A Suboptimal Diet Is Associated with Poorer Cognition: The NUDAD Project

 , ,
, ,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dietary Quality
2.3. Neuropsychological Assessment
2.4. Data Analyses
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Prince, M.J. World Alzheimer Report 2015: The global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [Green Version]
- Okubo, H.; Inagaki, H.; Gondo, Y.; Kamide, K.; Ikebe, K.; Masui, Y.; Arai, Y.; Ishizaki, T.; Sasaki, S.; Nakagawa, T.; et al. Association between dietary patterns and cognitive function among 70-year-old Japanese elderly: A cross-sectional analysis of the SONIC study. Nutr. J. 2017, 16, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loef, M.; Walach, H. Fruit, vegetables and prevention of cognitive decline or dementia: A systematic review of cohort studies. J. Nutr. Health Aging 2012, 16, 626–630. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C.; Wang, Y.; Barnes, L.L.; Bennett, D.A.; Dawson-Hughes, B.; Booth, S.L. Nutrients and bioactives in green leafy vegetables and cognitive decline. Neurology 2018, 90, e214. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Huang, J.; Song, D.; Deng, R.; Wei, J.; Zhang, Z. Increased Consumption of Fruit and Vegetables Is Related to a Reduced Risk of Cognitive Impairment and Dementia: Meta-Analysis. Front. Aging Neurosci. 2017, 9, 18. [Google Scholar] [CrossRef] [Green Version]
- Wesselman, L.M.P.; Doorduijn, A.S.; de Leeuw, F.A.; Verfaillie, S.C.J.; van Leeuwenstijn-Koopman, M.; Slot, R.E.R.; Kester, M.I.; Prins, N.D.; van de Rest, O.; de van der Schueren, M.A.E.; et al. Dietary Patterns Are Related to Clinical Characteristics in Memory Clinic Patients with Subjective Cognitive Decline: The SCIENCe Project. Nutrients 2019, 11, 1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nurk, E.; Drevon, C.A.; Refsum, H.; Solvoll, K.; Vollset, S.E.; Nygård, O.; Nygaard, H.A.; Engedal, K.; Tell, G.S.; Smith, A.D. Cognitive performance among the elderly and dietary fish intake: The Hordaland Health Study. Am. J. Clin. Nutr. 2007, 86, 1470–1478. [Google Scholar] [CrossRef]
- Loughrey, D.G.; Lavecchia, S.; Brennan, S.; Lawlor, B.A.; Kelly, M.E. The Impact of the Mediterranean Diet on the Cognitive Functioning of Healthy Older Adults: A Systematic Review and Meta-Analysis. Adv. Nutr. 2017, 8, 571–586. [Google Scholar] [CrossRef] [PubMed]
- Lourida, I.; Soni, M.; Thompson-Coon, J.; Purandare, N.; Lang, I.A.; Ukoumunne, O.C.; Llewellyn, D.J. Mediterranean diet, cognitive function, and dementia: A systematic review. Epidemiology 2013, 24, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Barbagallo, M. Nutritional prevention of cognitive decline and dementia. Acta Biomed. 2018, 89, 276–290. [Google Scholar] [CrossRef]
- van den Brink, A.C.; Brouwer-Brolsma, E.M.; Berendsen, A.A.; van de Rest, O. The Mediterranean, Dietary Approaches to Stop Hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diets Are Associated with Less Cognitive Decline and a Lower Risk of Alzheimer’s Disease—A Review. Adv. Nutr. 2019, 10, 1010–1065. [Google Scholar] [CrossRef] [PubMed]
- Petersson, S.D.; Philippou, E. Mediterranean Diet, Cognitive Function, and Dementia: A Systematic Review of the Evidence. Adv. Nutr. 2016, 7, 889–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calil, S.R.B.; Brucki, S.M.D.; Nitrini, R.; Yassuda, M.S. Adherence to the Mediterranean and MIND diets is associated with better cognition in healthy seniors but not in MCI or AD. Clin. Nutr. ESPEN 2018, 28, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Doorduijn, A.S.; Visser, M.; Van de Rest, O.; Kester, M.; De Leeuw, F.A.; Boesveldt, S.; Fieldhouse, J.L.P.; Van den Heuvel, E.G.H.M.; Teunissen, C.C.; Scheltens, P.; et al. Associations of AD biomarkers and cognitive performance with nutritional status: The NUDAD project. Nutrients 2019, 11, 1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Flier, W.M.; Pijnenburg, Y.A.; Prins, N.; Lemstra, A.W.; Bouwman, F.H.; Teunissen, C.E.; van Berckel, B.N.; Stam, C.J.; Barkhof, F.; Visser, P.J.; et al. Optimizing patient care and research: The Amsterdam Dementia Cohort. J. Alzheimer’s Dis. JAD 2014, 41, 313–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [Green Version]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild Cognitive Impairment: Clinical Characterization and Outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef]
- Verhage, F. Intelligence and Age in a Dutch Sample. Hum. Dev. 1965, 8, 238–245. [Google Scholar] [CrossRef]
- van Lee, L.; Geelen, A.; van Huysduynen, E.J.C.H.; de Vries, J.H.M.; van’t Veer, P.; Feskens, E.J.M. The Dutch Healthy Diet index (DHD-index): An instrument to measure adherence to the Dutch Guidelines for a Healthy Diet. Nutr. J. 2012, 11, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Lee, L.; Feskens, E.J.M.; Meijboom, S.; Hooft van Huysduynen, E.J.C.; van’t Veer, P.; de Vries, J.H.M.; Geelen, A. Evaluation of a screener to assess diet quality in the Netherlands. Br. J. Nutr. 2015, 115, 517–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Council of the Netherlands. Guidelines for a Healthy Diet 2006; Health Council of the Netherlands: The Hague, The Netherlands, 2006. [Google Scholar]
- Rey, A. L’examen Clinique En Psychologie [The Clinical Psychological Examination]; Presses Universitaires de France: Paris, France, 1964. [Google Scholar]
- Lindeboom, J.; Schmand, B.; Tulner, L.; Walstra, G.; Jonker, C. Visual association test to detect early dementia of the Alzheimer type. J. Neurol. Neurosurg. Psychiatry 2002, 73, 126–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benton, A.L. Differential behavioral effects in frontal lobe disease. Neuropsychologia 1968, 6, 53–60. [Google Scholar] [CrossRef]
- Warrington, E.K.; James, M.; Thames Valley Test Company. The Visual Object and Space Perception Battery; Thames Valley Test Company: Bury St. Edmunds, UK, 1991. [Google Scholar]
- Reitan, R.M. The relation of the trail making test to organic brain damage. J. Consult. Psychol. 1955, 19, 393–394. [Google Scholar] [CrossRef]
- Wechsler, D.; Psychological, C. WAIS-III: Administration and Scoring Manual: Wechsler Adult Intelligence Scale, 3rd ed.; Psychological Corporation: San Antonio, TX, USA, 1997. [Google Scholar]
- Stroop, J.R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 1935, 18, 643. [Google Scholar] [CrossRef]
- Hughes, B. Missile wounds of the brain. A study of psychological deficits. J. Neurol. Neurosurg. Psychiatry 1970, 33, 551. [Google Scholar] [CrossRef] [Green Version]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B. The FAB a frontal assessment battery at bedside. Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef] [Green Version]
- Gordon, M.; Lumley, T. Forestplot: Advanced Forest Plot Using’grid’Graphics, R Package Version; 2015, Volume 1. Available online: https://cran.r-project.org/web/packages/forestplot/forestplot.pdf (accessed on 20 February 2020).
- Irimata, K.E.; Dugger, B.N.; Wilson, J.R. Impact of the Presence of Select Cardiovascular Risk Factors on Cognitive Changes among Dementia Subtypes. Curr. Alzheimer Res. 2018, 15, 1032–1044. [Google Scholar] [CrossRef]
- Martínez-Lapiscina, E.H.; Clavero, P.; Toledo, E.; Estruch, R.; Salas-Salvadó, J.; San Julián, B.; Sanchez-Tainta, A.; Ros, E.; Valls-Pedret, C.; Martinez-Gonzalez, M.Á. Mediterranean diet improves cognition: The PREDIMED-NAVARRA randomised trial. J. Neurol. Neurosurg. Psychiatry 2013, 84, 1318. [Google Scholar] [CrossRef] [Green Version]
- Soininen, H.; Solomon, A.; Visser, P.J.; Hendrix, S.B.; Blennow, K.; Kivipelto, M.; Hartmann, T.; Hallikainen, I.; Hallikainen, M.; Helisalmi, S.; et al. 24-month intervention with a specific multinutrient in people with prodromal Alzheimer’s disease (LipiDiDiet): A randomised, double-blind, controlled trial. Lancet Neurol. 2017, 16, 965–975. [Google Scholar] [CrossRef] [Green Version]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Study Population | Controls | MCI | AD Dementia |
|---|---|---|---|---|
| n | 357 | 133 | 90 | 134 |
| Age (years) | 65 ± 8.3 | 61 ± 7.2 | 66 ± 7.5 † | 68 ± 8.3 † |
| Sex, female | 165 (46) | 62 (47) | 34 (38) | 69 (52) |
| Level of education | 5 ± 1.2 | 6 ± 1.2 | 5 ± 1.2 | 5 ± 1.2 † |
| BMI (kg/m2) | 26 ± 4.1 | 27 ± 4.7 | 26 ± 3.4 | 25 ± 3.8 † |
| Hypertension, yes | 87 (24) | 24 (18) | 23 (26) | 40 (30) |
| Hypercholesterolaemia, yes | 50 (14) | 14 (11) | 16 (18) | 20 (15) |
| Diabetes mellitus, yes | 33 (9) | 9 (7) | 13 (14) | 11 (8) |
| MMSE score | 26 ± 3.3 | 28 ± 1.7 | 26 ± 2.5 † | 23 ± 3.0 †,‡ |
| Dietary quality score a | ||||
| Total diet | 53.9 ± 0.6 | 54.7 ± 11.6 | 53.0 ± 12.2 | 53.6 ± 11.0 |
| Vegetables | 6.1 ± 0.1 | 6.3 ± 3.0 | 6.5 ± 2.5 | 5.6 ± 2.7 |
| Fruit | 7.4 ± 0.2 | 7.6 ± 3.0 | 7.3 ± 3.3 | 7.1 ± 3.3 |
| Fibers | 7.2 ± 0.1 | 7.1 ± 2.1 | 7.4 ± 2.0 | 7.0 ± 2.0 |
| Fish | 5.6 ± 0.2 | 5.7 ± 3.5 | 5.8 ± 3.5 | 5.2 ± 3.2 |
| Saturated fat | 5.3 ± 0.2 | 5.4 ± 4.1 | 4.5 ± 4.1 | 5.8 ± 4.1 |
| Trans fat | 7.8 ± 0.2 | 7.8 ± 4.1 | 7.3 ± 4.4 | 8.0 ± 4.0 |
| Salt | 5.9 ± 0.2 | 6.0 ± 3.0 | 5.3 ± 3.0 | 6.1 ± 3.1 |
| Alcohol | 8.8 ± 0.1 | 8.8 ± 2.3 | 8.8 ± 2.4 | 8.8 ± 2.5 |
| Cognitive performance a | ||||
| Global cognition | - | 0.5 ± 0.4 | 0.0 ± 0.3 † | −0.6 ± 0.6 †,‡ |
| Memory | - | 0.8 ± 0.6 | −0.1 ± 0.6 † | −0.7 ± 0.5 †,‡ |
| Language | - | 0.5 ± 0.6 | 0.1 ± 0.4 † | −0.5 ± 0.8 †,‡ |
| Visuospatial functioning | - | 0.3 ± 0.3 | 0.2 ± 0.4 | −0.4 ± 1.1 †,‡ |
| Attention | - | 0.5 ± 0.6 | 0.0 ± 0.6 † | −0.5 ± 0.8 †,‡ |
| Executive functioning | - | 0.5 ± 0.6 | 0.0 ± 0.5 † | −0.6 ± 0.8 †,‡ |
| Dietary Quality Score | Global Cognition | Memory | Language | Visuospatial Functioning | Attention | Executive Functioning |
|---|---|---|---|---|---|---|
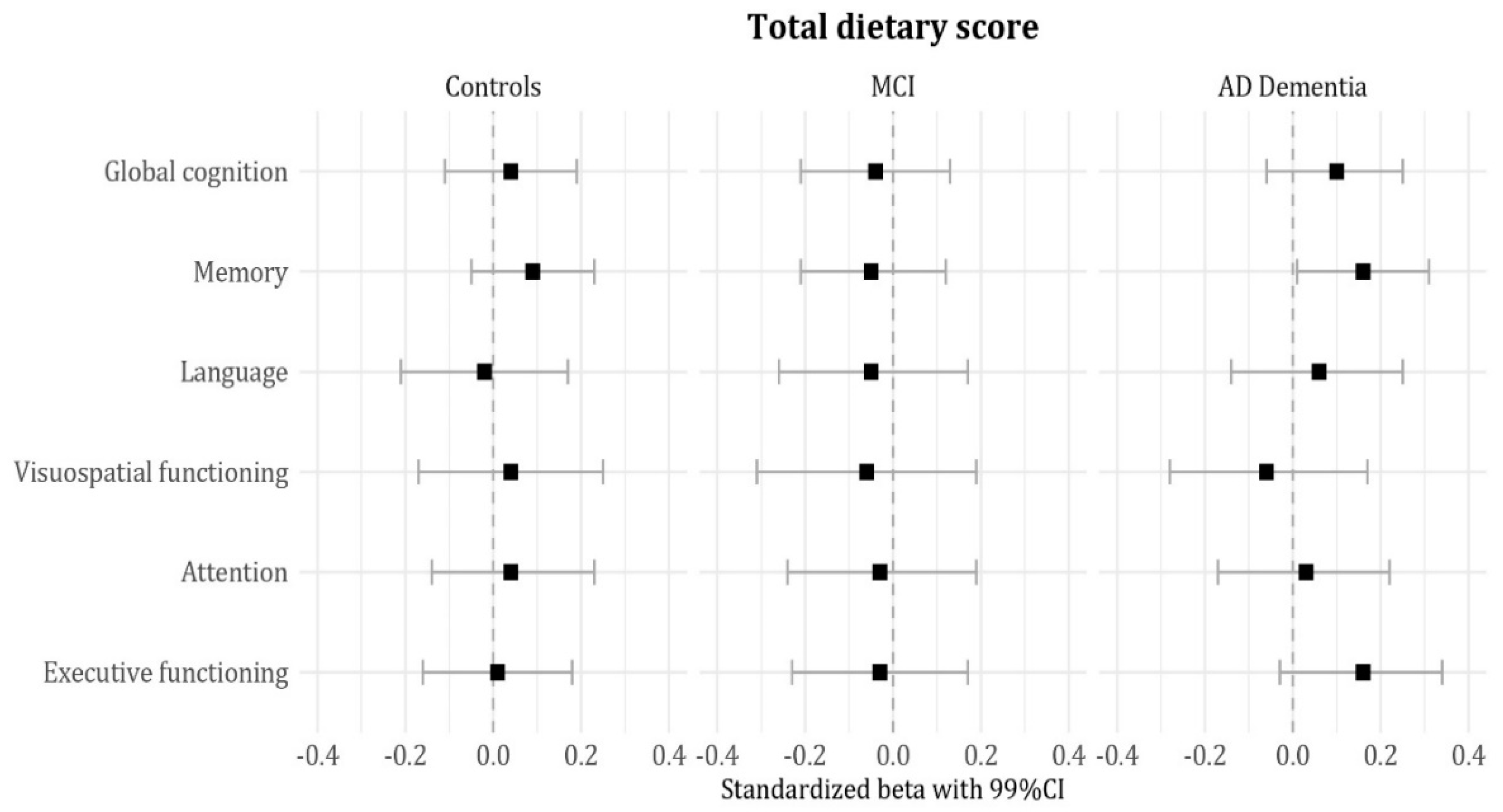
| Total diet | 0.06 (−0.00; 0.01) | 0.10 (−0.00; 0.02) | 0.01 (−0.01; 0.01) | −0.01 (−0.01; 0.01) | 0.03 (−0.01; 0.01) | 0.07 (−0.00; 0.01) |
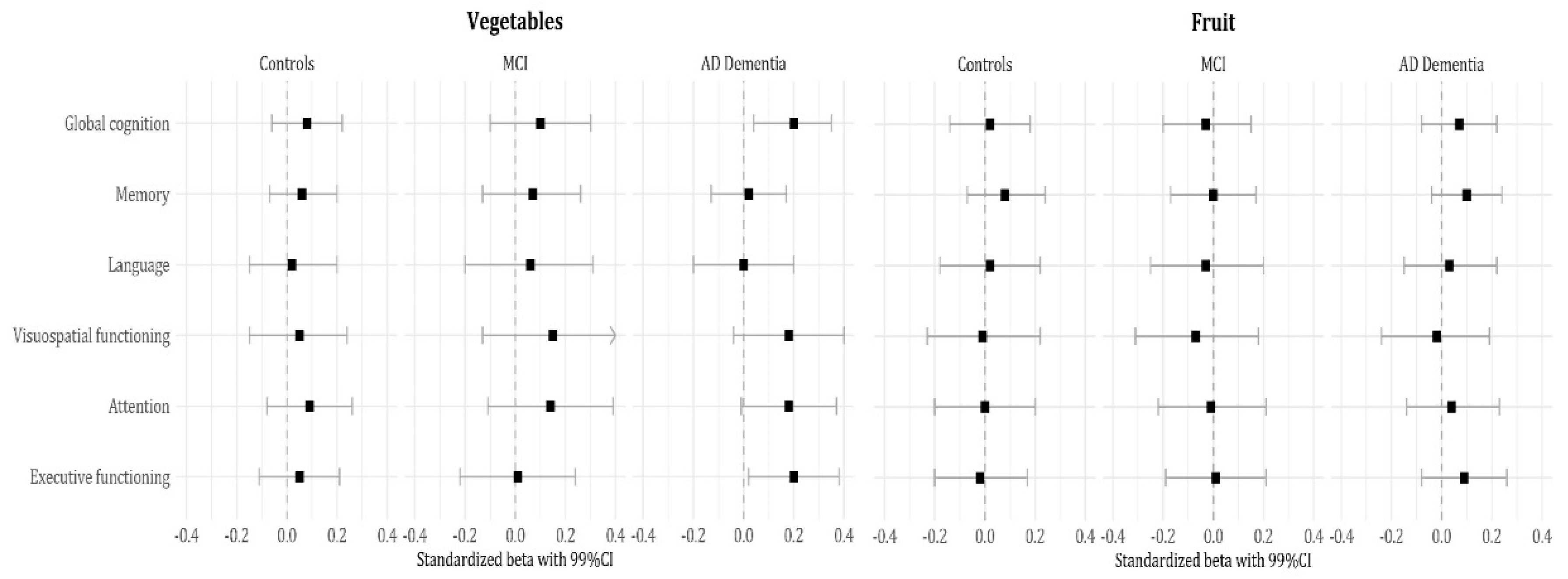
| Vegetables | 0.18 * (0.01; 0.07) | 0.09 (−0.01; 0.07) | 0.06 (−0.02; 0.05) | 0.15 * (0.00; 0.08) | 0.17 * (0.01; 0.09) | 0.13 * (0.00; 0.08) |
| Fruit | 0.09 (−0.01; 0.04) | 0.13 (−0.00; 0.07) | 0.05 (−0.02; 0.04) | 0.01 (−0.03; 0.04) | 0.05 (−0.02; 0.05) | 0.07 (−0.01; 0.05) |
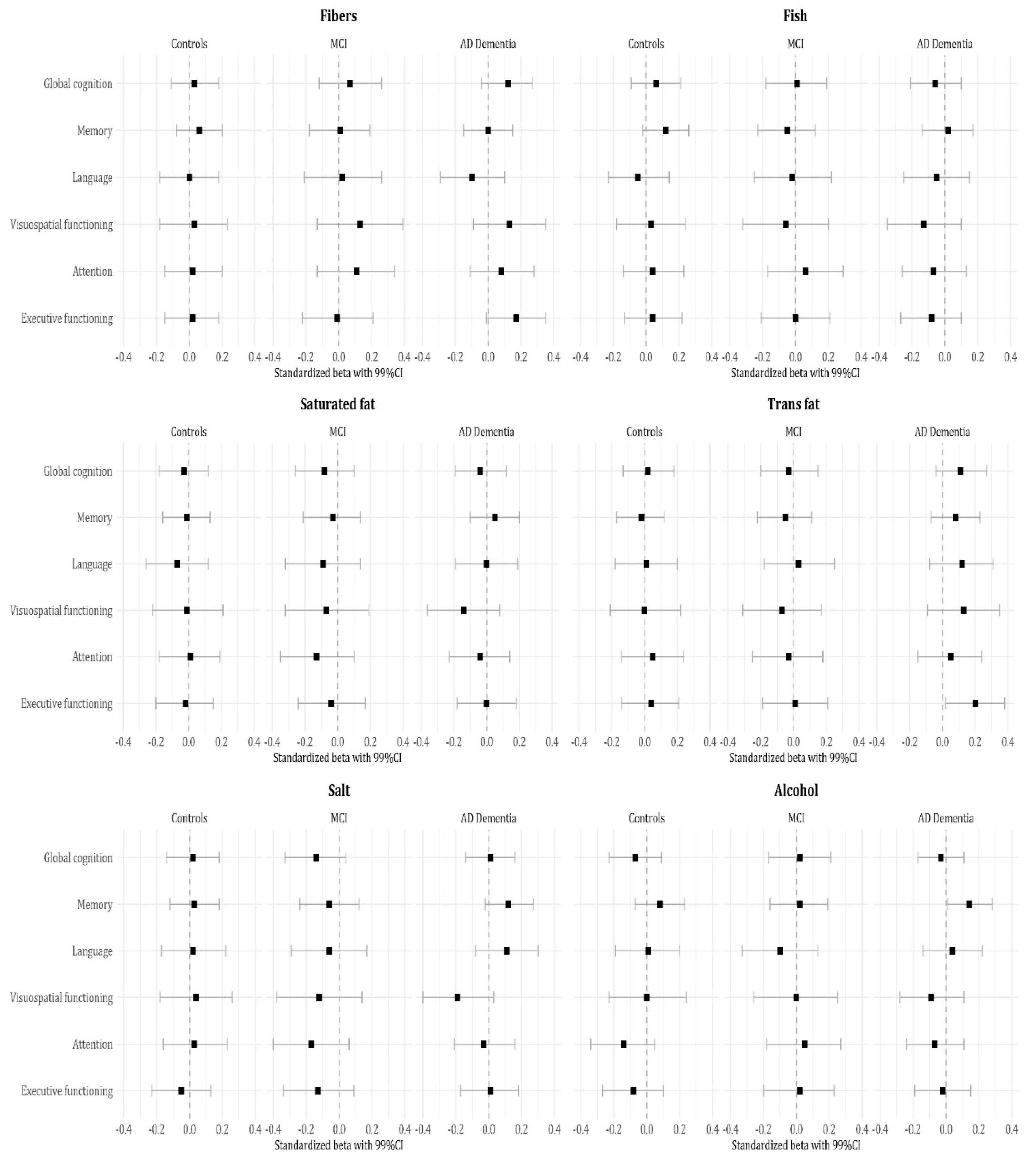
| Fibers | 0.07 (−0.02; 0.07) | 0.02 (−0.05; 0.06) | −0.02 (−0.06; 0.04) | 0.09 (−0.02; 0.09) | 0.06 (−0.03; 0.08) | 0.07 (−0.02; 0.08) |
| Fish | 0.04 (−0.02; 0.03) | 0.07 (−0.02; 0.05) | −0.00 (−0.03; 0.03) | −0.01 (−0.04; 0.03) | 0.04 (−0.02; 0.04) | 0.03 (−0.03; 0.04) |
| Saturated fat | −0.09 (−0.03; 0.01) | −0.03 (−0.03; 0.02) | −0.08 (−0.04; 0.01) | −0.10 (−0.05; 0.01) | −0.08 (−0.04; 0.01) | −0.05 (−0.04; 0.02) |
| Trans fat | 0.04 (−0.01; 0.03) | 0.01 (−0.03; 0.03) | 0.05 (−0.02; 0.03) | 0.02 (−0.02; 0.03) | 0.02 (−0.02; 0.03) | 0.08 (−0.01; 0.04) |
| Salt | −0.05 (−0.04; 0.02) | 0.04 (−0.03; 0.05) | 0.02 (−0.03; 0.04) | −0.11 (−0.07; 0.01) | −0.06 (−0.05; 0.02) | −0.06 (−0.05; 0.02) |
| Alcohol | −0.03 (−0.04; 0.03) | 0.09 (−0.01; 0.08) | −0.01 (−0.05; 0.04) | −0.03 (−0.06; 0.04) | −0.06 (−0.07; 0.02) | −0.03 (−0.05; 0.03) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fieldhouse, J.L.P.; Doorduijn, A.S.; de Leeuw, F.A.; Verhaar, B.J.H.; Koene, T.; Wesselman, L.M.P.; de van der Schueren, M.A.E.; Visser, M.; van de Rest, O.; Scheltens, P.; et al. A Suboptimal Diet Is Associated with Poorer Cognition: The NUDAD Project. Nutrients 2020, 12, 703. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030703
Fieldhouse JLP, Doorduijn AS, de Leeuw FA, Verhaar BJH, Koene T, Wesselman LMP, de van der Schueren MAE, Visser M, van de Rest O, Scheltens P, et al. A Suboptimal Diet Is Associated with Poorer Cognition: The NUDAD Project. Nutrients. 2020; 12(3):703. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030703
Chicago/Turabian StyleFieldhouse, Jay L. P., Astrid S. Doorduijn, Francisca A. de Leeuw, Barbara J. H. Verhaar, Ted Koene, Linda M. P. Wesselman, Marian A.E. de van der Schueren, Marjolein Visser, Ondine van de Rest, Philip Scheltens, and et al. 2020. "A Suboptimal Diet Is Associated with Poorer Cognition: The NUDAD Project" Nutrients 12, no. 3: 703. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030703