Gestational Diabetes Mellitus Treatment Schemes Modify Maternal Plasma Cholesterol Levels Dependent to Women´s Weight: Possible Impact on Feto-Placental Vascular Function

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. GDM Diagnosis and Treatment
2.3. Determination of Lipid Profiles
2.4. High Cholesterol Cut-Off Value
2.5. Umbilical Vein Reactivity
2.6. Data Analysis
3. Results
3.1. Clinical Characteristics of the Participants
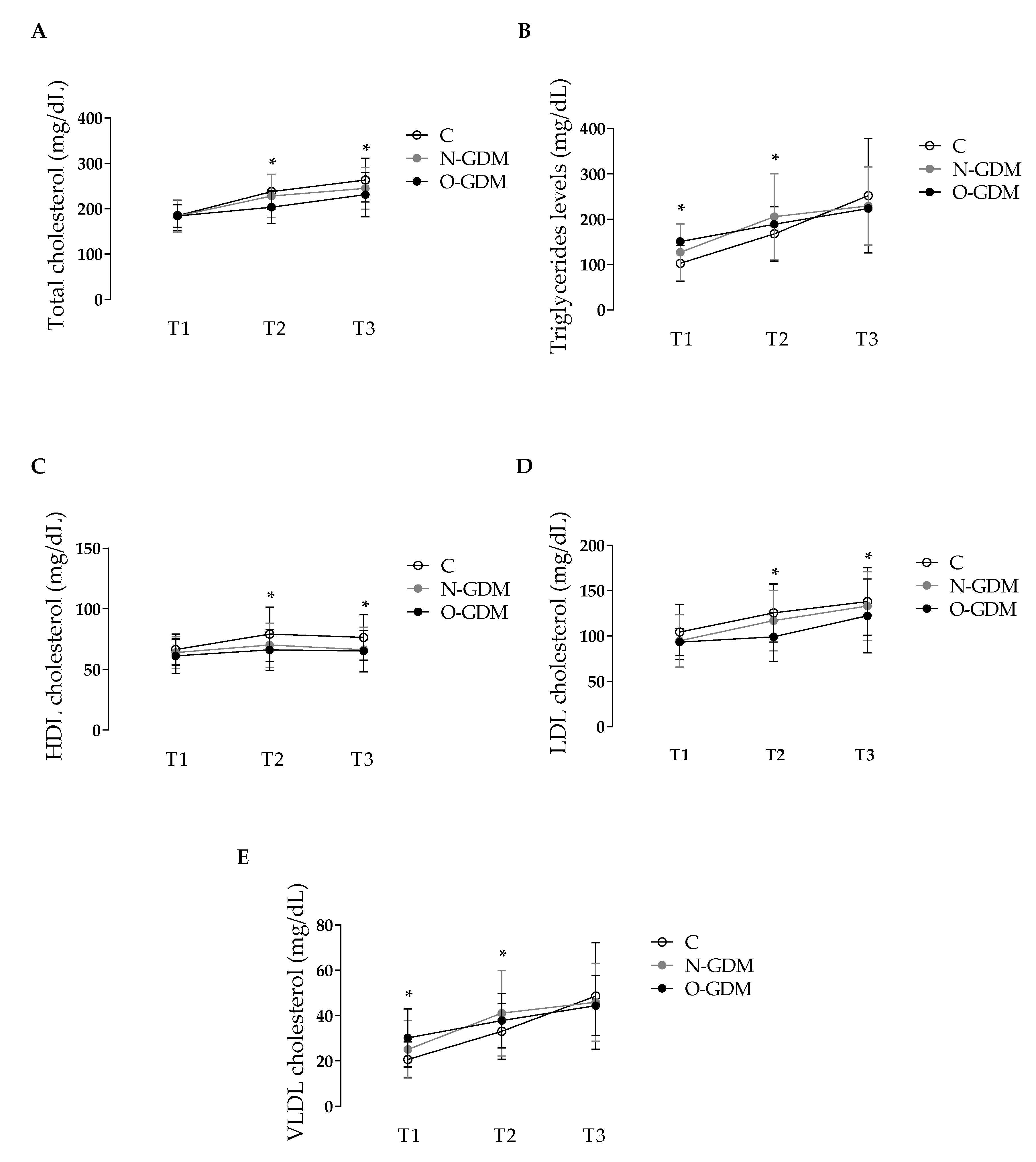
3.2. Effects of Obesity and GDM on the Lipid Profile of Pregnant Women
3.3. Correlation Between Maternal BMI and Lipid Levels
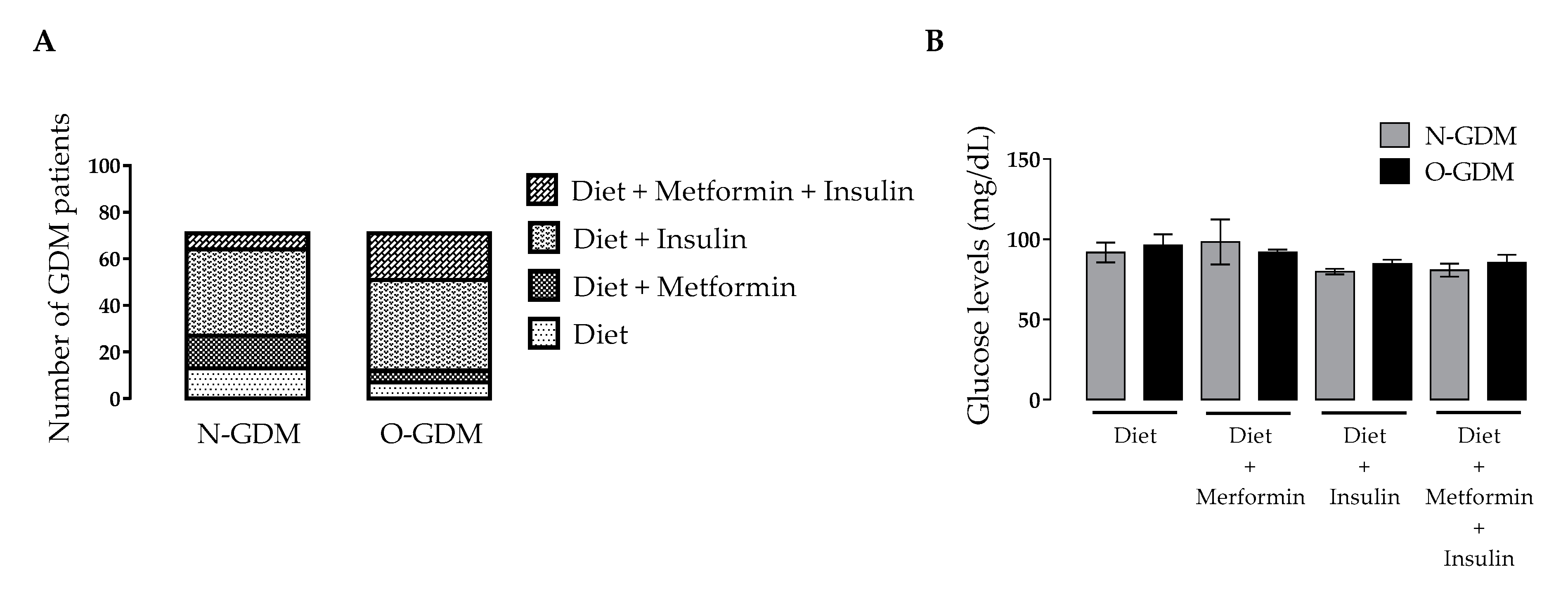
3.4. Effect of GDM Treatments on Glycemic Control
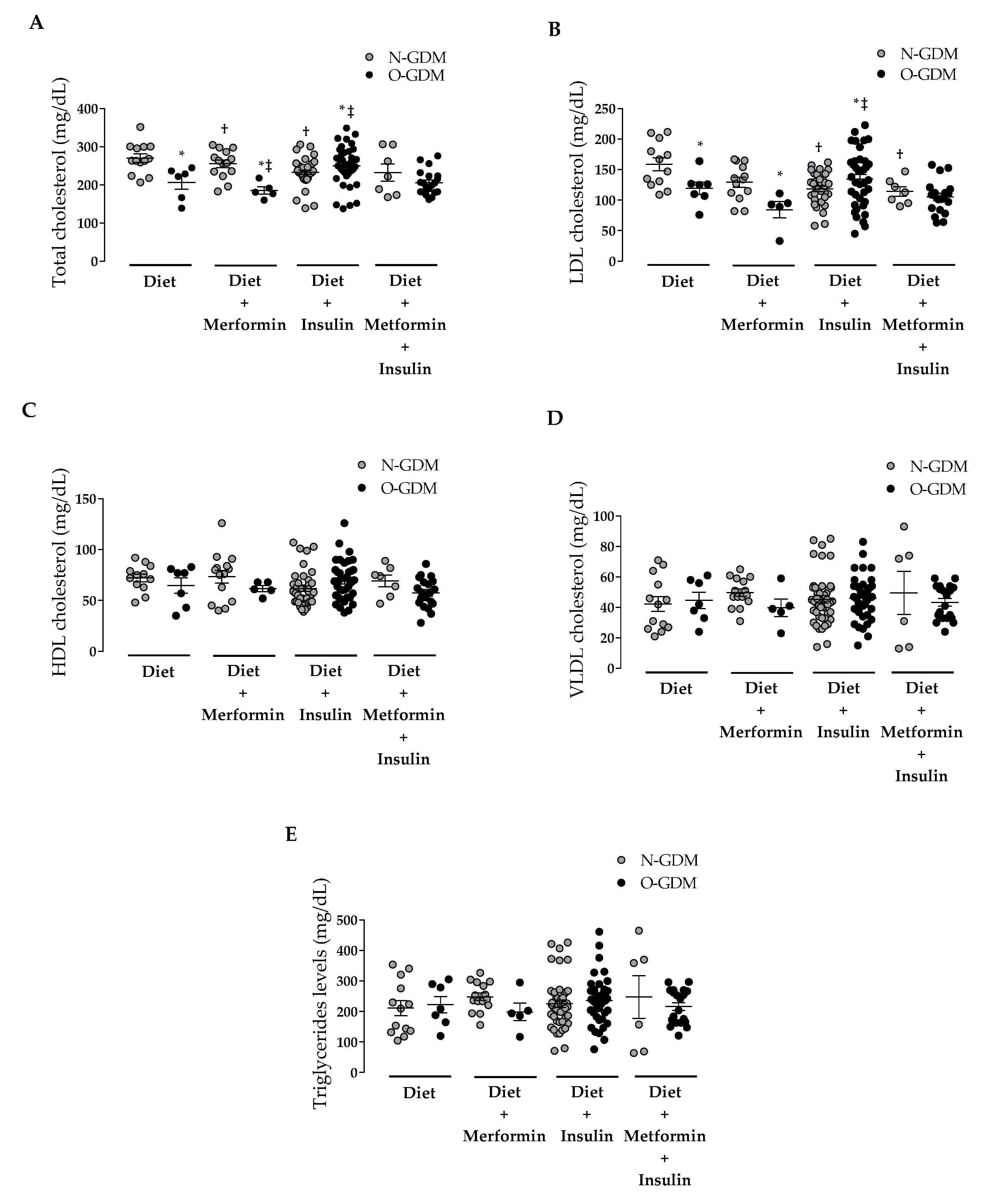
3.5. Effect of GDM Treatment on Lipid Levels
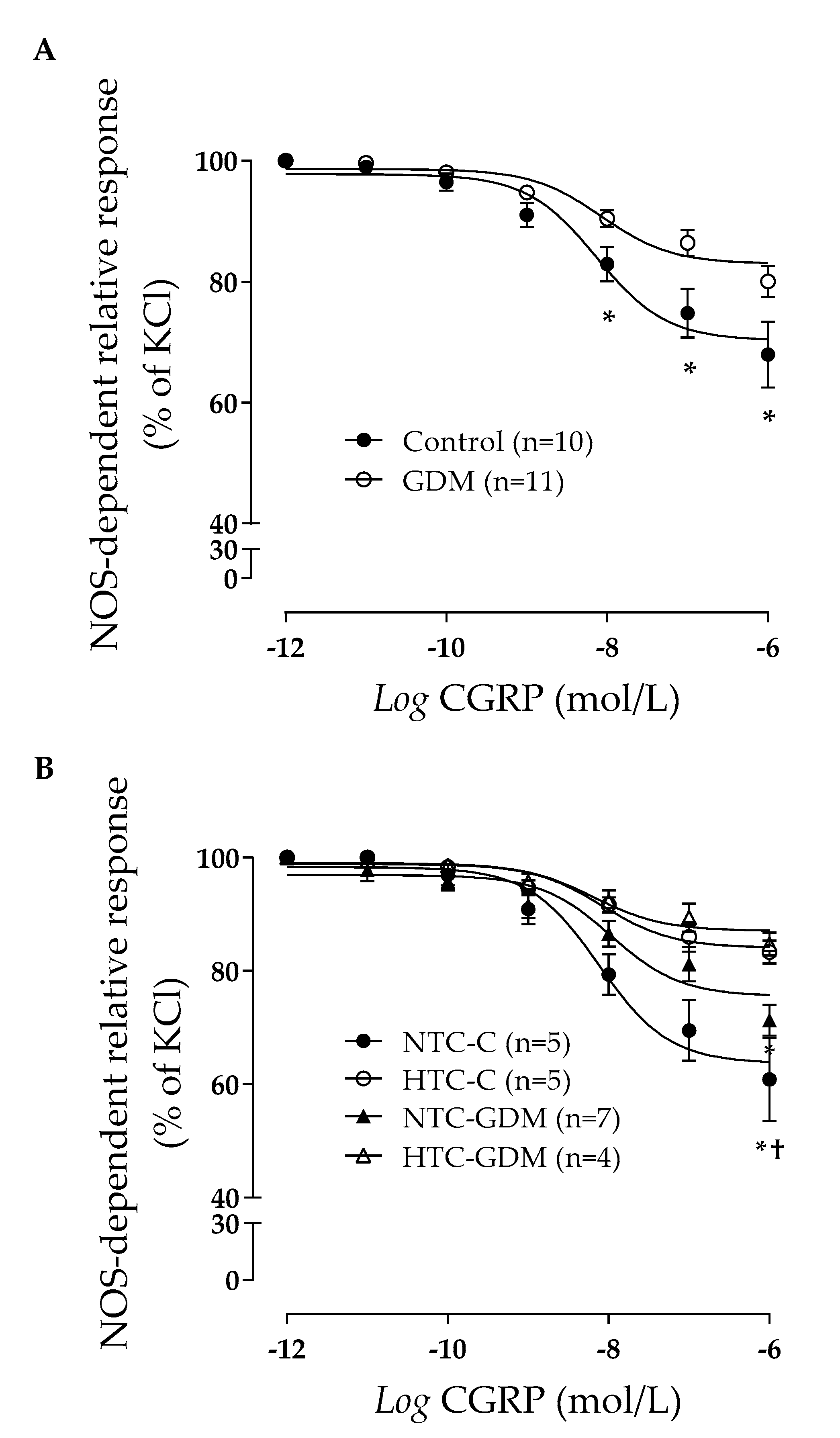
3.6. Effect of GDM and Maternal Lipids on Human Umbilical Vein Reactivity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association. Classification and diagnosis of diabetes. Diabetes Care 2017, 40, S11–S24. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Diagnostic criteria and classification of hyperglycaemia first detected in pregnancy. Diabetes Res. Clin. Pract. 2013, 103, 341–363. [Google Scholar]
- Metzger, B.; Lowe, L.; Dyer, A.; Trimble, E.; Chaovarindr, U.; Coustan, D.; Hadden, D.; McCance, D.; Hod, M.; McIntyre, H.; et al. Hyperglycemia and adverse pregnancy outcomes. HAPO Study Cooperative Research Group. N. Engl. J. Med. 2008, 358, 1991–2002. [Google Scholar] [PubMed] [Green Version]
- Kjos, S.; Buchanan, T. Gestational diabetes mellitus. N. Engl. J. Med. 1999, 341, 1749–1756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, S.; Callaghan, W.; Kim, S.; Schmid, C.; Lau, J.; England, L.; Dietz, P. Maternal obesity and risk of gestational diabetes mellitus. Diabetes Care 2007, 30, 2070–2076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kongubol, A.; Phupong, V. Prepregnancy obesity and the risk of gestational diabetes mellitus. BMC Pregnancy Childbirth 2011, 10, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padmanabhan, S.; Wagstaff, A.; Tung, V.; Chan, Y.; Bartlett, A.; Lau, S.M. Increase in body mass index during pregnancy and risk of gestational diabetes. Diabetes Res. Clin. Pract. 2014, 106, e79–e82. [Google Scholar] [CrossRef]
- Colomiere, M.; Permezel, M.; Riley, C.; Desoye, G.; Lappas, M. Defective insulin signaling in placenta from pregnancies complicated by gestational diabetes mellitus. Eur. J. Endocrinol. 2009, 160, 567–578. [Google Scholar] [CrossRef] [Green Version]
- Guzmán-Gutiérrez, E.; Arroyo, P.; Salsoso, R.; Fuenzalida, B.; Sáez, T.; Leiva, A.; Pardo, F.; Sobrevia, L. Role of insulin and adenosine in the human placenta microvascular and macrovascular endothelial cell dysfunction in gestational diabetes mellitus. Microcirculation 2014, 21, 26–37. [Google Scholar] [CrossRef]
- Haas, T. Shaping and remodeling of the fetoplacental circulation: Aspects of health and disease. Microcirculation 2014, 21, 1–3. [Google Scholar] [CrossRef]
- Subiabre, M.; Silva, L.; Villalobos-Labra, R.; Toledo, F.; Paublo, M.; López, M.A.; Salsoso, R.; Pardo, F.; Leiva, A.; Sobrevia, L. Maternal insulin therapy does not restore foetoplacental endothelial dysfunction in gestational diabetes mellitus. Biochim. Biophys. Acta Mol. Basis Dis. 2017, 1863, 2987–2998. [Google Scholar] [CrossRef] [PubMed]
- Bayraktar, F.; Akinci, B.; Celtik, A.; Tunali, S.; Genc, S.; Ozcan, M.A.; Secil, M.; Yesil, S. Insulin need in gestational diabetes is associated with a worse cardiovascular risk profile after pregnancy. Intern. Med. 2012, 51, 839–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savvidou, M.; Anderson, J.; Kaihura, C.; Nicolaides, K. Maternal arterial stiffness in pregnancies complicated by gestational and type 2 diabetes mellitus. Am. J. Obstet. Gynecol. 2010, 203, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Mrizak, I.; Arfa, A.; Fekih, M.; Debbabi, H.; Bouslema, A.; Boumaiza, I.; Zaouali, M.; Khan, N.A.; Tabka, Z. Inflammation and impaired endothelium-dependant vasodilatation in non obese women with gestational diabetes mellitus: Preliminary results. Lipids Health Dis. 2013, 12, 93. [Google Scholar] [CrossRef] [Green Version]
- Ryckman, K.; Spracklen, C.; Smith, C.; Robinson, J.; Saftlas, A. Maternal lipid levels during pregnancy and gestational diabetes: A systematic review and meta-analysis. BJOG 2015, 122, 643–651. [Google Scholar] [CrossRef]
- Contreras-Duarte, S.; Carvajal, L.; Fuenzalida, B.; Cantin, C.; Sobrevia, L.; Leiva, A. Maternal Dyslipidaemia in Pregnancy with Gestational Diabetes Mellitus: Possible Impact on Foetoplacental Vascular Function and Lipoproteins in the Neonatal Circulation. Curr. Vasc. Pharmacol. 2019, 17, 52–71. [Google Scholar] [CrossRef]
- Akinci, B.; Celtik, A.; Genc, S.; Yener, S.; Demir, T.; Secil, M.; Kebapcilar, L.; Yesil, S. Evaluation of postpartum carbohydrate intolerance and cardiovascular risk factors in women with gestational diabetes. Gynecol. Endocrinol. 2011, 27, 361–367. [Google Scholar] [CrossRef]
- Metzger, B. Long-term outcomes in mothers diagnosed with gestational diabetes mellitus and their offspring. Clin. Obstet. Gynecol. 2007, 50, 972–979. [Google Scholar] [CrossRef]
- Daly, B.; Toulis, K.; Thomas, N.; Gokhale, K.; Martin, J.; Webber, J.; Keerthy, D.; Jolly, K.; Saravanan, P.; Nirantharakumar, K. Increased risk of ischemic heart disease, hypertension, and type 2 diabetes in women with previous gestational diabetes mellitus, a target group in general practice for preventive interventions: A population-based cohort study. PLoS Med. 2018, 15, e1002488. [Google Scholar] [CrossRef] [Green Version]
- McKenzie-Sampson, S.; Paradis, G.; Healy-Profitós, J.; St-Pierre, F.; Auger, N. Gestational diabetes and risk of cardiovascular disease up to 25 years after pregnancy: A retrospective cohort study. Acta Diabetol. 2018, 55, 315–322. [Google Scholar] [CrossRef]
- Olmos, P.; Rigotti, A.; Busso, D.; Berkowitz, L.; Santos, J.; Borzone, G.; Poblete, J.; Vera, C.; Belmar, C.; Goldenberg, D.; et al. Maternal hypertriglyceridemia: A link between maternal overweight-obesity and macrosomia in gestational diabetes. Obesity 2014, 22, 2156–2163. [Google Scholar] [CrossRef] [PubMed]
- Subiabre, M.; Silva, L.; Toledo, F.; Paublo, M.; López, M.; Boric, M.; Sobrevia, L. Insulin therapy and its consequences for the mother, foetus, and newborn in gestational diabetes mellitus. Biochim. Biophys. Acta Mol. Basis Dis. 2018, 1864, 2949–2956. [Google Scholar] [CrossRef] [PubMed]
- Leiva, A.; de Medina, C.; Salsoso, R.; Sáez, T.; San Martín, S.; Abarzúa, F.; Farías, M.; Guzmán-Gutiérrez, E.; Pardo, F.; Sobrevia, L. Maternal hypercholesterolemia in pregnancy associates with umbilical vein endothelial dysfunction: Role of endothelial nitric oxide synthase and arginase II. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 2444–2453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leiva, A.; Fuenzalida, B.; Westermeier, F.; Toledo, F.; Salomón, C.; Gutiérrez, J.; Sanhueza, C.; Pardo, F.; Sobrevia, L. Role for tetrahydrobiopterin in the fetoplacental endothelial dysfunction in maternal supraphysiological hypercholesterolemia. Oxid. Med. Cell. Longev. 2015, 2015, 5346327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leiva, A.; Fuenzalida, B.; Salsoso, R.; Barros, E.; Toledo, F.; Gutiérrez, J.; Pardo, F.; Sobrevia, L. Tetrahydrobiopterin Role in human umbilical vein endothelial dysfunction in maternal supraphysiological hypercholesterolemia. Biochim. Biophys. Acta 2016, 1862, 536–544. [Google Scholar] [CrossRef]
- Marzioni, D.; Tamagnone, L.; Capparuccia, L.; Marchini, C.; Amici, A.; Todros, T.; Bischof, P.; Neidhart, S.; Grenningloh, G.; Castellucci, M. Restricted innervation of uterus and placenta during pregnancy: Evidence for a role of the repelling signal Semaphorin 3A. Dev. Dyn. 2004, 231, 839–848. [Google Scholar] [CrossRef]
- Fuenzalida, B.; Sobrevia, B.; Cantin, C.; Carvajal, L.; Salsoso, R.; Gutiérrez, J.; Contreras-Duarte, S.; Sobrevia, L.; Leiva, A. Maternal supraphysiological hypercholesterolemia associates with endothelial dysfunction of the placental microvasculature. Sci. Rep. 2018, 8, 7690. [Google Scholar] [CrossRef]
- IOM. Weight Gain during Pregnancy: Reexamining the Guidelines; Institute of Medicine (us) and National research Council (us) and Committee To Reexamine iom Pregnancy Weight Guidelines; The National Academies Press: Cambridge, MA, USA, 2009. [Google Scholar]
- Taskinen, M.; Borén, J. New insights into the pathophysiology of dyslipidemia in type 2 diabetes. Atherosclerosis 2015, 239, 483–495. [Google Scholar] [CrossRef]
- Barrett, H.; Dekker Nitert, M.; McIntyre, H.; Callaway, L. Normalizing metabolism in diabetic pregnancy: Is it time to target lipids? Diabetes Care 2014, 37, 1484–1493. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, E.; Pawlak, D.; Takoudes, T.; Ebbeling, C.; Feldman, H.; Lovesky, M.; Cooke, E.; Leidig, M.; Ludwig, D. Effects of a low-glycemic load diet in overweight and obese pregnant women: A pilot randomized controlled trial. Am. J. Clinl. Nutr. 2010, 92, 1306–1315. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Jiang, H.; Yang, L.; Zhang, M. Impacts of dietary fat changes on pregnant women with gestational diabetes mellitus: A randomized controlled study. Asia. Pac. J. Clin. Nutr. 2015, 24, 58–64. [Google Scholar] [PubMed]
- Asemi, Z.; Samimi, M.; Tabassi, Z.; Sabihi, S.; Esmaillzadeh, A. A randomized controlled clinical trial investigating the effect of DASH diet on insulin resistance, inflammation, and oxidative stress in gestational diabetes. Nutrition 2013, 29, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Tabassi, Z.; Samimi, M.; Fahiminejad, T.; Esmaillzadeh, A. Favourable effects of the dietary approaches to stop hypertension diet on glucose tolerance and lipid profiles in gestational diabetes: A randomised clinical trial. Br. J. Nutr. 2013, 109, 2024–2030. [Google Scholar] [CrossRef] [PubMed]
- Jamilian, M.; Asemi, Z. The effect of soy intake on metabolic profiles of women with gestational diabetes mellitus. J. Clin. Endocrinol. Metab. 2015, 100, 4654–4661. [Google Scholar] [CrossRef]
- Magee, M.; Knopp, R.; Benedetti, T. Metabolic effects of 1200-kcal diet in obese pregnant women with gestational diabetes. Diabetes 1990, 39, 234–240. [Google Scholar] [CrossRef]
- Barrett, H.; Dekker Nitert, M.; Jones, L.; O’Rourke, P.; Lust, K.; Gatford, K.; De Blasio, M.; Coat, S.; Owens, J.; Hague, W.; et al. Determinants of maternal triglycerides in women with gestational diabetes mellitus in the Metformin in Gestational Diabetes (MiG) study. Diabetes Care 2013, 36, 1941–1946. [Google Scholar] [CrossRef] [Green Version]
- Barrett, H.; Gatford, K.; Houda, C.; De Blasio, M.; McIntyre, H.; Callaway, L.; Dekker Nitert, M.; Coat, S.; Owens, J.; Hague, W.; et al. Maternal and neonatal circulating markers of metabolic and cardiovascular risk in the metforminin gestational diabetes (MiG) trial: Responses to maternal metformin versus insulin treatment. Diabetes Care 2013, 36, 529–536. [Google Scholar] [CrossRef] [Green Version]
- Zawiejska, A.; Wender-Ozegowska, E.; Grewling-Szmit, K.; Brazert, M.; Brazert, J. Short-term antidiabetic treatment with insulin or metformin has a similar impact on the components of metabolic syndrome in women with gestational diabetes mellitus requiring antidiabetic agents: Results of a prospective, randomised study. J. Physiol. Pharmacol. 2016, 67, 227–233. [Google Scholar]
- Krishnamoorthy, U.; Schram, C.; Hill, S. Maternal obesity in pregnancy: Is it time for meaningful research to inform preventive and management strategies? BJOG 2006, 113, 1134–1140. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Task Force on Hypertension in Pregnancy. Obstet. Gynecol. 2013, 122, 1122–1131. [Google Scholar]
- American Diabetes Association. Standars of medical care in diabetes. Diabetes Care 2013, 36, S11–S66. [Google Scholar]
- American Diabetes Association. Standards of Medical Care in Diabetes Summary of Revisions. Diabetes Care 2015, 38, S4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnell, Z.; Leeuwen, A.; Kranpitz, T. Davis’s Comprehensive Laboratory and Diagnostic Test Handbook-with Nursing Implications, 2nd ed.; F.A. Davis Company: Philadelphia, PA, USA, 2006; pp. 1–1804. [Google Scholar]
- Ozcimen, E.; Uckuyu, A.; Ciftci, F.; Yanik, F.; Bakar, C. Diagnosis of gestational diabetes mellitus by use of the homeostasis model assessment-insulin resistance index in the first trimester. Gynecol. Endocrinol. 2008, 24, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.; Hosker, J.; Rudenski, A.; Naylor, B.; Treacher, D.; Turner, R. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buccini, G.; Wolfthal, D. Valores de corte para índices de insulinorresistencia, inmunosensibilidad e insulinosecreción derivados de la fórmula HOMA y del programa HOMA2. Interpretación de los datos. RAEM 2008, 45, 3–21. [Google Scholar]
- Wallace, T.; Levy, J.; Matthews, D. Use and Abuse of HOMA Modeling. Diabetes Care 2004, 27, 61487–61495. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Clinical Excellence. Diabetes in Pregnancy: Management of Diabetes and Its Complications from Preconception to the Postnatal Period; RCOG Press: London, UK, 2008. [Google Scholar]
- Ministerio de salud. Guía Perinatal, Gobierno de Chile 2015; Ministerio de salud: Santiago, Chile, 2015; pp. 1–466. [Google Scholar]
- Olmos, P.; Borzone, G. Basal-bolus insulin therapy reduces maternal triglycerides in gestational diabetes without modifying cholesteryl ester transfer protein activity. Obstet. Gynaecol. Res. 2017, 43, 1397–1404. [Google Scholar] [CrossRef]
- Napoli, C.; D’Armiento, F.; Mancini, F.; Postiglione, A.; Witztum, J.; Palumbo, G.; Palinski, W. Fatty streak formation occurs in human fetal aortas and is greatly enhanced by maternal hypercholesterolemia. Intimal accumulation of low density lipoprotein and its oxidation precede monocyte recruitment into early atherosclerotic lesions. Clin. Investig. 1997, 100, 2680–2690. [Google Scholar] [CrossRef]
- Napoli, C.; Glass, C.; Witztum, J.; Deutsch, R.; D’Armiento, F.; Palinski, W. Influence of maternal hypercholesterolaemia during pregnancy on progression of early atherosclerotic lesions in childhood: Fate of Early Lesions in Children (FELIC) study. Lancet 1999, 354, 1234–1241. [Google Scholar] [CrossRef]
- Liguori, A.; D’Armiento, F.; Palagiano, A.; Balestrieri, M.; Williams-Ignarro, S.; de Nigris, F.; Lerman, L.; D’Amora, M.; Rienzo, M.; Fiorito, C.; et al. Effect of gestational hypercholesterolaemia on omental vasoreactivity, placental enzyme activity and transplacental passage of normal and oxidised fatty acids. BJOG 2007, 114, 1547–1556. [Google Scholar] [CrossRef]
- Marseille-Tremblay, C.; Ethier-Chiasson, M.; Forest, J.; Giguère, Y.; Masse, A.; Mounier, C.; Lafond, J. Impact of maternal circulating cholesterol and gestational diabetes mellitus on lipid metabolism in human term placenta. Mol. Reprod. Dev. 2008, 75, 1054–1062. [Google Scholar] [CrossRef]
- Zhang, R.; Dong, S.; Ma, W.; Cai, X.; Le, Z.; Xiao, R.; Zhou, Q.; Yu, H. Modulation of cholesterol transport by maternal hypercholesterolemia in human full-term placenta. PLoS ONE 2017, 12, e0171934. [Google Scholar] [CrossRef] [PubMed]
- Knopp, R.; Magee, M.; Raisys, V.; Benedetti, T.; Bonet, B. Hypocaloric diets and ketogenesis in the management of obese gestational diabetic women. J. Am. Coll Nutr. 1991, 10, 649–667. [Google Scholar] [CrossRef]
- Metzger, B.; Freinkel, N. Accelerated starvation in pregnancy: Implications for dietary treatment of obesity and gestational diabetes mellitus. Biol. Neonate 1987, 51, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Belmar, C.; Salinas, P.; Becker, J.; Abarzua, F.; Olmos, P.; Gonzalez, P.; Oyarzun, E. Incidence of gestational diabetes according to two diagnostic criteria and its clinical impact. Rev. Chil. Obstet. Gynecol. 2004, 69, 2–7. [Google Scholar]
- Zhou, T.; Sun, D.; Li, X.; Heianza, Y.; Nisa, H.; Hu, G.; Pei, X.; Shang, X.; Qi, L. Prevalence and trends in gestational diabetes mellitus among women in the united states, 2006–2016. Diabetes 2018, 67, S1. [Google Scholar] [CrossRef]
- Hirst, J.; Raynes-Greenow, C.; Jeffery, H. A systematic review of trends of gestational diabetes mellitus in Asia. J. Diabetol. 2012, 3, 5. [Google Scholar]
- Nguyen, C.; Pham, N.; Binns, C.; Duong, D.; Lee, A. Prevalence of gestational diabetes mellitus in eastern and southeastern asia: A systematic review and meta-analysis. J. Diabetes Res. 2018, 20, 6536974. [Google Scholar] [CrossRef] [Green Version]
- Macaulay, S.; Dunger, D.; Norris, S. Gestational diabetes mellitus in Africa: A systematic review. PLoS ONE 2014, 9, e97871. [Google Scholar] [CrossRef]
- Melchior, H.; Kurch-Bek, D.; Mund, M. The Prevalence of Gestational Diabetes. Dtsch. Arztebl. Int. 2017, 114, 412–418. [Google Scholar]
- Després, J. The insulin resistancedyslipidemic syndrome of visceral obesity: Effect on patients’ risk. Obes. Res. 1998, 6, 8S–17S. [Google Scholar] [CrossRef] [PubMed]
- Kahn, B.; Flier, J. Obesity and insulin resistance. J. Clin. Investig. 2000, 106, 473–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, J. Mechanisms of insulin resistance in obesity. Front. Med. 2013, 7, 14–24. [Google Scholar] [CrossRef] [Green Version]
- Hardy, O.; Czech, M.; Corvera, S. What causes the insulin resistance underlying obesity? Curr. Opin. Endocrinol. Diabetes Obes. 2012, 19, 81–87. [Google Scholar] [CrossRef] [Green Version]
- Kc, K.; Shakya, S.; Zhang, H. Gestational diabetes mellitus and macrosomia: A literature review. Ann. Nutr. Metab. 2015, 66, 14–20. [Google Scholar] [CrossRef]
- Plows, J.; Stanley, J.; Baker, P.; Reynolds, C.; Vickers, M. The pathophysiology of gestational diabetes mellitus. Int. J. Mol. Sci. 2018, 19, 3342. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, R.; Gruppuso, P.; Petzold, K.; Brambilla, D.; Hiilesmaa, V.; Teramo, K. Hyperinsulinemia and macrosomia in the fetus of the diabetic mother. Diabetes Care 1994, 17, 640–648. [Google Scholar] [CrossRef]
- Ryan, D.; Haddow, L.; Ramaesh, A.; Kelly, R.; Johns, E.; Denison, F.; Dover, A.; Reynolds, R. Early screening and treatment of gestational diabetes in high-risk women improves maternal and neonatal outcomes: A retrospective clinical audit. Diabetes Res. Clin. Pract. 2018, 144, 294–301. [Google Scholar] [CrossRef]
- Desoye, G.; Schweditsch, M.; Pfeiffer, K.; Zechner, R.; Kostner, G. Correlation of hormones with lipid and lipoprotein levels during normal pregnancy and postpartum. J. Clin. Endocrinol. Metab. 1987, 64, 704–712. [Google Scholar] [CrossRef]
- Herrera, E.; Amusquivar, E.; López-Soldado, I.; Ortega, H. Maternal lipid metabolism and placental lipid transfer. Horm. Res. 2006, 65, 59–64. [Google Scholar] [CrossRef]
- Herrera, E.; Desoye, G. Maternal and fetal lipid metabolism under normal and gestational diabetic conditions. Horm. Mol. Biol. Clin. Investig. 2016, 26, 109–127. [Google Scholar] [CrossRef] [PubMed]
- Knopp, R.; Warth, M.; Charles, D.; Childs, M.; Li, J.; Mabuchi, H.; Van Allen, M. Lipoprotein metabolism in pregnancy, fat transport to the fetus, and the effects of diabetes. Biol. Neonate 1986, 50, 297–317. [Google Scholar] [CrossRef] [PubMed]
- Geraghty, A.; Alberdi, G.; O’Sullivan, E.; O’Brien, E.; Crosbie, B.; Twomey, P.; McAuliffe, F. Maternal and fetal blood lipid concentrations during pregnancy differ by maternal body mass index: Findings from the ROLO study. BMC Pregnancy Childbirth 2017, 17, 360. [Google Scholar] [CrossRef]
- Lippi, G.; Albiero, A.; Montagnana, M.; Salvagno, G.; Scevarolli, S.; Franchi, M.; Guidi, G. Lipid and lipoprotein profile in physiological pregnancy. Clin. Lab. 2007, 53, 173–177. [Google Scholar]
- Warth, M.; Knopp, R. Lipid metabolism in pregnancy. V. Interactions of diabetes, body weight, age, and high carbohydrate diet. Diabetes 1977, 26, 1056–1062. [Google Scholar] [CrossRef]
- Emet, T.; Ustüner, I.; Güven, S.; Balık, G.; Ural, U.; Tekin, Y.; Sentürk, S.; Sahin, F.; Avşar, A. Plasma lipids and lipoproteins during pregnancy and related pregnancy outcomes. Arch. Gynecol. Obstet. 2013, 288, 49–55. [Google Scholar] [CrossRef]
- Jin, W.; Lin, S.; Hou, R.; Chen, X.; Han, T.; Jin, Y.; Tang, L.; Zhu, Z.; Zhao, Z. Associations between maternal lipid profile and pregnancy complications and perinatal outcomes: A population-based study from China. BMC Pregnancy Childbirth 2016, 21, 60. [Google Scholar] [CrossRef] [Green Version]
- Wiznitzer, A.; Mayer, A.; Novack, V.; Sheiner, E.; Gilutz, H.; Malhotra, A.; Novack, L. Association of lipid levels during gestation with preeclampsia and gestational diabetes mellitus: A population-based study. Am. J. Obstet. Gynecol. 2009, 201, e1–e8. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Vera, I.; Bonet, B.; Viana, M.; Quintanar, A.; Martín, M.; Blanco, P.; Donnay, S.; Albi, M. Changes in plasma lipids and increased low-density lipoprotein susceptibility to oxidation in pregnancies complicated by gestational diabetes: Consequences of obesity. Metabolism 2007, 56, 1527–1533. [Google Scholar] [CrossRef]
- Hollingsworth, D.; Grundy, S. Pregnancy-associated hypertriglyceridemia in normal and diabetic women. Differences in insulin-dependent, non-insulin-dependent, and gestational diabetes. Diabetes 1982, 31, 1092–1097. [Google Scholar] [CrossRef]
- Kern Pessôa, V.; Rodacki, M.; Negrato, C.; Zajdenverg, L. Changes in lipid profile after treatment of women with gestational diabetes mellitus. J. Clin. Lipidol. 2016, 10, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Metzger, B.; Phelps, R.; Freinkel, N.; Navickas, I. Effects of gestational diabetes on diurnal profiles of plasma glucose, lipids, and individual amino acids. Diabetes Care 1980, 3, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Xu, S.; Chen, H.; Zhong, L.; Wang, Z. The associations between triglyceride to high-density lipoprotein cholesterol ratios and the risks of gestational diabetes mellitus and large-for-gestational-age infant. Clin. Endocrinol. 2015, 83, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Whyte, K.; Kelly, H.; O’Dwyer, V.; Gibbs, M.; O’Higgins, A.; Turner, M. Offspring birth weight and maternal fasting lipids in women screened for gestational diabetes mellitus (GDM). Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 170, 67–70. [Google Scholar] [CrossRef]
- Zhou, J.; Zhao, X.; Wang, Z.; Hu, Y. Combination of lipids and uric acid in mid-second trimester can be used to predict adverse pregnancy outcomes. Matern. Fetal. Neonatal. Med. 2012, 25, 2633–2638. [Google Scholar] [CrossRef]
- Maple-Brown, L.; Ye, C.; Hanley, A.; Connelly, P.; Sermer, M.; Zinman, B.; Retnakaran, R. Maternal pregravid weight is the primary determinant of serum leptin and its metabolic associations in pregnancy, irrespective of gestational glucose tolerance status. J. Clin. Endocrinol. Metab. 2012, 97, 4148–4155. [Google Scholar] [CrossRef] [Green Version]
- Giannubilo, S.; Tiano, L.; Cecchi, S.; Principi, F.; Tranquilli, A.; Littarru, G. Plasma coenzyme Q10 is increased during gestational diabetes. Diabetes Res. Clin. Pract. 2011, 94, 230–235. [Google Scholar] [CrossRef]
- Qiu, C.; Rudra, C.; Austin, M.; Williams, M. Association of gestational diabetes mellitus and low-density lipoprotein (LDL) particle size. Physiol. Res. 2007, 56, 571–578. [Google Scholar]
- Dubé, E.; Ethier-Chiasson, M.; Lafond, J. Modulation of cholesterol transport by insulin-treated gestational diabetes mellitus in human full-term placenta. Biol. Reprod. 2013, 88, 16. [Google Scholar] [CrossRef] [Green Version]
- Ghafoor, S.; Shaikh, A. Shaheena. Maternal lipids in pregnancies with gestational diabetes mellitus. Pak. J. Med. Health. Sci. 2012, 6, 81–84. [Google Scholar]
- Sreckovic, I.; Birner-Gruenberger, R.; Besenboeck, C.; Miljkovic, M.; Stojakovic, T.; Scharnagl, H.; Marsche, G.; Lang, U.; Kotur-Stevuljevic, J.; Jelic-Ivanovic, Z.; et al. Gestational diabetes mellitus modulates neonatal high-density lipoprotein composition and its functional heterogeneity. Biochim. Biophys. Acta 2014, 1841, 1619–1627. [Google Scholar] [CrossRef]
- Koukkou, E.; Watts, G.; Lowy, C. Serum lipid, lipoprotein and apolipoprotein changes in gestational diabetes mellitus: A cross-sectional and prospective study. J. Clin. Pathol. 1996, 49, 634–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magon, N.; Seshiah, V. Gestational diabetes mellitus: Insulinic management. J. Obstet. Gynaecol. India 2014, 64, 82–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Snel, M.; Jonker, J.; Hammer, S.; Lamb, H.; de Roos, A.; Meinders, A.; Pijl, H.; Romijn, J.; Smit, J.; et al. Prolonged caloric restriction in obese patients with type 2 diabetes mellitus decreases plasma CETP and increases apolipoprotein AI levels without improving the cholesterol efflux properties of HDL. Diabetes Care 2011, 34, 2576–2580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Retnakaran, R.; Qi, Y.; Connelly, P.; Sermer, M.; Hanley, A.; Zinman, B. The graded relationship between glucose tolerance status in pregnancy and postpartum levels of low-density-lipoprotein cholesterol and apolipoprotein B in young women: Implications for future cardiovascular risk. Clin. Endocrinol. Metab. 2010, 95, 4345–4353. [Google Scholar] [CrossRef]
- Herrera, E.; Ortega-Senovilla, H. Disturbances in lipid metabolism in diabetic pregnancy―Are these the cause of the problem? Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 515–525. [Google Scholar] [CrossRef]
- Pihlajamäki, J.; Gylling, H.; Miettinen, T.A.; Laakso, M. Insulin resistance is associated with increased cholesterol synthesis and decreased cholesterol absorption in normoglycemic men. J. Lipid. Res. 2004, 45, 507–512. [Google Scholar] [CrossRef] [Green Version]
- Hoenig, M.; Sellke, F. Insulin resistance is associated with increased cholesterol synthesis, decreased cholesterol absorption and enhanced lipid response to statin therapy. Atherosclerosis 2010, 211, 260–265. [Google Scholar] [CrossRef]
- Rabbani, N.; Chittari, M.; Bodmer, C.; Zehnder, D.; Ceriello, A.; Thornalley, P. Increased glycation and oxidative damage to apolipoprotein B100 of LDL cholesterol in patients with type 2 diabetes and effect of metformin. Diabetes 2010, 59, 1038–1045. [Google Scholar] [CrossRef] [Green Version]
- Hannemann, M.; Liddell, W.; Shore, A.; Clark, P.; Tooke, J. Vascular function in women with previous gestational diabetes mellitus. J. Vasc. Res. 2002, 39, 311–319. [Google Scholar] [CrossRef]
- Kärkkäinen, H.; Laitinen, T.; Heiskanen, N.; Saarelainen, H.; Valtonen, P.; Lyyra-Laitinen, T.; Vanninen, E.; Heinonen, S. Need for insulin to control gestational diabetes is reflected in the ambulatory arterial stiffness index. BMC Pregnancy Childbirth 2013, 16, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westermeier, F.; Salomón, C.; González, M.; Puebla, C.; Guzmán-Gutiérrez, E.; Cifuentes, F.; Leiva, A.; Casanello, P.; Sobrevia, L. Insulin restores gestational diabetes mellitus-reduced adenosine transport involving differential expression of insulin receptor isoforms in human umbilical vein endothelium. Diabetes 2011, 60, 1677–1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lappas, M.; Hiden, U.; Desoye, G.; Froehlich, J.; Hauguel-de Mouzon, S.; Jawerbaum, A. The role of oxidative stress in the pathophysiology of gestational diabetes mellitus. Antioxid. Redox Signal. 2011, 15, 3061–3100. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Scholl, T.O. Oxidative stress: Changes in pregnancy and with gestational diabetes mellitus. Curr. Diab. Rep. 2005, 5, 282–288. [Google Scholar] [CrossRef]
- Sun, Y.; Kopp, S.; Strutz, J.; Gali, C.C.; Zandl-Lang, M.; Fanaee-Danesh, E.; Kirsch, A.; Cvitic, S.; Frank, S.; Saffery, R.; et al. Gestational diabetes mellitus modulates cholesterol homeostasis in human fetoplacental endothelium. Biochim. Biophys. Acta Mol. Cell Biol. Lipids 2018, 1863, 968–979. [Google Scholar] [CrossRef]
- Dong, Y.L.; Vegiraju, S.; Gangula, P.R.; Yallampalli, C. Involvement of CGRP in control of human fetoplacental vascular tone. Am. J. Physiol. Heart Circ. Physiol. 2004, 286, H230–H239. [Google Scholar] [CrossRef] [Green Version]
- Rosenfeld, M.G.; Mermod, J.J.; Amara, S.G.; Swanson, L.W.; Swchenko, P.E.; Rivier, J.; Vale, W.W.; Evans, R.M. Production of a novel neuropeptide encoded by the calcitonin gene via tissue-specific RNA processing. Nature 1983, 304, 129–135. [Google Scholar] [CrossRef]
- Roh, J.; Chang, C.L.; Bhalla, A.; Klein, C.; Hsu, S.Y.T. Intermedin is a calcitonin/ calcitonin gene-related peptide family peptide acting through the calcitonin receptor-like receptor/receptor activity-modifying protein receptor complexes. J. Biol. Chem. 2004, 279, 7264–7274. [Google Scholar] [CrossRef] [Green Version]
- Dong, Y.L.; Green, K.E.; Vegiragu, S.; Hankins, G.D.; Martin, E.; Chauhan, M.; Thota, C.; Yallampalli, C. Evidence for Decreased Calcitonin Gene-Related Peptide (CGRP) Receptors and Compromised Responsiveness to CGRP of Fetoplacental Vessels in Preeclamptic Pregnancies. J. Clin. Endocrinol. Metab. 2005, 90, 2336–2343. [Google Scholar] [CrossRef] [Green Version]
- Gangula, P.R.R.; Dong, Y.L.; Wimalawansa, S.J.; Yallampalli, C. Infusion of pregnant rats with calcitonin gene-related peptide (CGRP)(8–37), a CGRP receptor antagonist, increases blood pressure and fetal mortality and decreases fetal growth. Biol. Reprod. 2002, 67, 624–629. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | C (n = 41) | N-GDM (n = 69) | O-GDM (n = 48) | ||
|---|---|---|---|---|---|
| Maternal variables | |||||
| Age (years) | 31.7 ± 3.8 (23–36) | 34.8 ± 4.8 (25–55) | 34.6 ± 4.5 (26–42) | ||
| Height (cm) | 164 ± 0.1 (152–175) | 160 ± 0.1 * (149–173) | 160 ± 0.1 *,† (148–177) | ||
| Weight (Kg) | |||||
| T1 | 62.8 ± 5.8 (53–74) | 60.9 ± 7.0 (43.3–77) | 81.3 ± 7.8 *,† (68.8–96) | ||
| T2 | 68.8 ± 5.2 (59–78) | 64.9 ± 7.1 * (45–82.8) | 82.0 ± 9.6 *,† (64–115) | ||
| T3 | 75.2 ± 4.4 ‡ (68–83) | 68.8 ± 7.2 *,‡ (51.9–88.5) | 85.2 ± 10.0 *,†,‡ (66–120) | ||
| Weight gain (Kg) | 12.4 ± 4.8 | 8.0 ± 3.4 * | 5.8 ± 3.8 *,† | ||
| (4–22) | (0.2–12) | (0.2–13.5) | |||
| BMI (Kg/m2) | |||||
| T1 | 23.5 ± 1.8 (20.5–1.8) | 24.0 ± 2.3 (17.3–28.9) | 31.5 ± 2.3 *,† (30–38.9) | ||
| T2 | 25.7 ± 1.5 (22–29.3) | 25.6 ± 2.2 (18–30) | 32.0 ± 3.1 *,† (28.9–37.3) | ||
| T3 | 28.1 ± 2.0 ‡ (25.7–29.9) | 26.9 ± 2.0 *,‡ (20.8–29.8) | 33.4 ± 3.4 *,†,‡ (30.1–41.4) | ||
| Mean arterial pressure (mm Hg) | |||||
| T1 | 81.5 ± 5.9 (73.3–93.3) | 81.7 ± 7.1 (63.3–95.6) | 79.1 ± 5.6 † (67.3–86.7) | ||
| T2 | 82.2 ± 5.9 (73.3–93.3) | 88.4 ± 9.7 * (66.7–103.3) | 80.5 ± 7.5 † (66.7–93.3) | ||
| T3 | 86.4 ± 5.3 ‡ (73.3–96.7) | 83.1 ± 6.3 * (66.7–101.7) | 81.4 ± 7.5 * (70–95) | ||
| Fasting glycemia (mg/dL) | 84.0 ± 4.0 (80–88) | 85.5 ± 10.9 (63–103) | 84.3 ± 8.4 (69–98) | ||
| OGTT (mg/dL) | |||||
| Basal glycemia | 77.5 ± 4.3 (69–85) | 81.8 ± 8.4 * (70–110) | 87.2 ± 14.2 *,† (70–129) | ||
| Glycemia at 2 hours | 106.4 ± 17.4 (75–139) | 157.7 ± 15.7 * (140–201) | 154.7 ± 17.3 * (141–200) | ||
| Insulin (µUI/ml) | - | 9.5 ± 5.1 (2.7–27.4) | 11.9 ± 6.5 * (3.3–26.6) | ||
| HbA1c % | - | 5.7 ± 2.0 (2.4–14.4) | 5.9 ± 1.4 (4.9–13.5) | ||
| HOMA-IR | - | 2.0 ± 1.5 (0.5–5.2) | 3.1 ± 2.8 * (0.8–12.9) | ||
| Newborn variables | |||||
| Sex (female/male) | 25/16 | 37/32 | 21/27 | ||
| Gestational age (weeks) | 38.5 ± 1.0 (37–40) | 38.6 ± 3 (36–40) | 38.2 ± 3.2 (37–40) | ||
| Height (cm) | 49.5 ± 1.7 (45–52.5) | 49.9 ± 2.0 (46–52) | 49.5 ± 1.5 (48–52) | ||
| Birth weight (grams) | 3308 ± 382 (2600–4060) | 3286 ± 412 (2430–3830) | 3243 ± 405 (2700–3950) | ||
| Ponderal index (grams/cm3 x100) | 2.6 ± 0.2 (2.35–3.02) | 2.7 ± 0.2 (2.43–3.14) | 2.7 ± 0.3 (2.3–3.16) | ||
| T1 | ||||||||||||||||||||
| Lipid | TC | TG | HDL | LDL | VLDL | |||||||||||||||
| Group | C | GDM | C | GDM | C | GDM | C | GDM | C | GDM | ||||||||||
| N° pairs | 23 | 27 | 23 | 27 | 23 | 27 | 23 | 27 | 23 | 27 | ||||||||||
| Spearman r | 0.08 | 0.19 | 0.37 | 0.32 | -0.04 | -0.32 | 0.32 | 0.21 | 0.37 | 0.37 | ||||||||||
| P | 0.703 | 0.342 | 0.085 | 0.101 | 0.843 | 0.102 | 0.137 | 0.292 | 0.082 | 0.07 | ||||||||||
| T2 | ||||||||||||||||||||
| Lipid | TC | TG | HDL | LDL | VLDL | |||||||||||||||
| Group | C | GDM | C | GDM | C | GDM | C | GDM | C | GDM | ||||||||||
| N° pairs | 40 | 31 | 40 | 31 | 37 | 31 | 37 | 31 | 36 | 31 | ||||||||||
| Spearman r | −0.01 | −0.04 | 0.05 | 0.30 | 0.20 | −0.02 | −0.09 | −0.07 | −0.22 | 0.30 | ||||||||||
| P | 0.951 | 0.826 | 0.742 | 0.096 | 0.237 | 0.934 | 0.590 | 0.699 | 0.196 | 0.097 | ||||||||||
| T3 | ||||||||||||||||||||
| Lipid | TC | TG | HDL | LDL | VLDL | |||||||||||||||
| Group | C | GDM | C | GDM | C | GDM | C | GDM | C | GDM | ||||||||||
| N° pairs | 41 | 44 | 41 | 44 | 41 | 44 | 41 | 44 | 41 | 44 | ||||||||||
| Spearman r | 0.30 | −0.17 | −0.07 | 0.22 | 0.12 | −0.09 | −0.19 | −0.18 | −0.13 | 0.17 | ||||||||||
| P | 0.061 | 0.271 | 0.655 | 0.151 | 0.451 | 0.577 | 0.221 | 0.254 | 0.434 | 0.276 | ||||||||||
| Variables | NTC-C (n = 5) | HTC-C (n = 5) | NTC-GDM (n = 7) | HTC-GDM (n = 4) | |||
|---|---|---|---|---|---|---|---|
| Maternal variables | |||||||
| Weeks of gestation | 39.8 ± 0.4 (39–40) | 38.4 ± 1.1 * (37–40) | 38.6 ± 0.8 * (38–40) | 39.3 ± 0.5 (39–40) | |||
| Age (years) | 31.4 ± 8.0 (19–38) | 28.8 ± 3.5 (27–34) | 30.9 ± 5.6 (23–39) | 34.3 ± 3.6 (29–37) | |||
| Height (cm) | 1.65 ± 0.1 (1.59–1.73) | 1.61 ± 0.1 (1.51–1.67) | 1.60 ± 0.04 (1.55–1.64) | 1.63 ± 0.1 (1.57–1.78) | |||
| Weight (Kg) | |||||||
| T1 | 63.2 ± 6.4 (52–68) | 59.9 ± 7.1 (52.1–71) | 61.7 ± 5.9 (53–70) | 67.8 ± 2.1 (66–70) | |||
| T3 | 73.2 ± 6.9 ‡ (63–80) | 69.9 ± 5.0 ‡ (63–74) | 71.0 ± 5.9 ‡ (65–78) | 74.2 ± 1.0 ‡ (73.5–76) | |||
| Weight gain (Kg) | 10.0 ± 5.1 (3–16) | 9.0 ± 6.0 (1.5–10.5) | 7.6 ± 2.9 (5–11) | 7.8 ± 1.7 (6–10) | |||
| BMI (Kg/m2) | |||||||
| T1 | 23.3 ± 2.2 (21–26) | 23.0 ± 2.0 (21–25) | 24.4 ± 2.2 (21–27) | 25.7 ± 3.3 (21–28) | |||
| T3 | 26.1 ± 0.9 ‡ (25–27) | 27.1 ± 0.9 ‡ (26–28) | 27.7 ± 1.5 ‡ (25–29) | 28.3 ± 2.9 (24–29.8) | |||
| Mean arterial pressure (mm Hg) | |||||||
| T1 | 76.1 ± 5.4 (70–83) | 82.2 ± 5.1 (77–87) | 79.8 ± 6.6 (73–90) | 76.7 ± 4.7 (73–83) | |||
| T3 | 89.3 ± 11.5 (73–105) | 82.2 ± 5.9 (73–90) | 85.9 ± 9.5 (73–103) | 80.2 ± 3.7 (77–84) | |||
| Fasting glycemia (mg/dL) | 81.8 ± 4.0 (77–86) | 77.0 ± 9.8 (70–88) | 86.6 ± 5.7 (80–91) | 80.3 ± 3.6 (75–83) | |||
| OGTT (mg/dL) | |||||||
| Basal glycemia | 73.0 ± 7.0 (65–78) | 70.5 ± 0.7 (70–71) | 77.1 ± 5.0 (70–85) | 79.0 ± 5.7 (73–86) | |||
| Glycemia at 2 hours | 104.3 ± 10.0 (93–112) | 98.0 ± 35.4 (73–123) | 148.7 ± 4.7 * (144–155) | 164.3 ± 20.8 * (146–192) | |||
| Insulin (µUI/ml) | - | - | 13.6 ± 3.0 (11.5–17) | 11.5 ± 7.3 (2.5–17) | |||
| HbA1c % | - | - | 4.9 ± 0.3 (4.6–5.3) | 5.4 ± 1.7 (4.5–9.9) | |||
| HOMA-IR | - | - | 2.5 ± 0.4 (2.2–2.9) | 2.3 ± 1.4 (0.7–4.2) | |||
| Lipids (mg/dL) | |||||||
| Total cholesterol | 223 ± 29.2 (187–258) | 308 ± 22.3 * (292–347) | 232 ± 19.8 (202–256) | 337 ± 44.5*,† (298–376) | |||
| Triglycerides | 276 ± 45.4 (201–317) | 235 ± 96.3 (184–394) | 219 ± 73.3 (153–331) | 268 ± 76.6 (172–-335) | |||
| High density lipoproteins | 61 ± 14.5 (49–84) | 53 ± 8.0 (47–67) | 72 ± 14.0 (50–91) | 83 ± 23.3 (50–110) | |||
| Low density lipoproteins | 119 ± 18.1 (101–142) | 208 ± 25.2 * (166–234) | 147 ± 27.5 (109–176) | 159 ± 48.6 (113–220) | |||
| Very low density lipoproteins | 43 ± 24.4 (13–63) | 47 ± 18.7 (31–79) | 46 ± 13.2 (33–66) | 54 ± 15.5 (34–67) | |||
| Newborn variables | |||||||
| Sex (female/male) | 2/3 | 1/4 | 4/3 | 2/2 | |||
| Height (cm) | 51.6 ± 1.2 (50–53) | 50.2 ± 1.3 (49–53) | 50.3 ± 1.7 (47–52) | 50.6 ± 1.4 (49–52) | |||
| Birth weight (grams) | 3500 ± 199.1 (3320–3810) | 3220 ± 346.5 (2890–3800) | 3287 ± 312.1 (2640–3610) | 3545 ± 438.5 (2900–3860) | |||
| Ponderal index (grams/cm3 × 100) | 2.5 ± 0.1 (2.4–2.7) | 2.6 ± 0.1 (2.4–2.7) | 2.6 ± 0.2 (2.3–2.8) | 2.7 ± 0.3 (2.5–3.1) | |||
| Parameter | CGRP | |||||
|---|---|---|---|---|---|---|
| Group | Control (n = 10) | GDM (n = 11) | NTC-C (n = 5) | HTC-C (n = 5) | NTC-GDM (n = 7) | HTC-GDM (n = 4) |
| EC50 average (nM) | 7.4 ± 0.18 | 7.4 ± 0.16 | 7.6 ± 0.2 | 8.4 ± 0.2 * | 10.7 ± 0.3 *,† | 6.5 ± 0.2 *,†,‡ |
| Rmax average (%) | 32.1 ± 5.2 | 18.3 ± 1.9 * | 39.1 ± 6.7 | 18.2 ± 2 * | 28.7 ± 2.4 † | 15.3 ± 1.8 *,† |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Contreras-Duarte, S.; Carvajal, L.; Garchitorena, M.J.; Subiabre, M.; Fuenzalida, B.; Cantin, C.; Farías, M.; Leiva, A. Gestational Diabetes Mellitus Treatment Schemes Modify Maternal Plasma Cholesterol Levels Dependent to Women´s Weight: Possible Impact on Feto-Placental Vascular Function. Nutrients 2020, 12, 506. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12020506
Contreras-Duarte S, Carvajal L, Garchitorena MJ, Subiabre M, Fuenzalida B, Cantin C, Farías M, Leiva A. Gestational Diabetes Mellitus Treatment Schemes Modify Maternal Plasma Cholesterol Levels Dependent to Women´s Weight: Possible Impact on Feto-Placental Vascular Function. Nutrients. 2020; 12(2):506. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12020506
Chicago/Turabian StyleContreras-Duarte, Susana, Lorena Carvajal, María Jesús Garchitorena, Mario Subiabre, Bárbara Fuenzalida, Claudette Cantin, Marcelo Farías, and Andrea Leiva. 2020. "Gestational Diabetes Mellitus Treatment Schemes Modify Maternal Plasma Cholesterol Levels Dependent to Women´s Weight: Possible Impact on Feto-Placental Vascular Function" Nutrients 12, no. 2: 506. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12020506