Study of the Inhibitory Effects of Enteral Nutrition Formula on Indomethacin-Induced Gastric Lesions in Mice

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagents
2.2. Animals
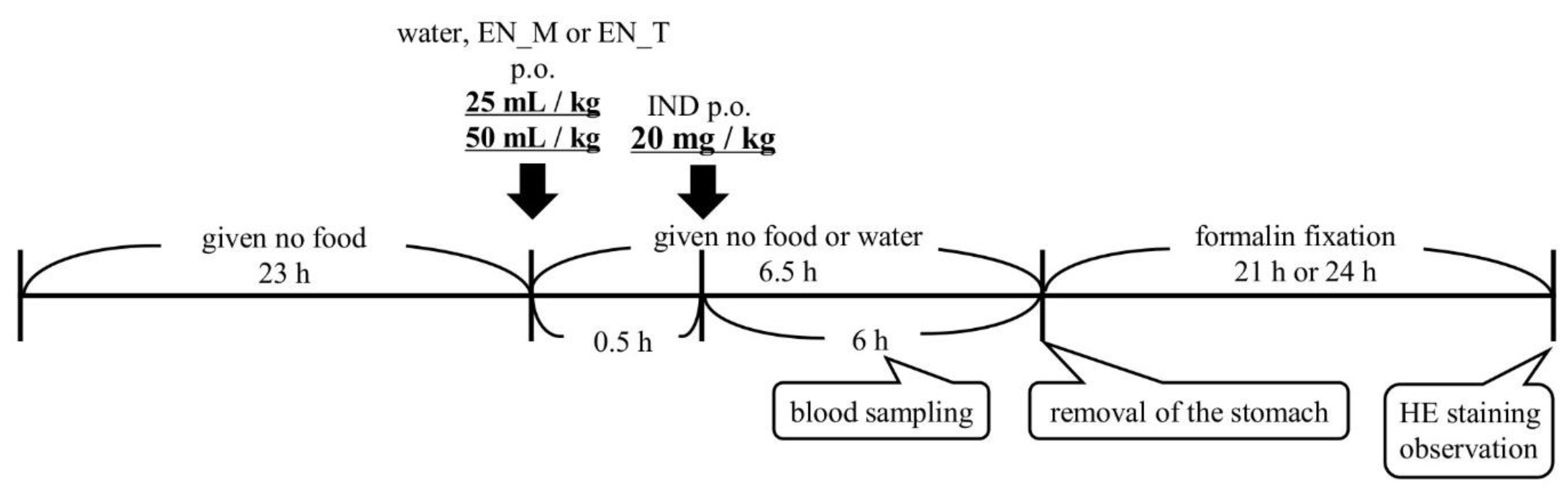
2.3. Dosing and Blood Sampling Schedule
2.4. Gross Observation of Gastric Mucosa and Histological Evaluation with Hematoxylin and Eosin Staining
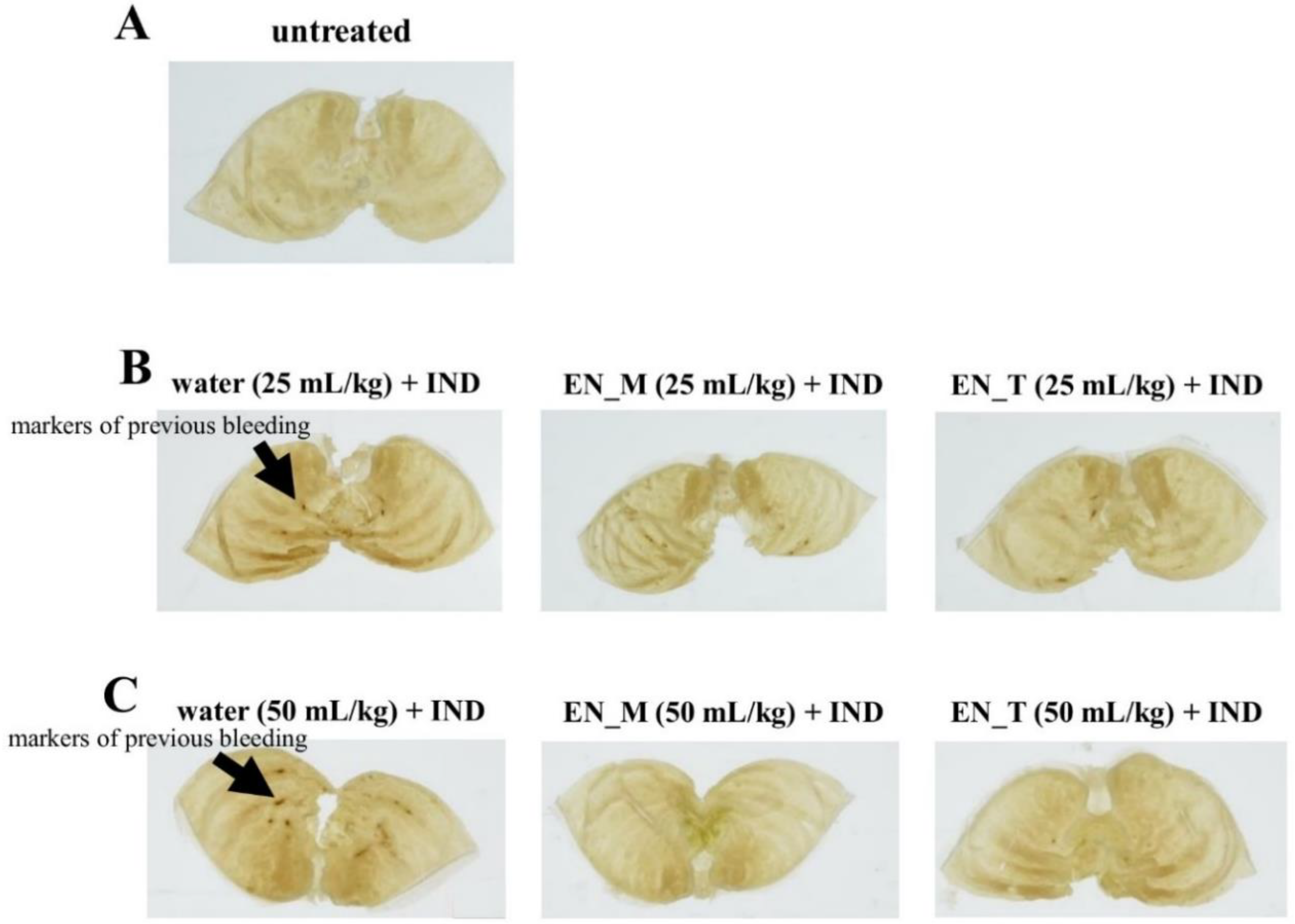
2.4.1. Observation of Gastric Lesions Induced by IND
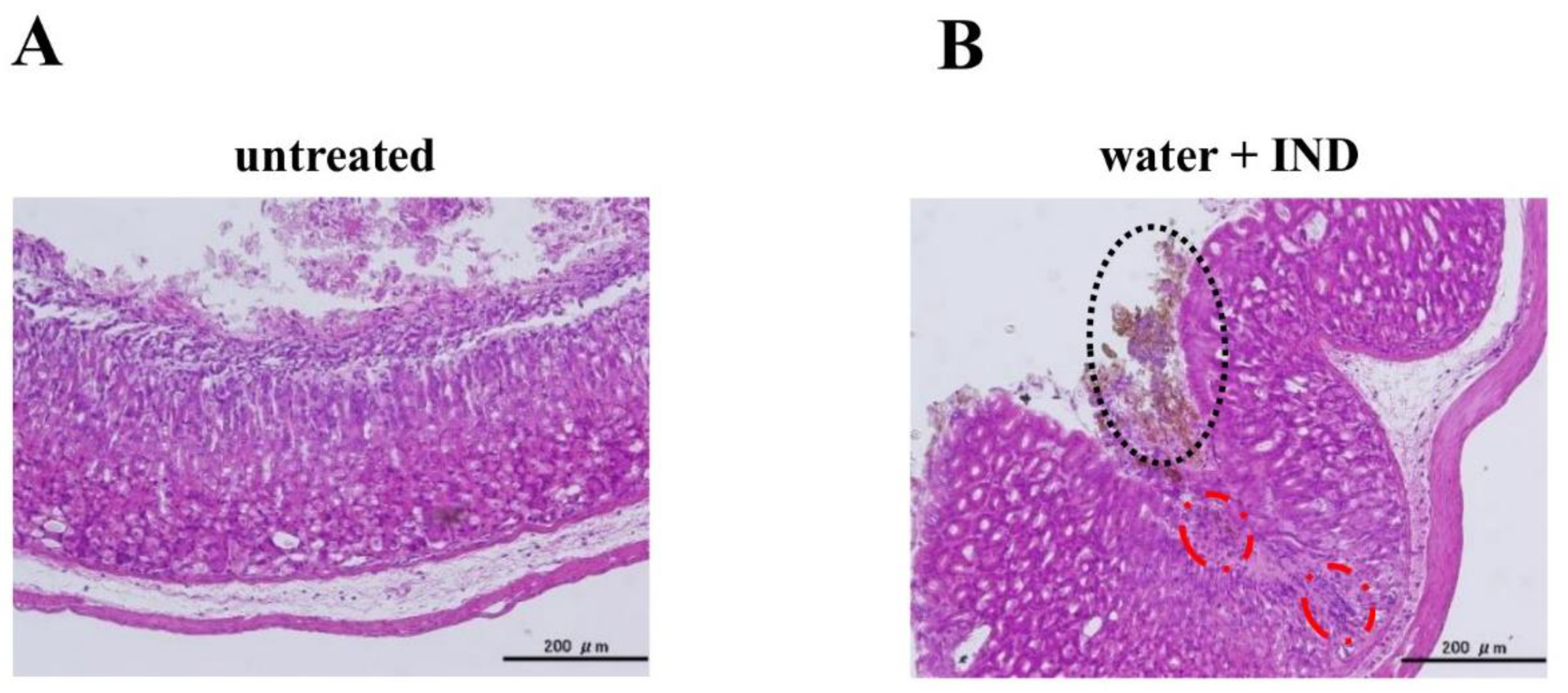
2.4.2. Histological Evaluation
2.5. Analysis of Plasma IND Concentrations
2.6. Calculation of Pharmacokinetic Parameters
2.7. Statistical Analysis
3. Results
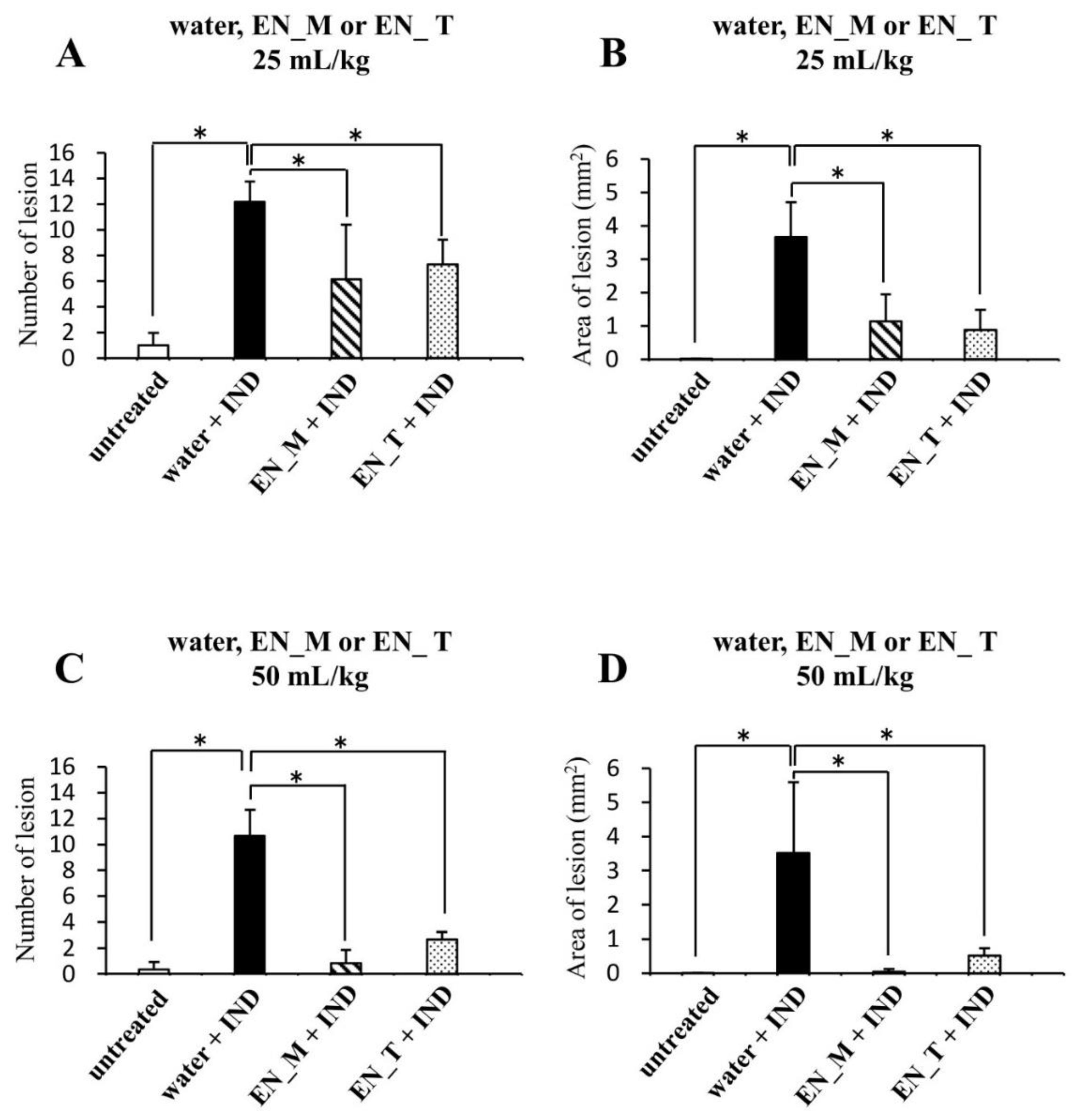
3.1. Effects of Enteral Nutrition Formula on IND-Induced Lesions
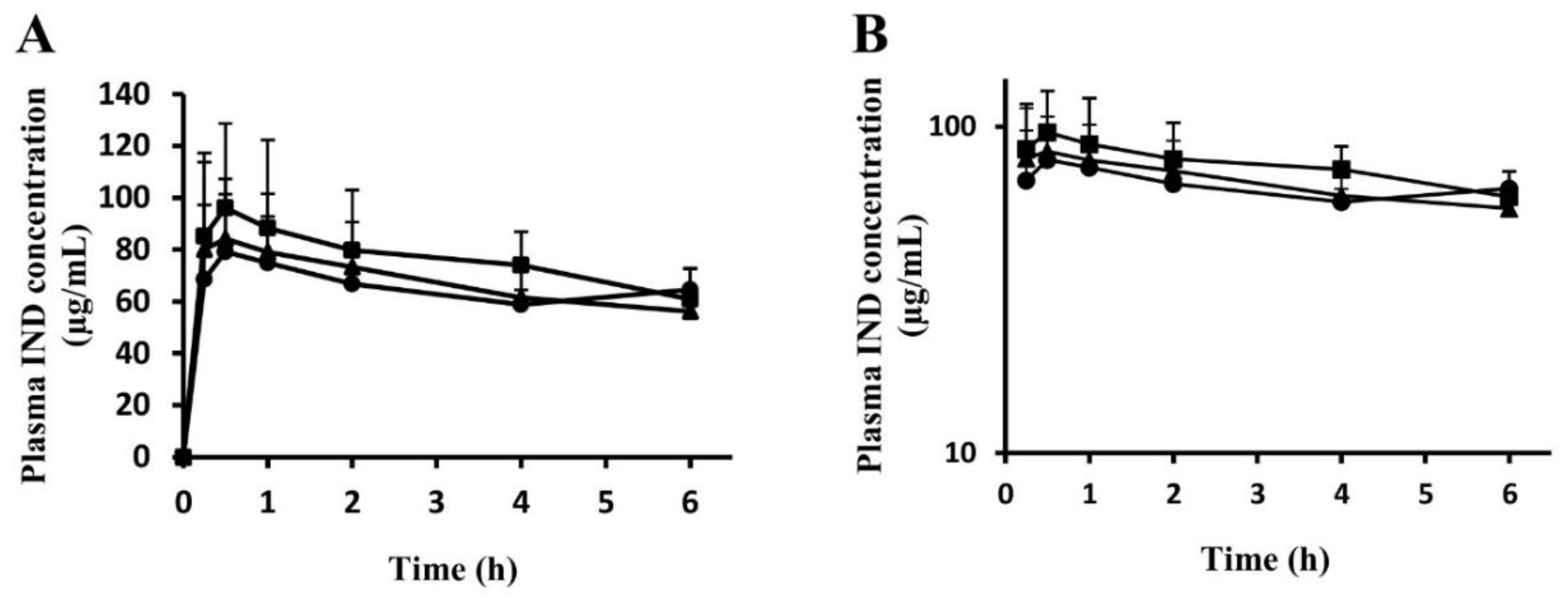
3.2. Time Courses of Plasma IND Concentrations
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Hiraishi, H.; Oki, R.; Tsuchida, K.; Yoshitake, N.; Tominaga, K.; Kusano, K.; Hashimoto, T.; Maeda, M.; Sasai, T.; Shimada, T. Frequency of nonsteroidal anti-inflammatory drug-associated ulcer. Clin. J. Gastroenterol. 2012, 5, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Warner, T.D.; Giuliano, F.; Vojnovic, I.; Bukasa, A.; Mitchell, J.A.; Vane, J.R. Nonsteroid drug selectivities for cyclo-oxygenase-1 rather than cyclo-oxygenase-2 are associated with human gastrointestinal toxicity: A full in vitro analysis. Proc. Natl. Acad. Sci. USA 1999, 96, 7563–7568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizokami, Y.; Narushima, K.; Shiraishi, T.; Otsubo, T.; Narasaka, T.; Matsuoka, T. Non-Helicobacter pylori ulcer disease in rheumatoid arthritis patients receiving long-term NSAID therapy. J. Gastroenterol. 2000, 35, 38–41. [Google Scholar] [PubMed]
- Vitale, P.; Panella, A.; Scilimati, A.; Perrone, M.G. COX-1 inhibitors: Beyond structure toward therapy. Med. Res. Rev. 2016, 36, 641–671. [Google Scholar] [CrossRef] [PubMed]
- Rayar, A.M.; Lagarde, N.; Ferroud, C.; Zagury, J.F.; Montes, M.; Sylla-Iyarreta Veitia, M. Update on COX-2 selective inhibitors: Chemical classification, side effects and their use in cancers and neuronal diseases. Curr. Top. Med. Chem. 2017, 17, 2935–2956. [Google Scholar] [CrossRef] [PubMed]
- Satoh, K.; Yoshino, J.; Akamatsu, T.; Itoh, T.; Kato, M.; Kamada, T.; Takagi, A.; Chiba, T.; Nomura, S.; Mizokami, Y.; et al. Evidence-Based Clinical Practice Guidelines for Peptic Ulcer 2015, 2nd ed.; The Japanese Society of Gastroenterology: Tokyo, Japan, 2015; pp. 108–125. [Google Scholar]
- Satoh, K.; Yoshino, J.; Akamatsu, T.; Itoh, T.; Kato, M.; Kamada, T.; Takagi, A.; Chiba, T.; Nomura, S.; Mizokami, Y.; et al. Evidence-based clinical practice guidelines for peptic ulcer disease 2015. J. Gastroenterol. 2016, 51, 177–194. [Google Scholar] [CrossRef] [Green Version]
- Mizokami, F.; Koide, Y.; Noro, T.; Furuta, K. Polypharmacy with common diseases in hospitalized elderly patients. Am. J. Geriatr. Pharmacother. 2012, 10, 123–128. [Google Scholar] [CrossRef]
- Vinks, T.H.; de Koning, F.H.; de Lange, T.M.; Egberts, T.C. Identification of potential drug-related problems in the elderly: The role of the community pharmacist. Pharm. World Sci. 2006, 28, 33–38. [Google Scholar] [CrossRef]
- Takeda, T.; Asaoka, D.; Tajima, Y.; Matsumoto, K.; Takeda, N.; Hiromoto, T.; Okubo, S.; Saito, H.; Aoyama, T.; Shibuya, T.; et al. Hemorrhagic polyps formed like fundic gland polyps during long-term proton pump inhibitor administration. Clin. J. Gastroenterol. 2017, 10, 478–484. [Google Scholar] [CrossRef] [Green Version]
- Williams, C. Occurrence and significance of gastric colonization during acid-inhibitory therapy. Best Pract. Res. Clin. Gastroenterol. 2001, 15, 511–521. [Google Scholar] [CrossRef]
- Cadle, R.M.; Mansouri, M.D.; Logan, N.; Kudva, D.R.; Musher, D.M. Association of proton-pump inhibitors with outcomes in Clostridium difficile colitis. Am. J. Health Syst. Pharm. 2007, 64, 2359–2363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mori, S.; Kadochi, Y.; Luo, Y.; Fujiwara-Tani, R.; Nishiguchi, Y.; Kishi, S.; Fujii, K.; Ohmori, H.; Kuniyasu, H. Proton pump inhibitor induced collagen expression in colonocytes is associated with collagenous colitis. World J. Gastroenterol. 2017, 23, 1586–1593. [Google Scholar] [CrossRef] [PubMed]
- Ianiro, G.; Cammarota, G.; Valerio, L.; Annicchiarico, E.B.; Milani, A.; Siciliano, M.; Gasbarrini, A. Microscopic colitis. World J. Gastroenterol. 2012, 18, 6206–6215. [Google Scholar] [CrossRef] [PubMed]
- Sekigawa, K.; Okubo, M.; Kobayashi, K.; Nuta, J.; Furuhata, S.; Sekine, M.; Mitsui, H.; Hashimoto, N.; Yamaguchi, H.; Kishida, Y.; et al. 3 cases of collagenous colitis which is suspected to be due to proton pump inhibitor. Prog. Dig. Endosc. 2012, 80, 126–128. [Google Scholar] [CrossRef] [Green Version]
- Morimoto, N.; Kurata, H.; Okitsu, K.; Sunada, F.; Akaike, Y. Collagenous Colitis Associated with Lansoprazole (Report on Three Cases). Nihon Noson Igakkai Zassi. 2013, 62, 146–150. [Google Scholar]
- Ohara, J.; Sugiyama, Y.; Asakawa, T.; Endo, M.; Ihduka, Y.; Gotoh, F.; Kawamura, T.; Furuya, H.; Kobayashi, D. Esomeprazole—Associated Collagenous Colitis: A Case Report. Prog. Dig. Endosc. 2017, 90, 126–128. [Google Scholar] [CrossRef]
- Inoue, H.; Kawashima, Y.; Hamada, K.; Yokota, S.; Sasaki, M. Functional evaluations of a new type formula that features a state change from liquid to semi-solidified state depending upon pH. Clin. Nutr. ESPEN 2014, 9, e185–e191. [Google Scholar] [CrossRef]
- Akashi, T.; Matsumoto, K.; Hashimoto, R.; Koikawa, N.; Yamada, M.; Shimizu, J.; Kakegawa, C.; Nakamura, M.; Kumamoto, C. Resumption of enteral nutrition using enteral formula containing sodium alginate following hemorrhaging after endoscopic sphincterotomy: A case report. Nihon Ronen Igakkai Zasshi. Jpn. J. Geriatr. 2017, 54, 573–580. [Google Scholar] [CrossRef]
- Yamamoto, A.; Itoh, T.; Nasu, R.; Nishida, R. Sodium alginate ameliorates indomethacin-induced gastrointestinal mucosal injury via inhibiting translocation in rats. World J. Gastroenterol. 2014, 20, 2641–2652. [Google Scholar] [CrossRef]
- Wang, T.; Zhao, S.; Wang, Y.; Yang, Y.; Yao, L.; Chu, L.; Du, H.; Fu, F. Protective effects of escin against indomethacin-induced gastric ulcer in mice. Toxicol. Mech. Methods 2014, 24, 560–566. [Google Scholar] [CrossRef]
- Banerjee, D.; Maity, B.; Nag, S.K.; Bandyopadhyay, S.K.; Chattopadhyay, S.; Bandyopadhyay, K.S.; Chattopadhyay, S. Healing potential of Picrorhiza kurroa (Scrofulariaceae) rhizomes against indomethacin-induced gastric ulceration: A mechanistic exploration. BMC Complement. Altern. Med. 2008, 8, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doll-Shankaruk, M.; Yau, W.N.; Oelke, C. Implementation and effects of a medication pass nutritional supplement program in a long-term care facility: A pilot study. J. Gerontol. Nurs. 2008, 34, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Xue, Q.L.; Bandeen-Roche, K.; Varadhan, R.; Zhou, J.; Fried, L.P. Initial Manifestations of Frailty Criteria and the Development of Frailty Phenotype in the Women’s Health and Aging Study II. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 984–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geller, A.I.; Nopkhun, W.; Dows-Martinez, M.N.; Strasser, D.C. Polypharmacy and the role of physical medicine and rehabilitation. PM & R 2012, 4, 198–219. [Google Scholar] [CrossRef]
- Nagai, K.; Omotani, S.; Ito, A.; Nishimura, I.; Hatsuda, Y.; Mukai, J.; Teramachi, H.; Myotoku, M. Alterations in Pharmacokinetics of Orally Administered Carbamazepine in Rats Treated with Sodium alginate: Possible Interaction between Therapeutic Drugs and Semi-solid Enteral Nutrients. Drug Res. 2019, 69, 168–172. [Google Scholar] [CrossRef]
- Silva, F.R.; Novaes, M.R.C.G. Interactions between drugs and drug-nutrient in enteral nutrition: A review based on evidences. Nutr. Hosp. 2014, 30, 514–518. [Google Scholar]
- Bonnici, A.; Ruiner, C.E.; St-Laurent, L.; Hornstein, D. An interaction between levodopa and enteral nutrition resulting in neuroleptic malignant-like syndrome and prolonged ICU stay. Ann. Pharmacother. 2010, 44, 1504–1507. [Google Scholar] [CrossRef]
- Cooper, M.K.; Brock, D.G.; McDaniel, C.M. Interaction between levodopa and enteral nutrition. The Annals of pharmacotherapy. Ann. Pharmacother. 2008, 42, 439–442. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Water + IND | EN_M + IND | EN_T + IND | |
|---|---|---|---|
| Tmax (h) | 0.85 ± 0.70 | 0.50 ± 0.31 | 1.7 ± 2.4 |
| Cmax (µg/mL) | 76.0 ± 35.6 | 88.8 ± 26.8 | 102 ± 22 |
| AUC0–6 (µg h/mL) | 385 ± 51 | 399 ± 82 | 435 ± 96 |
| MRT | 2.96 ± 0.21 | 2.84 ± 0.17 | 2.89 ± 0.35 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshimi, T.; Yamagishi, Y.; Kanegawa, I.; Suda, M.; Saiki, R.; Tanaka, K.-i.; Goda, H.; Kudo, T.; Ito, K. Study of the Inhibitory Effects of Enteral Nutrition Formula on Indomethacin-Induced Gastric Lesions in Mice. Nutrients 2019, 11, 3058. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11123058
Yoshimi T, Yamagishi Y, Kanegawa I, Suda M, Saiki R, Tanaka K-i, Goda H, Kudo T, Ito K. Study of the Inhibitory Effects of Enteral Nutrition Formula on Indomethacin-Induced Gastric Lesions in Mice. Nutrients. 2019; 11(12):3058. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11123058
Chicago/Turabian StyleYoshimi, Takeshi, Yoshiaki Yamagishi, Issei Kanegawa, Megumi Suda, Rei Saiki, Ken-ichiro Tanaka, Hitomi Goda, Toshiyuki Kudo, and Kiyomi Ito. 2019. "Study of the Inhibitory Effects of Enteral Nutrition Formula on Indomethacin-Induced Gastric Lesions in Mice" Nutrients 11, no. 12: 3058. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11123058