Influence of Sunlight and Oral D3 Supplementation on Serum 25(OH)D Concentration and Exercise Performance in Elite Soccer Players

 , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Subjects
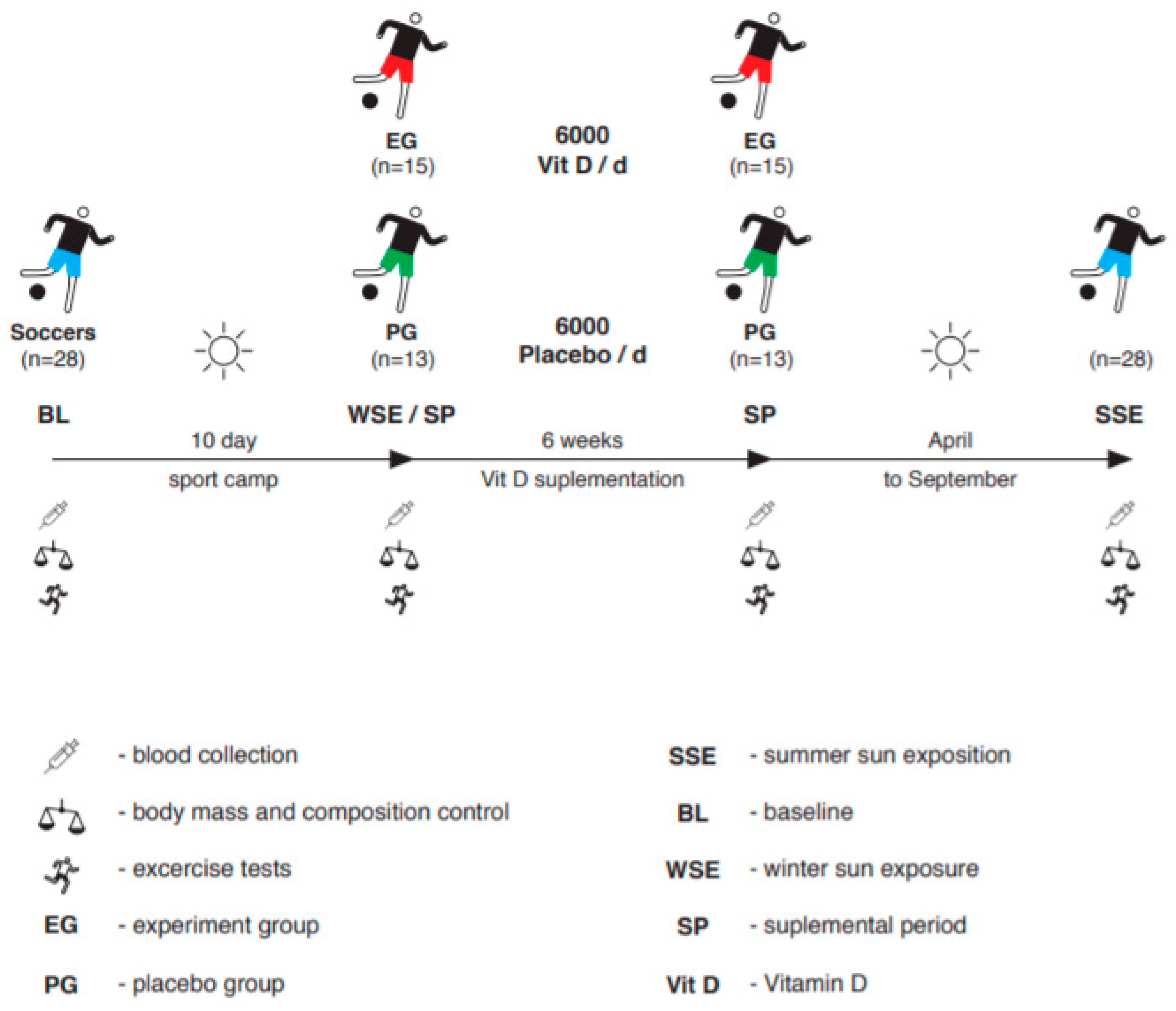
2.2. Study Design
2.3. Supplementation
2.4. Training Program
2.5. Sprint Test
2.6. PLL Test
2.7. VO2max Test
2.8. Biochemical Analysis
2.9. Body Mass and Body Composition Evaluation
2.10. Statistics Analysis
3. Results
4. Discussion
5. Conclusions
6. Strengths and limitations
Author Contributions
Funding
Conflicts of Interest
References
- Dzik, K.P.; Kaczor, J.J. Mechanisms of vitamin D on skeletal muscle function: Oxidative stress, energy metabolism and anabolic state. Eur. J. Appl. Physiol. 2019, 119, 825–839. [Google Scholar] [CrossRef] [Green Version]
- Jastrzębska, M.; Kaczmarczyk, M.; Jastrzębski, Z. The effect of vitamin d supplementation on training adaptation in well trained soccer players. J. Strength Cond. Res. 2016, 30, 2648–2655. [Google Scholar] [CrossRef] [PubMed]
- Lerchbaum, E.; Trummer, C.; Theiler-Schwetz, V.; Kollmann, M.; Wölfler, M.; Annemieke, C.; Heijboer, A.C.; Pilz, S.; Obermayer-Pietsch, B. Effects of vitamin D supplementation on androgens in men with low testosterone levels: A randomized controlled trial. Eur. J. Nutr. 2019, 58, 3135–3146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagpal, S.; Rathnachalam, R. Noncalcemic actions of vitamin D receptor ligands. Endocr. Rev. 2005, 26, 662–687. [Google Scholar] [CrossRef] [PubMed]
- Dahlquist, D.T.; Dieter, B.P.; Koehle, M.S. Plausible ergogenic effects of vitamin D on athletic performance and recovery. J. Int. Soc. Sports Nutr. 2015, 12, 33. [Google Scholar] [CrossRef] [Green Version]
- Wiciński, M.; Adamkiewicz, D.; Adamkiewicz, M.; Śniegocki, M.; Podhorecka, M.; Szychta, P.; Malinowski, B. Impact of Vitamin D on Physical Efficiency and Exercise Performance—A Review. Nutrients 2019, 11, 2826. [Google Scholar] [CrossRef] [Green Version]
- Jastrzebska, M.; Kaczmarczyk, M.; Michalczyk, M.; Radziminski, L.; Stepien, P.; Jastrzebska, J.; Wakuluk, D.; Suarez, A.D.; Lopez Sanchez, G.F.; Cieszczyk, P.; et al. Can Supplementation of Vitamin D Improve Aerobic Capacity in Well Trained Youth Soccer Players? J. Hum. Kinet. 2018, 61, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Krzywanski, J.; Mikulski, T.; Krysztofiak, M.; Dlynczak, M.; Gaczynska, M.; Ziemba, A. Seasonal Vitamin D Status in Polish Elite Athletes in Relation to Sun Exposure and Oral Supplementation. PLoS ONE 2016, 11, e0164395. [Google Scholar] [CrossRef]
- Carswell, A.T.; Oliver, S.J.; Wentz, L.M.; Kashi, D.S.; Roberts, R.; Tang, J.C.; Izard, R.M.; Jackson, S.; Allan, D.; Rhodes, L.E. Influence of Vitamin D Supplementation by Sunlight Or Oral D3 on Exercise Performance. Med. Sci. Sports Exerc. 2018, 50, 2555–2564. [Google Scholar] [CrossRef] [Green Version]
- Farrán, A.; Zamora, R.; Cervera, P. Tablas De Composición De Alimentos Del Centre D’Ensenyament Superior De Nutrició i Dietètica (CESNID); Universitat de Barcelona: Barcelona, Spain, 2004. [Google Scholar]
- Cassity, E.P.; Redzic, M.; Cassidy, R.T.; Travis, D.T. The effect of body composition and BMI on 25(OH)D response in vitamin D-supplemented athletes. Eur. J. Sport Sci. 2016, 16, 773–779. [Google Scholar] [CrossRef] [Green Version]
- Shuler, F.D.; Wingate, M.K.; Moore, G.H.; Giangarra, C. Sports health benefits of vitamin D. Sports Health 2012, 4, 496–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mielgo-Ayuso, J.; Calleja-González, J.; Urdampilleta, A.; León-Guereño, P.; Córdova, A.; Caballero-García, A.; Fernandez-Lázaro, D.; Calleja-González, J.; Urdampilleta, A.; León-Guereño, P.; et al. Effects of Vitamin D Supplementation on Haematological Values and Muscle Recovery in Elite Male Traditional Rowers. Nutrients 2018, 10, 1968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Close, G.L.; Russell, J.; Cobley, J.N.; Owens, D.J.; Wilson, G.; Gregson, W.; Fraser, W.D.; Morton, J.P. Assessment of vitamin D concentration in nonsupplemented professional athletes and healthy adults during the winter months in the UK: Implications for skeletal muscle function. J. Sports Sci. 2013, 31, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Aydin, C.G.; Dinçel, Y.M.; Arıkan, Y.; Taş, S.K.; Deniz, S. The effects of indoor and outdoor sports participation and seasonal changes on vitamin D levels in athletes. SAGE Open Med. 2019, 7, 2050312119837480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrokhyar, F.; Tabasinejad, R.; Dao, D.; Peterson, D.; Ayeni, O.R.; Hadioonzadeh, R.; Bhandari, M. Prevalence of vitamin D inadequacy in athletes: A systematic-review and meta-analysis. Sports Med. 2015, 45, 365–378. [Google Scholar] [CrossRef] [PubMed]
- Larson-Meyer, D.E.; Willis, K.S. Vitamin D and athletes. Curr. Sports Med. Rep. 2010, 9, 220–226. [Google Scholar] [CrossRef] [Green Version]
- Girgis, C.M.; Clifton-Bligh, R.J.; Hamrick, M.W.; Holick, M.F.; Gunton, J.E. The roles of vitamin D in skeletal muscle: Form, function, and metabolism. Endocr. Rev. 2013, 34, 33–83. [Google Scholar] [CrossRef] [Green Version]
- Dzedzej, A.; Ignatiuk, W.; Jaworska, J.; Grzywacz, T.; Lipińska, P.; Antosiewicz, J.; Korek, A.E. The effect of the competitive season in professional basketball on inflammation and iron metabolism. Biol. Sport 2016, 33, 223–229. [Google Scholar] [CrossRef]
- Skalska, M.; Nikolaidis, P.T.; Knechtle, B.; Rosemann, T.J.; Radzimiński, Ł.; Jastrzębska, J.; Kaczmarczyk, M.; Myśliwiec, A.; Dragos, P.; López-Sánchez, G.F.; et al. Vitamin D Supplementation and Physical Activity of Young Soccer Players during High-Intensity Training. Nutrients 2019, 11, 349. [Google Scholar] [CrossRef] [Green Version]
- Cannell, J.J.; Hollis, B.W.; Sorenson, M.B.; Taft, T.N.; Anderson, J.J. Athletic performance and vitamin D. Med. Sci. Sports Exerc. 2009, 41, 1102–1110. [Google Scholar] [CrossRef]
- Nimptsch, K.; Platz, E.A.; Willett, W.C.; Giovannucci, E. Association between Plasma 25-OH Vitamin D and Testosterone Levels in Men. Clin. Endocrinol. 2012, 77, 106–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Zhai, H.; Cheng, J.; Weng, P.; Chen, Y.; Li, Q.; Wang, C.; Xia, F.; Wang, N.; Lu, Y. Causal Link Between Vitamin D and Total Testosterone in Men: A Mendelian Randomization Analysis. J. Clin. Endocrinol. Metab. 2019, 104, 3148–3156. [Google Scholar] [CrossRef] [PubMed]
- West, D.W.; Phillips, S.M. Anabolic processes in human skeletal muscle restoring the identities of growth hormone and testosterone. Physician Sportsmed. 2010, 38, 97–104. [Google Scholar] [CrossRef]
- Michalczyk, M.M.; Chycki, J.; Zajac, A.; Maszczyk, A.; Zydek, G.; Langfort, J. Anaerobic Performance after a Low-Carbohydrate Diet (LCD) Followed by 7 Days of Carbohydrate Loading in Male Basketball Players. Nutrients 2019, 11, 778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilz, S.; Frisch, S.; Koertke, H.; Kuhn, J.; Dreier, J.; Obermayer-Pietsch, B.; Wehr, E.; Zittermann, A. Effect of vitamin D supplementation on testosterone levels in men. Horm. Metab. Res. 2011, 43, 223–225. [Google Scholar] [CrossRef]
- Lerchbaum, E.; Pilz, S.; Trummer, C.; Schwetz, V.; Pachernegg, O.; Heijboer, A.C.; Obermayer-Pietsch, B. Vitamin D and Testosterone in Healthy Men: A Randomized Controlled Trial. J. Clin. Endocrinol. Metab. 2017, 102, 4292–4302. [Google Scholar] [CrossRef]
- Saha, S.; Goswami, R.; Ramakrishnan, L.; Vishnubhatla, S.; Mahtab, S.; Kar, P.; Srinivasan, S.; Singh, N.; Singh, U. Vitamin D and calcium supplementation, skeletal muscle strength and serum testosterone in young healthy adult males: Randomized control trial. Clin. Endocrinol. 2018, 88, 217–226. [Google Scholar] [CrossRef]
- Kopeć, A.; Solarz, K.; Majda, F.; Słowińska-Lisowska, M.; Mędraś, M. An evaluation of the levels of vitamin D and bone turnover markers after the summer and winter periods in polish professional soccer players. J. Hum. Kinet. 2013, 38, 135–140. [Google Scholar] [CrossRef]
- Michalczyk, M.M.; Chycki, J.; Zajac, A.; Petr, M.; Czuba, M.; Langfort, J. Three weeks of intermittent hypoxic training affect antioxidant enzyme activity and increases lipid peroxidation in cyclists. Chem. Mon. 2019, 150, 1703–1710. [Google Scholar] [CrossRef]
- Hopkins, W.G. Linear models and effect magnitudes for research, clinical and practical applications. Sportscience 2010, 14, 49–57. [Google Scholar]
- Książek, A.; Zagrodna, A.; Słowińska-Lisowska, M. Vitamin D, Skeletal Muscle Function and Athletic Performance in Athletes-A Narrative Review. Nutrients 2019, 11, 1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halliday, T.M.; Peterson, N.J.; Thomas, J.J.; Kleppinger, K.; Hollis, B.W.; Larson-Meyer, D.E. Vitamin D status relative to diet, lifestyle, injury, and illness in college athletes. Med. Sci. Sports Exerc. 2011, 43, 335–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heijboer, A.C.; Oosterwerff, M.; Schroten, N.F.; Eekhoff, E.M.; Chel, V.G.; de Boer, R.A.; Blankenstein, M.A.; Lips, P. Vitamin D supplementation and testosterone concentrations in male human subjects. Clin. Endocrinol. 2015, 83, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, P.; Santos, A.C.; Casalta-Lopes, J.; Almeida, M.; Loureiro, J.; Ermida, V.; Caldas, J.; Fontes-Ribeiro, C. Prevalence of vitamin D deficiency amongst soccer athletes and effects of 8 weeks supplementation. J. Sports Med. Phys. Fit. 2019, 59, 693–699. [Google Scholar] [CrossRef]
- Kilby, K.; Mathias, H.; Boisvenue, L.; Heisler, C.; Jones, J.L. Micronutrient Absorption and Related Outcomes in People with Inflammatory Bowel Disease: A Review. Nutrients 2019, 11, 1388. [Google Scholar] [CrossRef] [Green Version]
- Barbáchano, A.; Fernández-Barral, A.; Ferrer-Mayorga, G.; Costales-Carrera, A.; Larriba, M.J.; Muñoz, A. The endocrine vitamin D system in the gut. Mol. Cell. Endocrinol. 2017, 453, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Lombardi, G.; Vitale, J.A.; Logoluso, S.; Logoluso, G.; Cocco, N.; Cocco, G.; Cocco, A.; Banfi, G. Circannual Rhythm of Plasmatic Vitamin D Levels and the Association with Markers of Psychophysical Stress in a Cohort of Italian Professional Soccer Players. Chronobiol. Int. 2017, 34, 471–479. [Google Scholar] [CrossRef]
- Bouillon, R.; Carmeliet, G.; Verlinden, L.; van Etten, E.; Verstuyf, A.; Luderer, H.F.; Lieben, L.; Mathieu, C.; Demay, M. Vitamin D and human health: Lessons from vitamin D receptor null mice. Endocr. Rev. 2008, 29, 726–776. [Google Scholar] [CrossRef]
- Rolf, L.; Damoiseaux, J.; Huitinga, I.; Kimenai, D.; van den Ouweland, J.; Hupperts, R.; Smolders, J. Stress-Axis Regulation by Vitamin D3 in Multiple Sclerosis. Front. Neurol. 2018, 9, 263. [Google Scholar] [CrossRef] [Green Version]
- Banfi, G.; Marinelli, M.; Roi, G.S.; Agape, V. Usefulness of free testosterone/cortisol ratio during a season of elite speed skating athletes. Int. J. Sports Med. 1993, 14, 373–379. [Google Scholar] [CrossRef]
- Oshima, S.; Takehata, C.; Sasahara, I.; Lee, E.; Akama, T.; Taguchi, O. Changes in Stress and Appetite Responses in Male Power-Trained Athletes during Intensive Training Camp. Nutrients 2017, 9, 912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogan, D.; Pritchett, K. Vitamin D and the athlete: Risks, recommendations, and benefits. Nutrients 2013, 5, 1856–1868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koundourakis, N.E.; Avgoustinaki, P.D.; Malliaraki, N.; Margioris, A.N. Muscular effects of vitamin D in young athletes and non-athletes and in the elderly. Hormones 2016, 15, 471–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giminiani, R.D.; Visca, C. Explosive strength and endurance adaptations in young elite soccer players during two soccer seasons. PLoS ONE 2017, 12, e0171734. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | BL | WSE | EG | PG | SSE | ||
|---|---|---|---|---|---|---|---|
| Before supl | After supl | Before supl | After supl | ||||
| fT, pg/mL | 10.16 ± 3.2 | 18.78 ± 5.3# | 18.66 ± 5.3 | 28.86 ± 3.6* | 18.21 ± 4.9 | 23.20 ± 5.2 | 20.84 ± 4.9## |
| tT, nmol/L | 19.22 ± 4.8 | 23.86 ± 6.5# | 22.95 ± 6.4 | 28.25 ± 3.2* | 23.64 ± 3.9 | 26.60 ± 5.1 | 20.42 ± 5.3 |
| Cortisol, μg/L | 357.61 ± 133.0 | 469.47# ± 142.4 | 469.50 ± 142.4 | 517.38 ± 127.8 | 512.44 ± 103.6 | 572.750 ± 227.12 | 739.53## ± 180.1 |
| Variables | BL | WSE | EG | PG | SSE | ||
|---|---|---|---|---|---|---|---|
| Before supl | After supl | Before supl | After supl | ||||
| VO2max, ml/kgO2/min | 56.57 ± 3.9 | 58.00 ± 4.9 | 57.8 ± 4.8 | 58.92 ± 5.3 | 58.0 ± 3.4 | 59.0 ± 3.9 | 58.05 ± 4.6 |
| 5m ST, s | 1.13 ± 0.05 | 1.09 ± 0.04# | 1.09 ± 0.04 | 1.04 ± 0.03# | 1.08 ± 0.06 | 1.06 ± 0.07 | 1.11 ± 0.06 |
| 30m ST, s | 4.20 ± 0.08 | 4.15 ± 0.07 | 4.16 ± 0.08 | 4.09 ± 0.09 | 4.16 ± 0.09 | 4.09 ± 0.1 | 4.16 ± 0.07 |
| PLL, watt | 1600.76 ± 124.7 | 1665.83 ± 116.7 | 1665.84 ± 116.7 | 1720.61 ± 113.2 | 1610.25 ± 11.8 | 1685.00 ± 96.2 | 1672.90 ± 112.8 |
| Variables | BL | WSE | EG | PG | SSE | ||
|---|---|---|---|---|---|---|---|
| Before supl | After supl | Before supl | After supl | ||||
| Body mass, kg | 77.81 ± 8.8 | 78.74 ± 8.4 | 78.74 ± 9.4 | 80.08 ± 8.5 | 75.47 ± 7.0 | 77.37 ± 6.0 | 80.60 ± 9.9 |
| Body fat, % | 12.38 ± 2.4 | 10.77 ± 1.4 | 10.67 ± 2.2 | 7.69 ± 2.4 | 9.87 ± 2.8 | 7.49 ± 2.8 | 7.5 ± 2.6 |
| Muscle mass, kg | 40.27 ± 5.3 | 41.52 ± 4.2 | 40.25 ± 3.4 | 44.15 ± 4.5 | 40.62 ± 5.5 | 42.16 ± 5.9 | 40.70 ± 5.2 |
| Variables | Pearson correlation |
|---|---|
| 25(OH)D | |
| Body fat | 0.341 |
| Muscle mass | 0.397 |
| VO2max | 0.017 |
| 5 m ST | −0.054 |
| 30 m ST | −0.052 |
| PLL | 0.021 |
| Cortisol | −0.237 |
| fT | 0.638 |
| Tt | 0.609 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michalczyk, M.M.; Gołaś, A.; Maszczyk, A.; Kaczka, P.; Zając, A. Influence of Sunlight and Oral D3 Supplementation on Serum 25(OH)D Concentration and Exercise Performance in Elite Soccer Players. Nutrients 2020, 12, 1311. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12051311
Michalczyk MM, Gołaś A, Maszczyk A, Kaczka P, Zając A. Influence of Sunlight and Oral D3 Supplementation on Serum 25(OH)D Concentration and Exercise Performance in Elite Soccer Players. Nutrients. 2020; 12(5):1311. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12051311
Chicago/Turabian StyleMichalczyk, Małgorzata Magdalena, Artur Gołaś, Adam Maszczyk, Piotr Kaczka, and Adam Zając. 2020. "Influence of Sunlight and Oral D3 Supplementation on Serum 25(OH)D Concentration and Exercise Performance in Elite Soccer Players" Nutrients 12, no. 5: 1311. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12051311