossRef] [PubMed]
- Zare, E.; Alirezaei, A.; Bakhtiyari, M.; Mansouri, A. Evaluating the effect of garlic extract on serum inflammatory markers of peritoneal dialysis patients: A randomized double-blind clinical trial study. BMC Nephrol. 2019, 20, 26. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Chhatwal, S.; Arora, S.; Sharma, S.; Singh, J.; Singh, N.; Bhandari, V.; Khurana, A. Antihyperglycemic, antihyperlipidemic, anti-inflammatory and adenosine deaminase-lowering effects of garlic in patients with type 2 diabetes mellitus with obesity. Diabetes Metab. Syndr. Obes. 2013, 6, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Zeb, I.; Ahmadi, N.; Nasir, K.; Kadakia, J.; Larijani, V.N.; Flores, F.; Li, D.; Budoff, M.J. Aged garlic extract and coenzyme Q10 have favorable effect on inflammatory markers and coronary atherosclerosis progression: A randomized clinical trial. J. Cardiovasc. Dis. Res. 2012, 3, 185–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkin, M.; Laight, D.; Cummings, M.H. The effects of garlic extract upon endothelial function, vascular inflammation, oxidative stress and insulin resistance in adults with type 2 diabetes at high cardiovascular risk. A pilot double blind randomized placebo-controlled trial. J. Diabetes Complicat. 2016, 30, 723–727. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.J.; Sutherland, W.H.; McCormick, M.P.; Yeoman, D.J.; de Jong, S.A. Aged garlic extract improves endothelial function in men with coronary artery disease. Phytother. Res. 2005, 19, 314–319. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, G.; Cong, X.; Wen, C. Black garlic improves heart function in patients with coronary heart disease by improving circulating antioxidant levels. Front. Physiol. 2018, 9, 1435. [Google Scholar] [CrossRef]
- Wang, L.; Mimura, K.; Fujimoto, S. Effects of black garlic supplementation on exercise-induced physiological responses. J. Phys. Fit. Sports Med. 2012, 1, 685–694. [Google Scholar] [CrossRef] [Green Version]
- McDougall, G.J.; Stewart, D. Berries and Health: A Review of the Evidence; Environmental and Biochemical Sciences Group, Enhancing Crop Productivity and Utilisation Theme, The James Hutton Institute: Dundee, UK, 2012. [Google Scholar]
- Nile, S.H.; Park, S.W. Edible berries: Bioactive components and their effect on human health. Nutrition 2014, 30, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Chen, G.; Liao, D.; Zhu, Y.; Xue, X. Effects of Berries Consumption on Cardiovascular Risk Factors: A Meta-analysis with Trial Sequential Analysis of Randomized Controlled Trials. Sci. Rep. 2016, 6, 23625. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, A. Berry anthocyanin intake and cardiovascular health. Mol. Aspects Med. 2018, 61, 76–82. [Google Scholar] [CrossRef] [Green Version]
- Yang, B.; Kortesniemi, M. Clinical evidence on potential health benefits of berries. Curr. Opin Food Sci. 2015, 2, 36–42. [Google Scholar] [CrossRef]
- Khurana, S.; Venkataraman, K.; Hollingsworth, A.; Piche, M.; Tai, T.C. Polyphenols: benefits to the cardiovascular system in health and in aging. Nutrients 2013, 5, 3779–3827. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Wang, T.T.Y.; Prior, R.L.; Pehrsson, P.R. Prevention of Atherosclerosis by Berries: The Case of Blueberries. J. Agric. Food Chem. 2018, 66, 9172–9188. [Google Scholar] [CrossRef]
- Cutler, B.R.; Petersen, C.; AnandhBabu, P.V. Mechanistic insights into the vascular effects of blueberries: Evidence from recent studies. Mol. Nutr. Food Res. 2017, 61, 1600271. [Google Scholar] [CrossRef]
- Basu, A.; Fu, D.X.; Wilkinson, M.; Simmons, B.; Wu, M.; Betts, N.M.; Du, M.; Lyons, T.J. Strawberries decrease atherosclerotic markers in subjects with metabolic syndrome. Nutr. Res. 2010, 30, 462–469. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.; Ling, W.; Du, Z.; Chen, Y.; Li, D.; Deng, S.; Liu, Z.; Yang, L. Effects of Anthocyanins on Cardiometabolic Health: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Adv. Nutr. 2017, 8, 684–693. [Google Scholar] [CrossRef]
- Shah, K.; Shah, P. Effect of Anthocyanin Supplementations on Lipid Profile and Inflammatory Markers: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Cholesterol 2018, 2018, 8450793. [Google Scholar] [CrossRef] [PubMed]
- Sangsefidi, Z.S.; Hasanizadeh, S.; Hosseinzadeh, M. Effect of purified anthocyanins or anthocyanin-rich extracts on C-reactive protein levels: A systematic review and meta-analysis of randomised clinical trials. Br. J. Nutr. 2018, 120, 1406–1414. [Google Scholar] [CrossRef] [PubMed]
- Bloedon, T.K.; Braithwaite, R.E.; Carson, I.A.; Klimis-Zacas, D.; Lehnhard, R.A. Impact of anthocyanin-rich whole fruit consumption on exercise-induced oxidative stress and inflammation: A systematic review and meta-analysis. Nutr. Rev. 2019, nuz018. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Sorn, S.R.; Park, Y.; Park, H.K. Anthocyanin Rich-Black Soybean Testa Improved Visceral Fat and Plasma Lipid Profiles in Overweight/Obese Korean Adults: A Randomized Controlled Trial. J. Med. Food 2016, 19, 995–1003. [Google Scholar] [CrossRef]
- Zhang, X.; Zhu, Y.; Song, F.; Yao, Y.; Ya, F.; Li, D.; Ling, W.; Yang, Y. Effects of purified anthocyanin supplementation on platelet chemokines in hypocholesterolemic individuals: A randomized controlled trial. Nutr. Metab. 2016, 13, 86. [Google Scholar] [CrossRef] [PubMed]
- Soltani, R.; Hakimi, M.; Asgary, S.; Ghanadian, S.M.; Keshvari, M.; Sarrafzadegan, N. Evaluation of the Effects of Vaccinium arctostaphylos L. Fruit Extract on Serum Lipids and hs-CRP Levels and Oxidative Stress in Adult Patients with Hyperlipidemia: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Evid. Based Complement Alternat. Med. 2014, 2014, 217451. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Suarez, J.M.; Giampieri, F.; Tulipani, S.; Casoli, T.; Di Stefano, G.; González-Paramás, A.M.; Santos-Buelga, C.; Busco, F.; Quiles, J.L.; Cordero, M.D.; et al. One-month strawberry-rich anthocyanin supplementation ameliorates cardiovascular risk, oxidative stress markers and platelet activation in humans. J. Nutr. Biochem. 2014, 25, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Davinelli, S.; Bertoglio, J.C.; Zarrelli, A.; Pina, R.; Scapagnini, G. A Randomized clinical trial evaluating the efficacy of an anthocyanin-maqui berry extract (Delphinol®) on oxidative stress biomarkers. J. Am. Coll. Nutr. 2015, 34, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Ling, W.; Yang, Y.; Chen, Y.; Tian, Z.; Du, Z.; Chen, J.; Xie, Y.; Liu, Z.; Yang, L. Role of Purified Anthocyanins in Improving Cardiometabolic Risk Factors in Chinese Men and Women with Prediabetes or Early Untreated Diabetes-A Randomized Controlled Trial. Nutrients 2017, 9, 1104. [Google Scholar] [CrossRef]
- Ferretti, G.; Turco, I.; Bacchetti, T. Apple as a Source of Dietary Phytonutrients: Bioavailability and Evidence of Protective Effects against Human Cardiovascular Disease. Food Nutr. Sci. 2014, 5, 1234–1246. [Google Scholar] [CrossRef] [Green Version]
- Boyer, J.; Liu, R.H. Apple phytochemicals and their health benefits. Nutr. J. 2004, 3, 5. [Google Scholar] [CrossRef]
- Hyson, D.A. A comprehensive review of apples and apple components and their relationship to human health. Adv. Nutr. 2011, 2, 408–420. [Google Scholar] [CrossRef]
- Dreher, M.L. Whole Fruits and Fruit Fiber Emerging Health Effects. Nutrients 2018, 10, 1833. [Google Scholar] [CrossRef]
- Menezes, R.; Rodriguez-Mateos, A.; Kaltsatou, A.; González-Sarrías, A.; Greyling, A.; Giannaki, C.; Andres-Lacueva, C.; Milenkovic, D.; Gibney, E.R.; Dumont, J.; et al. Impact of Flavonols on Cardiometabolic Biomarkers: A Meta-Analysis of Randomized Controlled Human Trials to Explore the Role of Interindividual Variability. Nutrients 2017, 9, 117. [Google Scholar] [CrossRef]
- Koutsos, A.; Tuohy, K.M.; Lovegrove, J.A. Apples and cardiovascular health--is the gut microbiota a core consideration? Nutrients 2015, 7, 3959–3998. [Google Scholar] [CrossRef] [PubMed]
- Ravn-Haren, G.; Dragsted, L.O.; Buch-Andersen, T.; Jensen, E.N.; Jensen, R.I.; Németh-Balogh, M.; Paulovicsová, B.; Bergström, A.; Wilcks, A.; Licht, T.R.; et al. Intake of whole apples or clear apple juice has contrasting effects on plasma lipids in healthy volunteers. Eur. J. Nutr. 2013, 52, 1875–1889. [Google Scholar] [CrossRef] [PubMed]
- Serban, M.C.; Sahebkar, A.; Zanchetti, A.; Mikhailidis, D.P.; Howard, G.; Antal, D.; Andrica, F.; Ahmed, A.; Aronow, W.S.; Muntner, P.; et al. Effects of Quercetin on Blood Pressure: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2016, 5, e002713. [Google Scholar] [CrossRef] [PubMed]
- Borgi, L.; Muraki, I.; Satija, A.; Willett, W.C.; Rimm, E.B.; Forman, J.P. Fruit and Vegetable Consumption and the Incidence of Hypertension in Three Prospective Cohort Studies. Hypertension 2016, 67, 288–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostadmohammadi, V.; Milajerdi, A.; Ayati, E.; Kolahdooz, F.; Asemi, Z. Effects of quercetin supplementation on glycemic control among patients with metabolic syndrome and related disorders: A systematic review and meta-analysis of randomized controlled trials. Phytother. Res. 2019, 33, 1330–1340. [Google Scholar] [CrossRef] [PubMed]
- Soriano-Maldonado, A.; Hidalgo, M.; Arteaga, P.; de Pascual-Teresa, S.; Nova, E. Effects of regular consumption of vitamin C-rich or polyphenol-rich apple juice on cardiometabolic markers in healthy adults: A randomized crossover trial. Eur. J. Nutr. 2014, 53, 1645–1657. [Google Scholar] [CrossRef] [PubMed]
- Chai, S.C.; Hooshmand, S.; Saadat, R.L.; Payton, M.E.; Brummel-Smith, K.; Arjmandi, B.H. Daily apple versus dried plum: Impact on cardiovascular disease risk factors in postmenopausal women. J. Acad. Nutr. Diet 2012, 112, 1158–1168. [Google Scholar] [CrossRef] [PubMed]
- Bondonno, C.P.; Yang, X.; Croft, K.D.; Considine, M.J.; Ward, N.C.; Rich, L.; Puddey, I.B.; Swinny, E.; Mubarak, A.; Hodgson, J.M. Flavonoid-rich apples and nitrate-rich spinach augment nitric oxide status and improve endothelial function in healthy men and women: A randomized controlled trial. Free Radic. Biol. Med. 2012, 52, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Bomser, J.; Joseph, E.L.; Di Silvestro, R.A. Intakes of apples or apple polyphenols decease plasma values for oxidized low-density lipoprotein/β2-glycoprotein I complex. J. Funct. Foods 2013, 5, 493–497. [Google Scholar] [CrossRef]
- Auclair, S.; Chironi, G.; Milenkovic, D.; Hollman, P.C.; Renard, C.M.; Mégnien, J.L.; Gariepy, J.; Paul, J.L.; Simon, A.; Scalbert, A. The Regular Consumption of a Polyphenol-Rich Apple Does Not Influence Endothelial Function: A Randomised Double-Blind Trial in Hypercholesterolemic Adults. Eur. J. Clin. Nutr. 2010, 64, 1158–1165. [Google Scholar] [CrossRef]
- Saarenhovi, M.; Salo, P.; Scheinin, M.; Lehto, J.; Lovró, Z.; Tiihonen, K.; Lehtinen, M.J.; Junnila, J.; Hasselwander, O.; Tarpila, A.; et al. The effect of an apple polyphenol extract rich in epicatechin and flavan-3-ol oligomers on brachial artery flow-mediated vasodilatory function in volunteers 2213 with elevated blood pressure. Nutr. J. 2017, 16, 73. [Google Scholar] [CrossRef]
- Conzatti, A.; Fróes, F.C.; Schweigert Perry, I.D.; Souza, C.G. Clinical and molecular evidence of the consumption of broccoli, glucoraphanin and sulforaphane in humans. Nutr. Hosp. 2014, 31, 559–569. [Google Scholar] [CrossRef]
- Renaud, E.N.; Lammerts van Bueren, E.T.; Myers, J.R.; Paulo, M.J.; van Eeuwijk, F.A.; Zhu, N.; Juvik, J.A. Variation in broccoli cultivar phytochemical content under organic and conventional management systems: Implications in breeding for nutrition. PLoS ONE 2014, 9, e95683. [Google Scholar] [CrossRef] [PubMed]
- Manchali, S.; Murthy, K.N.C.; Patil, B.S. Crucial facts about health benefits of popular cruciferous vegetables. J. Funct. Foods 2012, 4, 94–106. [Google Scholar] [CrossRef]
- Mahn, A.; Reyes, A. An overview of health-promoting compounds of broccoli (Brassica oleracea var. italica) and the effect of processing. Food Sci. Technol. Int. 2012, 18, 503–514. [Google Scholar] [CrossRef] [PubMed]
- Latté, K.P.; Appel, K.-E.; Lampen, A. Health benefits and possible risks of broccoli—An overview. Food Chem. Toxicol. 2011, 49, 3287–3309. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, K.E.; Juvik, J.A. Feasibility for improving phytonutrient content in vegetable crops using conventional breeding strategies: Case study with carotenoids and tocopherols in sweet corn and broccoli. J. Agric. Food Chem. 2009, 57, 4636–4644. [Google Scholar] [CrossRef]
- Cartea, M.E.; Francisco, M.; Soengas, P.; Velasco, P. Phenolic compounds in Brassica vegetables. Molecules 2011, 176, 251–280. [Google Scholar] [CrossRef]
- Vallejo, F.; Tomas-Barberan, F.A.; Garcia-Viguera, C. Phenolic compound contents in edible parts of broccoli inflorescences after domestic cooking. J. Sci. Food Agric. 2003, 83, 1511–1516. [Google Scholar] [CrossRef]
- Chun-Hsien, L.; Chi-Yue, C. Textural change and antioxidant properties of broccoli under different cooking treatments. Food Chem. 2005, 90, 9–15. [Google Scholar] [CrossRef]
- Zhang, X.; Shu, X.O.; Xiang, Y.B.; Yang, G.; Li, H.; Gao, J.; Cai, H.; Gao, Y.T.; Zheng, W. Cruciferous vegetable consumption is associated with a reduced risk of total and cardiovascular disease mortality. Am. J. Clin. Nutr. 2011, 94, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Blekkenhorst, L.C.; Bondonno, C.P.; Lewis, J.R.; Devine, A.; Zhu, K.; Lim, W.H.; Woodman, R.J.; Beilin, L.J.; Prince, R.L.; Hodgson, J.M. Cruciferous and Allium Vegetable Intakes Are Inversely Associated with 15-Year Atherosclerotic Vascular Disease Deaths in Older Adult Women. J. Am. Heart Assoc. 2017, 6, e006558. [Google Scholar] [CrossRef] [PubMed]
- Armah, C.N.; Derdemezis, C.; Traka, M.H.; Dainty, J.R.; Doleman, J.F.; Saha, S.; Leung, W.; Potter, J.F.; Lovegrove, J.A.; Mithen, R.F. Diet rich in high glucoraphanin broccoli reduces plasma LDL cholesterol: Evidence from randomised controlled trials. Mol. Nutr. Food Res. 2015, 59, 918–926. [Google Scholar] [CrossRef] [PubMed]
- Bahadoran, Z.; Mirmiran, P.; Hosseinpanah, F.; Rajab, A.; Asghari, G.; Azizi, F. Broccoli sprouts powder could improve serum triglyceride and oxidized LDL/LDL-cholesterol ratio in type 2 diabetic patients: A randomized double-blind placebo-controlled clinical trial. Diabetes Res. Clin. Pract. 2012, 96, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Armah, C.N.; Traka, M.H.; Dainty, J.R.; Defernez, M.; Janssens, A.; Leung, W.; Doleman, J.F.; Potter, J.F.; Mithen, R.F. A diet rich in high-glucoraphanin broccoli interacts with genotype to reduce discordance in plasma metabolite profiles by modulating mitochondrial function. Am. J. Clin. Nutr. 2013, 98, 712–722. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, B.; Bellostas Muguerza, N.; Petersen, A.M.; Kveiborg, B.; Madsen, C.R.; Thomas, H.; Ihlemann, N.; Sørensen, J.C.; Køber, L.; Sørensen, H.; et al. Ingestion of Broccoli Sprouts Does Not Improve Endothelial Function in Humans with Hypertension. PLoS ONE 2010, 5, e12461. [Google Scholar] [CrossRef]
- Mirmiran, P.; Bahadoran, Z.; Hosseinpanah, F.; Keyzad, A.; Azizi, F. Effects of broccoli sprout with high sulforaphane concentration on inflammatory markers in type 2 diabetic patients: A randomized double-blind placebo-controlled clinical trial. J. Func. Foods 2012, 4, 837–841. [Google Scholar] [CrossRef]
- Bahadoran, Z.; Mirmiran, P.; Hosseinpanah, F.; Hedayati, M.; Hosseinpour-Niazi, S.; Azizi, F. Broccoli sprouts reduce oxidative stress in type 2 diabetes: A randomized double-blind clinical trial. Eur. J. Clin. Nutr. 2011, 65, 972–977. [Google Scholar] [CrossRef]
- López-Chillón, M.T.; Carazo-Díaz, C.; Prieto-Merino, D.; Zafrilla, P.; Moreno, D.A.; Villaño, D. Effects of long-term consumption of broccoli sprouts on inflammatory markers in overweight subjects. Clin. Nutr. 2019, 38, 745–752. [Google Scholar] [CrossRef]
- Jiang, Y.; Wu, S.H.; Shu, X.O.; Xiang, Y.B.; Ji, B.T.; Milne, G.L.; Cai, Q.; Zhang, X.; Gao, Y.T.; Zheng, W.; et al. Cruciferous vegetable intake is inversely correlated with circulating levels of proinflammatory markers in women. J. Acad. Nutr. Diet 2014, 114, 700–708.e2. [Google Scholar] [CrossRef] [PubMed]
- Blekkenhorst, L.C.; Bondonno, C.P.; Lewis, J.R.; Woodman, R.J.; Devine, A.; Bondonno, N.P.; Lim, W.H.; Zhu, K.; Beilin, L.J.; Thompson, P.L.; et al. Cruciferous and Total Vegetable Intakes Are Inversely Associated with Subclinical Atherosclerosis in Older Adult Women. J. Am. Heart Assoc. 2018, 7, e008391. [Google Scholar] [CrossRef] [PubMed]
- Mellor, D.D. Cocoa: Composition and Health Effects; Elsevier: Birmingham, UK, 2016; pp. 179–184. [Google Scholar]
- Tuenter, E.; Foubert, K.; Pieters, L. Mood Components in Cocoa and Chocolate: The Mood Pyramid. Planta Med. 2018, 84, 839–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morze, J.; Schwedhelm, C.; Bencic, A.; Hoffmann, G.; Boeing, H.; Przybylowicz, K.; Schwingshackl, L. Chocolate and risk of chronic disease: A systematic review and dose-response meta-analysis. Eur. J. Nutr. 2019. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Salvatori, T.; Nucci, D.; Villarini, M.; Moretti, M. Can chocolate consumption reduce cardio-cerebrovascular risk? A systematic review and meta-analysis. Nutrition 2018, 46, 103–114. [Google Scholar] [CrossRef]
- Yuan, S.; Li, X.; Jin, Y.; Lu, J. Chocolate Consumption and Risk of Coronary Heart Disease, Stroke, and Diabetes: A Meta-Analysis of Prospective Studies. Nutrients 2017, 9, 688. [Google Scholar] [CrossRef] [PubMed]
- Gong, F.; Yao, S.; Wan, J.; Gan, X. Chocolate Consumption and Risk of Heart Failure: A Meta-Analysis of Prospective Studies. Nutrients 2017, 9, 402. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Åkesson, A.; Gigante, B.; Wolk, A. Chocolate consumption and risk of myocardial infarction: A prospective study and meta-analysis. Heart 2016, 102, 1017–1022. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Liu, Y.; Sun, X.Z.; Wang, B.Y.; Zhao, Y.; Liu, D.C.; Zhang, D.D.; Liu, X.J.; Zhang, R.Y.; Sun, H.H.; et al. Chocolate consumption and risk of cardiovascular diseases: A meta-analysis of prospective studies. Heart 2019, 105, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Zhang, I.; Li, A.; Manson, J.E.; Sesso, H.D.; Wang, L.; Liu, S. Cocoa Flavanol Intake and Biomarkers for Cardiometabolic Health: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Nutr. 2016, 146, 2325–2333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Sarrías, A.; Combet, E.; Pinto, P.; Mena, P.; Dall’Asta, M.; Garcia-Aloy, M.; Rodríguez-Mateos, A.; Gibney, E.R.; Dumont, J.; Massaro, M.; et al. A Systematic Review and Meta-Analysis of the Effects of Flavanol-Containing Tea, Cocoa and Apple Products on Body Composition and Blood Lipids: Exploring the Factors Responsible for Variability in Their Efficacy. Nutrients 2017, 9, 746. [Google Scholar] [CrossRef]
- Sarriá, B.; Martínez-López, S.; Sierra-Cinos, J.L.; García-Diz, L.; Mateos, R.; Bravo, L. Regular consumption of a cocoa product improves the cardiometabolic profile in healthy and moderately hypercholesterolaemic adults. Br. J. Nutr. 2014, 111, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Martínez-López, S.; Sarriá, B.; Sierra-Cinos, J.L.; Goya, L.; Mateos, R.; Bravo, L. Realistic intake of a flavanol-rich soluble cocoa product increases HDL-cholesterol without inducing anthropometric changes in healthy and moderately hypercholesterolemic subjects. Food Funct. 2014, 5, 364–374. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.M.; Smolders, L.; Lin, Y.; de Roo, N.; Trautwein, E.A.; van Duynhoven, J.; Mensink, R.P.; Plat, J.; Mihaleva, V.V. Effect of Theobromine Consumption on Serum Lipoprotein Profiles in Apparently Healthy Humans with Low HDL-Cholesterol Concentrations. Front. Mol. Biosci. 2017, 4, 59. [Google Scholar] [CrossRef] [PubMed]
- Ried, K.; Sullivan, T.R.; Fakler, P.; Frank, O.R.; Stocks, N.P. Effect of cocoa on blood pressure. Cochrane Database Syst. Rev. 2012, 15, CD008893. [Google Scholar] [CrossRef]
- West, S.G.; McIntyre, M.D.; Piotrowski, M.J.; Poupin, N.; Miller, D.L.; Preston, A.G.; Wagner, P.; Groves, L.F.; Skulas-Ray, A.C. Effects of dark chocolate and cocoa consumption on endothelial function and arterial stiffness in overweight adults. Br. J. Nutr. 2014, 111, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Rull, G.; Mohd-Zain, Z.N.; Shiel, J.; Lundberg, M.H.; Collier, D.J.; Johnston, A.; Warner, T.D.; Corder, R. Effects of high flavanol dark chocolate on cardiovascular function and platelet aggregation. Vascul. Pharmacol. 2015, 71, 70–78. [Google Scholar] [CrossRef] [Green Version]
- Pereira, T.; Bergqvist, J.; Vieira, C.; GrünerSveälv, B.; Castanheira, J.; Conde, J. Randomized study of the effects of cocoa-rich chocolate on the ventricle-arterial coupling and vascular function of young, healthy adults. Nutrition 2019, 63–64, 175–183. [Google Scholar] [CrossRef]
- Montagnana, M.; Danese, E.; Angelino, D.; Mena, P.; Rosi, A.; Benati, M.; Gelati, M.; Salvagno, G.L.; Favaloro, E.J.; Del Rio, D.; et al. Dark chocolate modulates platelet function with a mechanism mediated by flavan-3-ol metabolites. Medicine 2018, 97, e13432. [Google Scholar] [CrossRef]
- Kwok, C.S.; Boekholdt, S.M.; Lentjes, M.A.; Loke, Y.K.; Luben, R.N.; Yeong, J.K.; Wareham, N.J.; Myint, P.K.; Khaw, K.T. Habitual chocolate consumption and risk of cardiovascular disease among healthy men and women. Heart 2015, 101, 1279–1287. [Google Scholar] [CrossRef] [Green Version]
- Peluso, I.; Miglio, C.; Morabito, G.; Ioannone, F.; Serafini, M. Flavonoids and immune function in human: A systematic review. Crit. Rev. Food Sci. Nutr. 2015, 55, 383–395. [Google Scholar] [CrossRef] [PubMed]
- Suen, J.; Thomas, J.; Kranz, A.; Vun, S.; Miller, M. Effect of Flavonoids on Oxidative Stress and Inflammation in Adults at Risk of Cardiovascular Disease: A Systematic Review. Healthcare 2016, 4, 69. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Xiao, Y.Y. Grape Phytochemicals and Associated Health Benefits. Crit. Rev. Food Sci. Nutr. 2013, 53, 1202–1225. [Google Scholar] [CrossRef] [PubMed]
- Howes, M.J.; Simmonds, M.S. The role of phytochemicals as micronutrients in health and disease. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 558–566. [Google Scholar] [CrossRef]
- Ferrieres, J. The French paradox: Lessons for other countries. Heart 2004, 90, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Breuss, J.; Atanasov, A.; Uhrin, P. Resveratrol and Its Effects on the Vascular System. Int. J. Mol. Sci. 2019, 20, 1523. [Google Scholar] [CrossRef]
- Mashhadi, D.; Salari, R.; Ghorbanzadeh, H. The effect of resveratrol dose and duration of treatment on blood pressure in patients with cardiovascular disorders: A systematic review. Curr. Drug Discov. Technol. 2019. [Google Scholar] [CrossRef]
- Woerdeman, J.; van Poelgeest, E.; Ket, J.C.F.; Eringa, E.C.; Serné, E.H.; Smulders, Y.M. Do grape polyphenols improve metabolic syndrome components? A systematic review. Eur. J. Clin. Nutr. 2017, 71, 1381–1392. [Google Scholar] [CrossRef]
- Li, S.H.; Zhao, P.; Tian, H.B.; Chen, L.H.; Cui, L.Q. Effect of Grape Polyphenols on Blood Pressure: A Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2015, 10, e0137665. [Google Scholar] [CrossRef]
- Liu, Y.; Ma, W.; Zhang, P.; He, S.; Huang, D. Effect of resveratrol on blood pressure: A meta-analysis of randomized controlled trials. Clin. Nutr. 2015, 34, 27–34. [Google Scholar] [CrossRef]
- Neto, M.M.; da Silva, T.F.; de Lima, F.F.; Siqueira, T.M.Q.; Toscano, L.T.; de Moura, S.K.M.S.F.; Silva, A.S. Whole Red Grape Juice Reduces Blood Pressure at Rest and Increases Post-Exercise Hypotension. J. Am. Coll. Nutr. 2017, 36, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Draijer, R.; de Graaf, Y.; Slettenaar, M.; de Groot, E.; Wright, C. Consumption of a Polyphenol-Rich Grape-Wine Extract Lowers Ambulatory Blood Pressure in Mildly Hypertensive Subjects. Nutrients 2015, 7, 3138–3153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urquiaga, I.; D’Acuña, S.; Pérez, D.; Dicenta, S.; Echeverría, G.; Rigotti, A.; Leighton, F. Wine grape pomace flour improves blood pressure, fasting glucose and protein damage in humans: A randomized controlled trial. Biol. Res. 2015, 48, 49. [Google Scholar] [CrossRef]
- Zhu, X.; Wu, C.; Qiu, S.; Yuan, X.; Li, L. Effects of resveratrol on glucose control and insulin sensitivity in subjects with type 2 diabetes: Systematic review and meta-analysis. Nutr. Metab. 2017, 14, 60. [Google Scholar] [CrossRef]
- Liu, K.; Zhou, R.; Wang, B.; Mi, M.T. Effect of resveratrol on glucose control and insulin sensitivity: A meta-analysis of 11 randomized controlled trials. Am. J. Clin. Nutr. 2014, 99, 1510–1519. [Google Scholar] [CrossRef] [PubMed]
- Pollack, R.M.; Barzilai, N.; Anghel, V.; Kulkarni, A.S.; Golden, A.; O’Broin, P.; Sinclair, D.A.; Bonkowski, M.S.; Coleville, A.J.; Powell, D.; et al. Resveratrol Improves Vascular Function and Mitochondrial Number but Not Glucose Metabolism in Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 1703–1709. [Google Scholar] [CrossRef]
- Imamura, H.; Yamaguchi, T.; Nagayama, D.; Saiki, A.; Shirai, K.; Tatsuno, I. Resveratrol Ameliorates Arterial Stiffness Assessed by Cardio-Ankle Vascular Index in Patients with Type 2 Diabetes Mellitus. Int. Heart J. 2017, 58, 577–583. [Google Scholar] [CrossRef]
- Haghighatdoost, F.; Hariri, M. Can resveratrol supplement change inflammatory mediators? A systematic review and meta-analysis on randomized clinical trials. Eur. J. Clin. Nutr. 2019, 73, 345–355. [Google Scholar] [CrossRef]
- Koushki, M.; Dashatan, N.A.; Meshkani, R. Effect of Resveratrol Supplementation on Inflammatory Markers: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Clin. Ther. 2018, 40, 1180–1192. [Google Scholar] [CrossRef]
- Tabrizi, R.; Tamtaji, O.R.; Lankarani, K.B.; Mirhosseini, N.; Akbari, M.; Dadgostar, E.; Peymani, P.; Asemi, Z. The effects of resveratrol supplementation on biomarkers of inflammation and oxidative stress among patients with metabolic syndrome and related disorders: A systematic review and meta-analysis of randomized controlled trials. Food Funct. 2018, 9, 6116–6128. [Google Scholar] [CrossRef]
- Sahebkar, A.; Serban, C.; Ursoniu, S.; Wong, N.D.; Muntner, P.; Graham, I.M.; Mikhailidis, D.P.; Rizzo, M.; Rysz, J.; Sperling, L.S.; et al. Lack of efficacy of resveratrol on C-reactive protein and selected cardiovascular risk factors—Results from a systematic review and meta-analysis of randomized controlled trials. Int. J. Cardiol. 2015, 189, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Knowlton, A. Olives. Curr. Biol. 2013, 23, R364–R365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visioli, F.; Galli, C. Biological Properties of Olive Oil Phytochemicals. Crit. Rev. Food Sci. Nutr. 2002, 42, 209–221. [Google Scholar] [CrossRef] [PubMed]
- Gouvinhas, I.; Machado, N.; Sobreira, C.; Domínguez-Perles, R.; Gomes, S.; Rosa, E.; Barros, A. Critical Review on the Significance of Olive Phytochemicals in Plant Physiology and Human Health. Molecules 2017, 22, 1986. [Google Scholar] [CrossRef] [PubMed]
- Gorzynik-Debicka, M.; Przychodzen, P.; Cappello, F.; Kuban-Jankowska, A.; Marino Gammazza, A.; Knap, N.; Wozniak, M.; Gorska-Ponikowska, M. Potential Health Benefits of Olive Oil and Plant Polyphenols. Int. J. Mol. Sci. 2018, 19, 686. [Google Scholar] [CrossRef]
- George, E.S.; Marshall, S.; Mayr, H.L.; Trakman, G.L.; Tatucu-Babet, O.A.; Lassemillante, A.-C.M.; Bramley, A.; Reddy, A.J.; Forsyth, A.; Tierney, A.C.; et al. The effect of high-polyphenol extra virgin olive oil on cardiovascular risk factors: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2018, 30, 1–24. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Krause, M.; Schmucker, C.; Hoffmann, G.; Rücker, G.; Meerpohl, J.J. Impact of different types of olive oil on cardiovascular risk factors: A systematic review and network meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 1030–1039. [Google Scholar] [CrossRef]
- Tsartsou, E.; Proutsos, N.; Castanas, E.; Kampa, M. Network Meta-Analysis of Metabolic Effects of Olive-Oil in Humans Shows the Importance of Olive Oil Consumption with Moderate Polyphenol Levels as Part of the Mediterranean Diet. Front. Nutr. 2019, 6, 6. [Google Scholar] [CrossRef]
- Ghobadi, S.; Hassanzadeh-Rostami, Z.; Mohammadian, F.; Nikfetrat, A.; Ghasemifard, N.; RaeisiDehkordi, H.; Faghih, S. Comparison of blood lipid-lowering effects of olive oil and other plant oils: A systematic review and meta-analysis of 27 randomized placebo-controlled clinical trials. Crit. Rev. Food Sci. Nutr. 2019, 59, 2110–2124. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Bogensberger, B.; Benčič, A.; Knüppel, S.; Boeing, H.; Hoffmann, G. Effects of oils and solid fats on blood lipids: A systematic review and network meta-analysis. J. Lipid Res. 2018, 59, 1771–1782. [Google Scholar] [CrossRef]
- Khaw, K.T.; Sharp, S.J.; Finikarides, L.; Afzal, I.; Lentjes, M.; Luben, R.; Forouhi, N.G. Randomised trial of coconut oil, olive oil or butter on blood lipids and other cardiovascular risk factors in healthy men and women. BMJ Open 2018, 8, e020167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lockyer, S.; Rowland, I.; Spencer, J.P.E.; Yaqoob, P.; Stonehouse, W. Impact of phenolic-rich olive leaf extract on blood pressure, plasma lipids and inflammatory markers: A randomised controlled trial. Eur. J. Nutr. 2017, 56, 1421–1432. [Google Scholar] [CrossRef] [PubMed]
- Zamora-Zamora, F.; Martínez-Galiano, J.M.; Gaforio, J.J.; Delgado-Rodríguez, M. Effects of olive oil on blood pressure: A systematic review and meta-analysis. Grasas y Aceites 2018, 69, e272. [Google Scholar] [CrossRef]
- Zamora-Zamora, F.; Martínez Galiano, J.M.; Gaforio Martínez, M.J.J.; Delgado Rodríguez, M. Olive Oil and BodyWeight. Systematic Review and Meta-Analysis of Randomized Controlled Trials. Rev. Esp. Salud Publica 2018, 92, e201811083. [Google Scholar]
- Fernandes, J.; Fialho, M.; Santos, R.; Peixoto-Plácido, C.; Madeira, T.; Sousa-Santos, N.; Virgolino, A.; Santos, O.; Vaz Carneiro, A. Is olive oilgoodforyou? A systematic review and meta-analysis on anti-inflammatory benefits from regular dietary intake. Nutrition 2019, 69, 110559. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Christoph, M.; Hoffmann, G. Effects of Olive Oil on Markers of Inflammation and Endothelial Function—A Systematic Review and Meta-Analysis. Nutrients 2015, 7, 7651–7675. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Study Design | Study Duration | Participants | Type of Study | Findings Plasma Lipids Analyzed Markers | |
|---|---|---|---|---|---|---|
| Valderas-Martinez et al. [53] | A single dose of 7.0 g of RT/kg of BW, 3.5 g of TS/kg BW, 3.5 g of TSOO/kg BW and 0.25 g of sugar dissolved in water/kg BW on a single occasion on four different days. | Acute | 40 healthy subjects | Open, prospective, randomized, cross-over, controlled feeding trial. | ↓ TC, TG and ↑ HDL. | ↑ IL-10 and ↓ MCP-1 TSOO: ↓ VCAM-1, IL-6, LFA-1 (lymphocytes) and CD36 (monocytes). |
| Burton-Freeman et al. [55] | Consumed high-fat meals of processed tomato product or non-tomato on two separate occasions. | Acute | 25 participants (mean age = 27 ± 8 years; mean BMI= 22 ± 2). | Single center, randomized, cross-over, two-arm, two-sequence, placebo-controlled, 360-min postprandial trial. | ↓OxLDL (p < 0.05) and ↑ IL-6 (p < 0.0001). | |
| Li et al. [50] | 280 mL of tomato juice (32.5 mg of lycopene) daily for 8-weeks. | Short | 30 young females, aged between 20 to 30 years with a BMI ≥20. | Uncontrolled supplementation trial | ↓ waist circumference and cholesterol levels. | ↓ MCP-1, ↑ adiponectin. |
| García-Alonso et al. [51] | 500 mL of n-3 PUFA-enriched juice (181 mg of phenols and 26.5 mg of lycopene) daily for 2-weeks. | Short | 18 healthy women (aged 35–55 years) and BMI: 21–30. | Randomized single-blind intervention trial. | ↓ ICAM-1, VCAM-1 and homocysteine ↓ MDA ↑ antioxidant capacity ↑β-Carotene and vitamin C. | |
| Deplanque et al. [56] | Lycopene and phytosterols in a 1:1 ratio (15 mg) or placebo for 2-weeks. | Short | 146 healthy normal weight individuals (BMI: ≥18.5 and <25), aged 18–70 year. | Randomized, double-blind, parallel-groups, placebo-controlled study. | ↓OxLDL (p < 0.0001) No changes in glucose, insulin, or TG levels. | |
| Ghavipour et al. [57] | 330 mL of tomato juice (37.0 mg of lycopene) or water daily for 20 days. | Short | 64 overweight or obese (BMI ≥ 25) female students | Randomized controlled clinical trial. | ↑ TAC ↑ SOD, GPx and CAT. ↓ MDA | |
| Pourahmadi et al. [58] | 330 mL of tomato juice (60 mg of lycopene) or water daily for 20 days. | Short | 75 overweight or obese female students, aged 20 to 30 years, and BMI ≥ 25. | Randomized controlled clinical trial. | No changes in SOD, GPx or CAT. | |
| Thies et al. [54] | <10 mg lycopene /day; 32–50 mg lycopene/day; 10 mg lycopene /day for 3-months. | Short | 225 volunteers aged 40–65 y and BMI: 18.5 and 35. | Single-blind, randomized controlled intervention trial. | No changes in markers of insulin resistance or sensitivity. | No changes in inflammatory markers. |
| Reference | Study Design | Study Duration | Participants | Type of Study | Findings Plasma Lipids Analyzed markers | |
|---|---|---|---|---|---|---|
| Wang et al. [92] | Daily doses of 9 g Black Garlic or placebo during 14 days. | Short | 19 healthy, nonsmoking and untrained males (22.8 ± 6.0). | Double-blind, parallel design study. | ↓dROMs, lipid peroxide, 8-iso-prostaglandin F2α. | |
| Atkin et al. [89] | 1200 mg of AGE or placebo daily for four weeks. | 26 subjects with T2DM, aged 18 to 70 years. | Double blind, placebo-controlled crossover pilot study. | No changes in TAOS, GSH/GSSG, LHP or CRP, IL-6. | ||
| Williams et al. [90] | 2.4 g/day of AGE or placebo for two weeks. | Short | 15 men with angiographically proven CAD aged 45 to 70 years. | Randomized, placebo-controlled, cross-over design. | No changes in oxLDL and peroxides, CRP and IL-6 and endothelial activation (VCAM-1) ↑ FMD. | |
| Zare et al. [86] | 400 mg of standardized garlic extract twice a day or placebo for two months. | Short | 42 peritoneal dialysis patients, aged 18 to 80 years. | Parallel-designed double blind randomized clinical trial. | ↓ IL-6 and CRP. | |
| Kumar et al. [87] | Control group and 500 mg/day garlic extract of Allium sativum twice a day for 12 weeks. | Short | 60 patients with T2DM and obesity. | Open-label, prospective, comparative study. | ↓Fasting blood glucose and postprandial blood glucose. ↓ TC, LDL and TG and ↑ HDL | ↓ CRP and adenosine deaminase. |
| Ried et al. [70] | Daily intake of 1.2 g of AGE (1.2 mg S-allylcysteine) or placebo for 12 weeks. | Short | 49 participants with uncontrolled hypertension (SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg). | Double-blind randomized placebo-controlled trial. | ↓ SBP (10 ± 3.6 mmHg) and DBP (5.4 ± 2.3 mmHg). ↓ Pulse pressure and arterial stiffness (p < 0.05). | ↓ TNF-α and IL-6 Improvement of gut microbiota (↑ Lactobacillus and Clostridia species). |
| Zeb et al. [88] | Daily intake of AGE (1200 mg) plus CoQ10 (120 mg) or placebo for one year. | Intermediate | 65 intermediate risk (CAC score >10 at baseline) firefighters (mean age: 55 ± 6 years). | Placebo-controlled, double-blind, randomized trial. | AGE+CoQ10: ↓ CAC progression (32 ± 6 vs. 58 ± 8, p = 0.01) and ↓ CRP (−0.12 ± 0.24 vs. 0.91 ± 0.56 mg/L, p < 0.05). | |
| Liu et al. [91] | 20 g garlic (2.60 mg GAeq/g) daily or placebo for six months. | Intermediate | 120 chronic heart failure patients caused by CHD. Age 35–75 years. | Randomized controlled clinical trial. | ↓ Nt-proBNP ↑ Circulating antioxidant levels. | |
| Reference | Study Design | Study Duration | Participants | Type of Study | Findings Plasma Lipids Analyzed Markers | |
|---|---|---|---|---|---|---|
| Lee et al. [106] | Daily intake of 2.5 g of anthocyanin-rich (12.58 mg/g extract) black soybean test extracts or placebo for two months. | Short | 63 overweight or obese participants, with BMI > 23 or waist circumference > 90 cm for males, >85 cm for females. Age 19 to 65 years. | Randomized, double-blinded, and placebo-controlled clinical trial. | ↓ abdominal fat, TG and LDL ↓ TC/HDL and LDL/HDL | ↓ MCP-1 (p = 0.031) and TNF-α (p = 0.011) |
| Soltani et al. [108] | Twice daily intake of 500 mg of dried granules equivalent to 45 ± 2 mg of total anthocyanin or placebo for one month. | Short | 50 hyperlipidemic adult patients (age ≥ 18 years). | Randomized, double-blind, placebo-controlled clinical trial. | ↓ TC (p < 0.001), LDL (p = 0.004), TG (p < 0.001). No changes in HDL | MDA (p = 0.013) No changes in CRP |
| Alvarez-Suarez et al. [109] | Intake of 500 g of strawberries for one month. | Short | 23 healthy volunteers (age 27 ± 3.2 and BMI 21.74 ± 2.5 kg/m2). | Randomized, double-blind, placebo-controlled clinical trial. | ↓ TC (−8.78%), LDL (−13.72%) and TG levels (−20.80%). | ↓ MDA, urinary 8-OHdG and isoprostane levels (p < 0.05; all) |
| Davinielli et al. [110] | Three capsules of 150 mg standardized maqui berry extract containing 54 mg of anthocyanins daily or placebo for four weeks. | Short | 42 healthy participants, aged 45–65 years and BMI between 25 and 30 kg/m2. | Randomized, double-blind, placebo-controlled clinical trial. | ↓ oxLDL and 8-iso-prostaglandin F2α | |
| Yang et al. [111] | Daily intake of 320 mg of purified anthocyanins (from bilberry and blackcurrant) or placebo for 12 weeks. | Short | 138 volunteers aged 40−75 years with prediabetes or early untreated diabetes | Randomized, double-blind, placebo-controlled clinical trial. | ↓ HbA1c (−0.14%, p = 0.005), LDL (−0.2 mmol/L, p = 0.04), apoA-1 (0.09 g/L, p = 0.02), and apo B (−0.07 g/L, p = 0.01) | No changes in CRP levels. |
| Zhang et al. [107] | Daily intake of 320 mg of purified anthocyanins or placebo for six months. | Intermediate | 146 hypercholesterolemic individuals. Age from 40 to 65 years | Randomized, double-blind, placebo-controlled trial. | ↓ CXCL7 (−12.32% vs. 4.22%, p = 0.001), CXCL5 (−9.95% vs. 1.93%, p = 0.011), CXCL8 (−6.07% vs. 0.66%, p = 0.004), CXCL12 (−8.11% vs. 5.43%, p = 0.023) and CCL2 levels (−11.63% vs. 12.84%, p = 0.001). ↓hs-CRP, IL-1β and sP-selectin | |
| Reference | Study Design | Study Duration | Participants | Type of Study | Findings Plasma Lipids Analyzed Markers | |
|---|---|---|---|---|---|---|
| Bondonno et al. [124] | Four energy-matched treatments: control (low-flavonoid apple control and low-nitrate control), apple (high-flavonoid apple active and low-nitrate control), spinach (low-flavonoid apple control and nitrate-rich spinach active), and apple+spinach (high-flavonoid apple active and nitrate-rich spinach active) at 100, 150, and 200 min after lunch/intervention (acute effects). | Kinetic | 30 healthy men and women. | A randomized, controlled, crossover trial. | ↑ FMD ↑ nitric oxide status | |
| Soriano-Maldonado et al. [122] | Twice daily intake of 250 mL/day of apple juice (60 mg/L vitamin C and 510 mg catechin equivalent/L) or a polyphenol-rich juice (22 mg/L vitamin C and 993 mg catechin equivalent/L) for one month. | Short | 20 healthy subjects, aged 21–29 years, BMI ≤ 27.5 kg/m2. | A randomized cross-over trial. | ↑ Plasma antioxidant activity (p = 0.031). ↓ IL-8, IL-6, IL-10, MCP-1, PAI-1, E-selectin, VCAM-1, and ICAM-1. | |
| Zhao et al. [125] | Three treatments: 1) one apple per day; 2) an apple extract in capsules (twice daily, 194 mg polyphenols/day); 3) Control group for one month. | Short | 51 healthy middle-aged adults (aged 40–60 years old) | Randomized, double-blind, placebo-controlled clinical trial. | Whole apple and extract: ↓oxLDL-β2GPI. No changes in SOD. | |
| Auclair et al. [126] | Daily intake of 40 g of two lyophilized apples: 1) polyphenol-rich (1.43 g of polyphenols per day); 2) polyphenol-poor (0.21 g of polyphenols per day) for four weeks. | Short | 30 hypercholesterolemic volunteers, with a mean age of 52.6 ± 5.5 years, a mean BMI of 25.7 ± 2.6. | Double-blind, randomized crossover trial. | No changes in lipid profile. | No changes in FMD, homocysteine, antioxidant capacity |
| Saarenhovi et al. [127] | Daily intake of apple polyphenol extract (100 mg epicatechin and flavan-3-ol) or placebo for four weeks. | Short | 81 otherwise healthy participants aged 40–65 years, with borderline hypertension or unmedicated mild hypertension. | Single-center, repeated-dose, double-blind, placebo-controlled, crossover study | No significant changes were observed in NMD, CRP, E-selectin, VCAM-1 or ICAM-1, ADMA, vWF, PAI-1 and asymmetric dimethylarginine. | |
| Chai et al. [123] | Daily intake of 75 g of dried apple or 75 g of dried plum (comparative control) for 12 months. | Intermediate | 160 healthy postmenopausal women (1–10 years after menopause), without hormonal treatment. | Randomized, double-blind, placebo-controlled clinical trial. | ↓ TC (9%) and LDL (16%) at 3 months ↓ TC (13%) and LDL (24%) at 6 months. | ↓ lipid hydroperoxide and CRP |
| Reference | Study Design | Study Duration | Participants | Type of Study | Findings Plasma Lipids Analyzed Markers | |
|---|---|---|---|---|---|---|
| Mirmiran et al. [143] | Daily intake of 10 g (225 µmol sulforaphane), 5 g (112 µmol sulforaphane) of broccoli sprouts powder or placebo for four weeks. | Short | 81 patients with T2DM aged 18–60 years. | Parallel, randomized, double-blind, and placebo controlled clinical trial. | ↓ hs-CRP (10 g: −20.5% and 5g: −16.4%). No significant changes in TNF-α or IL-6. | |
| Bahadoran et al. [140,144] | Daily intake of 10 g (225 µmol sulforaphane), 5 g (112 µmol sulforaphane) of broccoli sprouts powder or placebo for four weeks. | Short | 81 patients with T2DM, aged 18–60 years | Parallel, randomized, double-blind, and placebo controlled clinical trial. | 10 g/day: ↑ HDL (p < 0.01 for treatment). | ↓ MDA (p = 0.001 for treatment effect), oxLDL (p = 0.03 for treatment effect), OSI (p = 0.001 for treatment effect) and ↑ TAC (p = 0.001 for treatment effect). 10g/day: ↓oxLDL/LDL ratio, TG and AIP (p < 0.05 for treatment effect) |
| Lopez-Chillón et al. [145] | Daily consumption of broccoli sprouts (30 g/day) for 10 weeks. After, normal diet without broccoli sprouts intake for 10 weeks (the follow-up phase). | Short | 40 no- smoking overweight subjects. Aged 35–55 years and BMI from 24.9 to 29.9 kg/m2 | Interventional follow-up study. | ↓ IL-6 significantly decreased (−38%). ↓ CRP (−59%, p < 0.05). | |
| Jiang et al. [146] | Evaluate association between vegetable intake with inflammatory and oxidative stress markers. | 1005 women (40–70 y of age) selected from the Shanghai Women’s Health Study (SWHS). | Cross-sectional study. | ↓ TNF-α (−2.66%, p = 0.01), IL-1β (−18.18%, p = 0.02), and IL-6 (−24.68%, p = 0.02). | ||
| Reference | Study Design | Study Duration | Participants | Type of Study | Findings Plasma Lipids/Others Analyzed Markers | |
|---|---|---|---|---|---|---|
| Sarriá et al. [158] | Intervention group consuming two servings/day (15 g each) of a cocoa product rich in fiber in milk vs. control group consuming only milk for one month. | Short | Healthy (n = 24) and moderate hypercholesterolemic (>2000 mg/L, n = 20) subjects. | Randomized, controlled, cross-over, free-living study | ↑ HDL-c concentration ↓fasting serum glucose levels. | ↓ IL-1β and IL-10 |
| Martínez-López et al. [159] | Intervention group consumed two servings/day (7.5 g per serving) of a soluble cocoa product in milk vs. control group only taking milk for one month. | Short | Healthy (n =24) and moderate hypercholesterolemic (200–240 mg/dL, n = 20) individuals. | Non-randomized, controlled, crossover, free-living study | ↑ HDL-c and dietary fiber intake | ↓ IL-10 |
| Jacobs et al. [160] | Intervention group consumed a drink supplemented with 500 mg/day theobromine vs. control group for one month. | Short | Apparently healthy women and men with low baseline HDL-c levels. | Randomized, double-blind, placebo-controlled, cross-over study | Theobromine showed no effect on HDL-c in subjects characterized by low HDL-c and high TG in VLDL. | |
| West et al. [162] | Intervention group consumed 37 g/day of dark chocolate and a sugar-free cocoa beverage vs. control group for one month. | Short | Middle-aged, overweight adults. | Randomized, placebo-controlled, cross-over study | ↑ The basal diameter and peak diameter of the brachial artery by 6% (+2 mm) and basal blood flow volume by 22% | |
| Reference | Study Design | Study Duration | Participants | Type of Study | Findings Plasma Lipids/ Others | |
|---|---|---|---|---|---|---|
| Neto et al. [177] | Experimental group taking whole red grape juice (n = 14) and control group taking a control drink (n = 12) for 28-day period. | Short | 26 individuals with hypertension aged from 40 to 59 years old. | Double-blind, randomized controlled study | Whole red grape juice promotes reduces BP at rest and improves post-exercise hypotension in hypertensive subjects. | |
| Draijer et al. [178] | Placebo group, Grape juice extract alone group and Mixture of grape and wine extract group for four weeks. | Short | 60 males and females mildly hypertensive aged ≥35 and ≤75 years. | Double-blind placebo-controlled crossover study | The intervention with grape juice extract alone had no effect on BP while the polyphenol-rich grape-wine extract lowered SBP and DBP. | |
| Urquiaga et al. [179] | Intervention group taking 20 g/day of wine grape pomace flour (n= 25) and control group (n = 13) for 16 weeks. | Short | 38 males aged from 30 to 65 years old with at least one component of MetS. | Randomized controlled trial | Improvement of BP, glycemia and postprandial insulin. | |
| Pollack et al. [182] | Resveratrol group (2–3 g/day) and placebo group for six weeks. | Short | 30 older glucose-intolerant adults aged 50-80 years old without a prior diagnosis of diabetes | Randomized, double-blind crossover study | No effects on glucose metabolism or insulin sensitivity | Beneficial effects on vascular function |
| Reference | Study Design | Study Duration | Participants | Type of Study | Findings Plasma Lipids/Others |
|---|---|---|---|---|---|
| Khaw et al. [197] | EVCO group (50 g/day, n = 30), EVOO group (50 g/day, n = 33) and unsalted butter group (50 g/day, n = 33) for four weeks. | Short | 94 men and women aged 50–75 years, with no known history of cancer, CVD or diabetes, not on lipid lowering medication and no contra-indications to a high-fat diet. | Randomized clinical trial | EVCO and butter, may have different effects on blood lipid profile compared with EVOO with respect to LDL-c. |
| Lockyer et al. [198] | Liquid OLE supplement group (136 mg oleuropein; 6 mg hydroxytyrosol) and a control polyphenol-free group for six weeks. | Short | 60 pre-hypertensive males aged 24–72 years. | Double-blind, randomized, controlled, crossover trial | OLE intake confers lipid-lowering and hypotensive effects. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lapuente, M.; Estruch, R.; Shahbaz, M.; Casas, R. Relation of Fruits and Vegetables with Major Cardiometabolic Risk Factors, Markers of Oxidation, and Inflammation. Nutrients 2019, 11, 2381. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102381
Lapuente M, Estruch R, Shahbaz M, Casas R. Relation of Fruits and Vegetables with Major Cardiometabolic Risk Factors, Markers of Oxidation, and Inflammation. Nutrients. 2019; 11(10):2381. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102381
Chicago/Turabian StyleLapuente, Maria, Ramon Estruch, Mana Shahbaz, and Rosa Casas. 2019. "Relation of Fruits and Vegetables with Major Cardiometabolic Risk Factors, Markers of Oxidation, and Inflammation" Nutrients 11, no. 10: 2381. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102381