Dietary and Physical Activity Behaviors in Women with Polycystic Ovary Syndrome per the New International Evidence-Based Guideline

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Definition of PCOS
2.3. Study Procedures
2.3.1. Clinical Assessment
2.3.2. Ultrasonographic Assessment
2.3.3. Biochemical Assessment
2.3.4. Dietary Assessment
2.3.5. Physical Activity Assessment
2.4. Statistical Analyses
3. Results
3.1. Demographic, Clinical, and Biochemical Characteristics of Women
3.2. Dietary Behaviors of Women
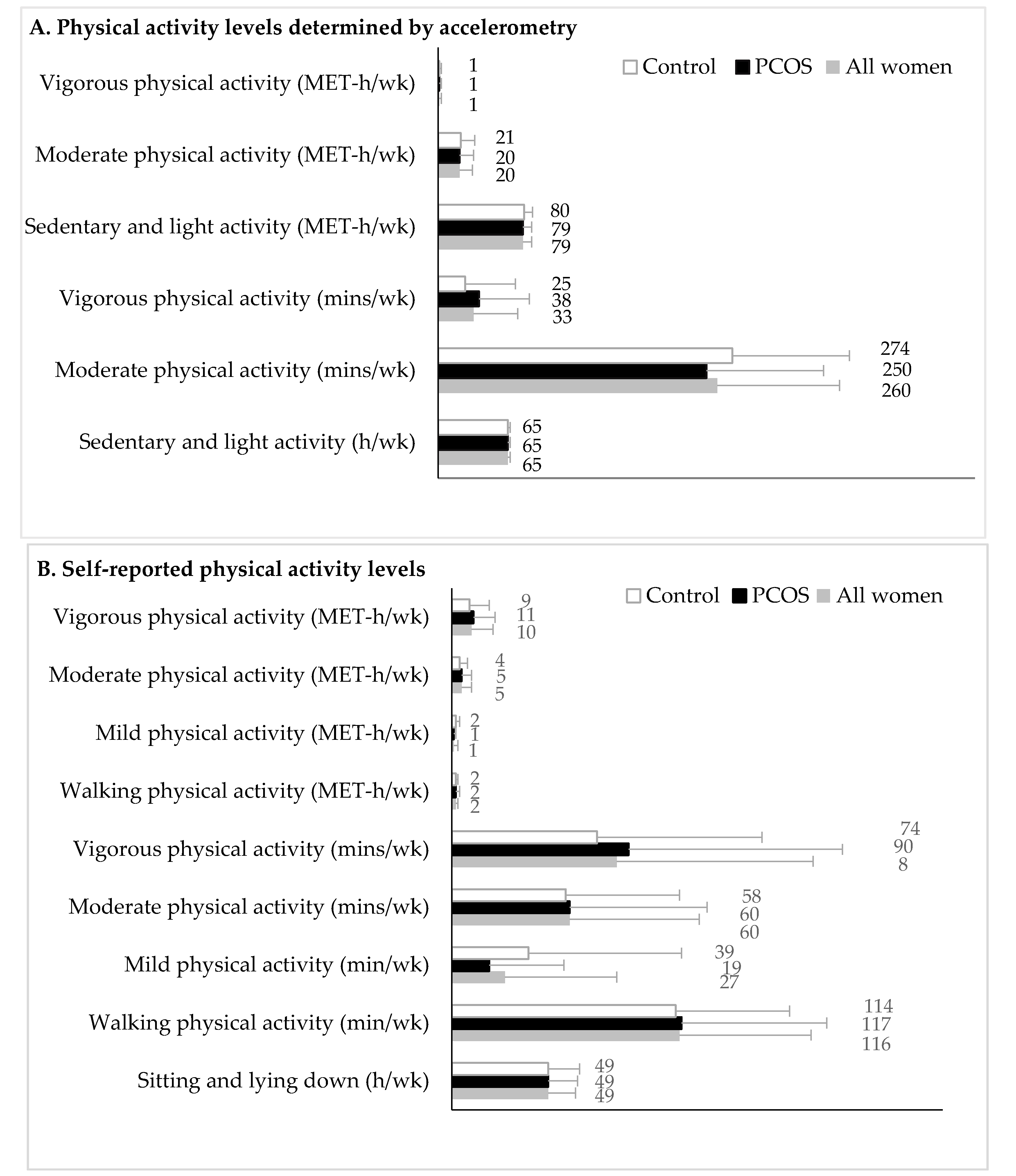
3.3. Physical Activity Behaviors of Women
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum. Reprod. 2018, 33, 1602–1618. [Google Scholar] [CrossRef] [PubMed]
- Chavarro, J.E.; Rich-Edwards, J.W.; Rosner, B.A.; Willett, W.C. A prospective study of dietary carbohydrate quantity and quality in relation to risk of ovulatory infertility. Eur. J. Clin. Nutr. 2007, 63, 78. [Google Scholar] [CrossRef] [PubMed]
- Chavarro, J.E.; Rich-Edwards, J.W.; Rosner, B.A.; Willett, W.C. Dietary fatty acid intakes and the risk of ovulatory infertility. Am. J. Clin. Nutr. 2007, 85, 231–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moran, L.J.; Pasquali, R.; Teede, H.J.; Hoeger, K.M.; Norman, R.J. Treatment of obesity in polycystic ovary syndrome: A position statement of the Androgen Excess and Polycystic Ovary Syndrome Society. Fertil. Steril. 2009, 92, 1966–1982. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, M.; McBreairty, L.E.; Zello, G.A.; Pierson, R.A.; Gordon, J.J.; Serrao, S.B.; Chilibeck, P.D.; Chizen, D.R. A pulse-based diet and the Therapeutic Lifestyle Changes diet in combination with health counseling and exercise improve health-related quality of life in women with polycystic ovary syndrome: Secondary analysis of a randomized controlled trial. J. Psychosom. Obstet. Gynaecol. 2019, 27, 1–10. [Google Scholar] [CrossRef]
- Legro, R.S.; Arslanian, S.A.; Ehrmann, D.A.; Hoeger, K.M.; Murad, M.H.; Pasquali, R.; Welt, C.K. Diagnosis and treatment of polycystic ovary syndrome: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2013, 98, 4565–4592. [Google Scholar] [CrossRef]
- Moran, L.J.; Gibson-Helm, M.; Teede, H.J.; Deeks, A.A. Polycystic ovary syndrome: A biopsychosocial understanding in young women to improve knowledge and treatment options. J. Psychosom. Obstet. Gynaecol. 2010, 31, 24–31. [Google Scholar] [CrossRef]
- Banting, L.K.; Gibson-Helm, M.; Polman, R.; Teede, H.J.; Stepto, N.K. Physical activity and mental health in women with polycystic ovary syndrome. BMC Women Health 2014, 14, 1–9. [Google Scholar] [CrossRef]
- Lin, A.W.; Lujan, M.E. Comparison of dietary intake and physical activity between women with and without polycystic ovary syndrome: A review. Adv. Nutr. 2014, 5, 486–496. [Google Scholar] [CrossRef]
- Barr, S.; Hart, K.; Reeves, S.; Sharp, K.; Jeanes, Y.M. Habitual dietary intake, eating pattern and physical activity of women with polycystic ovary syndrome. Eur. J. Clin. Nutr. 2011, 65, 1126–1132. [Google Scholar] [CrossRef] [Green Version]
- Kazemi, M.; Jarrett, B.; Vanden Brink, H.; Lin, A.; Hoeger, K.; Spandorfer, S.; Lujan, M. Associations between diet quality and ovarian dysmorphology in premenopausal women are mediated by obesity and metabolic aberrations (OR36-03-19). Curr. Dev. Nutr. 2019, 3. [Google Scholar] [CrossRef]
- Ahmadi, A.; Akbarzadeh, M.; Mohammadi, F.; Akbari, M.; Jafari, B.; Tolide-Ie, H.R. Anthropometric characteristics and dietary pattern of women with polycystic ovary syndrome. Indian J. Endocrinol. Metab. 2013, 17, 672–676. [Google Scholar] [CrossRef] [PubMed]
- Graff, S.K.; Mario, F.M.; Alves, B.C.; Spritzer, P.M. Dietary glycemic index is associated with less favorable anthropometric and metabolic profiles in polycystic ovary syndrome women with different phenotypes. Fertil. Steril. 2013, 100, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Moran, L.J.; Ranasinha, S.; Zoungas, S.; McNaughton, S.A.; Brown, W.J.; Teede, H.J. The contribution of diet, physical activity and sedentary behavior to body mass index in women with and without polycystic ovary syndrome. Hum. Reprod. 2013, 28, 2276–2283. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.; Zborowski, J.; Talbott, E.; McHugh-Pemu, K.; Youk, A. Dietary intake, physical activity, and obesity in women with polycystic ovary syndrome. Int. J. Obes. Relat. Metab. Disord. 2004, 28, 1026–1032. [Google Scholar] [CrossRef] [Green Version]
- Tsai, Y.-H.; Wang, T.-W.; Wei, H.-J.; Hsu, C.-Y.; Ho, H.-J.; Chen, W.-H.; Young, R.; Liaw, C.-M.; Chao, J.C.-J. Dietary intake, glucose metabolism and sex hormones in women with polycystic ovary syndrome (PCOS) compared with women with non-PCOS-related infertility. Br. J. Nutr. 2013, 109, 2190–2198. [Google Scholar] [CrossRef]
- Altieri, P.; Cavazza, C.; Pasqui, F.; Morselli, A.M.; Gambineri, A.; Pasquali, R. Dietary habits and their relationship with hormones and metabolism in overweight and obese women with polycystic ovary syndrome. Clin. Endocrinol. (Oxf.) 2013, 78, 52–59. [Google Scholar] [CrossRef]
- Douglas, C.C.; Norris, L.E.; Oster, R.A.; Darnell, B.E.; Azziz, R.; Gower, B.A. Difference in dietary intake between women with polycystic ovary syndrome and healthy controls. Fertil. Steril. 2006, 86, 411–417. [Google Scholar] [CrossRef]
- Álvarez-Blasco, F.; Luque-Ramirez, M.; Escobar-Morreale, H.F. Diet composition and physical activity in overweight and obese premenopausal women with or without polycystic ovary syndrome. Gynecol. Endocrinol. 2011, 27, 978–981. [Google Scholar] [CrossRef]
- Cutler, D.A.; Pride, S.M.; Cheung, A.P. Low intakes of dietary fiber and magnesium are associated with insulin resistance and hyperandrogenism in polycystic ovary syndrome: A cohort study. Food Sci. Nutr. 2019, 7, 1426–1437. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Liu, Y.; Liu, X.; Xu, L.; Zhou, L.; Tang, L.; Zhuang, J.; Guo, W.; Hu, R. High intake of energy and fat in southwest Chinese women with PCOS: A population-based case-control study. PLoS ONE 2015, 10, e0127094. [Google Scholar] [CrossRef] [PubMed]
- Shishehgar, F.; Ramezani Tehrani, F.; Mirmiran, P.; Hajian, S.; Baghestani, A.R.; Moslehi, N. Comparison of dietary intake between polycystic ovary syndrome women and controls. Glob. J. Health Sci. 2016, 8, 54801. [Google Scholar] [CrossRef] [PubMed]
- NIH Evidence Based Methodology Workshop on Polycystic Ovary Syndrome. Executive Summary; December 2012. Available online: https://prevention.nih.gov/sites/default/files/2018-06/FinalReport.pdf (accessed on 10 April 2019).
- Bremner, W.J.; Matsumoto, A.M. Serum testosterone assays—Accuracy matters. J. Clin. Endocrinol. Metab. 2004, 89, 520–524. [Google Scholar] [CrossRef]
- Lujan, M.E.; Brooks, E.D.; Kepley, A.L.; Chizen, D.R.; Pierson, R.A.; Peppin, A.K. Grid analysis improves reliability in follicle counts made by ultrasonography in women with polycystic ovary syndrome. Ultrasound Med. Biol. 2010, 36, 712–718. [Google Scholar] [CrossRef]
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef]
- Patel, S.S.; Truong, U.; King, M.; Ferland, A.; Moreau, K.L.; Dorosz, J.; Hokanson, J.E.; Wang, H.; Kinney, G.L.; Maahs, D.M. Obese adolescents with polycystic ovarian syndrome have elevated cardiovascular disease risk markers. Vasc. Med. 2017, 22, 85–95. [Google Scholar] [CrossRef] [Green Version]
- Broskey, N.T.; Klempel, M.C.; Gilmore, L.A.; Sutton, E.F.; Altazan, A.D.; Burton, J.H.; Ravussin, E.; Redman, L.M. Assessing energy requirements in women with polycystic ovary syndrome: A comparison against doubly labeled water. J. Clin. Endocrinol. Metab. 2017, 102, 1951–1959. [Google Scholar] [CrossRef]
- Mario, F.M.; Graff, S.K.; Spritzer, P.M. Habitual physical activity is associated with improved anthropometric and androgenic profile in PCOS: A cross-sectional study. J. Endocrinol. Investig. 2017, 40, 377–384. [Google Scholar] [CrossRef]
- The Rotterdam ESHRE/ASRM-sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Lujan, M.E.; Jarrett, B.Y.; Brooks, E.D.; Reines, J.K.; Peppin, A.K.; Muhn, N.; Haider, E.; Pierson, R.A.; Chizen, D.R. Updated ultrasound criteria for polycystic ovary syndrome: Reliable thresholds for elevated follicle population and ovarian volume. Hum. Reprod. 2013, 28, 1361–1368. [Google Scholar] [CrossRef]
- Waist Circumference and Waist–Hip Ratio. Report of a WHO Expert Consultation. Geneva, 8–11 December 2008. Available online: https://www.who.int/nutrition/publications/obesity/WHO_report_waistcircumference_and_waisthip_ratio/en/ (accessed on 18 July 2016).
- Balen, A.H.; Laven, J.S.E.; Tan, S.L.; Dewailly, D. Ultrasound assessment of the polycystic ovary: International consensus definitions. Hum. Reprod. Update 2003, 9, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Vanden Brink, H.; Willis, A.D.; Jarrett, B.Y.; Lin, A.W.; Soler, S.; Best, S.; Bender, E.L.; Peppin, A.K.; Hoeger, K.M.; Lujan, M.E. Sonographic markers of ovarian morphology, but not hirsutism indices, predict serum total testosterone in women with regular menstrual cycles. Fertil. Steril. 2016, 105, 1322–1329. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.F.; Marcellus, S.; deLory, B.; Bird, C.E. Plasma testosterone free index: A better indicator of plasma androgen activity? Fertil. Steril. 1975, 26, 1001–1005. [Google Scholar] [CrossRef]
- VioScreen™. VIOCARE®® Website. Available online: https://www.viocare.com/vioscreen.html (accessed on 25 December 2018).
- Kristal, A.R.; Kolar, A.S.; Fisher, J.L.; Plascak, J.J.; Stumbo, P.J.; Weiss, R.; Paskett, E.D. Evaluation of web-based, self-administered, graphical food frequency questionnaire. J. Acad. Nutr. Diet. 2014, 114, 613–621. [Google Scholar] [CrossRef]
- Deierlein, A.L.; Bihuniak, J.D.; Nagi, E.; Litvak, J.; Victoria, C.; Braune, T.; Weiss, R.; Parekh, N. Development of a technology-assisted food frequency questionnaire for elementary and middle school children: Findings from a pilot study. Nutrients 2019, 11, 1103. [Google Scholar] [CrossRef]
- 2015–2020 Dietary Guidelines for Americans, 8th ed.; Office of Disease Prevention and Health Promotion Website, Skyhorse Publishing Inc: Washington, DC, USA, 2015; Available online: http://health.gov/dietaryguidelines/2015 (accessed on 25 January 2019).
- Population Ratio Method. Epidemiology and Genomics Research Program. National Cancer Institute. Division of Cancer Control and Population Sciences. Available online: https://epi.grants.cancer.gov/hei/population-ratio-method.html (accessed on 20 August 2019).
- Panizza, C.E.; Shvetsov, Y.B.; Harmon, B.E.; Wilkens, L.R.; Le Marchand, L.; Haiman, C.; Reedy, J.; Boushey, C.J. Testing the predictive validity of the Healthy Eating Index-2015 in the multiethnic cohort: Is the score associated with a reduced risk of all-cause and cause-specific mortality? Nutrients 2018, 10, 452. [Google Scholar] [CrossRef]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the healthy eating index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef]
- Reedy, J.; Lerman, J.L.; Krebs-Smith, S.M.; Kirkpatrick, S.I.; Pannucci, T.E.; Wilson, M.M.; Subar, A.F.; Kahle, L.L.; Tooze, J.A. Evaluation of the Healthy Eating Index-2015. J. Acad. Nutr. Diet. 2018, 118, 1622–1633. [Google Scholar] [CrossRef]
- Matthews, C.E.; Ainsworth, B.E.; Thompson, R.W.; Bassett, D.R., Jr. Sources of variance in daily physical activity levels as measured by an accelerometer. Med. Sci. Sports Exerc. 2002, 34, 1376–1381. [Google Scholar] [CrossRef]
- Sasaki, J.E.; John, D.; Freedson, P.S. Validation and comparison of ActiGraph activity monitors. J. Sci. Med. Sport 2011, 14, 411–416. [Google Scholar] [CrossRef]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.-M.; Evenson, K.R.; Morimoto, L.; Siscovick, D.; White, E. Test-retest reliability of the Women’s Health Initiative physical activity questionnaire. Med. Sci. Sports Exerc. 2009, 41, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R.; Schmitz, K.H.; Emplaincourt, P.O. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B (Methodol.) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Kazemi, M.; McBreairty, L.E.; Chizen, D.R.; Pierson, R.A.; Chilibeck, P.D.; Zello, G.A. A comparison of a pulse-based diet and the Therapeutic Lifestyle Changes diet in combination with exercise and health counselling on the cardio-metabolic risk profile in women with polycystic ovary syndrome: A randomized controlled trial. Nutrients 2018, 10, 1387. [Google Scholar] [CrossRef]
- Wild, R.A.; Carmina, E.; Diamanti-Kandarakis, E.; Dokras, A.; Escobar-Morreale, H.F.; Futterweit, W.; Lobo, R.; Norman, R.J.; Talbott, E.; Dumesic, D.A. Assessment of cardiovascular risk and prevention of cardiovascular disease in women with the polycystic ovary syndrome: A consensus statement by the Androgen Excess and Polycystic Ovary Syndrome (AE-PCOS) Society. J. Clin. Endocrinol. Metab. 2010, 95, 2038–2049. [Google Scholar] [CrossRef]
- Kazemi, M.; Pierson, R.A.; Lujan, M.E.; Chilibeck, P.D.; McBreairty, L.E.; Gordon, J.J.; Serrao, S.B.; Zello, G.A.; Chizen, D.R. Comprehensive evaluation of type 2 diabetes and cardiovascular disease risk profiles in reproductive-age women with polycystic ovary syndrome: A large Canadian cohort. J. Obstet. Gynecol. Can. 2019, 41, 1453–1460. [Google Scholar] [CrossRef]
- He, C.; Lin, Z.; Robb, S.W.; Ezeamama, A.E. Serum vitamin D levels and polycystic ovary syndrome: A systematic review and meta-analysis. Nutrients 2015, 7, 4555–4577. [Google Scholar] [CrossRef]
- Balen, A.H.; Conway, G.; Homburg, R.; Legro, R. Polycystic Ovary Syndrome: A Guide to Clinical Management; Taylor & Francis: London, UK, 2005. [Google Scholar]
- Dunaif, A. Insulin resistance and the polycystic ovary syndrome: Mechanism and implications for pathogenesis. Endocr. Rev. 1997, 18, 774–800. [Google Scholar] [CrossRef]
- Yildiz, B.O.; Knochenhauer, E.S.; Azziz, R. Impact of obesity on the risk for polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2008, 93, 162–168. [Google Scholar] [CrossRef]
- Hahn, S.; Haselhorst, U.; Tan, S.; Quadbeck, B.; Schmidt, M.; Roesler, S.; Kimmig, R.; Mann, K.; Janssen, O. Low serum 25-hydroxyvitamin D concentrations are associated with insulin resistance and obesity in women with polycystic ovary syndrome. Exp. Clin. Endocrinol. Diabetes 2006, 114, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Li, H.W.; Brereton, R.E.; Anderson, R.A.; Wallace, A.M.; Ho, C.K. Vitamin D deficiency is common and associated with metabolic risk factors in patients with polycystic ovary syndrome. Metabolism 2011, 60, 1475–1481. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, K.; Hurukawa, Y.; Okuyama, M.; Kikuchi, M.; Yoshinaga, K. Glucose tolerance and insulin secretion in patients with parathyroid disorders: Effect of serum calcium on insulin release. N. Engl. J. Med. 1975, 292, 501–504. [Google Scholar] [CrossRef] [PubMed]
- Daval, J.L.; Guéant, J.L.; Alberto, J.M.; Guéant-Rodriguez, R.M.; Monnier-Barbarino, P.; Forges, T. Impact of folate and homocysteine metabolism on human reproductive health. Hum. Reprod. Update 2007, 13, 225–238. [Google Scholar] [CrossRef]
- Otten, J.J.; Hellwig, J.P.; Meyers, L.D. DRI, Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; National Academies Press: Washington, DC, USA, 2006; pp. 1–1344. ISBN 978-030-915-742-1. [Google Scholar] [CrossRef]
- Nutrient Recommendations: Dietary Reference Intakes (DRI). National Institue of Health. Office of Dietary Supplements Website. Available online: https://ods.od.nih.gov/Health_Information/Dietary_Reference_Intakes.aspx (accessed on 2 April 2019).
- Reilly, J.J.; Penpraze, V.; Hislop, J.; Davies, G.; Grant, S.; Paton, J.Y. Objective measurement of physical activity and sedentary behaviour: Review with new data. Arch. Dis. Child. 2008, 93, 614–619. [Google Scholar] [CrossRef]
- Dowd, K.P.; Szeklicki, R.; Minetto, M.A.; Murphy, M.H.; Polito, A.; Ghigo, E.; van der Ploeg, H.; Ekelund, U.; Maciaszek, J.; Stemplewski, R.; et al. A systematic literature review of reviews on techniques for physical activity measurement in adults: A DEDIPAC study. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 15. [Google Scholar] [CrossRef]
- Lujan, M.E.; Chizen, D.R.; Peppin, A.K.; Kriegler, S.; Leswick, D.A.; Bloski, T.G.; Pierson, R.A. Improving inter-observer variability in the evaluation of ultrasonographic features of polycystic ovaries. Reprod. Biol. Endocrinol. 2008, 6, 30. [Google Scholar] [CrossRef]
- Thompson, F.E.; Kirkpatrick, S.I.; Subar, A.F.; Reedy, J.; Schap, T.E.; Wilson, M.M.; Krebs-Smith, S.M. The national cancer institute’s dietary assessment primer: A resource for diet research. J. Acad. Nutr. Diet. 2015, 115, 1986–1995. [Google Scholar] [CrossRef]
- McCarney, R.; Warner, J.; Iliffe, S.; van Haselen, R.; Griffin, M.; Fisher, P. The Hawthorne Effect: A randomised, controlled trial. BMC Med. Res. Methodol. 2007, 7, 30. [Google Scholar] [CrossRef]
- Shim, J.-S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef]
- Moran, L.; Grieger, J.; Mishra, G.; Teede, H. The association of a Mediterranean-style diet pattern with polycystic ovary syndrome status in a community cohort study. Nutrients 2015, 7, 8553–8564. [Google Scholar] [CrossRef]
- Cosar, E.; Köken, G.; Sahin, F.K.; Akgün, L.; Üçok, K.; Genç, A.; Yilmazer, M. Resting metabolic rate and exercise capacity in women with polycystic ovary syndrome. Int. J. Gynaecol. Obstet. 2008, 101, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Romualdi, D.; Versace, V.; Tagliaferri, V.; De Cicco, S.; Immediata, V.; Apa, R.; Guido, M.; Lanzone, A. The resting metabolic rate in women with polycystic ovary syndrome and its relation to the hormonal milieu, insulin metabolism, and body fat distribution: A cohort study. J. Endocrinol. Investig. 2019. [Google Scholar] [CrossRef] [PubMed]
- Georgopoulos, N.A.; Saltamavros, A.D.; Vervita, V.; Karkoulias, K.; Adonakis, G.; Decavalas, G.; Kourounis, G.; Markou, K.B.; Kyriazopoulou, V. Basal metabolic rate is decreased in women with polycystic ovary syndrome and biochemical hyperandrogenemia and is associated with insulin resistance. Fertil. Steril. 2009, 92, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Bhasin, G.; Wang, E.T.; Alexander, C.J.; Pal, M.; Azziz, R.; Pisarska, M.D. Women with polycystic ovary syndrome (PCOS) have lower basal metabolic rates compared to eumenorrheic controls. Fertil. Steril. 2013, 100, S38–S39. [Google Scholar] [CrossRef]
- Jarrett, B.Y.; Lin, A.W.; Lujan, M.E. A commentary on the new evidence-based lifestyle recommendations for patients with polycystic ovary syndrome and potential barriers to their implementation in the United States. J. Acad. Nutr. Diet. 2019, 119, 205–210. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Measure (unit) | All Women a | PCOS a | Control a | Reference | p-Value |
|---|---|---|---|---|---|
| Age (year) | 27.7 (26.6–28.8) | 26.8 (25.4–28.1) | 29.5 (27.5–31.4) | N/A | 0.02 |
| Ethnicity, Hispanic (n (%)) | 18 (14.5) | 9 (11.3) | 9 (20.5) | N/A | 0.10 |
| Race (n (%)) | N/A | 0.15 | |||
| Black | 15 (12) | 8 (10) | 7 (16) | ||
| Asian | 11 (9) | 7 (9) | 4 (9) | ||
| White | 77 (62) | 55 (69) | 22 (50) | ||
| Other | 21 (17) | 10 (12) | 11 (25) | ||
| Metformin use (n (yes %)) | 1 (1) | 1 (1) | 0 (0) | N/A | 1.00 |
| OCP use (n (yes %)) | 7 (6) | 4 (5) | 3 (7) | N/A | 0.70 |
| BMI (kg/m2) | 30.2 (28.8–31.6) | 31.5 (29.5–33.4) | 28.0 (26.1–29.8) | 18.5–24.9 | 0.01 |
| Normal BMI (n (yes %)) | 42 (33.9) | 24 (30.0) | 18 (40.0) | 18.5–24.9 | |
| Overweight (n (yes %)) | 20 (16.1) | 11 (13.8) | 9 (20.4) | 25.0–29.9 | 0.19 |
| Obese (n (yes %)) | 62 (50.0) | 45 (56.2) | 17 (38.6) | ≥30.0 | |
| WHR | 0.84 (0.82–0.85) | 0.83 (0.81–0.85) | 0.84 (0.83–0.86) | ≤0.85 | 0.49 |
| Menstrual cycle length (d) | 64 (49–78) | 86 (63–108) | 29.5 (26.7–32.3) | <36 | 0.001 |
| Modified hirsutism score | 6 (5–7) | 8 (6–9) | 4 (3–5) | <6 | <0.0001 |
| TT (nmol/L) | 1.6 (1.4–1.7) | 1.8 (1.6–1.9) | 1.2 (1.1–1.4) | <2.1 | <0.0001 |
| FAI | 4 (4–5) | 6 (6–6) | 2 (2–3) | <6 | 0.001 |
| Free T (nmol/L) | 0.02 (0.02–0.03) | 0.03 (0.03–0.03) | 0.02 (0.01–0.02) | <0.03 | <0.0001 |
| Bioavailable T (nmol/L) | 0.6 (0.5–0.6) | 0.7 (0.6–0.8) | 0.4 (0.3–0.4) | <0.7 | <0.0001 |
| OV (mL) | 9.9 (8.9–10.9) | 11.0 (9.7–12.2) | 7.8 (6.3–9.4) | <10 | <0.004 |
| FNPS (n) | 9 (8–10) | 10 (9–11) | 7 (6–8) | <10 | <0.005 |
| FNPO 2–9 mm (n) | 36 (32–40) | 42 (36–47) | 24 (20–28) | <20 | <0.0001 |
| Measure (unit) | All Women a | PCOS a | Control a | Reference | p-Value |
|---|---|---|---|---|---|
| Dietary factors b | |||||
| Energy (kcal/d) | 2204 (2036–2373) | 2218 (2017–2419) | 2180 (1866–2494) | 2403 c | 0.64 |
| Total carbohydrate (g/d) | 267 (245–290) | 264 (240–288) | 273 (225–321) | 100 d | 0.70 |
| Added sugars (g/d) | 70 (59–82) | 68 (56–80) | 75 (52–99) | N/A | 0.64 |
| Total protein (g/d) | 85 (79–92) | 86 (78–95) | 83 (72–94) | 46 e | 0.60 |
| Total fat (g/d) | 87 (80–94) | 89 (80–99) | 83 (72–94) | N/A | 0.42 |
| Total SFA (g/d) | 28 (26–31) | 29 (25–32) | 28 (23–33) | N/A | 0.77 |
| Total MUFA (g/d) | 34 (33–37) | 35 (31–39) | 32 (28–36) | N/A | 0.40 |
| Total PUFA (g/d) | 18 (16–19) | 18 (16–20) | 17 (15–19) | N/A | 0.37 |
| Cholesterol (mg/d) | 291 (262–321) | 303 (264–342) | 271 (229–314) | N/A | 0.34 |
| Trans fats (g/d) | 3 (3–3) | 3 (3–4) | 3 (2–3) | N/A | 0.94 |
| Total fiber (g/d) | 23 (22–26) | 24 (22–26) | 25 (22–28) | 28 f | 0.49 |
| Vitamin A (IU/d) | 14511 (12634–16388) | 13933 (117167–16150) | 15561 (12029–19094) | 500 d | 0.60 |
| Vitamin B1 (mg/d) | 1.8 (1.7–1.9) | 1.8 (1.7–2.0) | 1.8 (1.5–2.0) | 0.9 d | 0.46 |
| Vitamin B2 (mg/d) | 2.4 (2.2–2.6) | 2.4 (2.2–2.6) | 2.3 (2.0–2.7) | 0.9 d | 0.27 |
| Vitamin B3 (mg/d) | 24 (22–25) | 24 (22–26) | 22 (19–25) | 11 d | 0.15 |
| Vitamin B5 (mg/d) | 7 (6–7) | 7 (6–7) | 7 (6–8) | 5 h | 0.37 |
| Vitamin B6 (mg/d) | 2.2 (2.0–2.3) | 2.2 (2.1–2.4) | 2.1 (1.8–2.3) | 1.1 d | 0.28 |
| Vitamin B9 (μg/d) | 285 (265–305) | 275 (252–298) | 303 (265–340) | 320 d | 0.38 |
| Vitamin B12 (μg/d) | 5.7 (5.1–6.3) | 5.9 (5.2–6.6) | 5.3 (4.3–6.3) | 2.0 d | 0.17 |
| Vitamin C (mg/d) | 141 (125–157) | 136 (118–154) | 151 (120–181) | 60 d | 0.55 |
| Vitamin D (μg/d) | 6 (5–7) | 6 (5–7) | 6 (4–7) | 10 d | 0.48 |
| Vitamin E (mg/d) | 21 (19–22) | 21 (19–23) | 20 (17–23) | 12 d | 0.60 |
| Vitamin K (μ/d) | 219 (190–251) | 197 (166–228) | 259 (188–331) | 90 h | 0.11 |
| Calcium (mg/d) | 1141 (1033–1250) | 1117 (997–1236) | 1187 (967–1407) | 800 d | 0.89 |
| Copper (μg/d) | 1536 (1441–1630) | 1516 (1407–1624) | 1572 (1387–1758) | 700 d | 0.57 |
| Iron (mg/d) | 16 (15–18) | 17 (15–18) | 16 (14–18) | 8.1 d | 0.54 |
| Magnesium (mg/d) | 363 (340–386) | 357 (331–383) | 375 (330–420) | 255–265 d | 0.46 |
| Manganese (mg/d) | 4.5 (4.1–5.0) | 4.3 (3.9–4.6) | 5.0 (4.0–6.0) | 1.8 g | 0.27 |
| Phosphorus (mg/d) | 1439 (1130–1548) | 1445 (1311–1580) | 1427 (1235–1618) | 580 e | 0.87 |
| Potassium (g/d) | 3.2 (3.0–3.5) | 3.2 (2.9–3.5) | 3.3 (2.8–3.8) | 2.6 g | 0.68 |
| Selenium (μg/d) | 123 (114–133) | 126 (114–138) | 118 (103–134) | 45 d | 0.45 |
| Sodium (g/d) | 4.0 (3.7–4.3) | 4.0 (3.6–4.4) | 4.1 (3.5–4.7) | 2.3 h | 0.75 |
| Zinc (mg/d) | 13 (12–14) | 13 (11–14) | 13 (11–14) | 6.8 d | 0.44 |
| Caffeine (mg/d) | 165 (138–192) | 151 (123–180) | 191 (135–247) | N/A | 0.46 |
| Alcohol (g/d) | 9 (7–11) | 9 (5–12) | 9 (5–13) | N/A | 0.58 |
| HEI-2015 components b | Maximum points i | ||||
| Total fruits | 3.6 (3.3–3.9) | 3.5 (3.1–3.9) | 3.7 (3.2–4.2) | 5 | 0.59 |
| Whole fruits | 3.9 (3.6–4.2) | 3.9 (3.5–4.2) | 3.9 (3.4–4.4) | 5 | 0.98 |
| Total vegetables | 4.2 (4.0–4.4) | 4.2 (3.9–4.4) | 4.3 (4–4.6) | 5 | 0.67 |
| Greens and beans | 3.8 (3.5–4.0) | 3.7 (3.3–4.1) | 3.9 (3.4–4.4) | 5 | 0.51 |
| Whole grains | 4.9 (4.3–5.3) | 4.0 (5.3–4.6) | 5.2 (4.3–6.1) | 10 | 0.31 |
| Dairy | 6.2 (5.7–6.6) | 6.1 (5.5–6.7) | 6.4 (5.6–7.2) | 10 | 0.55 |
| Total protein foods | 4.6 (4.4–4.7) | 4.5 (4.3–4.7) | 4.6 (4.4–4.9) | 5 | 0.40 |
| Seafood and plant proteins | 4.3 (4.0–4.5) | 4.1 (3.8–4.4) | 4.5 (4.2–4.8) | 5 | 0.12 |
| Fatty acids | 5.3 (4.8–5.9) | 5.5 (4.8–6.3) | 4.9 (4.1–5.8) | 10 | 0.39 |
| Refined grains | 8.3 (7.9–8.7) | 8.3 (7.6–8.8) | 8.3 (7.6–9.1) | 10 | 0.49 |
| Sodium | 2.9 (2.4–3.3) | 3.0 (2.4–3.5) | 2.7 (2.0–3.5) | 10 | 0.49 |
| Added sugars | 8.3 (7.9–8.7) | 8.4 (7.9–8.8) | 8.2 (7.5–8.7) | 10 | 0.74 |
| Saturated fats | 5.9 (5.4–6.4) | 5.9 (5.2–6.6) | 5.8 (5.0–6.6) | 10 | 0.86 |
| Total HEI-2015 score | 65.9 (63.7–68.1) | 65.6 (62.6–68.6) | 66.5 (63.5–69.6) | 100 i | 0.70 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, A.W.; Kazemi, M.; Jarrett, B.Y.; Vanden Brink, H.; Hoeger, K.M.; Spandorfer, S.D.; Lujan, M.E. Dietary and Physical Activity Behaviors in Women with Polycystic Ovary Syndrome per the New International Evidence-Based Guideline. Nutrients 2019, 11, 2711. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112711
Lin AW, Kazemi M, Jarrett BY, Vanden Brink H, Hoeger KM, Spandorfer SD, Lujan ME. Dietary and Physical Activity Behaviors in Women with Polycystic Ovary Syndrome per the New International Evidence-Based Guideline. Nutrients. 2019; 11(11):2711. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112711
Chicago/Turabian StyleLin, Annie W., Maryam Kazemi, Brittany Y. Jarrett, Heidi Vanden Brink, Kathleen M. Hoeger, Steven D. Spandorfer, and Marla E. Lujan. 2019. "Dietary and Physical Activity Behaviors in Women with Polycystic Ovary Syndrome per the New International Evidence-Based Guideline" Nutrients 11, no. 11: 2711. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112711