Human Milk Feeding and Preterm Infants’ Growth and Body Composition: A Literature Review

 , , and
, , and
Abstract
:1. Introduction
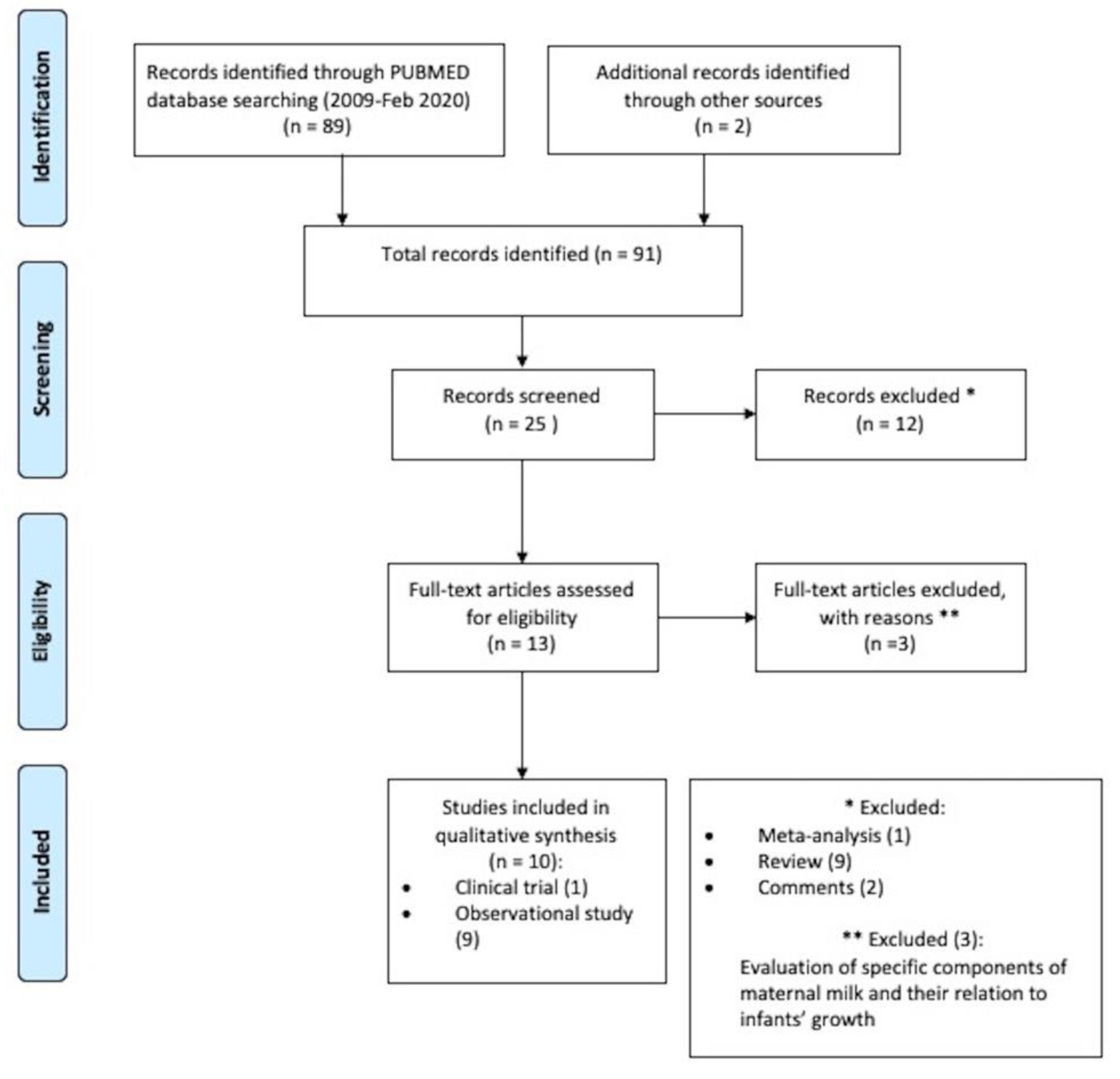
2. Materials and Methods
3. Results
3.1. Human Milk Feeding and Growth Parameters
3.2. Human Milk Feeding and Body Composition Parameters
3.3. Human Milk Feeding and Growth and Body Composition Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Vogel, J.P.; Chawanpaiboon, S.; Moller, A.B.; Watananirun, K.; Bonet, M.; Lumbiganon, P. The global epidemiology of preterm birth. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 52, 3–12. [Google Scholar] [CrossRef]
- Harrison, M.S.; Goldenberg, R.L. Global burden of prematurity. Semin. Fetal Neonatal Med. 2016, 21, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Boquien, C.Y. Human Milk: An Ideal Food for Nutrition of Preterm Newborn. Front. Pediatr. 2018, 6, 295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosca, F.; Giannì, M.L. Human Milk: Composition and Health Benefits. Pediatr. Med. Chir. 2017, 39, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bardanzellu, F.; Peroni, D.G.; Fanos, V. Human Breast Milk: Bioactive Components, from Stem Cells to Health Outcomes. Curr. Nutr. Rep. 2020, 9, 1–13. [Google Scholar] [CrossRef]
- Msall, M.E.; Sobotka, S.A.; Dmowska, A.; Hogan, D.; Sullivan, M. Life Course Health Development Outcomes After Prematurity: Developing a Community, Clinical, and Translational Research Agenda to Optimize Health, Behavior, and Functioning. In Handbook of Life Course Health Development [Internet]; Halfon, N., Forrest, C.B., Lerner, R.M., Faustman, E.M., Eds.; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Giannì, M.L.; Roggero, P.; Liotto, N.; Amato, O.; Piemontese, P.; Morniroli, D.; Bracco, B.; Mosca, F. Postnatal catch-Up fat after late preterm birth. Pediatr. Res. 2012, 72, 637–640. [Google Scholar] [CrossRef]
- Parlapani, E.; Agakidis, C.; Karagiozoglou-Lampoudi, T. Anthropometry and Body Composition of Preterm Neonates in the Light of Metabolic Programming. J. Am. Coll. Nutr. 2018, 37, 350–359. [Google Scholar] [CrossRef]
- Bonnar, K.; Fraser, D. Extrauterine Growth Restriction in Low Birth Weight Infants. Neonatal Netw. 2019, 38, 27–33. [Google Scholar] [CrossRef]
- Gianni, M.L.; Roggero, P.; Mosca, F. Human milk protein vs. formula protein and their use in preterm infants. Curr. Opin. Clin. Nutr. Metab. Care 2019, 22, 76–81. [Google Scholar] [CrossRef]
- Colaizy, T.T.; Carlson, S.; Saftlas, A.F.; Morriss, F.H., Jr. Growth in VLBW infants fed predominantly fortified maternal and donor human milk diets: A retrospective cohort study. BMC Pediatr. 2012, 12, 124. [Google Scholar] [CrossRef] [Green Version]
- Verd, S.; Porta, R.; Botet, F.; Gutiérrez, A.; Ginovart, G.; Barbero, A.H.; Ciurana, A.; Plata, I.I. Hospital outcomes of extremely low birth weight infants after introduction of donor milk to supplement mother’s milk. Breastfeed. Med. 2015, 10, 150–155. [Google Scholar] [CrossRef]
- Brownell, E.A.; Matson, A.P.; Smith, K.C.; Moore, J.E.; Esposito, P.A.; Lussier, M.M.; Lerer, T.J.; Hagadorn, I.J. Dose-Response Relationship Between Donor Human Milk, Mother’s Own Milk, Preterm Formula, and Neonatal Growth Outcomes. J. Pediatric Gastroenterol. Nutr. 2018, 67, 90–96. [Google Scholar] [CrossRef]
- Giannì, M.L.; Consonni, D.; Liotto, N.; Roggero, P.; Morlacchi, L.; Piemontese, P.; Menis, C.; Mosca, F. Does Human Milk Modulate Body Composition in Late Preterm Infants at Term-Corrected Age? Nutrients 2016, 8, 664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piemontese, P.; Liotto, N.; Mallardi, D.; Roggero, P.; Puricelli, V.; Giannì, M.L.; Morniroli, D.; Tabasso, C.; Perrone, M.; Menis, C.; et al. The Effect of Human Milk on Modulating the Quality of Growth in Preterm Infants. Front. Pediatr. 2018, 6, 291. [Google Scholar] [CrossRef]
- Morlacchi, L.; Roggero, P.; Giannì, M.L.; Bracco, B.; Porri, D.; Battiato, E.; Menis, C.; Liotto, N.; Mallardi, D.; Mosca, F. Protein use and weight-Gain quality in very-Low-Birth-Weight preterm infants fed human milk or formula. Am. J. Clin. Nutr. 2018, 107, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Mól, N.; Zasada, M.; Kwinta, P. Does type of feeding affect body composition in very low birth weight infants? -A prospective cohort study. Pediatr. Neonatol. 2019, 60, 135–140. [Google Scholar] [CrossRef] [Green Version]
- Beliaeva, I.A.; Namazova-Baranova, L.S.; Tarzian, É.O.; Skvortsova, V.A.; Boldakova, I.A. Peculiarities of physical growth and body composition of preterm infants, received different types of feeding, at the discharge from hospital. Vestn. Ross. Akad. Med. Nauk. 2014, 69, 71–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visuthranukul, C.; Abrams, S.A.; Hawthorne, K.M.; Hagan, J.L.; Hair, A.B. Premature small for gestational age infants fed an exclusive human milk-based diet achieve catch-up growth without metabolic consequences at 2 years of age. Arch. Dis. Child. Fetal Neonatal Edition 2019, 104, F242–F247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Liu, X.; Modi, N.; Uthaya, S. Impact of breast milk intake on body composition at term in very preterm babies: Secondary analysis of the Nutritional Evaluation and Optimisation in Neonates randomised controlled trial. Arch. Dis. Child. Fetal Neonatal Edition 2019, 104, F306–F312. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Boquien, C.Y.; King, C.; Lamireau, D.; Tonetto, P.; Barnett, D.; Bertino, E.; Gaya, A.; Gebauer, C.; Grovslien, A.; et al. Fortification of Human Milk for Preterm Infants: Update and Recommendations of the European Milk Bank Association (EMBA) Working Group on Human Milk Fortification. Front. Pediatr. 2019, 7, 76. [Google Scholar] [CrossRef]
- Piemontese, P.; Mallardi, D.; Liotto, L.; Tabasso, C.; Menis, C.; Perrone, M.; Roggero, P.; Mosca, F. Macronutrient content of pooled donor human milk before and after Holder pasteurization. BMC Pediatr. 2019, 19, 58. [Google Scholar] [CrossRef] [PubMed]
- Fengler, J.; Heckmann, M.; Lange, A.; Kramer, A.; Flessa, S. Cost analysis showed that feeding preterm infants with donor human milk was significantly more expensive than mother’s milk or formula. Acta Paediatr. 2019. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics, Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aceti, A.; Cavallarin, L.; Martini, S.; Giribaldi, M.; Vitali, F.; Ambretti, S.; Zambrini, V.; Corvaglia, L. Effect of Alternative Pasteurization Techniques on Human Milk’s Bioactive Proteins. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 508–512. [Google Scholar] [CrossRef]
- Taine, M.; Charles, M.A.; Beltrand, J.; Rozé, J.C.; Léger, J.; Botton, J.; Heude, B. Early postnatal growth and neurodevelopment in children born moderately preterm or small for gestational age at term: A systematic review. Paediatr. Perinat. Epidemiol. 2018, 32, 268–280. [Google Scholar] [CrossRef]
- Haschke, F.; Binder, C.; Huber-Dangl, M.; Haiden, N. Early-Life Nutrition, Growth Trajectories, and Long-Term Outcome. Nestle Nutr. Inst. Workshop Ser. 2019, 90, 107–120. [Google Scholar] [CrossRef]
- Rozé, J.C.; Darmaun, D.; Boquien, C.Y.; Flamant, C.; Picaud, J.C.; Savagner, C.; Claris, O.; Lapillonne, A.; Mitanchez, D.; Branger, B.; et al. The apparent breastfeeding paradox in very preterm infants: Relationship between breast feeding, early weight gain and neurodevelopment based on results from two cohorts, EPIPAGE and LIFT. BMJ Open. 2012, 2, e000834. [Google Scholar] [CrossRef]
- Nuyt, A.M.; Lavoie, J.C.; Mohamed, I.; Paquette, K.; Luu, T.M. Adult Consequences of Extremely Preterm Birth Cardiovascular and Metabolic Diseases Risk Factors, Mechanisms, and Prevention Avenues. Clin. Perinatol. 2017, 44, 315–332. [Google Scholar] [CrossRef]
- Mericq, V.; Martinez-Aguayo, A.; Uauy, R.; Iñiguez, G.; Van der Steen, M.; Hokken-Koelega, A. Long-Term metabolic risk among children born premature or small for gestational age. Nat. Rev. Endocrinol. 2017, 13, 50–62. [Google Scholar] [CrossRef]
- Chehade, H.; Simeoni, U.; Guignard, J.P.; Boubred, F. Preterm Birth: Long Term Cardiovascular and Renal Consequences. Curr. Pediatr. Rev. 2018, 14, 219–226. [Google Scholar] [CrossRef] [Green Version]
- Ramel, S.E.; Haapala, J.; Super, J.; Boys, C.; Demerath, E.W. Nutrition, Illness and Body Composition in Very Low Birth Weight Preterm Infants: Implications for Nutritional Management and Neurocognitive Outcomes. Nutrients 2020, 12, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Study | Type of Study | Population | Timing of Evaluation | Principal Aim | Method of Assessment | Main Findings |
|---|---|---|---|---|---|---|
| Colaizy et al. [11] | Retrospective cohort study | n = 171 infants, VLBW ≤ 1250 g | From birth to discharge | Growth in VLBW fed with increasing proportions of HM Growth in VLBW infants predominantly MM vs. predominantly DM fed | Anthropometric measurements (z-scores calculated by Fenton growth charts) | Wider reduction in weight z-score from birth to discharge in infants fed with HM > 75% compared to infants receiving HM < 75% (−0.6 vs. −0.4, p = 0.03) Decrease in weight z-score from birth to discharge (p < 0.0001) in all the different groups of HM % intake |
| Verd et al. [12] | Multi-center pre-post retrospective study before and after implementation of a donor human milk policy | n = 201, EBLW < 1000 g | From birth to discharge | Growth in VLBW infants exclusively HM vs. FM fed | Anthropometric measurements (z-scores calculated by Fenton growth charts) | No difference of weight, length or HC z-score from birth to discharge between exclusively HM and FM-fed infants |
| Brownell et al. [13] | Single-centre retrospective study | n = 314, GA < 32 weeks or ≤ 1800 g | At 36 weeks or at hospital discharge | Growth in preterm infants receiving exclusively HM or any FM | Anthropometric measurements (z-scores calculated by revised Fenton growth charts) | Reduction of adjusted mean growth velocity for weight for every 10% rise of DM amount (β −0.17, 95% CI −0.28 −0.05, p = 0.01) Adjusted mean change in weight z score decreased with increasing amounts of DM (β −0.04 95% CI −0.06 −0.02, p < 0.001), but improved with increasing proportion of FM intake (β 0.03, 95% CI 0.01 0.05, p = 0.01) Reduction of mean adjusted HC velocity for every 10% rise of DM amount (β −0.01, 95% CI −0.02 −0.001, p = 0.03) |
| Study | Type of Study | Population | Timing of Evaluation | Principal Aim | Method of Assessment | Main Findings |
|---|---|---|---|---|---|---|
| Giannì et al. [14] | Observational cohort study | n = 284, GA 34–36 weeks | At term CGA | Body composition in late preterms infants fed with exclusively MM/any MM vs. FM | Air-displacement pletysmograph (PEA POD Infant Body Composition System) | Positive association of any MM feeding at discharge and at term CGA and exclusively MM feeding at term CGA with FFM content (β =−47.9, 95%, CI = −95.7; −0.18; p = 0.049; β = −89.6, 95% CI = −131.5; −47.7; p < 0.0001; β= −104.1, 95% CI = −151.4; −56.7, p < 0.0001) |
| Piemontese et al. [15] | Longitudinal observational study | n = 73, VLBW< 1500 g, GA 26–34 weeks | At term CGA | Body composition in VLBW preterm infants fed with HM at < 50% vs. HM ≥ 50% of the total volume intake | PEA POD Infant Body Composition System | Positive association between the HM % and FFM % after correction for birth weight and gender (β = 0.12 ± 0.05, p = 0.01) Increase in FFM % at term GCA when HM ≥ 50% (p = 0.01) |
| Morlacchi et al. [16] | Prospective observational study | n = 32, VLBW< 1500 g, GA ≤ 32 weeks | At discharge and at term CGA | Body composition and protein balance in VLBW premature neonates exclusively MM vs. FM fed | PEA POD Infant Body Composition System Standard nitrogen balance method; Infrared spectroscopy analysis to assess nutritional composition of the MM; for FM, macronutrients calculated based on manufactures’ info | At discharge, higher nitrogen balance in MM-fed infants compared with FM fed (mean 488.3 ± 75 compared with 409.8 ± 85 mg kg−1 d−1, p = 0.009) At term CGA, in MM-fed compared to FM-fed infants higher FFM % (85.1 ± 2.8 vs. 80.8 ± 3.2, p = 0.002), lower ATM % (14.9 ± 2.8 vs. 19.2 ± 3.2, p = 0.002), lower ATM (458 ± 118, p = 0.004) FFM independently associated with MM feeding (R2 = 0.93, p < 0.0001) |
| Mól et al. [17] | Prospective cohort study | n = 53, VLBW 1000–1500 g | At birth and at term CGA | Body composition of VLBW newborns fed with either MM or FM compared to full-term infants | Multi-frequency impedance body composition monitor | In the FM-fed VLBW preterms compared to full-term newborns lower FFM % (83.5 vs. 85.5, p < 0.001), higher ATM % (16.4 vs.14.5, p < 0.01) and higher ATM kg (0.617 ± 0.18 vs. 0.494 ± 0.1, p = 0.02) No differences in FFM or FM between the HM fed VLBW infants and the term newborns |
| Study | Type of Study | Population | Timing of Evaluation | Principal Aim | Method of Assessment | Main Findings-Growth | Main Findings Body-Composition |
|---|---|---|---|---|---|---|---|
| Beliaeva et al. [18] | Observational cohort study | n = 80, GA 28–36 weeks | From birth to discharge | Growth and body composition in premature infants fed with FM vs. FM + MM vs. exclusively MM | Anthropometric measuraments (z-score calculated by ANTHRO-WHO 2009) Air-displacement pletysmography (PEA POD Infant Body Composition System) | Lower body weight, length, head and chest circumference at discharge in exclusively MM-fed infants compared to infants receiving FM (p < 0.05) Similar differences in premature infants (GA < 34 weeks) receiving exclusively MM compared to MM + FM-fed infants (p < 0.05) | Higher ATM in FM group compared to MM fed infants (p < 0.05) |
| Visuthranukul et al. [19] | Single-centre longitudinal cohort study | n = 51, VLBW ≤ 1250 g, GA < 37 weeks | At 12–15 months (visit 1) and at 18–22 months CGA (visit 2) | Growth and body composition of VLBW SGA vs. AGA exclusively fed with HM | Anthropometric measurements with centile (WHO growth data) Dual-energy X-ray absorptiometry | SGA greater BMI z-score gain from visit 1 to visit 2 (0.25 ± 1.10 vs. −0.21 ± 0.84, p = 0.02), also after controlling for GA and diet at discharge (p = 0.004) In both SGA and AGA groups, from birth to visit 2: increase of weight (from 3rd-25th pcl to 25th pcl; from 25th pcl to 50th pcl, respectively, p = 0.022) and HC (from 3rd-10th pcl to 25th pcl; from 10th-25th pcl to 50th pcl, respectively, p = 0.002) | No difference in body composition between the two groups |
| Li et al. [20] | Preplanned secondary analysis of the Nutritional Evaluation and Optimisation in Neonates (NEON) trial | n = 133, GA < 31 weeks | At birth and at term CGA | Body composition at term CGA in very preterm infants HM vs. FM fed | Anthropometric measurements (growth charts used for calculation of z-scores not mentioned) Whole body MRI | Predominantly FM group weighed more than the exclusively HM-fed group, mean difference 283.6 g (95% CI, 121.6–445.6) Greater positive weight Z-score change between birth and term CGA in predominantly FM group compared to exclusively HM-fed group, mean difference 0.6 (95% CI, 0.2–1.0), p < 0.01 | Higher FFM in predominantly FM-fed group than in exclusively HM-fed group, mean difference 257.4 g (95% CI, 139.1–375.7 g), p < 0.01 No significant differences between exclusively HM-fed group in ATM or % ATM and the predominantly HM and predominantly FM-fed groups, respectively. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cerasani, J.; Ceroni, F.; De Cosmi, V.; Mazzocchi, A.; Morniroli, D.; Roggero, P.; Mosca, F.; Agostoni, C.; Giannì, M.L. Human Milk Feeding and Preterm Infants’ Growth and Body Composition: A Literature Review. Nutrients 2020, 12, 1155. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12041155
Cerasani J, Ceroni F, De Cosmi V, Mazzocchi A, Morniroli D, Roggero P, Mosca F, Agostoni C, Giannì ML. Human Milk Feeding and Preterm Infants’ Growth and Body Composition: A Literature Review. Nutrients. 2020; 12(4):1155. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12041155
Chicago/Turabian StyleCerasani, Jacopo, Federica Ceroni, Valentina De Cosmi, Alessandra Mazzocchi, Daniela Morniroli, Paola Roggero, Fabio Mosca, Carlo Agostoni, and Maria Lorella Giannì. 2020. "Human Milk Feeding and Preterm Infants’ Growth and Body Composition: A Literature Review" Nutrients 12, no. 4: 1155. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12041155