Adherence to Time-Restricted Feeding and Impact on Abdominal Obesity in Primary Care Patients: Results of a Pilot Study in a Pre–Post Design


Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruiting
2.2. Intervention
2.3. Data Assessment
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
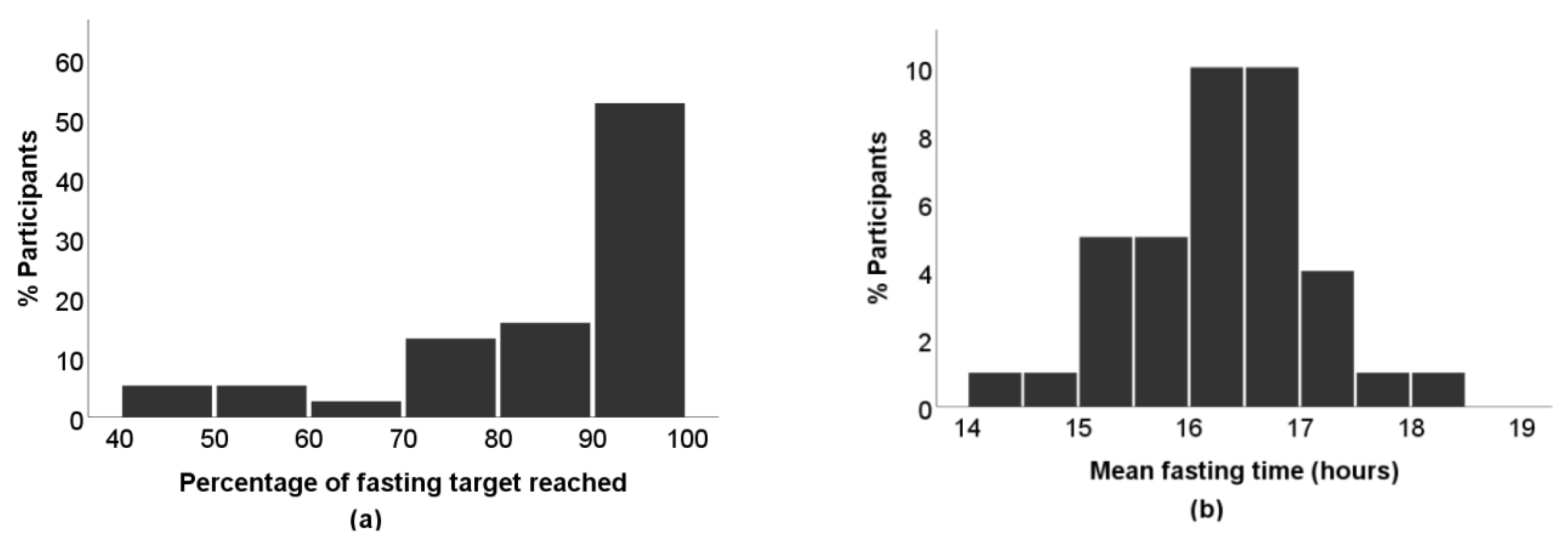
3.2. Primary Outcome and Diaries
3.3. Secondary Outcomes
3.4. Feelings of Hunger, Side Effects, and Participants’ Assessment
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organisation (WHO). Noncommunicable Diseses, Factsheet. Available online: http://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 4 October 2019).
- World Health Organization (WHO). Germany WHO: Noncommunicable Diseases (NCD) Country Profiles. Available online: https://www.who.int/nmh/countries/deu_en.pdf?ua=1 (accessed on 4 October 2019).
- National Center for Health Statistics. Health, United States, 2017: With Special Feature on Mortality. Available online: https://www.cdc.gov/nchs/data/hus/hus17.pdf (accessed on 18 July 2019).
- Ritchie, S.A.; Connell, J.M.C. The Link between Abdominal Obesity, Metabolic Syndrome and Cardiovascular Disease. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Freemantle, N.; Holmes, J.; Hockey, A.; Kumar, S. How Strong Is the Association between Abdominal Obesity and the Incidence of Type 2 Diabetes? Int. J. Clin. Pract. 2008, 62, 1391–1396. [Google Scholar] [CrossRef] [PubMed]
- Doyle, S.L.; Donohoe, C.L.; Lysaght, J.; Reynolds, J.V. Visceral Adiposity, Insulin Resistance and Cancer Risk. Proc. Nutr. Soc. 2012, 3, 12. [Google Scholar] [CrossRef]
- Zammit, C.; Liddicoat, H.; Moonsie, I.; Makker, H. Obesity and Respiratory Diseases. Int. J. Gen. Med. 2010, 3, 335–343. [Google Scholar] [CrossRef]
- Kesztyüs, D.; Erhardt, J.; Schönsteiner, D.; Kesztyüs, T. Therapeutic Treatment for Abdominal Obesity in Adults—A Meta-Analysis and Systematic Review of Randomized Controlled Trials. Dtsch. Arztebl. Int. 2018, 115, 487–493. [Google Scholar] [CrossRef]
- Johnston, B.C.; Kanters, S.; Bandayrel, K.; Wu, P.; Naji, F.; Siemieniuk, R.A.; Ball, G.D.C.; Busse, J.W.; Thorlund, K.; Guyatt, G.; et al. Comparison of Weight Loss among Named Diet Programs in Overweight and Obese Adults: A Meta-Analysis. JAMA 2014, 312, 923–933. [Google Scholar] [CrossRef]
- Arterburn, D.E.; Courcoulas, A.P. Bariatric Surgery for Obesity and Metabolic Conditions in Adults. BMJ 2014, 349, 1–15. [Google Scholar] [CrossRef]
- Patterson, R.E.; Sears, D.D. Metabolic Effects of Intermittent Fasting. Annu. Rev. Nutr. 2017, 37, 371–393. [Google Scholar] [CrossRef]
- Chaix, A.; Zarrinpar, A.; Miu, P.; Panda, S. Time-Restricted Feeding Is a Preventative and Therapeutic Intervention against Diverse Nutritional Challenges. Cell Metab. 2014, 20, 991–1005. [Google Scholar] [CrossRef]
- Rothschild, J.; Hoddy, K.K.; Jambazian, P.; Varady, K.A. Time-Restricted Feeding and Risk of Metabolic Disease: A Review of Human and Animal Studies. Nutr. Rev. 2014, 72, 308–318. [Google Scholar] [CrossRef]
- Gill, S.; Panda, S. A Smartphone App Reveals Erratic Diurnal Eating Patterns in Humans that Can Be Modulated for Health Benefits. Cell Metab. 2015, 22, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Marinac, C.R.; Nelson, S.H.; Breen, C.I.; Hartman, S.J.; Natarajan, L.; Pierce, J.P.; Flatt, S.W.; Sears, D.D.; Patterson, R.E. Prolonged Nightly Fasting and Breast Cancer Prognosis. JAMA Oncol. 2016, 2, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Antoni, R.; Robertson, T.M.; Robertson, M.D.; Johnston, J.D. A Pilot Feasibility Study Exploring the Effects of a Moderate Time-Restricted Feeding Intervention on Energy Intake, Adiposity and Metabolic Physiology in Free-Living Human Subjects. J. Nutr. Sci. 2018, 1–6. [Google Scholar] [CrossRef]
- Gabel, K.; Hoddy, K.K.; Haggerty, N.; Song, J.; Kroeger, C.M.; Trepanowski, J.F.; Panda, S.; Varady, K.A. Effects of 8-Hour Time Restricted Feeding on Body Weight and Metabolic Disease Risk Factors in Obese Adults: A Pilot Study. Nutr. Heal. Aging 2018, 4, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Moro, T.; Tinsley, G.; Bianco, A.; Marcolin, G.; Pacelli, Q.F.; Battaglia, G.; Palma, A.; Gentil, P.; Neri, M.; Paoli, A. Effects of Eight Weeks of Time-Restricted Feeding (16/8) on Basal Metabolism, Maximal Strength, Body Composition, Inflammation, and Cardiovascular Risk Factors in Resistance-Trained Males. J. Transl. Med. 2016, 14, 1–10. [Google Scholar] [CrossRef]
- Sutton, E.F.; Beyl, R.; Early, K.S.; Cefalu, W.T.; Ravussin, E.; Peterson, C.M. Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even without Weight Loss in Men with Prediabetes. Cell Metab. 2018, 27, 1212–1221. [Google Scholar] [CrossRef] [PubMed]
- Jamshed, H.; Beyl, R.A.; Della Manna, D.L.; Yang, E.S.; Ravussin, E.; Peterson, C.M. Early Time-Restricted Feeding Improves 24-Hour Glucose Levels and Affects Markers of the Circadian Clock, Aging, and Autophagy in Humans. Nutrients 2019, 11, 1234. [Google Scholar] [CrossRef] [PubMed]
- Tinsley, G.M.; Forsse, J.S.; Butler, N.K.; Paoli, A.; Bane, A.A.; La Bounty, P.M.; Morgan, G.B.; Grandjean, P.W. Time-Restricted Feeding in Young Men Performing Resistance Training: A Randomized Controlled Trial. Eur. J. Sport Sci. 2017, 17, 200–207. [Google Scholar] [CrossRef]
- International Diabetes Federation. The IDF Consensus Worldwide Definition of the Metabolic Syndrome; International Diabetes Federation: Brussels, Belgium, 2006. [Google Scholar]
- Ashwell, M.; Cole, T.C.; Dixon, A.K. Ratio of Waist Circumference to Height Is Strong Predictor of Intra-Abdominal Fat. BMJ 1996, 313, 559–560. [Google Scholar] [CrossRef]
- De Toledo, F.W.; Buchinger, A.; Burggrabe, H.; Hölz, G.; Kuhn, C.; Lischka, E.; Lischka, N.; Lützner, H.; May, W.; Ritzmann-Widderich, M.; et al. Fasting Therapy—An Expert Panel Update of the 2002 Consensus Guidelines. Forsch. Komplementmed. 2013, 20, 434–443. [Google Scholar] [CrossRef]
- Kurth, B.-M. Der Kinder-Und Jugendgesundheitssurvey (KiGGS): Ein Überblick Über Planung, Durchführung Und Ergebnisse Unter Berücksichtigung von Aspekten Eines Qualitätsmanagements TL—50. Bundesgesundheitsblatt Gesundheitsforsch. Gesundh. 2007, 50, 533–546. [Google Scholar] [CrossRef] [PubMed]
- Dreyhaupt, J.; Koch, B.; Wirt, T.; Schreiber, A.; Brandstetter, S.; Kesztyues, D.; Wartha, O.; Kobel, S.; Kettner, S.; Prokopchuk, D.; et al. Evaluation of a Health Promotion Program in Children: Study Protocol and Design of the Cluster-Randomized Baden-Wuerttemberg Primary School Study [DRKS-ID: DRKS00000494]. BMC Public Health 2012, 12, 157. [Google Scholar] [CrossRef] [PubMed]
- Stewart, A.; Marfell-Jones, M.; Olds, T.; de Ridder, H. International Standards for Anthropometric Assessment; ISAK: Lower Hutt, New Zealand, 2011. [Google Scholar]
- Ashwell, M.; Hsieh, S.D. Six Reasons Why the Waist-to-Height Ratio is a Rapid and Effective Global Indicator for Health Risks of Obesity and How its Use Could Simplify the International Public Health Message on Obesity. Int. J. Food Sci. Nutr. 2005, 56, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Longo, V.D.; Panda, S. Fasting, Circadian Rhythms, and Time-Restricted Feeding in Healthy Lifespan. Cell Metab. 2016, 23, 1048–1059. [Google Scholar] [CrossRef]
- Hu, D.; Mao, Y.; Xu, G.; Liao, W.; Yang, H.; Zhang, H. Gut Flora Shift Caused by Time-Restricted Feeding Might Protect the Host from Metabolic Syndrome, Inflammatory Bowel Disease and Colorectal Cancer. Transl. Cancer Res. 2018, 7, 1282–1289. [Google Scholar] [CrossRef]
- Sunderram, J.; Sofou, S.; Kamisoglu, K.; Karantza, V.; Androulakis, I.P. Time-Restricted Feeding and the Realignment of Biological Rhythms: Translational Opportunities and Challenges. J. Transl. Med. 2014, 12, 1–9. [Google Scholar] [CrossRef]
- Di Francesco, A.; Di Germanio, C.; Bernier, M.; De Cabo, R. A Time to Fast. Science 2018, 362, 770–775. [Google Scholar] [CrossRef]
- Harrington, J.M. Health Effects of Shift Work and Extended Hours of Work. Occup. Environ. Med. 2001, 58, 68–72. [Google Scholar] [CrossRef]
- Gu, F.; Han, J.; Laden, F.; Pan, A.; Caporaso, N.E.; Stampfer, M.J.; Kawachi, I.; Rexrode, K.M.; Willett, W.C.; Hankinson, S.E.; et al. Total and Cause-Specific Mortality of U.S. Nurses Working Rotating Night Shifts. Am. J. Prev. Med. 2015, 48, 241–252. [Google Scholar] [CrossRef]
- Hutchison, A.T.; Wittert, G.A.; Heilbronn, L.K. Matching Meals to Body Clocks—Impact on Weight and Glucose Metabolism. Nutrients 2017, 9, 222. [Google Scholar] [CrossRef]
- Kahleova, H.; Belinova, L.; Malinska, H.; Oliyarnyk, O.; Trnovska, J.; Skop, V.; Kazdova, L.; Dezortova, M.; Hajek, M.; Tura, A.; et al. Eating Two Larger Meals a Day (Breakfast and Lunch) is More Effective than Six Smaller Meals in a Reduced-Energy Regimen for Patients with Type 2 Diabetes: A Randomised Crossover Study. Diabetologia 2014, 57, 1552–1560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaughan, K.L.; Mattison, J.A. Watch the Clock, Not the Scale. Cell Metab. 2018, 27, 1159–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, M.L.; Kenward, M.G.; Fairclough, D.L.; Horton, N.J. Differential Dropout and Bias in Randomised Controlled Trials: When It Matters and When It May Not. BMJ 2013, 346, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.L.; Bergeron, C.D.; Ahn, S.N.; Towne, S.D.; Mingo, C.A.; Robinson, K.T.; Mathis, J.; Meng, L.; Ory, M.G. Engaging the Underrepresented Sex: Male Participation in Chronic Disease Self-Management Education (CDSME) Programs. Am. J. Mens. Health 2018, 12, 935–943. [Google Scholar] [CrossRef] [PubMed]
- Feldman, S.; Ammar, W.; Lo, K.; Trepman, E.; van Zuylen, M.; Etzioni, O. Quantifying Sex Bias in Clinical Studies at Scale With Automated Data Extraction. JAMA Netw. Open 2019, 2, e196700. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Female (n = 31) | Male (n = 9) | Total (n = 40) | |
|---|---|---|---|
| Age, years M (SD) | 49.2 (11.3) | 48.6 (16.2) | 49.1 (12.4) |
| Weight, kg M (SD) | 84.2 (18.3) 1 | 104.6 (23.6) | 88.8 (21.1) |
| Waist circumference, cm M (SD) | 104.7 (11.5) | 114.3 (17.0) | 106.9 (13.3) |
| BMI, kg/m2 M (SD) | 31.1 (6.0) | 31.9 (5.7) | 31.3 (5.9) |
| WHtR, M (SD) | 0.64 (0.07) | 0.63 (0.09) | 0.64 (0.07) |
| Normal weight, n (%) | 4 (12.9) | 1 (11.1) | 5 (12.5) |
| Overweight, n (%) | 10 (32.3) | 3 (33.3) | 13 (32.5) |
| Obese, n (%) | 17 (54.8) | 5 (55.6) | 22 (55.0) |
| Abdominal obese, n (%) | 31 (100) | 9 (100) | 40 (100) |
| HbA1c, mmol/mol | 36.6 (5.6) | 40.4 (13.4) | 37.5 (8.0) |
| LDL, mmol/L M (SD) | 3.4 (1.1) | 2.85 (1.1) | 3.3 (1.1) |
| HDL, mmol/L M (SD) | 1.5 (0.4) 2 | 1.0 (0.3) | 1.4 (0.4) |
| TCHOL, mmol/L M (SD) | 6.0 (1.2) | 4.7 (1.1) | 5.4 (1.2) |
| Triglycerides, mmol/L M (SD) | 1.2 (0.7) 3 | 2.1 (0.9) | 1.4 (0.8) |
| hsCRP, mg/L M (SD) * | 2.69 (2,36) | 1.47 (1.23) | 2.41 (2.20) |
| Daily eating time, h M (SD) | 12.40 (2.15) | 11.13 (2.81) | 12.23 (2.27) |
| Female (n = 30) | Male (n = 8) | Total (n = 38) | |
|---|---|---|---|
| Time of first meal, M (SD) | 10.57 (1.72) | 9.58 (1.92) | 10.36 (1.78) |
| Time of last meal, M (SD) | 18.24 (1.70) | 17.35 (1.31) | 18.05 (1.65) |
| Eating phase, h M (SD) | 7.74 (0.71) | 7.71 (1.23) | 7.73 (0.82) |
| Fasting phase, h M (SD) | 16.24 (0.69) | 16.30 (1.23) | 16.25 (0.81) |
| Fasting target reached, % M (SD) | 85.9 (14.6) | 83.8 (18.1) | 85.5 (15.2) |
| Female (n = 31) | Male (n = 9) | Total (n = 40) | |
|---|---|---|---|
| Weight, kg M (SD) | 82.3 (18.5) 1 | 103.7 (24.7) | 87.1 (21.7) |
| Waist circumference, cm M (SD) | 99.4 (12.7) | 109.2 (17.4) | 101.6 (14.2) |
| BMI, kg/m2 M (SD) | 30.4 (6.1) | 31.5 (5.9) | 30.7 (6.0) |
| WHtR, M (SD) | 0.61 (0.07) | 0.60 (0.09) | 0.61 (0.08) |
| Normal weight, n (%) | 9 (29.0) | 1 (11.1) | 10 (25.0) |
| Overweight, n (%) | 6 (19.4) | 3 (33.3) | 9 (22.5) |
| Obesity, n (%) | 16 (51.6) | 5 (55.6) | 21 (52.5) |
| Abdominal obesity, n (%) | 29 (93.5) | 8 (88.9) | 37 (92.5) |
| HbA1c, mmol/mol | 35.2 (4.1) | 38.7 (7.8) | 36.0 (5.3) |
| LDL, mmol/L M (SD) | 3.6 (1.1) | 3.0 (1.2) | 3.5 (1.2) |
| HDL, mmol/l M (SD) | 1.5 (0.3) 2 | 1.0 (0.3) | 1.4 (0.4) |
| TCHOL, mmol/L M (SD) | 5.6 (1.3) | 4.8 (1.2) | 5.4 (1.3) |
| Triglycerides, mmol/L M (SD) | 1.2 (0.8) 3 | 2.0 (1.4) | 1.4 (1.0) |
| hsCRP, nmol/L M (SD) * | 2.63 (2.43) | 2.28 (2.74) | 2.55 (2.47) |
| Δ Weight, kg M (SD) | −1.93 (1.93) | −0.92 (4.05) | −1.71 (2.53) a1 |
| Δ Waist circumference, cm M (SD) | −5.29 (3.15) | −5.12 (3.12) | −5.26 (3.10) a1 |
| Δ BMI, M (SD) | −1.01 (0.75) | −0.32 (1.27) | −0.64 (0.89) a1 |
| Δ WHtR, M (SD) | −0.03 (0.02) | −0.03 (0.02) | −0.03 (0.02) a1 |
| Δ HbA1c, mmol/mol M (SD) | −1.4 (2.4) | −1.7 (6.0) | −1.4 (3.5) a2 |
| Δ LDL, mmol/L M (SD) | 0.2 (0.5) | 0.2 (0.4) | 0.2 (0.5) |
| Δ HDL, mmol/L M (SD) | 0.0 (0.1) | 0.1 (0.1) | 0.0 (0.1) |
| Δ TCHOL, mmol/L M (SD) | 0.0 (0.4) | 0.1 (0.3) | 0.0 (0.4) |
| Δ Triglycerides, mmol/L M (SD) | 0.0 (0.4) | −0.1 (1.3) | 0.0 (0.7) |
| Δ hsCRP, nmol/L M (SD) * | −0.10 (1.86) | 0.82 (3.05) | 0.11 (2.18) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kesztyüs, D.; Cermak, P.; Gulich, M.; Kesztyüs, T. Adherence to Time-Restricted Feeding and Impact on Abdominal Obesity in Primary Care Patients: Results of a Pilot Study in a Pre–Post Design. Nutrients 2019, 11, 2854. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11122854
Kesztyüs D, Cermak P, Gulich M, Kesztyüs T. Adherence to Time-Restricted Feeding and Impact on Abdominal Obesity in Primary Care Patients: Results of a Pilot Study in a Pre–Post Design. Nutrients. 2019; 11(12):2854. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11122854
Chicago/Turabian StyleKesztyüs, Dorothea, Petra Cermak, Markus Gulich, and Tibor Kesztyüs. 2019. "Adherence to Time-Restricted Feeding and Impact on Abdominal Obesity in Primary Care Patients: Results of a Pilot Study in a Pre–Post Design" Nutrients 11, no. 12: 2854. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11122854