A Randomized Controlled Open Label Crossover Trial to Study Vaginal Colonization of Orally Administered Lactobacillus Reuteri RC-14 and Rhamnosus GR-1 in Pregnant Women at High Risk for Preterm Labor


Abstract
:1. Introduction
2. Subjects and Methods
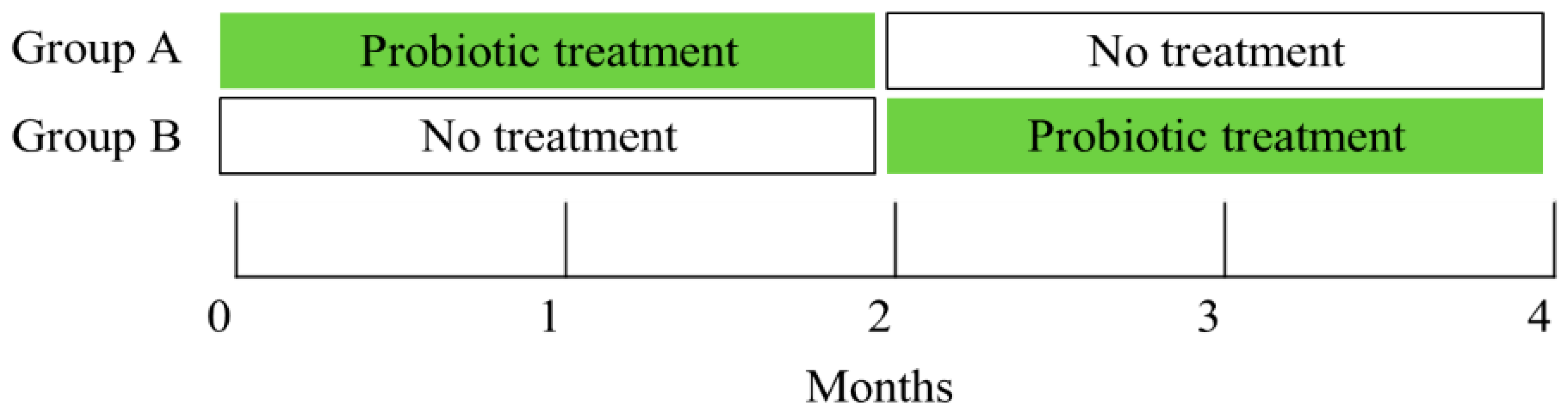
2.1. Design
2.2. Interventions
2.3. Laboratory Assessments
2.3.1. Diagnosis of Vaginal Infections
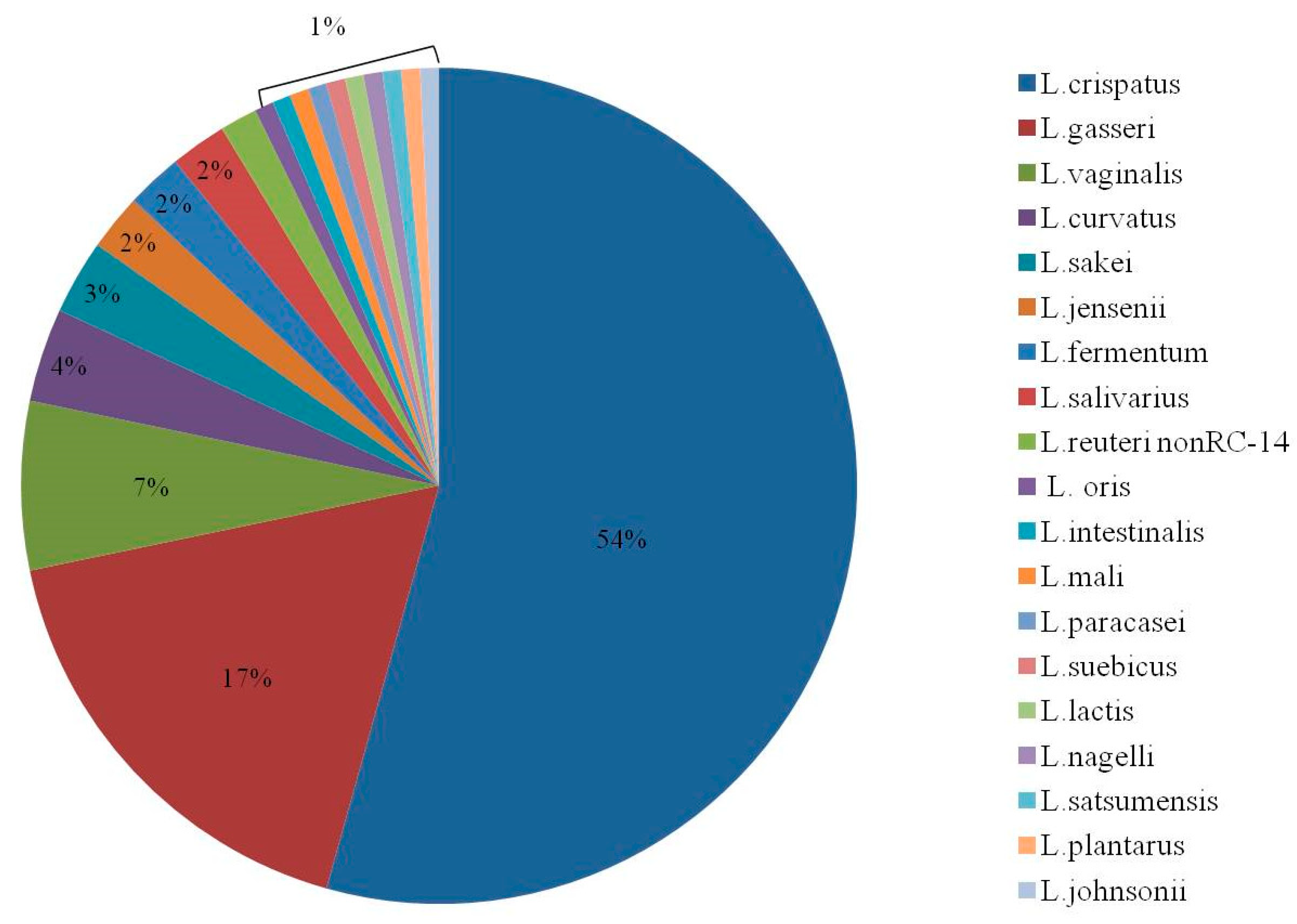
2.3.2. Identifying Vaginal Lactobacilli
2.4. Study Endpoints
2.5. Sample Size and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Carey, J.C.; Klebanoff, M.A.; Hauth, J.C.; Hillier, S.L.; Thom, E.A.; Ernest, J.M.; Heine, R.P.; Nugent, R.P.; Fischer, M.L.; Leveno, K.J.; et al. Metronidazole to prevent preterm delivery in pregnant women with asymptomatic bacterial vaginosis. National Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units. N. Engl. J. Med. 2000, 342, 534–540. [Google Scholar] [CrossRef]
- Kent, H.L. Epidemiology of vaginitis. Am. J. Obstet. Gynecol. 1991, 165, 1168–1176. [Google Scholar] [CrossRef]
- Delaney, M.L.; Onderdonk, A.B. Nugent score related to vaginal culture in pregnant women. Obstet. Gynecol. 2001, 98, 79–84. [Google Scholar] [PubMed]
- Nugent, R.P.; Krohn, M.A.; Hillier, S.L. Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J. Clin. Microbiol. 1991, 29, 297–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillier, S.L.; Martius, J.; Krohn, M.; Kiviat, N.; Holmes, K.K.; Eschenbach, D.A. A case-control study of chorioamnionic infection and histologic chorioamnionitis in prematurity. N. Engl. J. Med. 1988, 319, 972–978. [Google Scholar] [CrossRef] [PubMed]
- McGregor, J.A.; French, J.I. Bacterial vaginosis in pregnancy. Obstet. Gynecol. Surv. 2000, 55 (Suppl. 1), S1–S19. [Google Scholar] [CrossRef]
- Yudin, M.H.; Money, D.M. Screening and management of bacterial vaginosis in pregnancy. J. Obstet. Gynaecol. Can. 2008, 30, 702–716. [Google Scholar] [CrossRef]
- Ugwumadu, A.; Manyonda, I.; Reid, F.; Hay, P. Effect of early oral clindamycin on late miscarriage and preterm delivery in asymptomatic women with abnormal vaginal flora and bacterial vaginosis: A randomised controlled trial. Lancet 2003, 361, 983–988. [Google Scholar] [CrossRef]
- Oduyebo, O.O.; Anorlu, R.I.; Ogunsola, F.T. The effects of antimicrobial therapy on bacterial vaginosis in non-pregnant women. Cochrane Database Syst. Rev. 2009, 3, CD006055. [Google Scholar] [CrossRef]
- Donders, G. Diagnosis and management of bacterial vaginosis and other types of abnormal vaginal bacterial flora: A review. Obstet. Gynecol. Surv. 2010, 65, 462–473. [Google Scholar] [CrossRef]
- Borges, S.; Silva, J.; Teixeira, P. The role of lactobacilli and probiotics in maintaining vaginal health. Arch. Gynecol. Obstet. 2014, 289, 479–489. [Google Scholar] [CrossRef] [PubMed]
- De Vrese, M.; Laue, C.; Papazova, E.; Petricevic, L.; Schrezenmeir, J. Impact of oral administration of four Lactobacillus strains on Nugent score - systematic review and meta-analysis. Benef. Microbes 2019, 10, 483–496. [Google Scholar] [CrossRef] [PubMed]
- Marcone, V.; Rocca, G.; Lichtner, M.; Calzolari, E. Long-term vaginal administration of Lactobacillus rhamnosus as a complementary approach to management of bacterial vaginosis. Int. J. Gynaecol. Obstet. 2010, 110, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Reid, G.; Charbonneau, D.; Erb, J.; Kochanowski, B.; Beuerman, D.; Poehner, R.; Bruce, A.W. Oral use of Lactobacillus rhamnosus GR-1 and L. fermentum RC-14 significantly alters vaginal flora: Randomized, placebo-controlled trial in 64 healthy women. FEMS Immunol. Med. Microbiol. 2003, 35, 131–134. [Google Scholar] [CrossRef] [Green Version]
- Petricevic, L.; Unger, F.M.; Viernstein, H.; Kiss, H. Randomized, double-blind, placebo-controlled study of oral lactobacilli to improve the vaginal flora of postmenopausal women. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 141, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Shalev, E.; Battino, S.; Weiner, E.; Colodner, R.; Keness, Y. Ingestion of yogurt containing Lactobacillus acidophilus compared with pasteurized yogurt as prophylaxis for recurrent candidal vaginitis and bacterial vaginosis. Arch. Fam. Med. 1996, 5, 593–596. [Google Scholar] [CrossRef] [PubMed]
- Reid, G.; Bruce, A.W. Selection of lactobacillus strains for urogenital probiotic applications. J. Infect. Dis. 2001, 183 (Suppl. 1), S77–S80. [Google Scholar] [CrossRef]
- De Man, J.C.; Rogosa, M.; Sharpe, M.E. A medium for the cultivation of lactobacilli. J. Appl. Bacteriol. 1960, 23, 130–135. [Google Scholar] [CrossRef]
- Schmidt, F.; Fiege, T.; Hustoft, H.K.; Kneist, S.; Thiede, B. Shotgun mass mapping of Lactobacillus species and subspecies from caries related isolates by MALDI-MS. Proteomics 2009, 9, 1994–2003. [Google Scholar] [CrossRef]
- Angelakis, E.; Million, M.; Henry, M.; Raoult, D. Rapid and accurate bacterial identification in probiotics and yoghurts by MALDI-TOF mass spectrometry. J. Food. Sci. 2011, 76, M568–M572. [Google Scholar] [CrossRef]
- Petricevic, L.; Domig, K.J.; Nierscher, F.J.; Sandhofer, M.J.; Fidesser, M.; Krondorfer, I.; Husslein, P.; Kneifel, W.; Kiss, H. Characterisation of the vaginal Lactobacillus microbiota associated with preterm delivery. Sci. Rep. 2014, 4, 5136. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, G.E.; Heinemann, C.; Bruce, A.W.; Beuerman, D.; Reid, G. Persistence of Lactobacillus fermentum RC-14 and Lactobacillus rhamnosus GR-1 but not L. rhamnosus GG in the human vagina as demonstrated by randomly amplified polymorphic DNA. Clin. Diagn. Lab. Immunol. 2002, 9, 92–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petricevic, L.; Domig, K.J.; Nierscher, F.J.; Sandhofer, M.J.; Krondorfer, I.; Kneifel, W.; Kiss, H. Differences in the vaginal lactobacilli of postmenopausal women and influence of rectal lactobacilli. Climacteric 2013, 16, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Petricevic, L.; Domig, K.J.; Nierscher, F.J.; Krondorfer, I.; Janitschek, C.; Kneifel, W.; Kiss, H. Characterisation of the oral, vaginal and rectal Lactobacillus flora in healthy pregnant and postmenopausal women. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 160, 93–99. [Google Scholar] [CrossRef]
- Dommels, Y.E.; Kemperman, R.A.; Zebregs, Y.E.; Draaisma, R.B.; Jol, A.; Wolvers, D.A.; Vaughan, E.E.; Albers, R. Survival of Lactobacillus reuteri DSM 17938 and Lactobacillus rhamnosus GG in the human gastrointestinal tract with daily consumption of a low-fat probiotic spread. Appl. Environ. Microbiol. 2009, 75, 6198–6204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, R. MALDI-TOF MS for the diagnosis of infectious diseases. Clin. Chem. 2015, 61, 100–111. [Google Scholar] [CrossRef] [Green Version]
- Hamprecht, A.; Christ, S.; Oestreicher, T.; Plum, G.; Kempf, V.A.; Gottig, S. Performance of two MALDI-TOF MS systems for the identification of yeasts isolated from bloodstream infections and cerebrospinal fluids using a time-saving direct transfer protocol. Med. Microbiol. Immunol. 2014, 203, 93–99. [Google Scholar] [CrossRef]
- Fosch, S.E.; Ficoseco, C.A.; Marchesi, A.; Cocucci, S.; Nader-Macias, M.E.F.; Perazzi, B.E. Contraception: Influence on Vaginal Microbiota and Identification of Vaginal Lactobacilli Using MALDI-TOF MS and 16S rDNA Sequencing. Open Microbiol. J. 2018, 12, 218–229. [Google Scholar] [CrossRef]
- Binghuai, L.; Yanli, S.; Shuchen, Z.; Fengxia, Z.; Dong, L.; Yanchao, C. Use of MALDI-TOF mass spectrometry for rapid identification of group B Streptococcus on chromID Strepto B agar. Int. J. Infect. Dis. 2014, 27, 44–48. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Group A (Probiotic Treatment at 1 + 2 Months) n = 20 | Group B (Probiotic Treatment at 3 + 4 Months) n = 18 | p Value | |
|---|---|---|---|
| Age | 32.1 (5.0) [32.0] | 31.8 (4.0) [32.5] | 0.9 |
| Body mass index | 24.0 (3.9) [23.5] | 23.7 (4.6) [22.2] | 0.65 |
| Previous pregnancies | 3.3 (1.3) [3] | 3.9 (2.2) [3] | 0.49 |
| Number of children | 1.7 (1.0) [2] | 1.8 (1.3) [2] | 0.8 |
| Previous abortions | 0.6 (0.8) [0] | 1.2 (1.5) [1] | 0.18 |
| Previous births | 1.8 (1.1) [2.0] | 1.8 (1.4) [1.5] | 0.89 |
| Gestational week | 19.4 (4.1) [19.2] | 16.3 (3.5) [17.2] | 0.02 |
| Subjective vaginal complaints | 2 (10%) | 2 (11%) | 1 |
| Number of women with findings in per-speculum (PS) examination | 2 (10%) | 1 (6%) | 1 |
| pH > 5 | 1 (5%) | 0 (0%) | 1 |
| Positive vs. sense | 1 (5%) | 0 (0%) | 1 |
| Risk Factors for Preterm Labor * | |||
| Number of previous preterm deliveries | 0.8 (0.6) [1] | 0.3 (0.5) [0] | 0.02 |
| Preterm uterine contractions | 1 (5%) | 1 (6%) | 1 |
| Cervical shortening | 2 (10%) | 1 (6%) | 1 |
| Bleeding from placenta previa | 0 (0%) | 1 (6%) | 0.47 |
| Past abruption | 0 (0%) | 1 (6%) | 0.47 |
| Malformed uterus | 1 (5%) | 0 (0%) | 1 |
| Past preterm delivery | 14 (70%) | 6 (33%) | 0.02 |
| Past late abortion ** | 0 (0%) | 3 (17%) | 0.1 |
| Multiple pregnancy | 4 (20%) | 8 (44%) | 0.1 |
| Group A (Probiotic Treatment at 1 + 2 Months) n = 20 | Group B (Probiotic Treatment at 3 + 4 Months) n = 18 | p Value | |
|---|---|---|---|
| Compliance with study protocol $ | |||
| Full | 20 (100%) | 16 (80%) | |
| Partial | 0 (0%) | 2 (20%) | 0.11 |
| Subjective vaginal complaints | |||
| In the first 2 months of treatment * | 3 (15%) | 0 (0%) | 0.23 |
| In the second 2 months of treatment *€ | 2 (13%) | 1 (6%) | 0.59 |
| Findings in per-speculum (PS) examination | |||
| In the first 2 months of treatment * | 2 (10%) | 0 (0%) | 0.49 |
| In the second 2 months of treatment *€ | 1 (6%) | 0 (0%) | 0.47 |
| Presence of L. rhamnosus GR-1 | |||
| In the first 2 months of treatment * | 1 (5%) | 2 (11%) | 0.6 |
| In the second 2 months of treatment *€ | 0 (0%) | 3 (17%) | 0.23 |
| Vaginal infection § | |||
| In the first 2 months of treatment * | 2 (10%) | 2 (11%) | 1 |
| In the second 2 months of treatment *€ | 0 (0%) | 1 (6%) | 1 |
| Effect of crossover on L. rhamnosus GR-1 colonization € | |||
| None | 16 (100%) | 13 (72%) | 0.08 |
| lactobacili appeared | 0 (0%) | 3 (17%) | |
| lactobacili disappeared | 0 (0%) | 2 (11%) | |
| Effect of crossover on vaginal infection € | |||
| None | 15 (94%) | 15 (83%) | 1 |
| Vaginal infection resolved | 1 (6%) | 2 (11%) | |
| Vaginal infection developed | 0 (0%) | 1 (6%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yefet, E.; Colodner, R.; Strauss, M.; Gam Ze Letova, Y.; Nachum, Z. A Randomized Controlled Open Label Crossover Trial to Study Vaginal Colonization of Orally Administered Lactobacillus Reuteri RC-14 and Rhamnosus GR-1 in Pregnant Women at High Risk for Preterm Labor. Nutrients 2020, 12, 1141. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12041141
Yefet E, Colodner R, Strauss M, Gam Ze Letova Y, Nachum Z. A Randomized Controlled Open Label Crossover Trial to Study Vaginal Colonization of Orally Administered Lactobacillus Reuteri RC-14 and Rhamnosus GR-1 in Pregnant Women at High Risk for Preterm Labor. Nutrients. 2020; 12(4):1141. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12041141
Chicago/Turabian StyleYefet, Enav, Raul Colodner, Merav Strauss, Yifat Gam Ze Letova, and Zohar Nachum. 2020. "A Randomized Controlled Open Label Crossover Trial to Study Vaginal Colonization of Orally Administered Lactobacillus Reuteri RC-14 and Rhamnosus GR-1 in Pregnant Women at High Risk for Preterm Labor" Nutrients 12, no. 4: 1141. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12041141