Dietary Patterns and the Double Burden of Malnutrition in Mexican Adolescents: Results from ENSANUT-2006

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
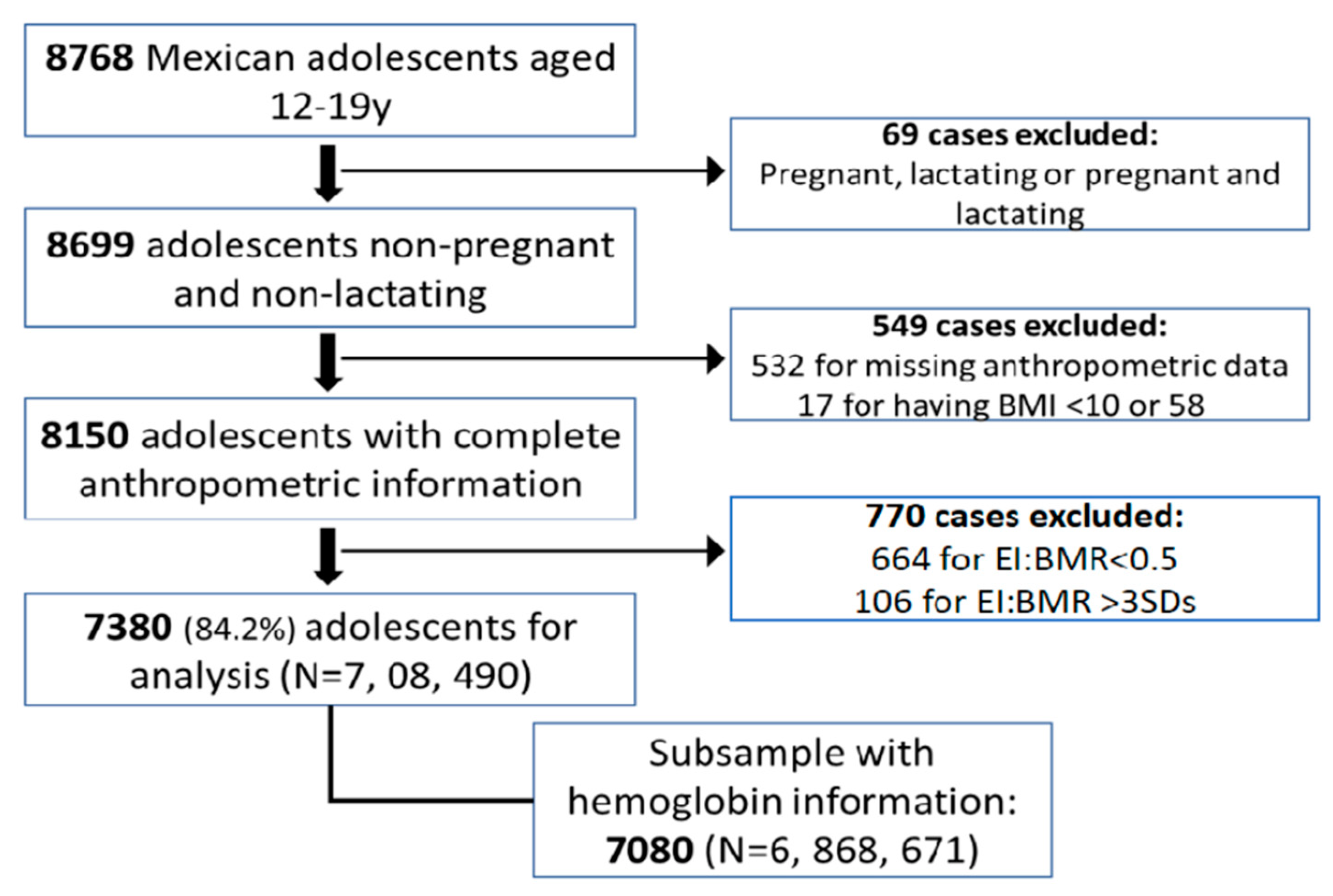
2.1. Study Design and Study Population
2.2. Population Characteristics
2.3. Dietary Data
2.4. Statistical Analysis
3. Results
3.1. Dietary Patterns
3.2. Association of Dietary Patterns with Overweight and Obesity
3.3. Association of Dietary Patterns with Anemia
3.4. Association of Dietary Patterns with Stunting
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Das, J.K.; Salam, R.A.; Thornburg, K.L.; Prentice, A.M.; Campisi, S.; Lassi, Z.S.; Koletzko, B.; Bhutta, Z.A. Nutrition in adolescents, physiology, metabolism, and nutritional needs. Ann. N. Y. Acad. Sci. 2017, 1393, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, S.M.; Afifi, R.A.; Bearinger, L.H.; Blakemore, S.J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence, a foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Cutler, G.J.; Flood, A.; Hannan, P.; Neumark-Sztainer, D. Multiple sociodemographic and socioenvironmental characteristics are correlated with major patterns of dietary intake in adolescents. J. Am. Diet. Assoc. 2011, 111, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood, systematic review. Int. J. Obes. 2011, 35, 891–898. [Google Scholar] [CrossRef] [PubMed]
- Hauta-Alus, H.H.; Korkalo, L.; Freese, R.; Ismael, C.; Mutanen, M. Urban and rural dietary patterns are associated with anthropometric and biochemical indicators of nutritional status of adolescent Mozambican girls. Public Health Nutr. 2017, 21, 1057–1064. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, H.; Wang, Y.; Xue, H.; Wang, Z.; Du, W.; Su, C.; Zhang, J.; Jiang, H.; Zhai, F.; et al. Dietary patterns and their associations with childhood obesity in China. Br. J. Nutr. 2015, 113, 1978–1984. [Google Scholar] [CrossRef]
- Perng, W.; Fernandez, C.; Peterson, K.E.; Zhang, Z.; Cantoral, A.; Sanchez, B.N.; Solano-Gonzalez, M.; Tellez-Rojo, M.M.; Baylin, A. Dietary Patterns Exhibit Sex-Specific Associations with Adiposity and Metabolic Risk in a Cross-Sectional Study in Urban Mexican Adolescents. J. Nutr. 2017, 147, 1977–1985. [Google Scholar] [CrossRef]
- Khalid, S.; Williams, C.M.; Reynolds, S.A. Is there an association between diet and depression in children and adolescents? A systematic review. Br. J. Nutr. 2016, 116, 2097–2108. [Google Scholar] [CrossRef]
- Kim, T.H.; Choi, J.Y.; Lee, H.H.; Park, Y. Associations between Dietary Pattern and Depression in Korean Adolescent Girls. J. Pediatr. Adolesc. Gynecol. 2015, 28, 533–537. [Google Scholar] [CrossRef]
- Double Burden of Malnutrition. Available online: https://www.who.int/nutrition/double-burden-malnutrition/en/ (accessed on 3 November 2019).
- De la Cruz-Gongora, V.; Gaona, B.; Villalpando, S.; Shamah-Levy, T.; Robledo, R. Anemia and iron, zinc, copper and magnesium deficiency in Mexican adolescents, National Health and Nutrition Survey 2006. Salud Publica Mex. 2012, 54, 135–145. [Google Scholar] [CrossRef]
- De la Cruz-Gongora, V.; Villalpando, S.; Shamah-Levy, T. Prevalence of anemia and consumption of iron-rich food groups in Mexican children and adolescents, Ensanut MC 2016. Salud Publica Mex. 2018, 60, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Cordero, S.; Cuevas-Nasu, L.; Morales-Ruan, M.C.; Humaran, I.M.; Avila-Arcos, M.A.; Rivera-Dommarco, J.A. Overweight and obesity in Mexican children and adolescents during the last 25 years. Nutr. Diabetes 2017, 7, e280. [Google Scholar] [CrossRef] [PubMed]
- Cardenas-Villareal, V.M.; Lopez Alvarenga, J.C.; Bastarrachea, R.A.; Rizo-Baeza, M.M.; Cortes-Castell, E. Metabolic syndrome prevalence in teenagers of Monterrey, Nuevo Leon. Arch. Cardiol. Mex. 2010, 80, 19–26. [Google Scholar] [PubMed]
- Cardoso-Saldana, G.C.; Yamamoto-Kimura, L.; Medina-Urrutia, A.; Posadas-Sanchez, R.; Caracas-Portilla, N.A.; Posadas-Romero, C. Obesity or overweight and metabolic syndrome in Mexico City teenagers. Arch. Cardiol. Mex. 2010, 80, 12–18. [Google Scholar]
- Castro-Quezada, I.; Angulo-Estrada, S.; Sanchez-Villegas, A.; Ruiz-López, M.D.; Artacho, R.; Serra-Majem, L.; Shamah-Levy, T. Glycemic index, glycemic load, and metabolic syndrome in Mexican adolescents, a cross-sectional study from the NHNS-2012. BMC Nutr. 2017, 3, 44. [Google Scholar] [CrossRef]
- Rodriguez-Ramirez, S.; Mundo Rosas, V.; Shamah-Levy, T.; Ponce-Martínez, X.; Jiménez-Aguilar, A.; Cosio, T. Ingesta de energía y nutrimentos en adolescentes mexicanos, análisis de la Encuesta Nacional de Salud y Nutrición 2006. Salud Pública Méx. 2008, 51, S551–S561. [Google Scholar]
- Gaona-Pineda, E.B.; Mejía-Rodríguez, F.; Cuevas-Nasu, L.; Gómez-Acosta, L.M.; Rangel-Baltazar, E.; Flores-Aldana, M.E. Dietary intake and adequacy of energy and nutrients in Mexican adolescents: Results from Ensanut 2012. Salud Pública Méx. 2018, 60, 404–413. [Google Scholar] [CrossRef]
- Allès, B.; Samieri, C.; Féart, C.; Jutand, M.A.; Laurin, D.; Barberger-Gateau, P. Dietary patterns: A novel approach to examine the link between nutrition and cognitive function in older individuals. Nutr. Res. Rev. 2012, 25, 207–222. [Google Scholar] [CrossRef]
- Palma, O.; Shamah, T.; Franco, A.; Olaiz, G.; Mendez, I.; Metodología. Encuesta Nacional de Salud y Nutrición 2006. Salud Publica Mex. 2006, 51, S523–S529. [Google Scholar]
- Ramirez-Silva, I.; Jimenez-Aguilar, A.; Valenzuela-Bravo, D.; Martinez-Tapia, B.; Rodriguez-Ramirez, S.; Gaona-Pineda, E.B.; Angulo-Estrada, S.; Shamah-Levy, T. Methodology for estimating dietary data from the semi-quantitative food frequency questionnaire of the Mexican National Health and Nutrition Survey 2012. Salud Publica Mex. 2016, 58, 629–638. [Google Scholar] [CrossRef]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake, basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [PubMed]
- Romero-Martínez, M.; Shamah-Levy, T.; Franco-Núñez, A.; Villalpando, S.; Cuevas-Nasu, L.; Gutiérrez, J.P.; Rivera-Dommarco, J.Á. Encuesta Nacional de Salud y Nutrición 2012, diseño y cobertura. Salud Publica Mex. 2013, 55, S332–S340. [Google Scholar] [CrossRef] [PubMed]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Haemoglobin Concentrations for the Diagnosis of Anaemia and assessment of Severity. Available online: http://www.who.int/vmnis/indicators/haemoglobin.pdf (accessed on 6 June 2019).
- Hernandez-Avila, M.; Romieu, I.; Parra, S.; Hernandez-Avila, J.; Madrigal, H.; Willett, W. Validity and reproducibility of a food frequency questionnaire to assess dietary intake of women living in Mexico City. Salud Publica Mex. 1998, 40, 133–140. [Google Scholar] [CrossRef]
- Barros, A.J.; Hirakata, V.N. Alternatives for logistic regression in cross-sectional studies, an empirical comparison of models that directly estimate the prevalence ratio. BMC Med. Res. Methodol. 2003, 3, 21. [Google Scholar] [CrossRef]
- Cepeda-Lopez, A.C.; Osendarp, S.J.; Melse-Boonstra, A.; Aeberli, I.; Gonzalez-Salazar, F.; Feskens, E.; Villalpando, S.; Zimmermann, M.B. Sharply higher rates of iron deficiency in obese Mexican women and children are predicted by obesity-related inflammation rather than by differences in dietary iron intake. Am. J. Clin. Nutr. 2011, 93, 975–983. [Google Scholar] [CrossRef]
- Afeiche, M.C.; Taillie, L.S.; Hopkins, S.; Eldridge, A.L.; Popkin, B.M. Breakfast Dietary Patterns among Mexican Children Are Related to Total-Day Diet Quality. J. Nutr. 2017, 147, 404–412. [Google Scholar] [CrossRef]
- Kroker-Lobos, M.F.; Pedroza-Tobias, A.; Pedraza, L.S.; Rivera, J.A. The double burden of undernutrition and excess body weight in Mexico. Am. J. Clin. Nutr. 2014, 100, 1652s–1658s. [Google Scholar] [CrossRef]
- Jones, A.D.; Mundo-Rosas, V.; Cantoral, A.; Levy, T.S. Household food insecurity in Mexico is associated with the co-occurrence of overweight and anemia among women of reproductive age, but not female adolescents. Matern. Child Nutr. 2017, 13, e12396. [Google Scholar] [CrossRef]
- Romieu, I.; Dossus, L.; Barquera, S.; Blottiere, H.M.; Franks, P.W.; Gunter, M.; Hwalla, N.; Hursting, S.D.; Leitzmann, M.; Margetts, B.; et al. Energy balance and obesity, what are the main drivers? Cancer Causes Control 2017, 28, 247–258. [Google Scholar] [CrossRef]
- Johnson, L.; Mander, A.P.; Jones, L.R.; Emmett, P.M.; Jebb, S.A. Energy-dense, low-fiber, high-fat dietary pattern is associated with increased fatness in childhood. Am. J. Clin. Nutr. 2008, 87, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Fidler Mis, N.; Braegger, C.; Bronsky, J.; Campoy, C.; Domellof, M.; Embleton, N.D.; Hojsak, I.; Hulst, J.; Indrio, F.; Lapillonne, A.; et al. Sugar in Infants, Children and Adolescents, A Position Paper of the European Society for Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 681–696. [Google Scholar] [CrossRef] [PubMed]
- Caamano, M.C.; Gutierrez, J.; Garcia, O.P.; Ronquillo, D.; Martinez, G.; Rosado, J.L. Increased calorie intake at a specific mid-morning meal and increased intake of soft drinks are strongly associated with obesity in Mexican rural women. Ecol. Food Nutr. 2015, 54, 157–174. [Google Scholar] [CrossRef] [PubMed]
- Naja, F.; Hwalla, N.; Itani, L.; Karam, S.; Sibai, A.M.; Nasreddine, L. A Western dietary pattern is associated with overweight and obesity in a national sample of Lebanese adolescents (13–19 years), a cross-sectional study. Br. J. Nutr. 2015, 114, 1909–1919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Y.; Park, M.J.; Paik, H.Y.; Joung, H. Secular trends in dietary patterns and obesity-related risk factors in Korean adolescents aged 10–19 years. Int. J. Obes. 2010, 34, 48–56. [Google Scholar] [CrossRef] [Green Version]
- Gutierrez-Pliego, L.E.; Camarillo-Romero Edel, S.; Montenegro-Morales, L.P.; Garduno-Garcia Jde, J. Dietary patterns associated with body mass index [BMI] and lifestyle in Mexican adolescents. BMC Public Health 2016, 16, 850. [Google Scholar] [CrossRef] [Green Version]
- Mendonca, R.D.; Pimenta, A.M.; Gea, A.; de la Fuente-Arrillaga, C.; Martinez-Gonzalez, M.A.; Lopes, A.C.; Bes-Rastrollo, M. Ultraprocessed food consumption and risk of overweight and obesity, the University of Navarra Follow-Up [SUN] cohort study. Am. J. Clin. Nutr. 2016, 104, 1433–1440. [Google Scholar] [CrossRef]
- Adolescent Health Epidemiology. Available online: https,//www.who.int/maternal_child_adolescent/epidemiology/adolescence/en/ (accessed on 6 June 2019).
- Azzopardi, P.S.; Hearps, S.J.C.; Francis, K.L.; Kennedy, E.C.; Mokdad, A.H.; Kassebaum, N.J.; Lim, S.; Irvine, C.M.S.; Vos, T.; Brown, A.D.; et al. Progress in adolescent health and wellbeing, tracking 12 headline indicators for 195 countries and territories, 1990–2016. Lancet 2019, 393, 1101–1118. [Google Scholar] [CrossRef] [Green Version]
- Petry, N.; Olofin, I.; Hurrell, R.F.; Boy, E.; Wirth, J.P.; Moursi, M.; Donahue Angel, M.; Rohner, F. The Proportion of Anemia Associated with Iron Deficiency in Low, Medium, and High Human Development Index Countries, A Systematic Analysis of National Surveys. Nutrients 2016, 8, 693. [Google Scholar] [CrossRef]
- Thomas, D.; Chandra, J.; Sharma, S.; Jain, A.; Pemde, H.K. Determinants of Nutritional Anemia in Adolescents. Indian Pediatr. 2015, 52, 867–869. [Google Scholar] [CrossRef]
- Nairz, M.; Theurl, I.; Wolf, D.; Weiss, G. Iron deficiency or anemia of inflammation? Wien. Med. Wochenschr. 2016, 166, 411–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leroy, J.L.; Frongillo, E.A. Perspective, What Does Stunting Really Mean? A Critical Review of the Evidence. Adv. Nutr. 2019, 10, 196–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keino, S.; Plasqui, G.; Ettyang, G.; van den Borne, B. Determinants of stunting and overweight among young children and adolescents in sub-Saharan Africa. Food Nutr. Bull. 2014, 35, 167–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraemer, S. The fragile male. BMJ 2000, 321, 1609–1612. [Google Scholar] [CrossRef]
- Christian, P.; Smith, E.R. Adolescent Undernutrition, Global Burden, Physiology, and Nutritional Risks. Ann. Nutr. Metab. 2018, 72, 316–328. [Google Scholar] [CrossRef]
- Bosch, A.M.; Baqui, A.H.; van Ginneken, J.K. Early-life determinants of stunted adolescent girls and boys in Matlab, Bangladesh. J. Health Popul. Nutr. 2008, 26, 189–199. [Google Scholar]
- Murakami, K. Livingstone MBE, Eating Frequency Is Positively Associated with Overweight and Central Obesity in US Adults. J. Nutr. 2015, 145, 2715–2724. [Google Scholar] [CrossRef] [Green Version]
- Huang, T.T.; Roberts, S.B.; Howarth, N.C.; McCrory, M.A. Effect of screening out implausible energy intake reports on relationships between diet and BMI. Obes. Res. 2005, 13, 1205–1217. [Google Scholar] [CrossRef]
- Arango-Angarita, A.; Shamah-Levy, T.; Rodriguez-Ramirez, S. Dietary energy density is associated with body mass index-for-age in Mexican adolescents. Matern. Child Nutr. 2018, 15, e12664. [Google Scholar] [CrossRef]


{kind=link}
| Girls | Boys | |||||
|---|---|---|---|---|---|---|
| 12–15 Years (n = 2222) | 16–19 Years (n = 1630) | p-Value | 12–15 Years (n = 2377) | 16–19 Years (n = 1377) | p-Value | |
| Age Median (Range) | 13.5 (12.0–15.0) | 17.5 (16.0–19.0) | 13.5 (12.0–15.0) | 17.5 (16.0–19.0) | ||
| Socioeconomic level (%) | 0.38 | 0.08 | ||||
| Low | 48.9 | 48.1 | 48.5 | 43.2 | ||
| Medium | 32.9 | 31.2 | 31.0 | 31.8 | ||
| High | 18.2 | 20.8 | 20.5 | 25.0 | ||
| Area of living | 0.12 | 0.07 | ||||
| Urban | 56.5 | 59.9 | 57.1 | 61.8 | ||
| Region | 0.27 | 0.06 | ||||
| North | 13.1 | 11.9 | 11.3 | 15.2 | ||
| Centre | 45.5 | 48.7 | 48.6 | 46.3 | ||
| South | 48.6 | 39.4 | 40.1 | 38.6 | ||
| Weight status (%) | 0.86 | 0.015 | ||||
| Thinness | 1.4 | 1.8 | 2.5 | 2.1 | ||
| Normal weight | 66.6 | 67.2 | 67.2 | 71.8 | ||
| Overweight/Obese | 31.9 | 31.1 | 30.3 | 26.2 | ||
| Stunting (%) | 13.8 | 21.1 | < 0.0001 | 14.3 | 19.2 | 0.012 |
| Stunted subjects with overweight–obesity (%) £ | 25.0 | 31.2 | 19.2 | 25.2 | ||
| Anemia (%) ₰ | 10.2 | 10.8 | 0.67 | 6.3 | 3.6 | 0.005 |
| Anemic subjects with overweight–obesity (%) ꜜ | 40.2 | 30.2 | 33.5 | 24.0 | ||
| Food Group | Average Intake (g/day) | Nontraditional and Breakfast-Type | Western | Plant-Based | Protein-Rich |
|---|---|---|---|---|---|
| Tortilla | 194.5 | −0.51 | |||
| Other cereals | 29.6 | 0.33 | |||
| Breakfast cereals | 5.0 | 0.63 | |||
| Maize-based food | 50.2 | 0.36 | |||
| Fast-food | 5.1 | 0.34 | |||
| Legumes | 74.3 | 0.58 | |||
| Fruit | 186.2 | 0.54 | |||
| Vegetables | 63.8 | 0.50 | |||
| Poultry and red meat | 47.1 | 0.31 | |||
| Fish and seafood | 8.3 | ||||
| Charcuterie | 8.3 | 0.49 | |||
| Milk * | 166.8 | 0.66 | |||
| Eggs | 31.4 | 0.51 | |||
| Fat | 1.9 | 0.40 | |||
| Sweets | 24.7 | 0.35 | |||
| Cookies | 202.7 | ||||
| Salty snacks | 9.0 | 0.55 | |||
| Industrialized sweet drinks * | 262.6 | 0.63 | |||
| Nonindustrialized sweet drinks * | 256.2 | 0.53 | |||
| Dairy | 33.5 | 0.37 | |||
| Sandwich | 21.6 | 0.30 | 0.36 | ||
| Fried vegetarian dishes | 6.6 | 0.36 | |||
| Sweet bakery | 27.3 | 0.31 | |||
| Soup | 66.3 | 0.50 | |||
| Pasta and rice | 23.7 | 0.57 | |||
| Nuts and avocado | 7.5 | 0.40 |
| Nontraditional and Breakfast-Type | Western | Plant-Based | Protein-Rich | |
|---|---|---|---|---|
| EI:BMR ratio | −0.04 * | 0.29 * | 0.48 * | 0.29 * |
| Energy (kcal) | −0.04 * | 0.36 * | 0.47 * | 0.33 * |
| Protein (% energy) | 0.38 * | −0.05 * | −0.09 * | 0.27 * |
| Fat (% energy) | 0.32 * | 0.43 * | −0.03 * | 0.13 * |
| CHO’s (% energy) | −0.37 * | −0.36 * | 0.05 * | −0.18 * |
| Fiber (g) | −0.30 * | −0.02 * | 0.41 * | 0.37 * |
| Sugar (g) | 0.15 * | 0.38 * | 0.23 * | −0.01 |
| Ca (mg) | 0.15 * | 0.06 * | 0.38 * | 0.20 * |
| Fe (mg) | −0.06 * | 0.26 * | 0.37 * | 0.35 * |
| Zn (mg) | 0.11 * | 0.31 * | 0.38 * | 0.39 * |
| Vit C (mg) | 0.18 * | −0.03 * | 0.51 * | 0.16 * |
| Vit A (IU) | 0.25 * | −0.04 * | 0.49 * | 0.23 * |
| Vit B12 (mg) | 0.40 * | 0.33 * | 0.26 * | 0.23 * |
| Dietary Pattern | Total * (n = 7380) | 12–15 years ₰ (n = 4451) | 16–19 years ₰ (n = 2929) | Boys ¥ (n = 3610) | Girls ¥ (n = 3770) |
|---|---|---|---|---|---|
| Nontraditional and breakfast-type | 1.03 (0.97–1.10) | 0.98 (0.97–1.00) | 0.91 (0.83–1.00) | 1.01 (0.93–1.11) | 1.05 (0.97–1.14) |
| Western | 1.15 (1.08–1.21) | 1.14 (1.06–1.22) | 1.05 (0.95–1.16) | 1.23 (1.12–1.34) | 1.08 (0.99–1.18) |
| Plant-based | 1.10 (1.03–1.17) | 1.20 (1.11–1.30) | 1.04 (0.92–1.17) | 1.07 (0.97–1.18) | 1.12 (1.04–1.22) |
| Protein-rich | 1.02 (0.95–1.09) | 0.97 (0.96–1.03) | 1.05 (0.95–1.16) | 1.06 (0.98–1.15) | 0.98 (0.91–1.05) |
| Dietary Pattern | Total * (n = 7080) | 12–15 years ₰ (n = 4288) | 16–19 years ₰ (n = 2792) | Boys ¥ (n = 3447) | Girls ¥ (n = 3633) |
|---|---|---|---|---|---|
| Nontraditional and breakfast-type | 0.91 (0.81–1.01) | 0.87 (0.76–0.99) | 0.96 (0.80–1.16) | 0.87 (0.76–0.99) | 0.83 (0.73–0.96) |
| Western | 1.11 (0.98–1.26) | 1.11 (0.94–1.30) | 1.13 (0.92–1.38) | 1.11 (0.94–1.30) | 1.24 (1.06–1.45) |
| Plant-based | 0.99 (0.88–1.11) | 1.04 (0.89–1.22) | 0.87 (0.76–1.01) | 1.04 (0.89–1.22) | 0.96 (0.84–1.09) |
| Protein-rich | 1.02 (0.92–1.12) | 1.09 (0.95–1.25) | 0.92 (0.79–1.06) | 1.09 (0.95–1.25) | 0.93 (0.83–1.05) |
| Dietary Pattern | Total * | 12–15 years ₰ (n = 4451) | 16–19 years ₰ (n = 2929) | Boys ¥ (n = 3610) | Girls ¥ (n = 3770) |
|---|---|---|---|---|---|
| Nontraditional and breakfast-type | 0.88 (0.81–0.95) | 0.90 (0.80–1.00) | 0.85 (0.77–0.95) | 0.89 (0.81–0.97) | 0.86 (0.77–1.03) |
| Western | 0.86 (0.80–0.92) | 0.88 (0.80–0.97) | 0.85 (0.76–0.96) | 0.81 (0.74–0.89) | 0.93 (0.83–1.03) |
| Plant-based | 0.85 (0.79–0.92) | 0.80 (0.71–0.90) | 0.90 (0.80–1.02) | 0.80 (0.71–0.90) | 0.80 (0.72–0.89) |
| Protein-rich | 0.96 (0.90–1.02) | 0.92 (0.84–1.01) | 1.00 (0.91–1.10) | 0.92 (0.84–1.01) | 0.98 (0.90–1.07) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zárate-Ortiz, A.G.; Melse-Boonstra, A.; Rodríguez-Ramírez, S.; Hernández-Cordero, S.; Feskens, E.J.M. Dietary Patterns and the Double Burden of Malnutrition in Mexican Adolescents: Results from ENSANUT-2006. Nutrients 2019, 11, 2753. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112753
Zárate-Ortiz AG, Melse-Boonstra A, Rodríguez-Ramírez S, Hernández-Cordero S, Feskens EJM. Dietary Patterns and the Double Burden of Malnutrition in Mexican Adolescents: Results from ENSANUT-2006. Nutrients. 2019; 11(11):2753. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112753
Chicago/Turabian StyleZárate-Ortiz, Arli Guadalupe, Alida Melse-Boonstra, Sonia Rodríguez-Ramírez, Sonia Hernández-Cordero, and Edith J. M. Feskens. 2019. "Dietary Patterns and the Double Burden of Malnutrition in Mexican Adolescents: Results from ENSANUT-2006" Nutrients 11, no. 11: 2753. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112753