Human Milk Oligosaccharide Profile Variation Throughout Postpartum in Healthy Women in a Brazilian Cohort

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
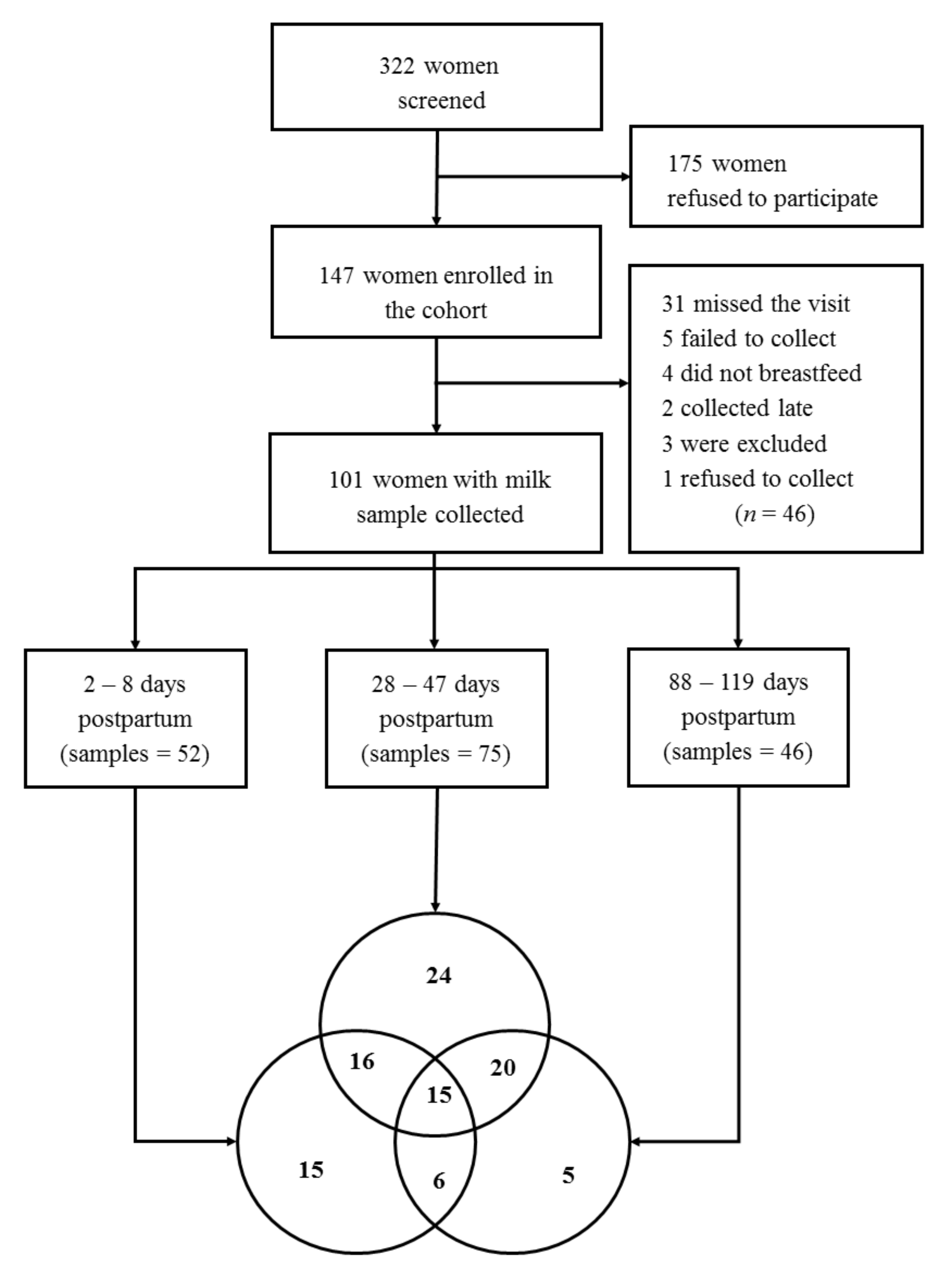
2.1. Study Design and Eligibility Criteria
2.2. Human Milk Data and Oligosaccharides Analysis
2.3. Co-Variables
2.4. Statistical Analysis
3. Results
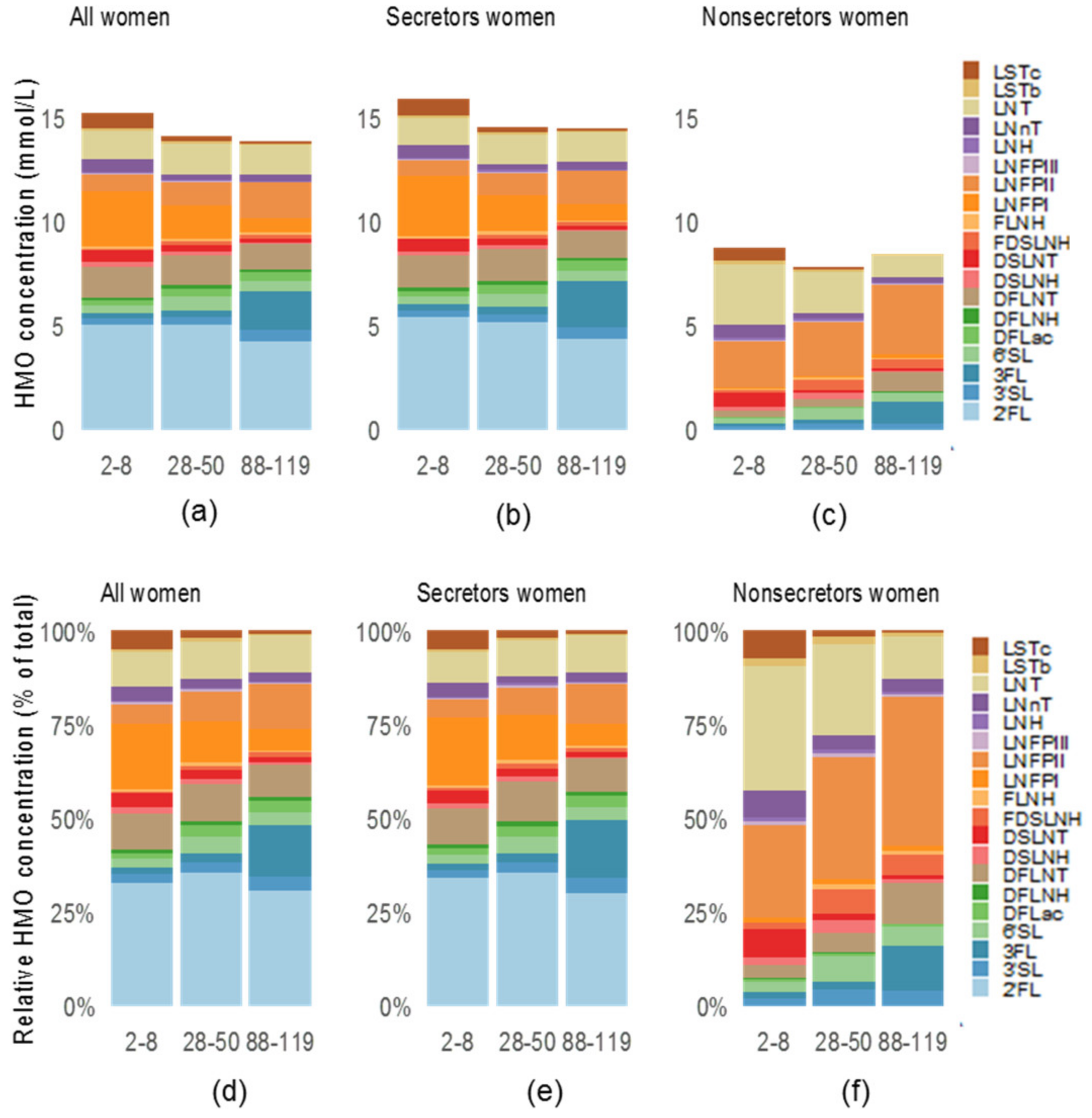
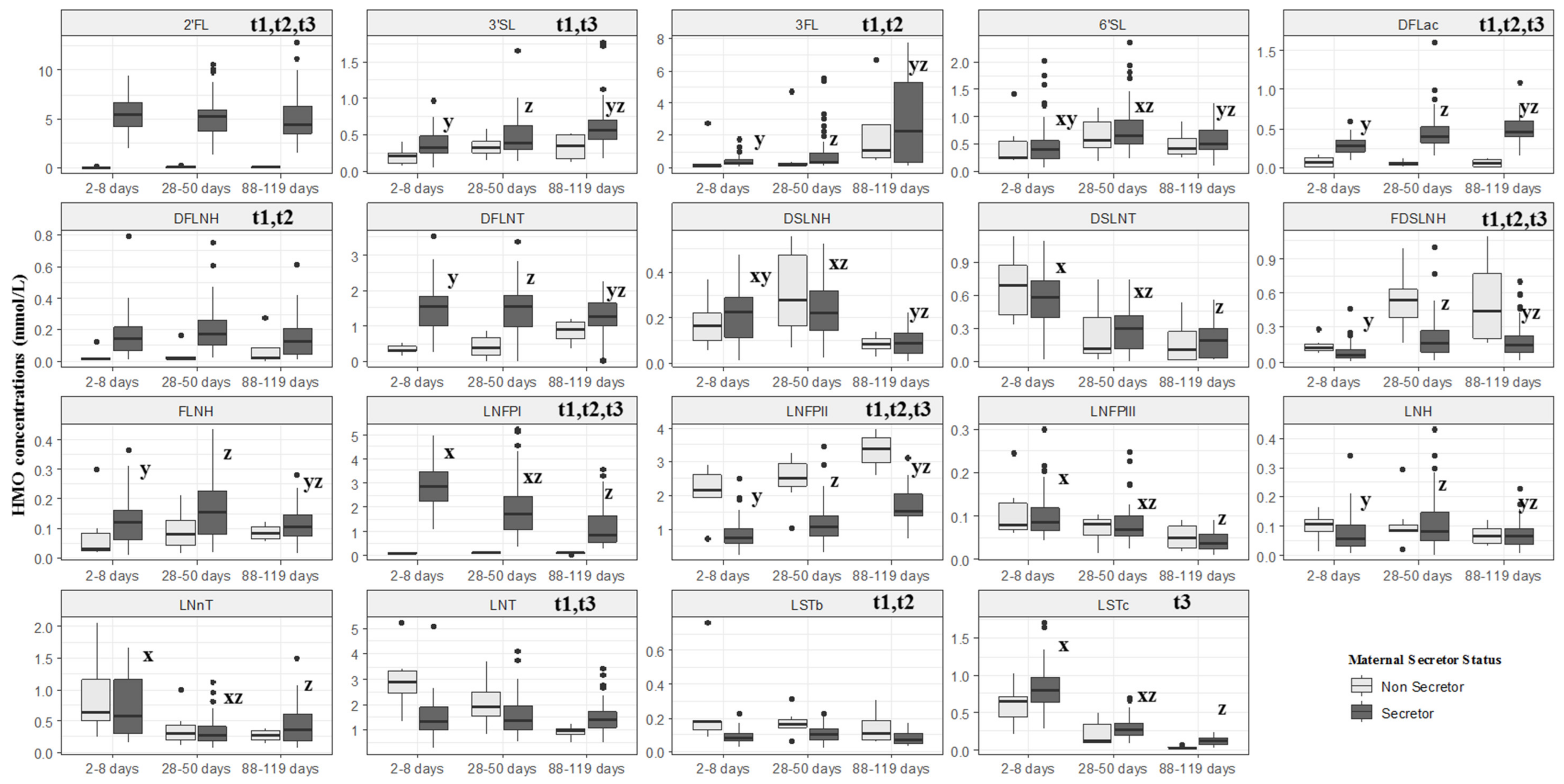
3.1. Participants and HMOs Concentrations
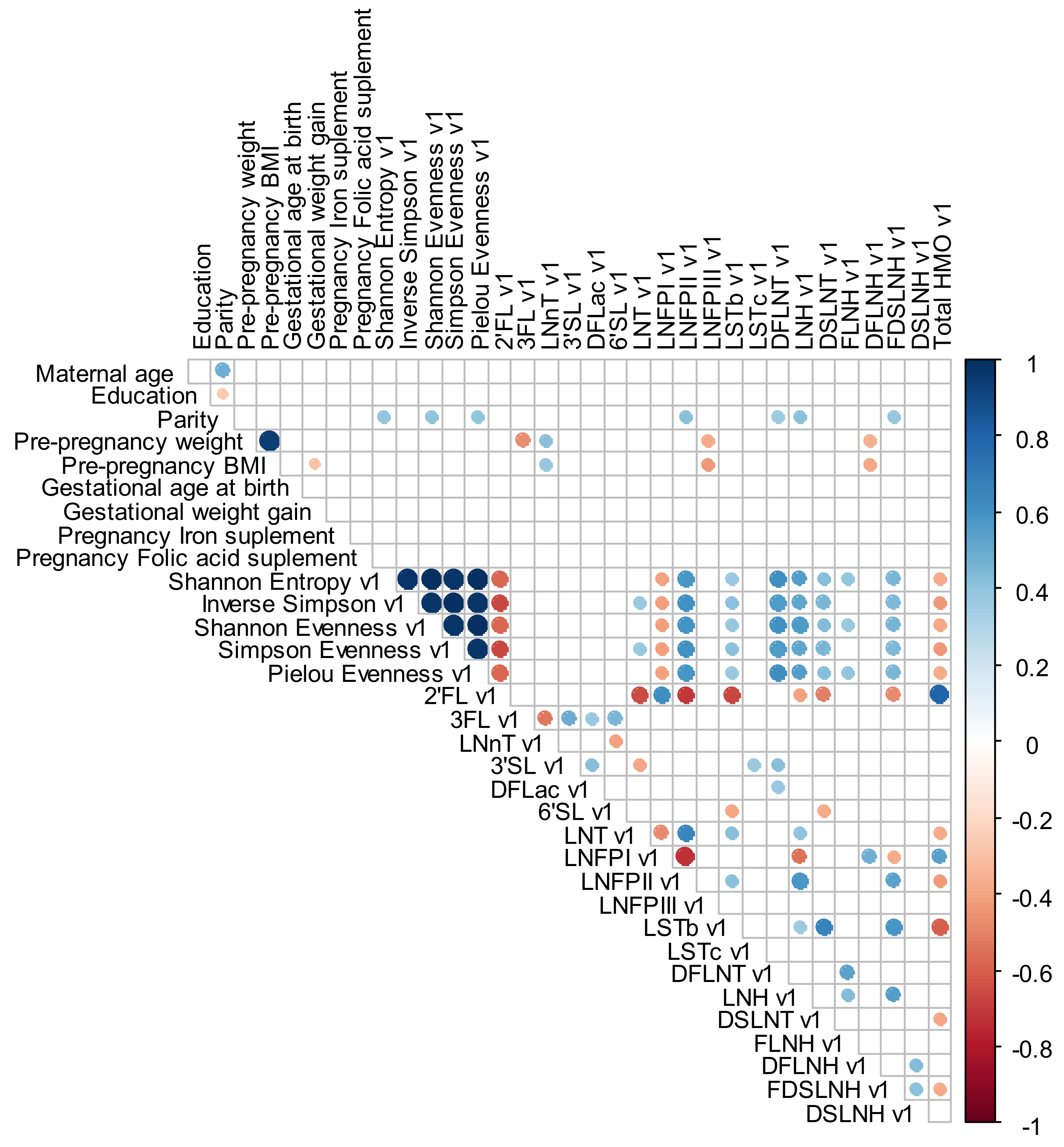
3.2. Relations between Maternal Anthropometric, Demographic and Reproductive Characteristics and HMO Compositions Concentrations
3.3. HMO Diversity and Evenness
3.4. HMO Profiles (NMF)
3.5. Sensitivity Analyses with Women with Samples in All Time Periods (n = 15)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Prentice, P.; Ong, K.K.; Schoemaker, M.H.; Van Tol, E.A.F.; Vervoort, J.; Hughes, I.A.; Acerini, C.L.; Dunger, D.B. Breast milk nutrient content and infancy growth. Acta Paediatr. 2016, 105, 641–647. [Google Scholar] [CrossRef] [Green Version]
- Bar, S.; Milanaik, R.; Adesman, A. Long-term neurodevelopmental benefits of breastfeeding. Curr. Opin. Pediatr. 2016, 28, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Giugliani, E.R.J.; Horta, B.L.; De Mola, C.L.; Lisboa, B.O.; Victora, C.G. Effect of breastfeeding promotion interventions on child growth: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 20–29. [Google Scholar] [CrossRef]
- Erick, M. Breast milk is conditionally perfect. Med. Hypotheses 2018, 111, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Bahl, R.; Barros, A.J.D.; França, G.V.A.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Escamilla, R.; Buccini, G.; Segura-Pérez, S.; Piwoz, E. Perspective: Should Exclusive Breastfeeding Still Be Recommended for 6 Months? Adv. Nutr. 2019, 10, 931–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. The Optimal Duration of Exclusive Breastfeeding Report of an Expert Consultation; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Ballard, O.; Morrow, A.L. Human milk composition: Nutrients and bioactive factors. Pediatr. Clin. North Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [Green Version]
- Fields, D.A.; Schneider, C.; Pavela, G. A narrative review of the associations between six bioactive components in breast milk and infant adiposity. Obesity 2016, 24, 1213–1221. [Google Scholar] [CrossRef] [Green Version]
- Bode, L. Human milk oligosaccharides: Every baby needs a sugar mama. Glycobiology 2012, 22, 1147–1162. [Google Scholar] [CrossRef] [Green Version]
- Urashima, T.; Hirabayashi, J.; Sato, S.; Kobata, A. Human Milk Oligosaccharides as Essential Tools for Basic and Application Studies on Galectins. Trends Glycosci. Glycotechnol. 2018, 30, SE51–SE65. [Google Scholar] [CrossRef] [Green Version]
- Bode, L. Human Milk Oligosaccharides: Next-Generation Functions and Questions. Nestle Nutr. Inst. Work. Ser. 2019, 90, 191–201. [Google Scholar]
- Davidson, B.; Meinzen-Derr, J.; Wagner, C.L.; Newburg, D.S.; Morrow, A.L. Fucosylated oligosaccharides in human milk in relation to gestational age and stage of lactation. Adv. Exp. Med. Biol. 2004, 554, 427–430. [Google Scholar] [PubMed]
- Coppa, G.V.; Gabrielli, O.; Pierani, P.; Catassi, C.; Carlucci, A.; Giorgi, P.L. Changes in carbohydrate composition in human milk over 4 months of lactation. Pediatrics 1993, 91, 637–641. [Google Scholar] [PubMed]
- Kumazaki, T.; Yoshida, A. Biochemical evidence that secretor gene, Se, is a structural gene encoding a specific fucosyltransferase. Proc. Natl. Acad. Sci. USA 1984, 81, 4193–4197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, P.H.; Watkins, W.M. Purification of the Lewis blood-group gene associated alpha-3/4-fucosyltransferase from human milk: An enzyme transferring fucose primarily to type 1 and lactose-based oligosaccharide chains. Glycoconj. J. 1992, 9, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Stanley, P.; Cummings, R. Chapter 14: Structures Common to Different Glycans. In Source Essentials of Glycobiology, 2nd ed.; Varki, A., Cummings, R., Esko, J., Freeze, H., Stanley, P., Bertozzi, C., Hart, G., Etzler, M., Eds.; Cold Spring Harbor Laboratory Press: New York, NY, USA, 2017. [Google Scholar]
- Bode, L.; Jantscher-Krenn, E. Structure-Function Relationships of Human Milk Oligosaccharides123. Adv. Nutr. 2012, 3, 383S–391S. [Google Scholar] [CrossRef] [PubMed]
- Smilowitz, J.T.; O’Sullivan, A.; Barile, D.; German, J.B.; Lönnerdal, B.; Slupsky, C.M. The human milk metabolome reveals diverse oligosaccharide profiles. J. Nutr. 2013, 143, 1709–1718. [Google Scholar] [CrossRef] [Green Version]
- Austin, S.; De Castro, C.A.; Bénet, T.; Hou, Y.; Sun, H.; Thakkar, S.K.; Pares, G.V.; Zhang, Y.; Wang, P. Temporal Change of the Content of 10 Oligosaccharides in the Milk of Chinese Urban Mothers. Nutrients 2016, 8, 346. [Google Scholar] [CrossRef] [Green Version]
- Samuel, T.M.; Binia, A.; De Castro, C.A.; Thakkar, S.K.; Billeaud, C.; Agosti, M.; Al-Jashi, I.; Costeira, M.J.; Marchini, G.; Martínez-Costa, C.; et al. Impact of maternal characteristics on human milk oligosaccharide composition over the first 4 months of lactation in a cohort of healthy European mothers. Sci. Rep. 2019, 9, 11767. [Google Scholar] [CrossRef]
- McGuire, M.; Meehan, C.L.; McGuire, M.A.; Williams, J.; Foster, J.; Sellen, D.W.; Kamau-Mbuthia, E.W.; Kamundia, E.W.; Mbugua, S.; Moore, S.E.; et al. What’s normal? Oligosaccharide concentrations and profiles in milk produced by healthy women vary geographically12. Am. J. Clin. Nutr. 2017, 105, 1086–1100. [Google Scholar] [CrossRef]
- Azad, M.B.; Robertson, B.; Atakora, F.; Becker, A.B.; Subbarao, P.; Moraes, T.; Mandhane, P.J.; Turvey, S.E.; Lefebvre, D.L.; Sears, M.R.; et al. Human Milk Oligosaccharide Concentrations Are Associated with Multiple Fixed and Modifiable Maternal Characteristics, Environmental Factors, and Feeding Practices. J. Nutr. 2018, 148, 1733–1742. [Google Scholar] [CrossRef] [PubMed]
- Austin, S.; De Castro, C.A.; Sprenger, N.; Affolter, M.; Affolter, M.; Garcia-Rodenas, C.L.; Beauport, L.; Tolsa, J.-F.; Fumeaux, C.J.F. Human Milk Oligosaccharides in the Milk of Mothers Delivering Term versus Preterm Infants. Nutrients 2019, 11, 1282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, J.C.C.; Lewis, Z.T.; Krishnan, S.; Bernstein, R.M.; Moore, S.E.; Prentice, A.M.; Mills, D.A.; Lebrilla, C.B.; Zivkovic, A.M. Growth and Morbidity of Gambian Infants are Influenced by Maternal Milk Oligosaccharides and Infant Gut Microbiota. Sci. Rep. 2017, 7, 40466. [Google Scholar] [CrossRef] [PubMed]
- Kunz, C.; Rudloff, S.; Baier, W.; Klein, N.; Strobel, S. OLIGOSACCHARIDES INHUMANMILK: Structural, Functional, and Metabolic Aspects. Annu. Rev. Nutr. 2000, 20, 699–722. [Google Scholar] [CrossRef] [PubMed]
- Bode, L. Recent Advances on Structure, Metabolism, and Function of Human Milk Oligosaccharides. J. Nutr. 2006, 136, 2127–2130. [Google Scholar] [CrossRef] [PubMed]
- Kobata, A. Structures and application of oligosaccharides in human milk. Proc. Jpn. Acad. Ser. B 2010, 86, 731–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alderete, T.; Autran, C.; Brekke, B.E.; Knight, R.; Bode, L.; Goran, M.; Fields, D.A. Associations between human milk oligosaccharides and infant body composition in the first 6 mo of life. Am. J. Clin. Nutr. 2015, 102, 1381–1388. [Google Scholar] [CrossRef]
- Wang, M.; Li, M.; Wu, S.; Lebrilla, C.B.; Chapkin, R.S.; Ivanov, I.; Donovan, S.M. Fecal Microbiota Composition of Breast-Fed Infants Is Correlated With Human Milk Oligosaccharides Consumed. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 825–833. [Google Scholar] [CrossRef] [Green Version]
- Underwood, M.; Gaerlan, S.; De Leoz, M.L.A.; Dimapasoc, L.; Kalanetra, K.M.; Lemay, D.G.; German, J.B.; Mills, D.A.; Lebrilla, C.B. Human milk oligosaccharides in premature infants: Absorption, excretion, and influence on the intestinal microbiota. Pediatr. Res. 2015, 78, 670–677. [Google Scholar] [CrossRef] [Green Version]
- Underwood, M.; Davis, J.C.C.; Kalanetra, K.M.; Gehlot, S.; Patole, S.; Tancredi, D.J.; Mills, D.A.; Lebrilla, C.B.; Simmer, K. Digestion of Human Milk Oligosaccharides by Bifidobacterium breve in the Premature Infant. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 449–455. [Google Scholar] [CrossRef]
- Paganini, D.; Uyoga, M.A.; Kortman, G.A.; Boekhorst, J.; Schneeberger, S.; Karanja, S.; Hennet, T.; Zimmermann, M. Maternal Human Milk Oligosaccharide Profile Modulates the Impact of an Intervention with Iron and Galacto-Oligosaccharides in Kenyan Infants. Nutrients 2019, 11, 2596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sprenger, N.; Lee, L.Y.; De Castro, C.A.; Steenhout, P.; Thakkar, S.K. Longitudinal change of selected human milk oligosaccharides and association to infants’ growth, an observatory, single center, longitudinal cohort study. PLoS ONE 2017, 12, e0171814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumiyoshi, W.; Urashima, T.; Nakamura, T.; Arai, I.; Saito, T.; Tsumura, N.; Wang, B.; Brand-Miller, J.; Watanabe, Y.; Kimura, K. Determination of each neutral oligosaccharide in the milk of Japanese women during the course of lactation. Br. J. Nutr. 2003, 89, 61–69. [Google Scholar] [CrossRef] [PubMed]
- REDCap. Available online: http://project-redcap.org (accessed on 30 August 2018).
- Agência Nacional de Vigilância Sanitária. Banco de Leite Humano: Funcionamento, Prevenção e Controle de Riscos; Agência Nacional de Vigilância Sanitária: Anvisa, Brazil, 2007; p. 156. [Google Scholar]
- Dave, J.; Wilcox, M.; Kellett, M. Glove powder: Implications for infection control. J. Hosp. Infect. 1999, 42, 283–285. [Google Scholar] [CrossRef]
- Jantscher-Krenn, E.; Lauwaet, T.; Bliss, L.A.; Reed, S.L.; Gillin, F.D.; Bode, L. Human milk oligosaccharides reduce Entamoeba histolytica attachment and cytotoxicity in vitro. Br. J. Nutr. 2012, 108, 1839–1846. [Google Scholar] [CrossRef] [Green Version]
- Ayechu-Muruzabal, V.; Van Stigt, A.H.; Mank, M.; Willemsen, L.E.M.; Stahl, B.; Garssen, J.; Land, B.V. Diversity of Human Milk Oligosaccharides and Effects on Early Life Immune Development. Front. Pediatr. 2018, 6, 239. [Google Scholar] [CrossRef] [Green Version]
- Triantis, V.; Bode, L.; Van Neerven, J. Immunological Effects of Human Milk Oligosaccharides. Front. Pediatr. 2018, 6, 190. [Google Scholar] [CrossRef]
- Committee on Obstetric Practice, American Institute of Ultrasound in Medicine, and Society for Maternal-Fetal Medicine. Committee Opinion No 700: Methods for Estimating the Due Date. Obstet. Gynecol. 2017, 129, e150–e154. [Google Scholar] [CrossRef]
- World Health Organization. Indicators for assessing infant and young child feeding practices. In Proceedings of the Conclusions of a Consensus Meeting, Washington, DC, USA, 6–8 November 2007. [Google Scholar]
- Foundation for Statistical Computing. A Language and Environment for Statistical Computing; Foundation for Statistical Computing: Vienna, Austria, 2015; Available online: http://www.R-project.org/ (accessed on 7 November 2019).
- Overholser, B.R.; Sowinski, K.M. Biostatistics Primer: Part 2. Nutr. Clin. Pr. 2008, 23, 76–84. [Google Scholar] [CrossRef]
- Tonon, K.M.; de Morais, M.B.; Abrão, A.C.F.V.; Miranda, A.; Morais, T.B. Maternal and Infant Factors Associated with Human Milk Oligosaccharides Concentrations According to Secretor and Lewis Phenotypes. Nutrients 2019, 11, 1358. [Google Scholar] [CrossRef] [Green Version]
- Thurl, S.; Munzert, M.; Boehm, G.; Matthews, C.; Stahl, B. Systematic review of the concentrations of oligosaccharides in human milk. Nutr. Rev. 2017, 75, 920–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thurl, S.; Munzert, M.; Henker, J.; Boehm, G.; Müller-Werner, B.; Jelinek, J.; Stahl, B. Variation of human milk oligosaccharides in relation to milk groups and lactational periods. Br. J. Nutr. 2010, 104, 1261–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conde-Agudelo, A.; Castaño, F.; Norton, M.H.; Rosas-Bermudez, A. Effects of Birth Spacing on Maternal, Perinatal, Infant, and Child Health: A Systematic Review of Causal Mechanisms. Stud. Fam. Plan. 2012, 43, 93–114. [Google Scholar] [CrossRef] [PubMed]
- Thurl, S.; Henker, J.; Taut, H.; Tovar, K.; Sawatzki, G. Variations of neutral oligosaccharides and lactose in human milk during the feeding. Eur. J. Nutr. 1993, 32, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Viverge, D.; Grimmonprez, L.; Cassanas, G.; Bardet, L.; Solère, M. Diurnal Variations and within the Feed in Lactose and Oligosaccharides of Human Milk. Ann. Nutr. Metab. 1986, 30, 196–209. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Participants | |||||||
|---|---|---|---|---|---|---|---|---|
| With Samples (n = 101) | Without Samples (n = 46) | |||||||
| Median | IQR | Mean | SD | Median | IQR | Mean | SD | |
| Maternal age (years) 1 | 26.1 | 22.8–31.6 | 27.2 | 5.5 | 27.8 | 22.8–30.4 | 26.9 | 5.4 |
| Education (years) 1 | 12.0 | 10.0–12.0 | 10.9 | 2.8 | 10.5 | 8.2–12.0 | 10.5 | 2.6 |
| Parity (livebirths) 1 | 0.0 | 0.0–1.0 | 0.7 | 0.8 | 0.5 | 0.0–1.0 | 0.8 | 1.1 |
| Pre-pregnancy weight (kg) 2 | 63.0 | 55.0–72.0 | 65.1 | 14.8 | 61.5 5 | 57.2–70.1 5 | 64.2 5 | 14.0 5 |
| Gestational age at birth (weeks) | 39.4 | 38.9–40.6 | 39.5 | 1.4 | 39.7 6 | 39.1–40.4 6 | 39.5 6 | 1.5 6 |
| Gestational weight gain (kg) | 12.4 | 8.6–15.5 | 12.4 | 6.2 | 11.77 | 8.7–18.0 7 | 12.8 7 | 7.9 7 |
| Pre-pregnancy body mass index (BMI) (kg/m2) 3 | 24.4 4 | 21.3–28.8 4 | 25.7 4 | 5.7 4 | 22.9 8 | 21.8–29.6 8 | 24.7 8 | 4.9 8 |
| n (%) | ||||||||
| Pre-pregnancy BMI categories (kg/m2) | ||||||||
| Underweight (<18.5) | 3 (3.2) 4 | 1 (6.7) 8 | ||||||
| Normal weight (18.5–24.9) | 48 (50.5) 4 | 8 (53.3) 8 | ||||||
| Overweight (≥25.0) | 44 (46.3) 4 | 6 (40.0) 8 | ||||||
| Iron supplement use (yes) 9 | 39 (42.9) | 15 (35.7) | ||||||
| Folic acid supplement (yes) 9 | 79 (87.8) | 40 (95.2) | ||||||
| HMOs | All Women—Median (IQR) (mmol/L) Days Postpartum (n) | ||
|---|---|---|---|
| 2–8 (n = 52) | 28–50 (n = 75) | 88–119 (n = 46) | |
| Fucosylated or Sialylated Lactose | |||
| 2′FL | 5.04 (4.02–6.48) | 5.04 (3.31–5.85) | 4.26 (2.96–6.16) |
| 3FL | 0.27 b (0.19–0.45) | 0.36 c (0.25–0.84) | 1.88 bc (0.39–5.29) |
| DFLac | 0.25 ab (0.17–0.35) | 0.37 ac (0.27–0.49) | 0.44 bc (0.37–0.57) |
| 3′SL | 0.32 b (0.23–0.43) | 0.38 c (0.28–0.60) | 0.54 bc (0.43–0.70) |
| 6′SL | 0.37 ab (0.22–0.58) | 0.63 ac (0.48–0.94) | 0.49 bc (0.37–0.74) |
| Non-Fucosylated, Non-Sialylated HMOs | |||
| LNT | 1.40 (1.08–2.27) | 1.45 (1.04–2.00) | 1.36 (1.03–1.71) |
| LNnT | 0.58 b (0.30–1.18) | 0.28 c (0.18–0.42) | 0.33 bc (0.17–0.58) |
| LNH | 0.06 ab (0.03–0.11) | 0.08 ac (0.06–0.14) | 0.07 bc (0.04–0.09) |
| Fucosylated, Non-Sialylated HMOs | |||
| LNFP I | 2.66 b (2.04–3.48) | 1.56 c (0.85–2.36) | 0.76 bc (0.47–1.58) |
| LNFP II | 0.77 ab (0.60–1.08) | 1.12 ac (0.90–1.58) | 1.69 bc (1.42–2.26) |
| LNFP III | 0.08 b (0.07–0.12) | 0.07 c (0.05–0.10) | 0.04 bc (0.02–0.06) |
| DFLNT | 1.47 b (0.62–1.81) | 1.42 c (0.87–1.80) | 1.20 bc (0.93–1.57) |
| FLNH | 0.11 ab (0.05–0.16) | 0.13 ac (0.08–0.22) | 0.10 bc (0.07–0.14) |
| DFLNH | 0.13 (0.05–0.21) | 0.16 (0.09–0.25) | 0.12 (0.04–0.21) |
| Non-Fucosylated, Sialylated HMOs | |||
| LSTb | 0.09 (0.07–0.12) | 0.11 (0.07–0.15) | 0.07 (0.05–0.11) |
| LSTc | 0.77 b (0.63–0.96) | 0.27 c (0.18–0.35) | 0.10 bc (0.07–0.15) |
| DSLNT | 0.58 b (0.38–0.74) | 0.30 c (0.10–0.41) | 0.18 bc (0.03–0.30) |
| DSLNH | 0.22 ab (0.11–0.27) | 0.22 ac (0.15–0.33) | 0.09 bc (0.05–0.13) |
| Fucosylated, Sialylated HMOs | |||
| FDSLNH | 0.06 ab (0.04–0.12) | 0.17 ac (0.09–0.31) | 0.16 bc (0.09–0.24) |
| Total | 16.6 b (15.66–17.36) | 15.48 c (14.73–16.42) | 16.79 bc (15.09–17.43) |
| Variable (mmol/L) | All Women | Secretors Women | Non-Secretors Women | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Days Postpartum (n) | |||||||||
| 2–8 (n = 52) | 28–50 (n = 75) | 88–119 (n = 46) | 2–8 (n = 46) | 28–50 (n = 68) | 88–119 (n = 42) | 2–8 (n = 6) | 28–50 (n = 7) | 88–119 (n = 4) | |
| Median (IQR) | |||||||||
| HMO-Bound Sialic Acid (All sialic acid moieties bound to HMOs) | 3.45 a (3.07–3.90) | 3.14 ac (2.64–3.64) | 2.40 c (1.97–2.88) | 3.45 x (3.08–3.88) | 3.00 xz (2.64–3.55) | 2.39 z (1.92–2.88) | 3.33 (3.08–3.85) | 3.85 (3.04–4.14) | 2.61 (2.34–2.89) |
| HMO-Bound Fucose (All fucose moieties bound to HMOs) | 13.59 b (12.63–14.67) | 13.436 c (11.86–14.48) | 15.04 bc (12.91–16.00) | 13.68 y (12.84–14.97) | 13.63 z (12.42–14.58) | 15.29 yz (13.22–16.09) | 3.77 (3.26–4.25) | 5.26 (3.82–5.60) | 8.09 (7.39–9.12) |
| Small HMOs (2′FL + 3FL + 3′SL + 6′SL) | 6.26 b (4.77–7.90) | 6.97 c (5.79–7.96) | 8.58 bc (7.38–10.54) | 6.66 (5.38–8.09) | 7.11 (6.22–8.11) | 8.86 (7.63–10.87) | 0.50 (0.46–0.92) | 1.53 (0.83–1.74) | 1.84 (1.42–3.58) |
| Type 1 (LNT + LNFP I + LNFP II + LSTb + DSLNT) | 5.80 a (5.30–6.58) | 4.95 ac (4.14–5.93) | 4.60 c (3.91–5.44) | 5.73 x (5.30–6.48) | 4.92 xz (4.15–5.94) | 4.50 z (3.78–5.48) | 6.26 (5.85–6.97) | 5.14 (4.46–5.69) | 4.73 (4.43–4.98) |
| Type 2 (LNnT + LNFP III + LSTc) | 1.51 a (1.19–1.94) | 0.65 ac (0.48–0.84) | 0.50 c (0.29–0.70) | 1.51 x (1.20–1.96) | 0.65 xz (0.49–0.83) | 0.55 z (0.31–0.76) | 1.40 (1.19–1.65) | 0.65 (0.43–0.93) | 0.34 (0.24–0.45) |
| Alpha 1,2 (LNFP I + 2′FL) | 7.94 (5.87–9.80) | 6.67 (4.81–8.23) | 5.36 (3.80–7.21) | 8.66 x (7.23–10.11) | 6.98 xz (5.59–8.37) | 5.53 z (4.22–7.84) | 0.12 (0.09–0.13) | 0.14 (0.12–0.18) | 0.17 (0.14–0.18) |
| Alpha 1,3 (LNFP III + 3FL) | 0.37 b (0.28–0.55) | 0.44 c (0.32–0.92) | 1.90 bc (0.42–5.30) | 0.38 y (0.30–0.55) | 0.46 z (0.34–1.02) | 2.27 yz (0.42–5.30) | 0.22 (0.14–0.26) | 0.24 (0.20–0.37) | 1.07 (0.72–2.70) |
| Alpha 2,6 (LSTc + 6′SL) | 1.28 a (0.97–1.68) | 0.92 ac (0.78–1.27) | 0.60 c (0.50–0.87) | 1.29 x (1.00–1.68) | 0.935 x (0.79–1.27) | 0.61 (0.53–0.87) | 0.92 (0.65–1.50) | 0.82 (0.53–1.15) | 0.46 (0.34–0.65) |
| Indexes | Follow Up Visits in Days Postpartum | ||
|---|---|---|---|
| 2–8 (n = 52) | 28–50 (n = 75) | 88–119 (n = 46) | |
| Shannon entropy | 2.152 ab (2.042–2.239) | 2.236 ac (2.111–2.295) | 2.073 bc (1.988– 2.189) |
| Inverse Simpson | 5.764 (4.778–6.671) | 5.890 (4.992–6.934) | 5.310 (4.525–6.238) |
| Shannon evenness | 0.730 ab (0.697–0.760) | 0.760 ac (0.715–0.780) | 0.700 bc (0.673–0.740) |
| Simpson evenness | 0.303 (0.251–0.351) | 0.310 (0.263–0.365) | 0.279 (0.238–0.328) |
| Pielou evenness | 0.731 ab (0.694–0.760) | 0.759 ac (0.717–0.780) | 0.704 bc (0.675–0.744) |
| Days Postpartum | ||||
|---|---|---|---|---|
| HMOs | 2–8 (n = 52) | 28–50 (n = 75) | 88–119 (n = 46) | All Women (n = 101) |
| Fucosylated or Sialylated Lactose | ||||
| 2′FL | 0.38 | 0.37 | 1.00 | 0.80 |
| 3FL | 0.36 | 0.74 | 0.89 | 0.01 |
| DFLac | 0.03 | 0.06 | 0.10 | 0.02 |
| 3′SL | 0.05 | 0.15 | 0.03 | 0.01 |
| 6′SL | 0.42 | 0.12 | 0.10 | 0.29 |
| Non-Fucosylated, Non-Sialylated HMOs | ||||
| LNT | 0.48 | 0.27 | 0.03 | 0.14 |
| LNnT | 0.37 | 0.04 | 0.41 | 0.89 |
| LNH | 0.38 | 0.11 | 0.13 | 0.28 |
| Fucosylated, Non-Sialylated HMOs | ||||
| LNFP I | 0.41 | 0.62 | 0.76 | 0.43 |
| LNFP II | 0.53 | 0.30 | 0.16 | 0.14 |
| LNFP III | 0.03 | 0.04 | 0.09 | 0.70 |
| DFLNT | 0.44 | 0.51 | 0.45 | 0.46 |
| FLNH | 0.10 | 0.05 | 0.01 | 0.43 |
| DFLNH | 0.27 | 0.38 | 0.38 | 0.35 |
| Fucosylated, Non-Sialylated HMOs | ||||
| LSTb | 0.45 | 0.07 | 0.13 | 0.12 |
| LSTc | 0.08 | 0.01 | 0.05 | 0.84 |
| DSLNT | 0.37 | 0.03 | 0.48 | 0.39 |
| DSLNH | 0.38 | 0.04 | 0.19 | 0.37 |
| Fucosylated, Sialylated HMOs | ||||
| FDSLNH | 0.48 | 0.31 | 0.57 | 0.38 |
| Maternal Age in Years 1 | ||||
|---|---|---|---|---|
| HMOs | 18.0–22.5 (n = 26) | 22.7–26.6 (n = 27) | 26.9–31.4 (n = 21) | 31.5–40.0 (n = 27) |
| Fucosylated or Sialylated Lactose | ||||
| 2′FL | 0.54 | 0.60 | 0.99 | 0.44 |
| 3FL | 0.16 | 0.01 | 0.06 | 0.20 |
| DFLac | 0.10 | 0.01 | 0.01 | 0.21 |
| 3′SL | 0.12 | 0.21 | 0.01 | 0.17 |
| 6′SL | 0.18 | 0.46 | 0.20 | 0.14 |
| Non-Fucosylated, Non-Sialylated HMOs | ||||
| LNT | 0.03 | 0.63 | 0.54 | 0.54 |
| LNnT | 0.65 | 0.79 | 0.92 | 0.64 |
| LNH | 0.22 | 0.09 | 0.39 | 0.03 |
| Fucosylated, Non-Sialylated HMOs | ||||
| LNFP I | 0.04 | 0.28 | 0.27 | 0.03 |
| LNFP II | 0.54 | 0.14 | 0.09 | 0.37 |
| LNFP III | 0.46 | 0.24 | 0.40 | 0.40 |
| DFLNT | 0.55 | 0.12 | 0.31 | 0.28 |
| FLNH | 0.47 | 0.30 | 0.43 | 0.08 |
| DFLNH | 0.37 | 0.02 | 0.29 | 0.44 |
| Non-Fucosylated, Sialylated HMOs | ||||
| LSTb | 0.02 | 0.06 | 0.40 | 0.05 |
| LSTc | 0.52 | 0.74 | 0.83 | 0.53 |
| DSLNT | 0.10 | 0.20 | 0.45 | 0.19 |
| DSLNH | 0.55 | 0.47 | 0.29 | 0.19 |
| Fucosylated, Sialylated HMOs | ||||
| FDSLNH | 0.24 | 0.12 | 0.25 | 0.21 |
| Pre-Pregnancy BMI in kg/m2 | ||||
|---|---|---|---|---|
| HMOs | Underweight (<18.5; n = 3) | Normal Weight (18.5–24.9; n = 48) | Overweight (25.0–29.9; n = 29) | Obesity (>29.9; n = 15) |
| Fucosylated or Sialylated Lactose | ||||
| 2′FL | 0.16 | 0.61 | 0.99 | 1.00 |
| 3FL | 0.10 | 0.05 | 0.16 | 0.04 |
| DFLac | 0.10 | 0.00 | 0.01 | 0.22 |
| 3′SL | 0.57 | 0.02 | 0.01 | 0.01 |
| 6′SL | 0.03 | 0.35 | 0.16 | 0.57 |
| Non-Fucosylated, Non-Sialylated HMOs | ||||
| LNT | 0.10 | 0.32 | 0.62 | 0.11 |
| LNnT | 0.10 | 0.80 | 0.84 | 0.90 |
| LNH | 0.04 | 0.31 | 0.19 | 0.23 |
| Fucosylated, Non-Sialylated HMOs | ||||
| LNFP I | 0.11 | 0.38 | 0.56 | 0.32 |
| LNFP II | 0.18 | 0.11 | 0.12 | 0.06 |
| LNFP III | 0.30 | 0.71 | 0.55 | 0.47 |
| DFLNT | 0.15 | 0.48 | 0.23 | 0.22 |
| FLNH | 0.31 | 0.28 | 0.35 | 0.49 |
| DFLNH | 0.28 | 0.22 | 0.10 | 0.31 |
| Non-Fucosylated, Sialylated HMOs | ||||
| LSTb | 0.07 | 0.06 | 0.33 | 0.08 |
| LSTc | 0.18 | 0.86 | 0.85 | 0.76 |
| DSLNT | 0.21 | 0.58 | 0.21 | 0.16 |
| DSLNH | 0.03 | 0.37 | 0.38 | 0.39 |
| Fucosylated, Sialylated HMOs | ||||
| FDSLNH | 0.06 | 0.30 | 0.21 | 0.31 |
| Parity in Number of Children 1 | ||||
|---|---|---|---|---|
| HMOs | 0 (n = 53) | 1 (n = 31) | 2 (n = 13) | ≥3 (n = 3) |
| Fucosylated or Sialylated Lactose | ||||
| 2′FL | 0.98 | 0.99 | 0.60 | 0.27 |
| 3FL | 0.02 | 0.01 | 0.11 | 0.44 |
| DFLac | 0.03 | 0.05 | 0.13 | 0.45 |
| 3′SL | 0.06 | 0.01 | 0.02 | 0.41 |
| 6′SL | 0.30 | 0.34 | 0.37 | 0.08 |
| Non-Fucosylated, Non-Sialylated HMOs | ||||
| LNT | 0.10 | 0.54 | 0.14 | 0.06 |
| LNnT | 0.90 | 0.96 | 0.82 | 0.50 |
| LNH | 0.26 | 0.36 | 0.17 | 0.38 |
| Fucosylated, Non-Sialylated HMOs | ||||
| LNFP I | 0.47 | 0.40 | 0.34 | 0.16 |
| LNFP II | 0.10 | 0.04 | 0.21 | 0.01 |
| LNFP III | 0.80 | 0.17 | 0.79 | 0.10 |
| DFLNT | 0.48 | 0.19 | 0.21 | 0.03 |
| FLNH | 0.46 | 0.39 | 0.19 | 0.39 |
| DFLNH | 0.35 | 0.14 | 0.18 | 0.19 |
| Non-Fucosylated, Sialylated HMOs | ||||
| LSTb | 0.03 | 0.13 | 0.11 | 0.45 |
| LSTc | 0.83 | 0.88 | 0.73 | 0.46 |
| DSLNT | 0.34 | 0.20 | 0.46 | 0.29 |
| DSLNH | 0.37 | 0.44 | 0.33 | 0.48 |
| Fucosylated, Sialylated HMOs | ||||
| FDSLNH | 0.40 | 0.04 | 0.35 | 0.23 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreira, A.L.; Alves, R.; Figueiredo, A.; Alves-Santos, N.; Freitas-Costa, N.; Batalha, M.; Yonemitsu, C.; Manivong, N.; Furst, A.; Bode, L.; et al. Human Milk Oligosaccharide Profile Variation Throughout Postpartum in Healthy Women in a Brazilian Cohort. Nutrients 2020, 12, 790. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030790
Ferreira AL, Alves R, Figueiredo A, Alves-Santos N, Freitas-Costa N, Batalha M, Yonemitsu C, Manivong N, Furst A, Bode L, et al. Human Milk Oligosaccharide Profile Variation Throughout Postpartum in Healthy Women in a Brazilian Cohort. Nutrients. 2020; 12(3):790. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030790
Chicago/Turabian StyleFerreira, Ana Lorena, Ronaldo Alves, Amanda Figueiredo, Nadya Alves-Santos, Nathalia Freitas-Costa, Mônica Batalha, Chloe Yonemitsu, Nadia Manivong, Annalee Furst, Lars Bode, and et al. 2020. "Human Milk Oligosaccharide Profile Variation Throughout Postpartum in Healthy Women in a Brazilian Cohort" Nutrients 12, no. 3: 790. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030790