Indirect Assessment of Skeletal Muscle Glycogen Content in Professional Soccer Players before and after a Match through a Non-Invasive Ultrasound Technology



Abstract
:1. Introduction
2. Methodology
2.1. Participants
2.2. Procedures
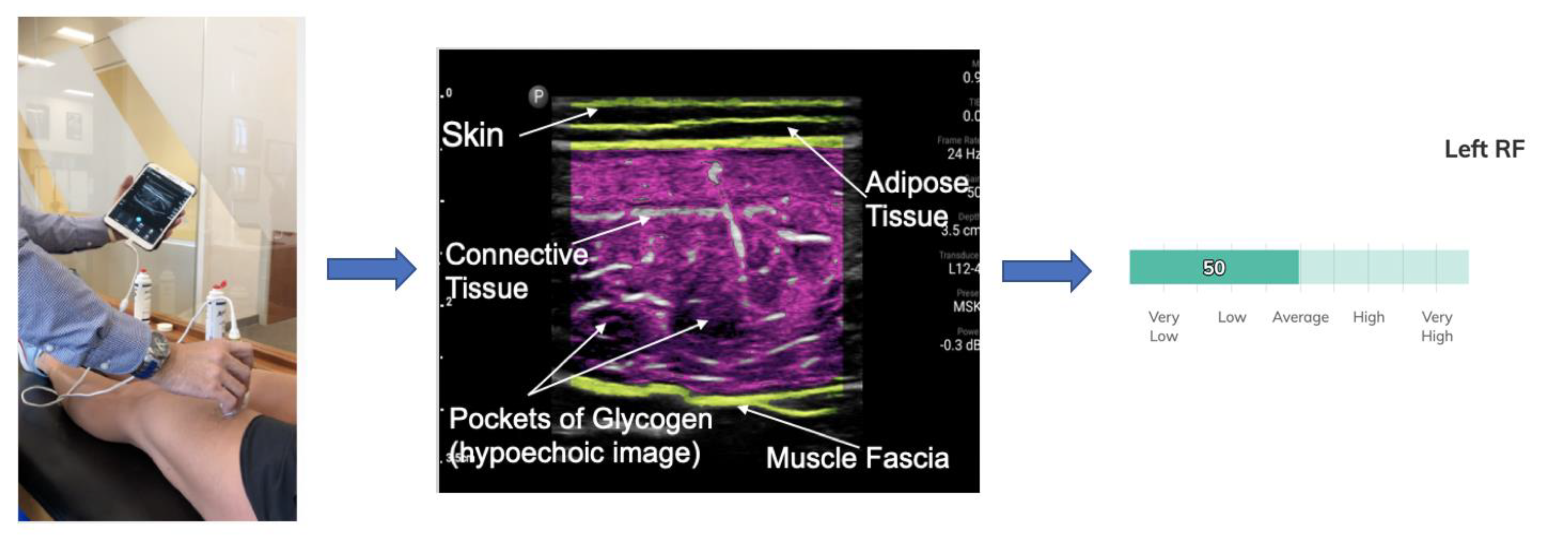
2.3. Muscle Glycogen Assessment
Pixel by Pixel Calculation to Establish the Glycogen Score Based on Ultrasound Echogenicity
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Conflicts of Interest
References
- Balsom, P.D.; Gaitanos, G.C.; Soderlund, K.; Ekblom, B. High-intensity exercise and muscle glycogen availability in humans. Acta. Physiol. Scand. 1999, 165, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Krustrup, P.; Mohr, M.; Steensberg, A.; Bencke, J.; Kjær, M.; Bangsbo, J. Muscle and blood metabolites during a soccer game: Implications for sprint performance. Med. Sci. Sports Exerc. 2006, 38, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jentjens, E.; Jeukendrup, A.E. Determinants of post-exercise glycogen synthesis during short-term recovery. Sports Med. 2003, 33, 117–144. [Google Scholar] [CrossRef] [PubMed]
- Ørtenblad, N.; Nielsen, J.; Saltin, B.; Holmberg, H.C. Role of glycogen availability in sarcoplasmic reticulum Ca2+ kinetics in human skeletal muscle. J. Physiol. 2011, 589, 711–725. [Google Scholar] [CrossRef]
- Nielsen, J.; Cheng, A.J.; Ørtenblad, N.; Westerblad, H. Subcellular distribution of glycogen and decreased tetanic Ca2+ in fatigued single intact mouse muscle fibers. J. Physiol. 2014, 592, 2003–2012. [Google Scholar] [CrossRef] [PubMed]
- Westerblad, H.; Bruton, J.D.; Allen, D.G.; Lännergren, J. Functional significance of Ca2+ in long-lasting fatigue of skeletal muscle. Eur. J. Appl. Physiol. 2000, 83, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Blomstrand, E.; Saltin, B. Effect of muscle glycogen on glucose, lactate and amino acid metabolism during exercise and recovery in human subjects. J. Physiol. 1999, 514, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Greene, J.; Louis, J.; Korostynska, O.; Mason, A. State-of-the-Art. Methods for skeletal muscle glycogen analysis in athletes-the need for novel non-invasive techniques. Biosensors (Basel) 2017, 7, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, J.C.; San Millán, I. Validation of musculoskeletal ultrasound to assess and quantify muscle glycogen content. A novel approach. Phys. Sportsm. 2014, 42, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Nieman, D.C.; Shanely, R.A.; Zwetsloot, K.A.; Meaney, M.P.; Farris, G.E. Ultrasonic assessment of exercise-induced change in skeletal muscle glycogen content. BMC Sports Sci. Med. Rehabil. 2015, 7, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Routledge, H.E.; Bradley, W.J.; Shepherd, S.O.; Cocks, M.; Erskine, R.M.; Close, G.L.; Morton, J.P. Ultrasound does not detect acute changes in glycogen in vastus lateralis of Man. Med. Sci. Sports Exerc. 2019, 51, 2286–2293. [Google Scholar] [CrossRef] [PubMed]
- Shiose, K.; Yamada, Y.; Motonaga, K.; Sagayama, H.; Higaki, Y.; Tanaka, H.; Takahashi, H. Segmental extracellular and intracellular water distribution and muscle glycogen after 72-h carbohydrate loading using spectroscopic techniques. J. Appl. Physiol. 2016, 121, 205–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiose, K.; Yamada, Y.; Motonaga, K.; Takahashi, H. Muscle glycogen depletion does not alter segmental extracellular and intracellular water distribution measured using bioimpedance spectroscopy. J. Appl. Physiol. 2018, 124, 1420–1425. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, S.S.; Wilk, M.B. An analysis of variance test for normality (complete samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Ferguson, C.J. An Effect Size Primer A Guide for Clinicians and Researchers. Prof. Psychol. Res. Pract. 2009, 40, 532–538. [Google Scholar] [CrossRef] [Green Version]
- San-Millán, I.; Brooks, G.A. Assessment of metabolic flexibility by means of measuring blood lactate, fat, and carbohydrate oxidation responses to exercise in professional endurance athletes and less-fit individuals. Sports Med. 2018, 48, 467–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohr, M.; Krustrup, P.; Bangsbo, J. Match performance of high-standard soccer players with special reference to development of fatigue. J. Sports Sci. 2003, 21, 519–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alghannam, A.F. Metabolic Limitations of Performance and Fatigue in Football. Asian J. Sports Med. 2012, 3, 65–73. [Google Scholar]
- Nicholas, C.W.; Tsintzas, K.; Boobis, L.; Williams, C. Carbohydrate-electrolyte ingestion during intermittent high-intensity running. Med. Sci. Sports Exerc. 1999, 31, 1280–1286. [Google Scholar] [CrossRef] [PubMed]
- Bradley, P.S.; Lago-Peñas, C.; Rey, E.; Díaz, A.G. The effect of high and low percentage ball possession on physical and technical profiles in English FA Premier League soccer matches. J. Sports Sci. 2013, 31, 1261–1270. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
 |
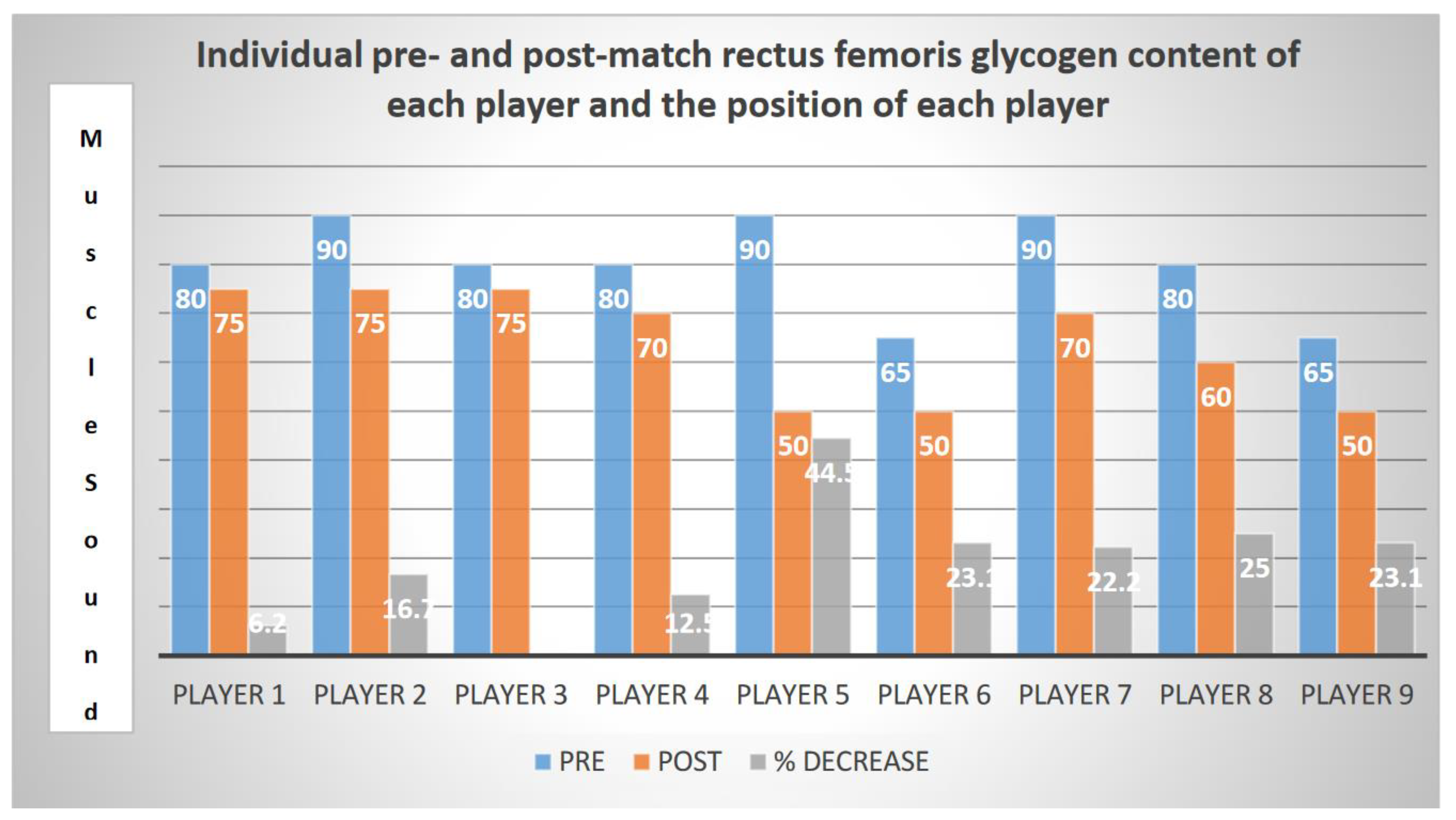
| Player | MuscleSound Score Pre | MuscleSound Score Post | % Decrease | Effect Size | Position |
|---|---|---|---|---|---|
| η2p | |||||
| Player 1 | 80 | 75 | 6.2 | Goal Keeper | |
| Player 2 | 90 | 75 | 16.7 | Defense | |
| Player 3 | 80 | 75 | 6.2 | Defense Center | |
| Player 9 | 80 | 70 | 12.5 | Defense | |
| Player 5 | 90 | 50 | 44.5 | Midfielder | |
| Player 6 | 65 | 50 | 23.1 | Midfielder | |
| Player 7 | 90 | 70 | 22.2 | Midfielder | |
| Player 8 | 80 | 60 | 25 | Forward | |
| Player 9 | 65 | 50 | 23.1 | Forward | |
| Team Average | 80 ± 8.6 | 63.9 ± 10.19 | 20 ± 10.4 | 1 | p = 0.005 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
San-Millán, I.; Hill, J.C.; Calleja-González, J. Indirect Assessment of Skeletal Muscle Glycogen Content in Professional Soccer Players before and after a Match through a Non-Invasive Ultrasound Technology. Nutrients 2020, 12, 971. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12040971
San-Millán I, Hill JC, Calleja-González J. Indirect Assessment of Skeletal Muscle Glycogen Content in Professional Soccer Players before and after a Match through a Non-Invasive Ultrasound Technology. Nutrients. 2020; 12(4):971. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12040971
Chicago/Turabian StyleSan-Millán, Iñigo, John C. Hill, and Julio Calleja-González. 2020. "Indirect Assessment of Skeletal Muscle Glycogen Content in Professional Soccer Players before and after a Match through a Non-Invasive Ultrasound Technology" Nutrients 12, no. 4: 971. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12040971