Using Group Model Building to Describe the System Driving Unhealthy Eating and Identify Intervention Points: A Participatory, Stakeholder Engagement Approach in the Caribbean

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Settings
2.2. Ethical Approval
2.3. Interviews and Stakeholder Selection
2.4. The Group Model Building Workshops
2.5. Identifying Places to Intervene
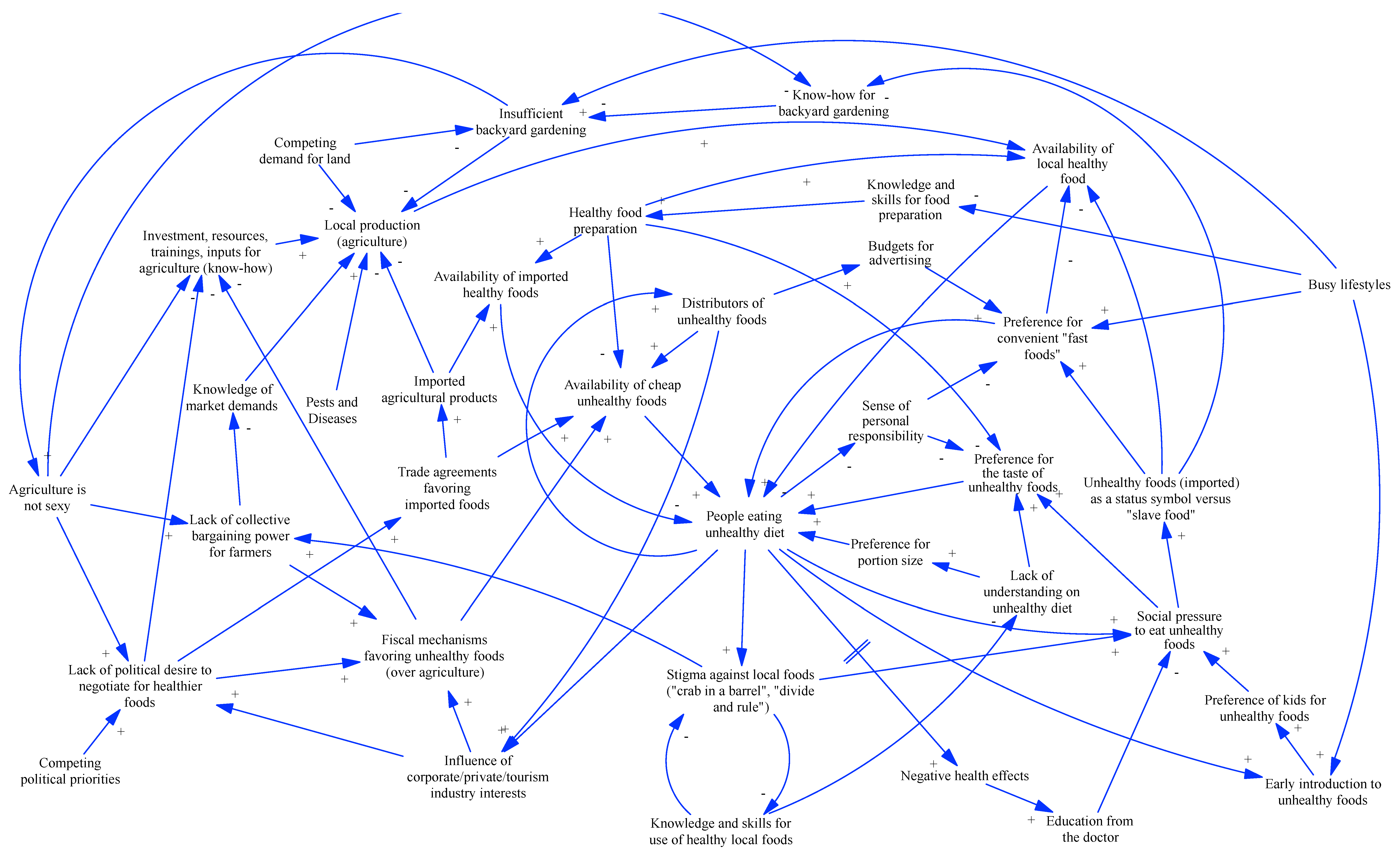
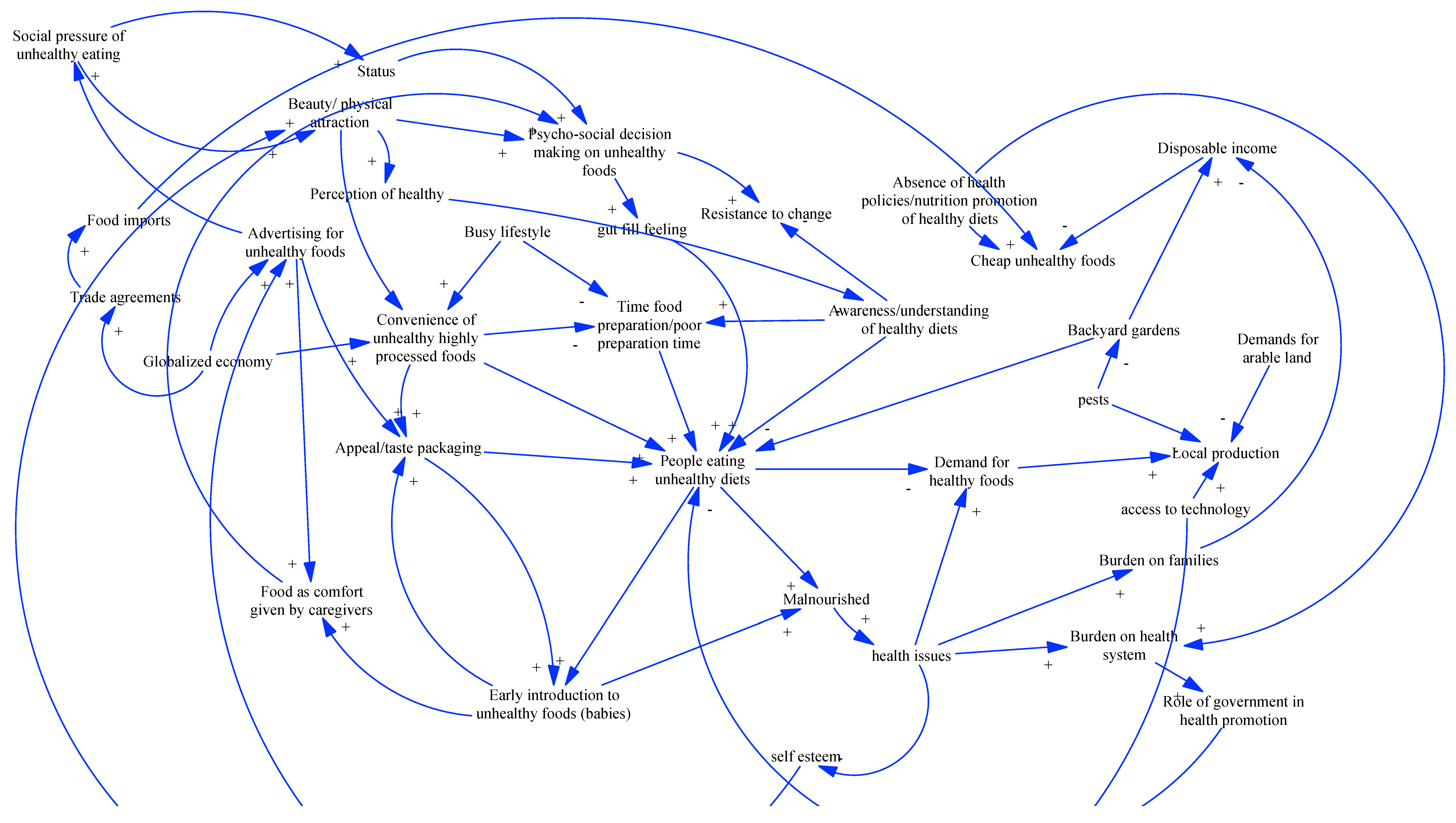
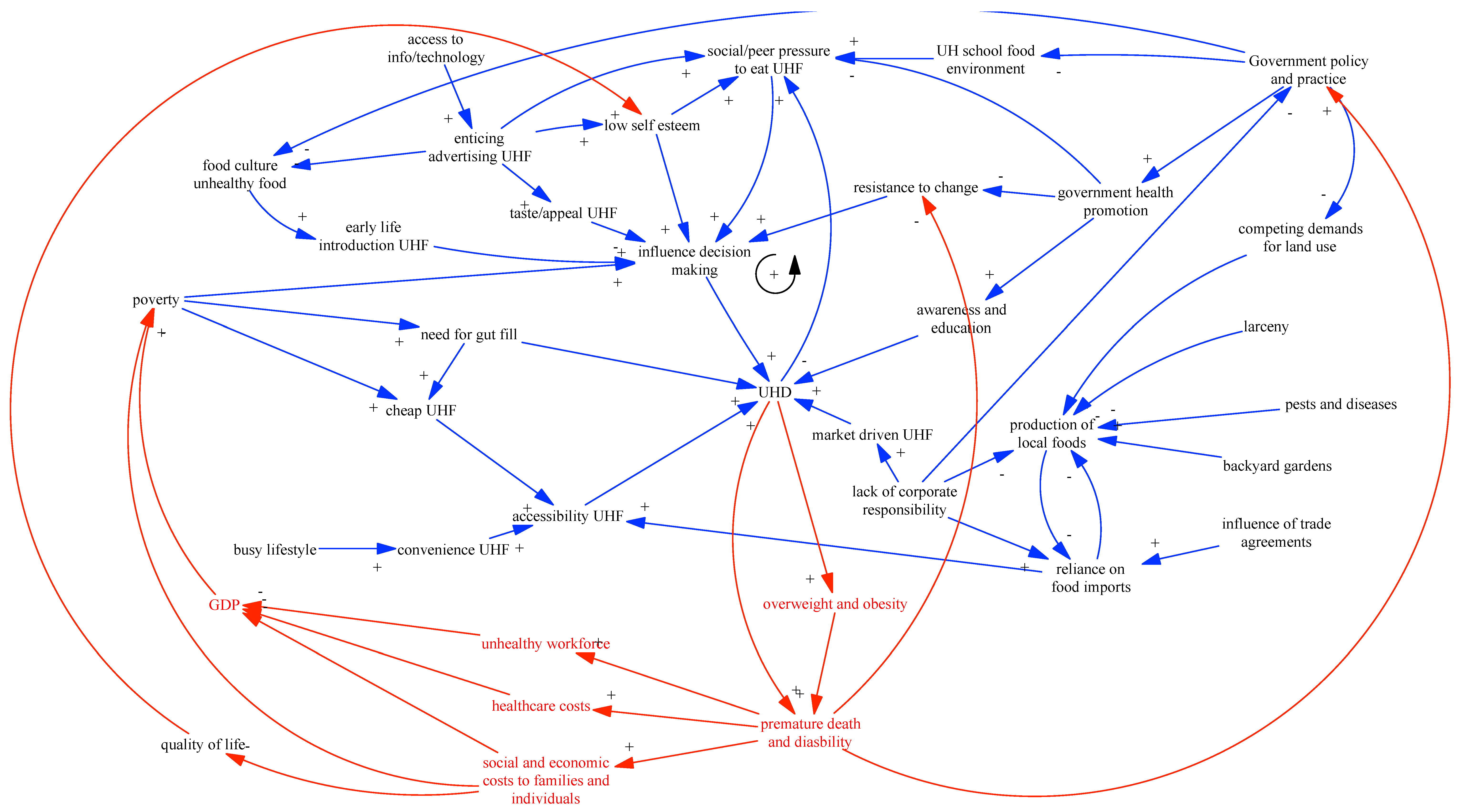
3. Results
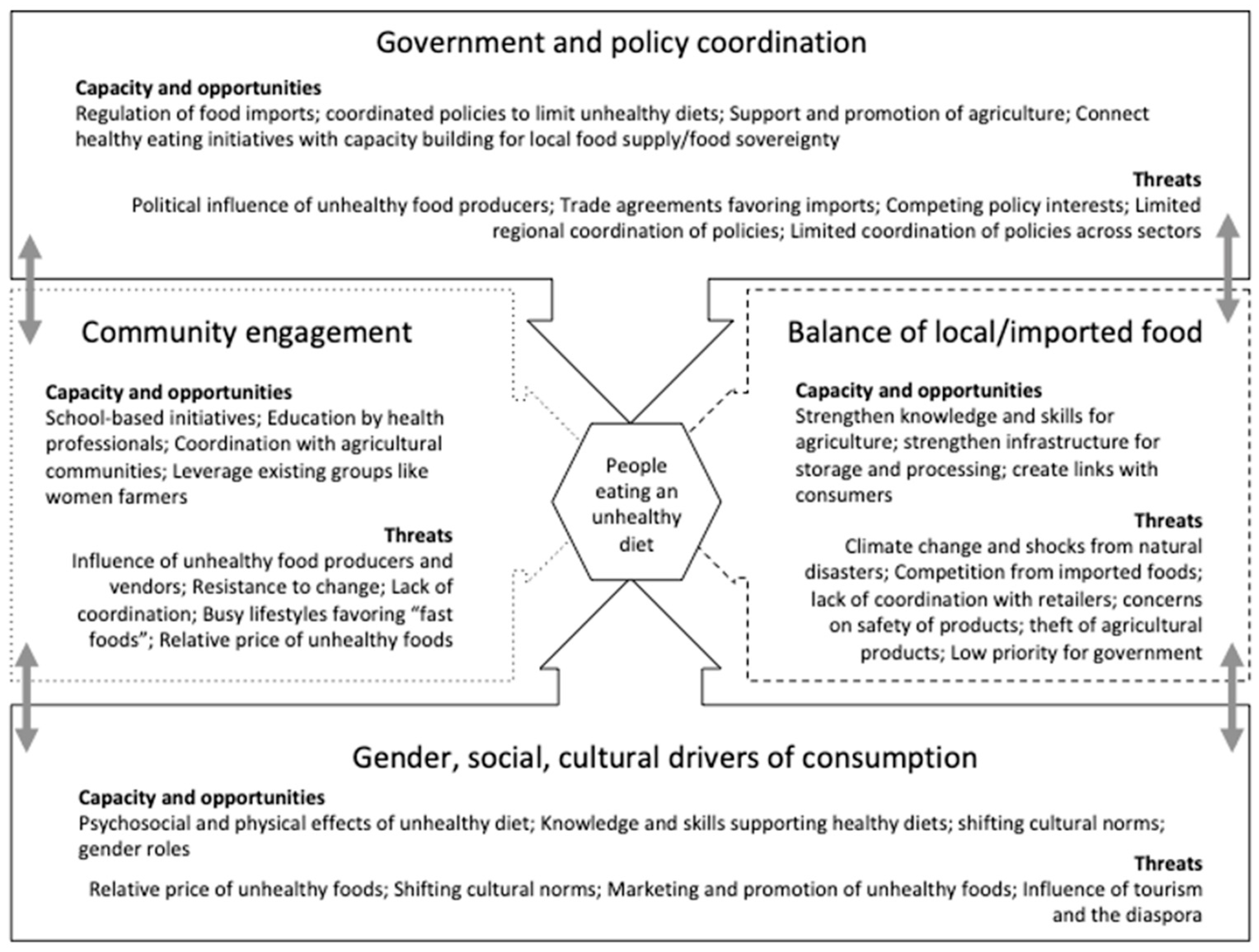
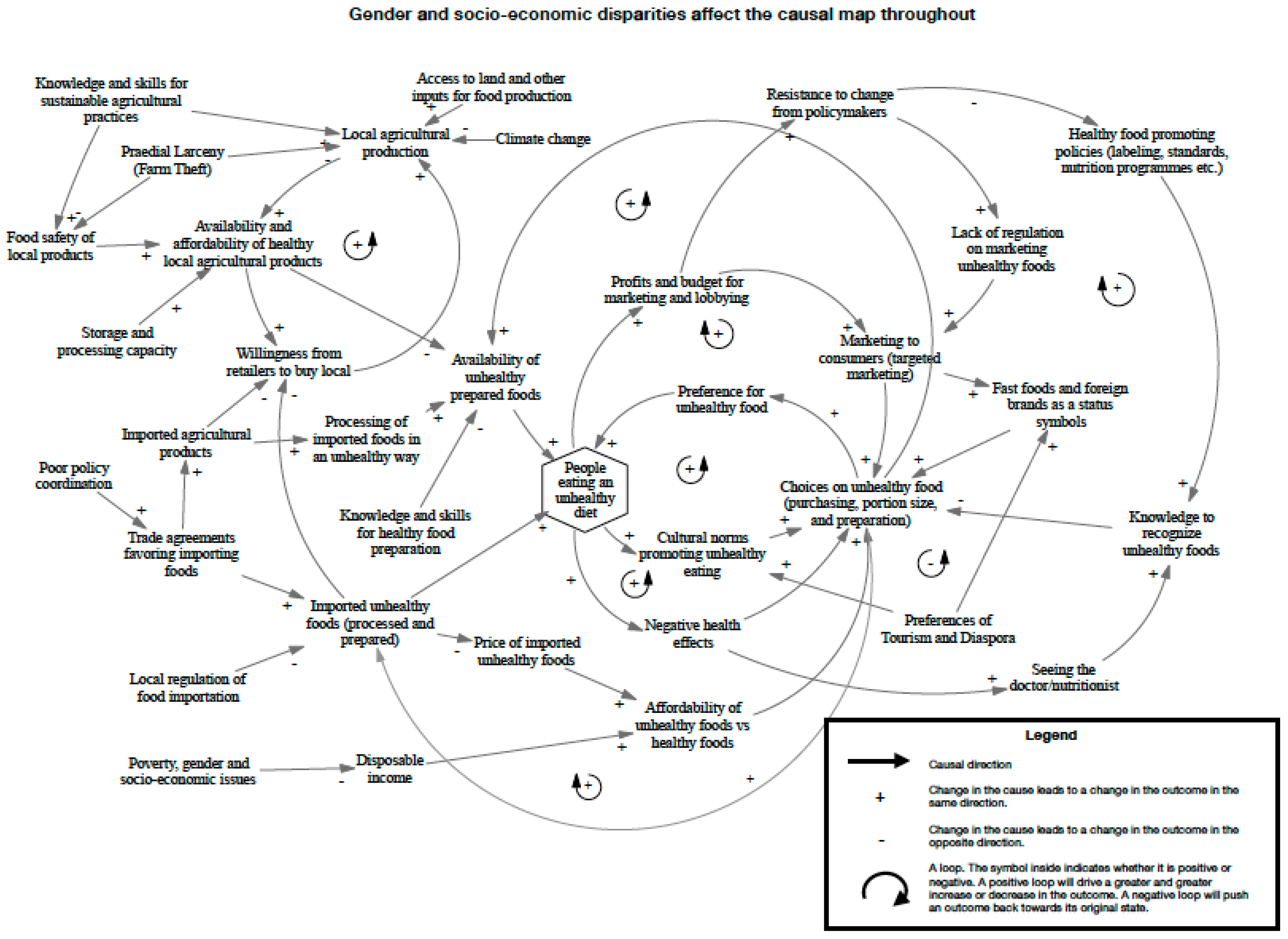
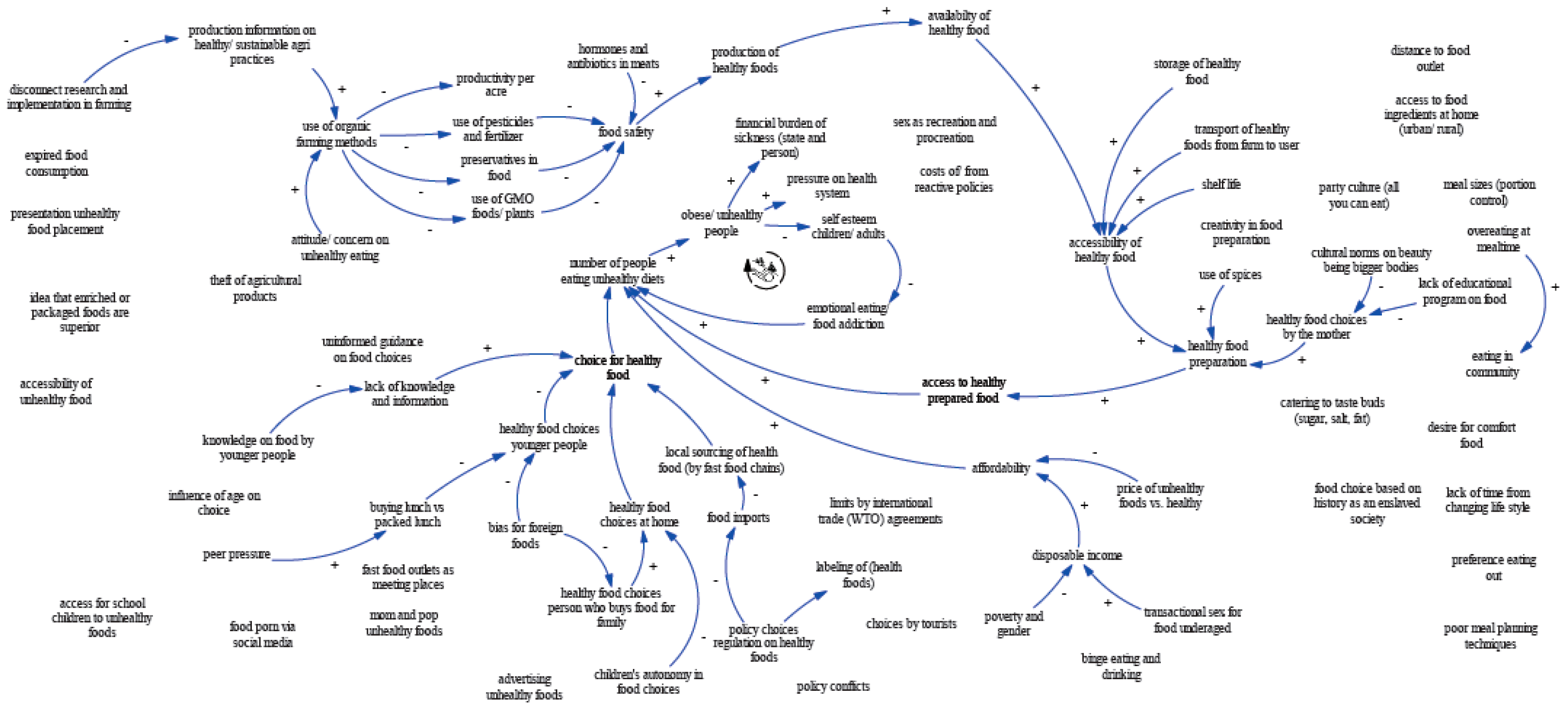
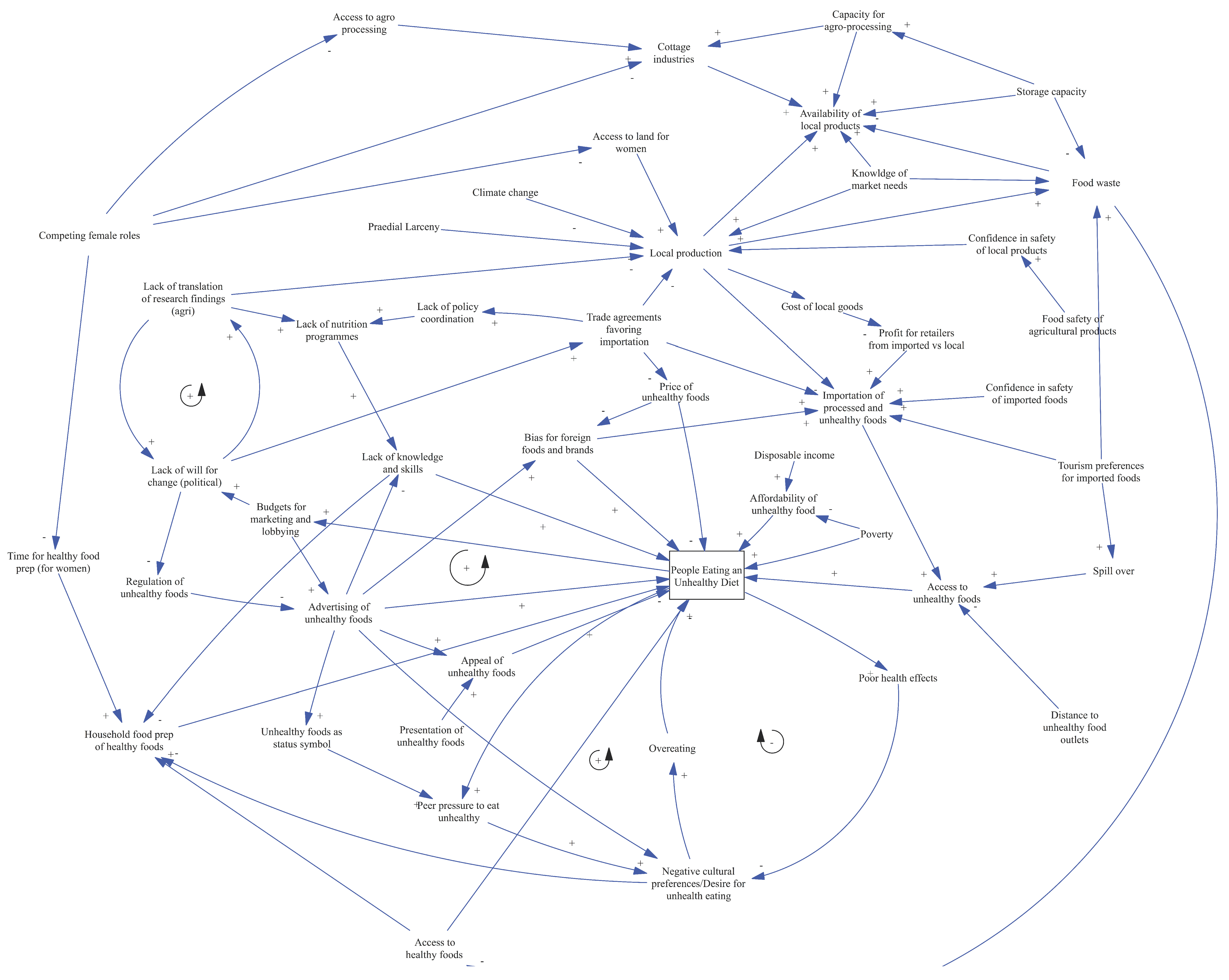
3.1. Drivers of Unhealthy Eating
3.2. Balance of Local/Imported Food Supply
3.3. Gender, Social, Cultural Drivers of Consumption
3.4. Community Engagement
3.5. Government and Policy Coordination
3.6. Assessing Interventions in the System
3.7. Improve Knowledge and Skills for Healthy Eating
3.8. Promote Healthy Eating Environments in Schools
3.9. Coordinate Policy and Fiscal Interventions for Healthy Eating
3.10. Reduce Access to and Promotion of Unhealthy Foods
3.11. Strengthen Local Agriculture
4. Discussion
4.1. Stakeholder Engagement and Perspectives on the Model Building Process
4.2. Principal Findings
4.3. Pathways and Feedbacks to Unhealthy Eating: Aligning with the Global Action Programme
4.3.1. Objective 1: Enabling Environments for Food Security
4.3.2. Objective 2: Sustainable, Resilient, and Nutrition-Sensitive Food Systems That Include the Management and Use of Oceans, Freshwater Resources, and Terrestrial Sources Relying on Local Crops, Sustainable Agricultural Practices, and Efficient Value Chains
4.3.3. Objective 3: Empowered People and Communities for Food Security and Nutrition
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Area to intervene | Votes |
|---|---|
| Price of unhealthy foods, amount of imported unhealthy foods; access to those foods; advertising | 11 |
| Lack of knowledge and information; translation of research findings into practice; technical capacity for sustainable agriculture | 9 |
| Local food supply | 7 |
| Production of healthy foods and local production | 6 |
| Household food preparation | 5 |
| Social drivers and consequences | 5 |
| The choices people make to eat an unhealthy diet | 3 |



| Area for intervention | Key stakeholders |
|---|---|
| Strengthening knowledge, skills, and practice for healthy eating | Government; community champions of healthy eating (including nutritionists; Rastafarians and other religious leaders; educators); community members; consumer groups |
| Promoting healthy eating environments in schools | Government; schools and their staff; children; parents and caregivers; vendors; parent-teacher associations |
| Actions at the community level | Community leaders; local food retailers and distributors (including restaurants, supermarkets, markets); farmers and those engaged in backyard gardening; women’s and men’s groups |
| Tax and fiscal measures | Government; civil society; consumers |
| Limit the influence of unhealthy foods | Government; food distributors and retailers; agricultural sector |
| Strengthen local agriculture | Government; agricultural sector; tourism; community leaders |
References
- List of SIDS. Sustainable Development Knowledge Platform. Available online: https://sustainabledevelopment.un.org/topics/sids/list (accessed on 13 November 2019).
- Small Island Developing States. Sustainable Development Knowledge Platform. Available online: https://sustainsabledevelopment.un.org/topics/sids (accessed on 13 November 2019).
- Country Nutrition Profiles—Global Nutrition Report. Available online: https://globalnutritionreport.org/resources/nutrition-profiles/ (accessed on 13 November 2019).
- Ministry of Health. 2008 STEPwise Approach to Chronic Disease Risk Factor Survey Report a Baseline for Non-Communicable Disease Surveillance in St Kitts; Ministry of Health: St Kitts and Nevis, 2008.
- Under- and Over-Reporting of Energy is Related to Obesity, Lifestyle Factors and Food Group Intakes in Jamaican Adults Public Health Nutrition Cambridge Core. Available online: https://0-www-cambridge-org.brum.beds.ac.uk/core/journals/public-health-nutrition/article/under-and-overreporting-of-energy-is-related-to-obesity-lifestyle-factors-and-food-group-intakes-in-jamaican-adults/26DBC39283FACC6C7884E3C55B6192F3 (accessed on 16 May 2019).
- State of Food Insecurity in the CARICOM Caribbean. Meeting the 2015 Hunger Targets: Taking Stock of Uneven Progress; Food and Agriculture Organization of the United Nations: Bridgetown, Barbados, 2015. [Google Scholar]
- Food and Agriculture Organization of the United Nations. State of Food Security and Nutrition in Small Island Developing States (SIDS); Food and Agriculture Organization: Rome, Italy, 2016. [Google Scholar]
- WHO. World Health Organization—Global Health Observatory. Available online: http://www.who.int/gho/ncd/en/ (accessed on 3 March 2015).
- Sustainable Development Goals. Sustainable Development Knowledge Platform. Available online: https://sustainabledevelopment.un.org/?menu=1300 (accessed on 13 November 2019).
- SAMOA Pathway. Sustainable Development Knowledge Platform. Available online: https://sustainabledevelopment.un.org/sids2014/samoapathway (accessed on 13 November 2019).
- FAO, UN-OHRLLS, UNDESA. Global Action Programme on Food Security and Nutrition in Small Island Developing States; FAO, UN-OHRLLS, UNDESA: New York, NY, USA, 2017. [Google Scholar]
- Declaration of Port-of-Spain: Uniting to Stop the Epidemic of Chronic NCDs. Available online: http://www.caricom.org/jsp/communications/meetings_statements/declaration_port_of_spain_chronic_ncds.jsp (accessed on 11 March 2016).
- Caribbean Unity in Health. The Evaluation of the 2007 CARICOM Heads of Government Port of Spain NCD Summit Declaration; George Alleyne Chronic Disease Research Centre: Bridgetown, Barbados, 2017. [Google Scholar]
- Committee on an Evidence Framework for Obesity Prevention Decision; Food and Nutrition Board; Institute of Medicine. Bridging the Evidence Gap in Obesity Prevention: A Framework to Inform Decision Making; National Academies Press: Washington, DC, USA, 2010; ISBN 978-0-309-14989-1. [Google Scholar]
- A Framework for Assessing Effects of the Food System; National Academies Press: Washington, DC, USA, 2015; ISBN 978-0-309-30780-2.
- Leischow, S.J.; Best, A.; Trochim, W.M.; Clark, P.I.; Gallagher, R.S.; Marcus, S.E.; Matthews, E. Systems thinking to improve the public’s health. Am. J. Prev. Med. 2008, 35, S196–S203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Homer, J.B.; Hirsch, G.B. System Dynamics Modeling for Public Health: Background and Opportunities. Am. J. Public Health 2006, 96, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Finegood, D.T. The Importance of Systems Thinking to Address Obesity. In Nestlé Nutrition Institute Workshop Series; Drewnowski, A., Rolls, B.J., Eds.; S. KARGER AG: Basel, Switzerland, 2012; Volume 73, pp. 123–137. ISBN 978-3-318-02115-8. [Google Scholar]
- Carey, G.; Malbon, E.; Carey, N.; Joyce, A.; Crammond, B.; Carey, A. Systems science and systems thinking for public health: A systematic review of the field. BMJ Open 2015, 5, e009002. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, J.-A.M.; Wells, R.; Page, A.; Dominello, A.; Haines, M.; Wilson, A. Applications of system dynamics modelling to support health policy. Public Health Res. Pract. 2015, 25, e2531531. [Google Scholar] [CrossRef] [PubMed]
- Vennix, J.A.M. Group Model Building: Facilitating Team Learning Using System Dynamics; John Wiley & Sons, Inc: Hoboken, NJ, USA, 1996; ISBN 978-0-471-95355-5. [Google Scholar]
- Waqa, G.; Moodie, M.; Snowdon, W.; Latu, C.; Coriakula, J.; Allender, S.; Bell, C. Exploring the dynamics of food-related policymaking processes and evidence use in Fiji using systems thinking. Health Res. Policy Syst. 2017, 15, 74. [Google Scholar] [CrossRef] [Green Version]
- Rutter, H.; Savona, N.; Glonti, K.; Bibby, J.; Cummins, S.; Finegood, D.T.; Greaves, F.; Harper, L.; Hawe, P.; Moore, L.; et al. The need for a complex systems model of evidence for public health. Lancet 2017, 390, 2602–2604. [Google Scholar] [CrossRef] [Green Version]
- Lee, B.Y.; Bartsch, S.M.; Mui, Y.; Haidari, L.A.; Spiker, M.L.; Gittelsohn, J. A systems approach to obesity. Nutr. Rev. 2017, 75, 94–106. [Google Scholar] [CrossRef]
- Guariguata, L.; Guell, C.; Samuels, T.A.; Rouwette, E.A.J.A.; Woodcock, J.; Hambleton, I.R.; Unwin, N. Systems Science for Caribbean Health: The development and piloting of a model for guiding policy on diabetes in the Caribbean. Health Res. Policy Syst. 2016, 14, 79. [Google Scholar] [CrossRef] [Green Version]
- Henry, F.J.; Caines, D.; Eyre, S. Healthy Eating in Jamaica: The Cost Factor. West Indian Med. J. 2015, 64, 181–185. [Google Scholar]
- Luna-Reyes, L.F.; Martinez-Moyano, I.J.; Pardo, T.A.; Cresswell, A.M.; Andersen, D.F.; Richardson, G.P. Anatomy of a group model-building intervention: Building dynamic theory from case study research. Syst. Dyn. Rev. 2006, 22, 291–320. [Google Scholar] [CrossRef]
- Vensim PLE Software; Ventana Systems, Inc.: Harvard, MA, USA, 2006.
- Rouwette, E.A.; Vennix, J.A.; Mullekom, T.V. Group model building effectiveness: A review of assessment studies. Syst. Dyn. Rev. 2002, 18, 5–45. [Google Scholar] [CrossRef]
- Popkin, B.M. The nutrition transition: An overview of world patterns of change. Nutr. Rev. 2004, 62, S140–S143. [Google Scholar] [CrossRef] [PubMed]
- Allender, S.; Owen, B.; Kuhlberg, J.; Lowe, J.; Nagorcka-Smith, P.; Whelan, J.; Bell, C. A Community Based Systems Diagram of Obesity Causes. PLoS ONE 2015, 10, e0129683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lounsbury, D.W.; Wylie-Rosett, J.; Conlon, B.A. Using Systems Thinking to Understand the Dynamics of Obesity in Low and Middle Income Countries. In Obesity and Disease in an Interconnected World: A Systems Approach to Turn Huge Challenges into Amazing Opportunities; Wylie-Rosett, J.S., Jhangiani, S., Eds.; Bentham Science Publishers: Sharjah, United Arab Emirates, 2015; pp. 306–325. ISBN 978-1-68108-036-9. [Google Scholar]
- Friel, S.; Pescud, M.; Malbon, E.; Lee, A.; Carter, R.; Greenfield, J.; Cobcroft, M.; Potter, J.; Rychetnik, L.; Meertens, B. Using systems science to understand the determinants of inequities in healthy eating. PLoS ONE 2017, 12, e0188872. [Google Scholar] [CrossRef]
- Brennan, L.K.; Sabounchi, N.S.; Kemner, A.L.; Hovmand, P. Systems Thinking in 49 Communities Related to Healthy Eating, Active Living, and Childhood Obesity. J. Public Health Manag. Pract. 2015, 21, S55–S69. [Google Scholar] [CrossRef]
- Johnston, L.M.; Matteson, C.L.; Finegood, D.T. Systems Science and Obesity Policy: A Novel Framework for Analyzing and Rethinking Population-Level Planning. Am. J. Public Health 2014, 104, 1270–1278. [Google Scholar] [CrossRef]
- Thomas, I.M.; Reilly, S.R. Group Model Building: A Framework for Organizing Healthy Community Program and Policy Initiatives in Columbia, Missouri. J. Public Health Manag. Pract. 2015, 21, S79–S83. [Google Scholar] [CrossRef]
- Keane, P.; Ortega, A.; Linville, J. Healthy Kids, Healthy Cuba: Findings from a group model building process in the rural Southwest. J. Public Health Manag. Pract. 2015, 21 (Suppl. 3), S70–S73. [Google Scholar] [CrossRef]
- Frerichs, L.; Hassmiller Lich, K.; Young, T.L.; Dave, G.; Stith, D.; Corbie-Smith, G. Development of a Systems Science Curriculum to Engage Rural African American Teens in Understanding and Addressing Childhood Obesity Prevention. Health Educ. Behav. 2018, 45, 423–434. [Google Scholar] [CrossRef]
- Majowicz, S.E.; Meyer, S.B.; Kirkpatrick, S.I.; Graham, J.L.; Shaikh, A.; Elliott, S.J.; Minaker, L.M.; Scott, S.; Laird, B. Food, health, and complexity: Towards a conceptual understanding to guide collaborative public health action. BMC Public Health 2016, 16, 487. [Google Scholar] [CrossRef]
- Hovmand, P. Community Based System Dynamics; Springer Science & Business Media: Berlin, Germany, 2013; ISBN 978-1-4614-8763-0. [Google Scholar]
- Forrester, J.; Cook, B.; Bracken, L.; Cinderby, S.; Donaldson, A. Combining participatory mapping with Q-methodology to map stakeholder perceptions of complex environmental problems. Appl. Geogr. 2015, 56, 199–208. [Google Scholar] [CrossRef] [Green Version]
- Willis, C.D.; Mitton, C.; Gordon, J.; Best, A. System tools for system change. BMJ Qual. Saf. 2012, 21, 250. [Google Scholar] [CrossRef]
- Peters, B.G. The challenge of policy coordination. Policy Des. Pract. 2018, 1, 1–11. [Google Scholar] [CrossRef]
- Hawley, N.L.; McGarvey, S.T. Obesity and Diabetes in Pacific Islanders: The Current Burden and the Need for Urgent Action. Curr. Diabetes Rep. 2015, 15, 29. [Google Scholar] [CrossRef]
- Samuels, T.A.; Guell, C.; Legetic, B.; Unwin, N. Policy initiatives, culture and the prevention and control of chronic non-communicable diseases (NCDs) in the Caribbean. Ethn. Health 2012, 17, 631–649. [Google Scholar] [CrossRef]
- Food and Agriculture Organization of the United Nations; Caribbean Development Bank. Study on the State of Agriculture in the Caribbean; Food and Agriculture Organization: Rome, Italy, 2019; ISBN 978-92-5-131488-3. [Google Scholar]
- Siokou, C.; Morgan, R.; Shiell, A. Group model building: A participatory approach to understanding and acting on systems. Public Health Res. Pract. 2014, 25, e2511404. [Google Scholar] [CrossRef] [Green Version]



| Country | Prevalence of Stunting in Children under 5 (%) | Child and Adolescent Underweight (5–19 Years) (%) (F/M) | Child and Adolescent Overweight (5–19 Years) (%) (F/M) | Adult Overweight (%) (F/M) | Anemia in Women of Reproductive Age (15–49 Years) (%) | NCD Deaths Occurring under 70 Years (%) * |
|---|---|---|---|---|---|---|
| Jamaica | 7 | 14.4/14.9 | 30.4/29.2 | 63.2/47.4 | 22.5 | 31 |
| St Kitts and Nevis | No data | 16.2/17.3 | 28.1/27.8 | 59.3/45 | No data | No data |
| St Vincent and the Grenadines | No data | 16.1/16.7 | 29.2/28.9 | 61.1/48.9 | 24.5 | 44 |
| Country | Government | Private Sector | Civil Society | Regional Agencies |
|---|---|---|---|---|
| Jamaica | Agriculture, industry and commerce n = 4 | Restaurant n = 1; Food distributors n = 2; Export and trade n = 1 | Vendors association n = 2; Market and vendors unions n = 3; Food production n = 1; Religious n = 2 | |
| St Kitts and Nevis | Agriculture n = 1; Health and gender n = 6; Education n = 1; Foreign affairs n = 1 | Agriculture n = 2 | Religious n = 1; Agriculture and food retailers n = 2; civil society n = 2 | Agriculture n = 2; Health n = 1 |
| St Vincent and the Grenadines | Health n = 1; Foreign affairs and trade n = 1 | Restaurant n = 1; Export and trade n = 1 | Religious n = 1; Agriculture and food production n = 1 |
| Area of Intervention | Leverage Points | Key Stakeholders | Intervention Examples |
|---|---|---|---|
| Improve knowledge and skills for healthy eating | Translate research findings into policy and practice; Promote healthy eating skills in communities; Promote sustainable agriculture; Connect communities to agriculture | Agricultural sector; Education; Government; Academia; Communications and media | Training on food preparation for households; Training on sustainable best practice for agriculture; Promote local agriculture through media campaigns |
| Promote health eating environments in schools | Limit unhealthy foods in schools; Promote child-friendly education on healthy eating; Create networks between school community and agriculture | Community leaders; Civil society; Education | Farm-to-school schemes for including local products; Engaging food vendors on healthy options; Policies limiting unhealthy food in schools |
| Coordinate policy and fiscal interventions for healthy eating | Coordinate policies across sectors; Engage in public-private partnerships; Earmark taxes on unhealthy foods for promoting agriculture and treatment of NCDs | Government; Agricultural sector | Establish and maintain networks across government sectors; Creation of regional coordinating bodies |
| Reduce access to and promotion of unhealthy foods | Increase prices of unhealthy foods through fiscal measures; Limits on amount of imported unhealthy foods; Limit advertising of unhealthy foods | Government; civil society; Consumers; private sector | Implement fiscal measures to tax unhealthy foods and subsidize healthy local foods; Regional standards for food labeling |
| Strengthen local agriculture | Build technical and infrastructure capacity for agriculture; Strengthen the role of women in agriculture; Promote coordination networks from farm to market | Agricultural sector; Government; Gender specialists; Civil society | Build and maintain infrastructure to support agriculture; Use digital platforms to connect agricultural producers to food retailers |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guariguata, L.; Rouwette, E.A.; Murphy, M.M.; Saint Ville, A.; Dunn, L.L.; Hickey, G.M.; Jones, W.; Samuels, T.A.; Unwin, N. Using Group Model Building to Describe the System Driving Unhealthy Eating and Identify Intervention Points: A Participatory, Stakeholder Engagement Approach in the Caribbean. Nutrients 2020, 12, 384. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12020384
Guariguata L, Rouwette EA, Murphy MM, Saint Ville A, Dunn LL, Hickey GM, Jones W, Samuels TA, Unwin N. Using Group Model Building to Describe the System Driving Unhealthy Eating and Identify Intervention Points: A Participatory, Stakeholder Engagement Approach in the Caribbean. Nutrients. 2020; 12(2):384. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12020384
Chicago/Turabian StyleGuariguata, Leonor, Etiënne AJA Rouwette, Madhuvanti M Murphy, Arlette Saint Ville, Leith L Dunn, Gordon M Hickey, Waneisha Jones, T Alafia Samuels, and Nigel Unwin. 2020. "Using Group Model Building to Describe the System Driving Unhealthy Eating and Identify Intervention Points: A Participatory, Stakeholder Engagement Approach in the Caribbean" Nutrients 12, no. 2: 384. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12020384