Difensil Immuno Reduces Recurrence and Severity of Tonsillitis in Children: A Randomized Controlled Trial

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
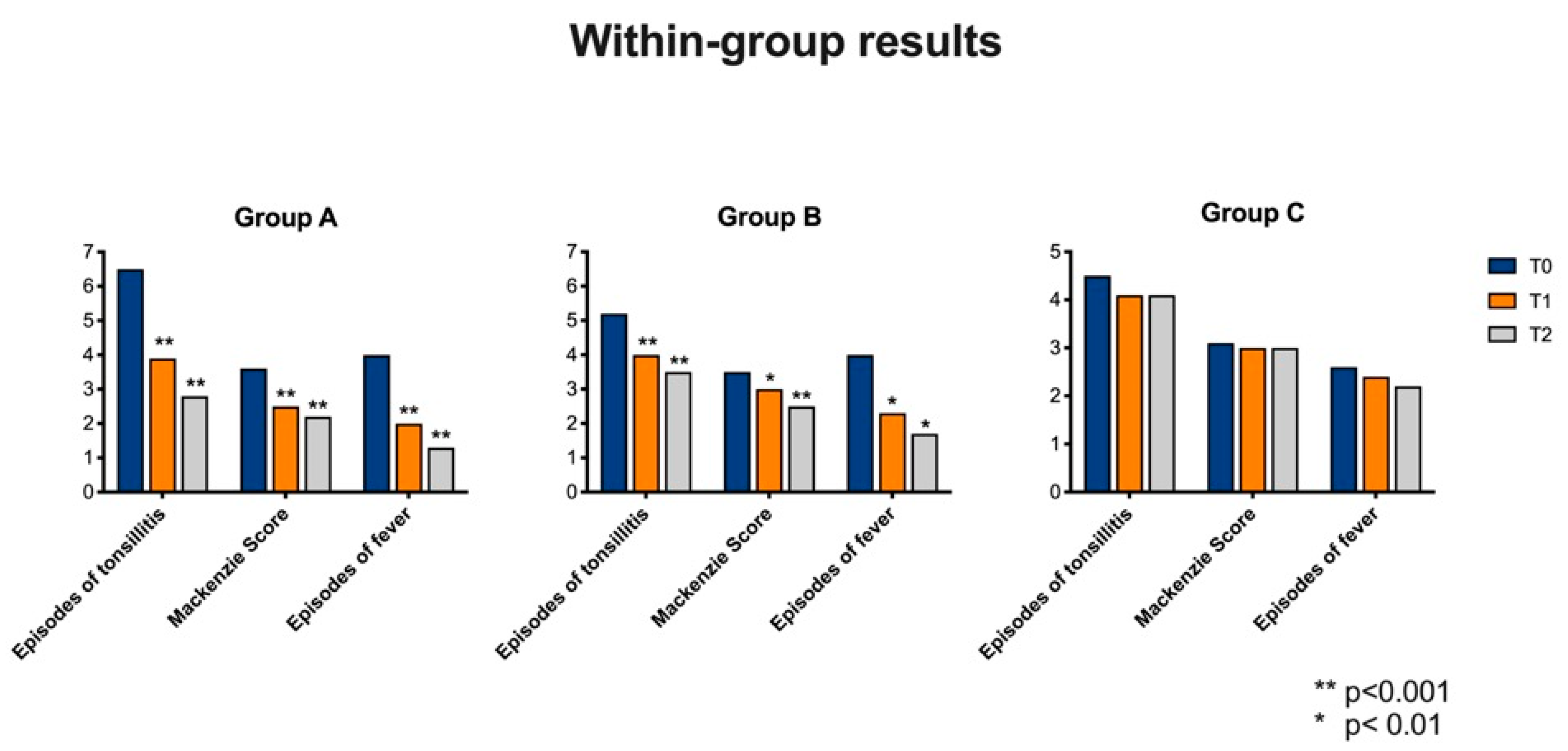
3.1. Treatment Results “within” Group Comparison
3.1.1. Group A
- (1)
- Number of tonsillitis episode (ANOVA: p < 0.0001) between T0 and T1 (BH: p < 0.0001), between T0 and T2 (BH: p < 0.0001) and T1 and T2 (BH: p < 0.0001).
- (2)
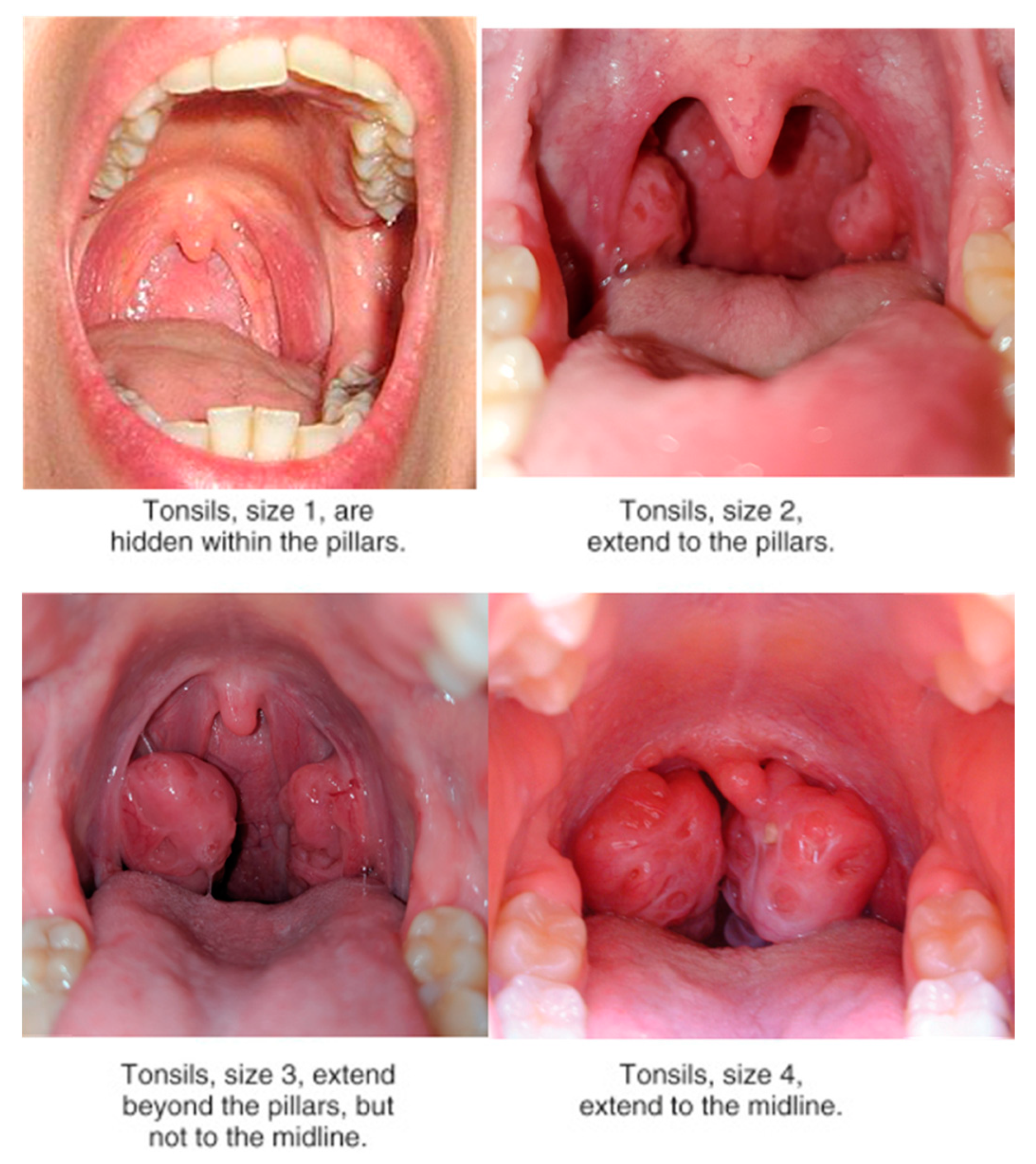
- Mackenzie score (ANOVA: p < 0.0001). In particular a significant variance was observed between T0 and T1 (HB: p < 0.0001), T0 and T2 (HB: p < 0.0001). No statistically significant variances were observed between T1 and T2 (HB: p = 0.3).
- (3)
- Number of fever episode (ANOVA: p < 0.0001). The variance was statistically significant by comparing T0 and T1 (HB: p < 0.0001), T0 and T2 (HB: p < 0.0001) and T1 and T2 (HB: p < 0.0001).
3.1.2. Group B
- (1)
- Number of tonsillitis episode (ANOVA: p < 0.0001) between T0 and T1 (BH: p < 0.0001), between T0 and T2 (BH: p < 0.0001). No statistically significant variances were observed between T1 and T2 (HB: p = 0.07).
- (2)
- Mackenzie score (ANOVA: p < 0.0001). In particular, a significant variance was observed between T0 and T2 (HB: p < 0.0001) and between T1 and T2 (HB: p = 0.01). No statistically significant variances were observed between T0 and T1 (HB: p = 0.06).
- (3)
- Number of fever episode (ANOVA: p = 0.002). The variance was statistically significant by comparing T0 and T1 (HB: p < 0.01), T0 and T2 (HB: p < 0.01) and T1 and T2 (HB: p < 0.01).
3.1.3. Control Group
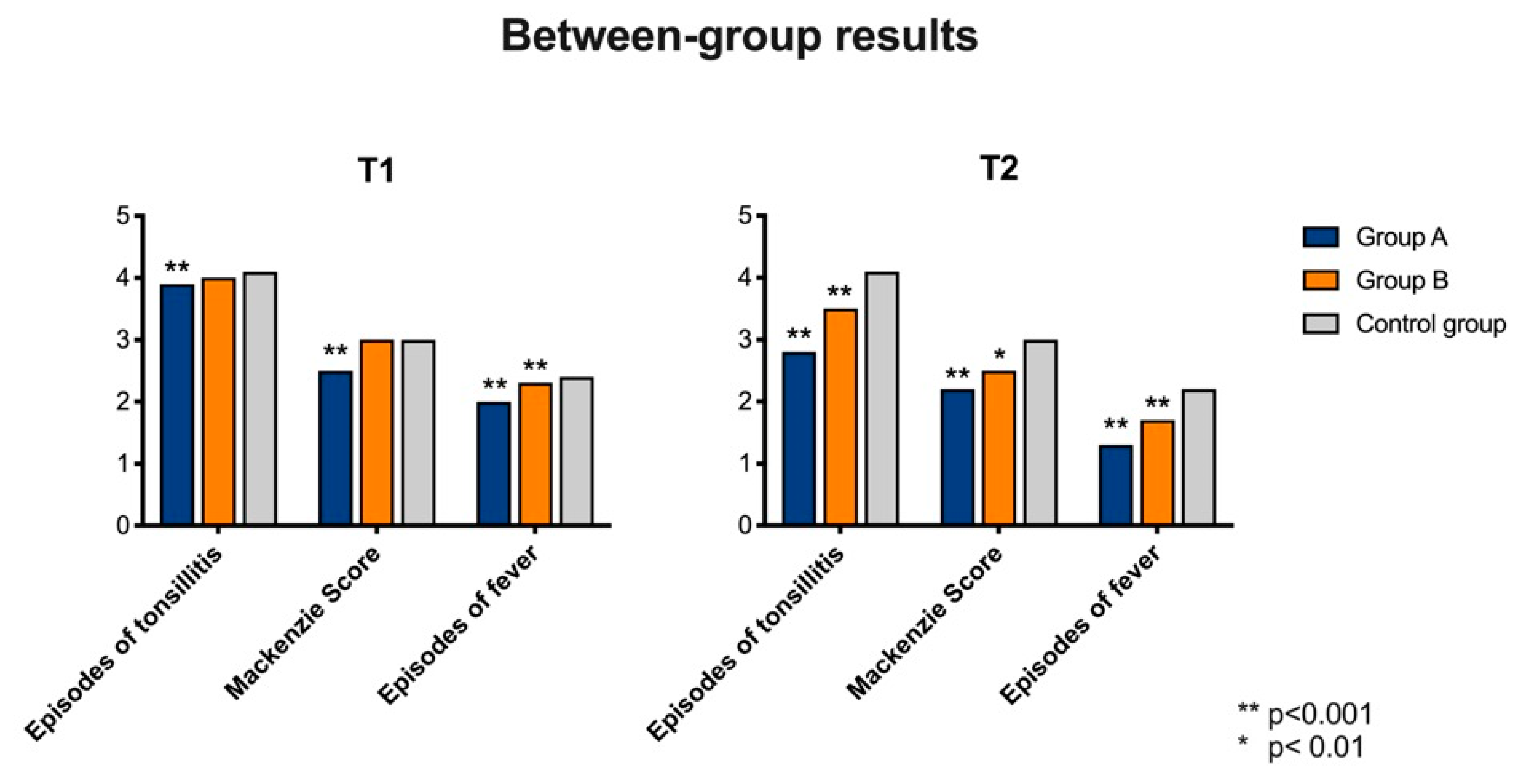
3.2. Treatment Results “between” Group Comparison
3.2.1. Comparison at T1
- (1)
- Number of tonsillitis episode (ANOVA: p < 0.0001). We observed statistically significant variances between GA (average: 3.9; SD: 1; CI 95%: 2–5) and CG (average: 4.1; SD: 0.9; CI 95%: 2–5) (BH: p < 0.0001), but not between GB (average: 4; SD: 1.1; CI 95%: 2–7) and CG (BH: p > 0.05). Statistically significant variances were observed between GA and GB (HB: p < 0.0001).
- (2)
- Mackenzie score (ANOVA: p < 0.0001). GA (average: 2.5; SD: 1; CI 95%: 1–4) showed statistically significant variances with CG (average: 3; SD: 0.6; CI 95%: 2–4) (HB: p = 0.0007), while no statistically significant variances were observed between GB (average: 3; SD: 0.6; CI 95%: 2–4) and CG (HB: p > 0.05). Statistically significant variance was observed by comparing GA and GB (HB: p < 0.00001).
- (3)
- Number of fever episode (ANOVA: p = 0.002). The variance was statistically significant by comparing GA (average: 2; SD: 0.7; CI 95%: 1–3) with CG (average: 2.4; SD: 0.7; CI 95%: 1–4) (HB: p = 0.001) and GB (average: 2.3; SD: 0.7; CI 95%: 1–4) with CG (HB: p = 0.002). No statistically significant differences were observed between GA and GB.
3.2.2. Comparison at T2
- (1)
- Number of tonsillitis episode (ANOVA: p < 0.0001). By comparing GA (average: 2.8; SD: 0.8; CI 95%: 1–4) and CG (average: 4.1; SD: 1; CI 95%: 2–6) we observed statistically significant variances at T2 (HB: p < 0.0001) and the same results were observed when comparing GB (average: 3.3; SD: 0.9; CI 95%: 2–5) with CG (HB: p = 0.0002). No statistically significant variances were observed between GA and GB.
- (2)
- Mackenzie score (ANOVA: p < 0.0001). GA (average: 2.3; SD: 0.7; CI 95%: 1–3) showed statistically significant variances with CG (average: 3; SD: 0.6; CI 95%: 2–4) at T2 (HB: p = 0.0001), as well as GB (average: 2.5; SD: 0.5; CI 95%: 2–3) versus CG (HB: p = 0.01). A statistically significant variance was observed by comparing GA and GB (HB: p = 0.003).
- (3)
- Number of fever episode (ANOVA: p = 0.002). The variance was statistically significant by comparing GA (average: 1.3; SD: 0.6; CI 95%: 0–2) and CG (average: 2.2; SD: 0.9; CI 95%: 1–3) at T2 (HB: p = 0.001) and GB (average: 1.7; SD: 0.7; CI 95%: 1–3) and CG at T2 (HB: p = 0.002). No statistically significant differences were observed between GA and GB.
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ceccarelli, G.; Statzu, M.; Santinelli, L.; Pinacchio, C.; Bitossi, C.; Cavallari, E.N.; Vullo, V.; Scagnolari, C.; d’Ettorre, G. Challenges in the management of HIV infection: Update on the role of probiotic supplementation as a possible complementary therapeutic strategy for cART treated people living with HIV/AIDS. Expert Opin. Biol. Ther. 2019, 19, 949–965. [Google Scholar] [CrossRef] [PubMed]
- Ledda, A.; Belcaro, G.; Dugall, M.; Luzzi, R.; Hosoi, M.; Feragalli, B.; Cotellese, R.; Cosentino, V.; Cosentino, M.; Eggenhoffner, R.; et al. A natural pharma standard supplement formulation to control treatment-related toxicity and oxidative stress in genitourinary cancer: A preliminary study. Eur. Rev. Med. Pharm. Sci. 2017, 21, 4196–4202. [Google Scholar]
- Harvie, M. Nutritional supplements and cancer: Potential benefits and proven harms. Am. Soc. Clin. Oncol. Educ. Book 2014, 34, e478–e486. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, L.; Clarke, L.; Khalilidehkordi, E.; Butzkueven, H.; Taylor, B.; Broadley, S.A. Vitamin D for the treatment of multiple sclerosis: A meta-analysis. J. Neurol. 2018, 265, 2893–2905. [Google Scholar] [CrossRef]
- Konijeti, G.G.; Arora, P.; Boylan, M.R.; Song, Y.; Huang, S.; Harrell, F.; Newton-Cheh, C.; O’Neill, D.; Korzenik, J.; Wang, T.J.; et al. Vitamin D Supplementation Modulates T Cell-Mediated Immunity in Humans: Results from a Randomized Control Trial. J. Clin. Endocrinol. Metab. 2016, 101, 533–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, C.Y.; Lin, H.C.; Hsueh, K.C.; Wu, S.F.; Fang, S.H. Oral administration of Lactobacillus salivarius inhibits the allergic airway response in mice. Can. J. Microbiol. 2010, 56, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Popovych, V.; Koshel, I.; Malofiichuk, A.; Pyletska, L.; Semeniuk, A.; Filippova, O.; Orlovska, R. A randomized, open-label, multicenter, comparative study of therapeutic efficacy, safety and tolerability of BNO 1030 extract, containing marshmallow root, chamomile flowers, horsetail herb, walnut leaves, yarrow herb, oak bark, dandelion herb in the treatment of acute non-bacterial tonsillitis in children aged 6 to 18 years. Am. J. Otolaryngol. 2019, 40, 265–273. [Google Scholar] [PubMed]
- Della Volpe, A.; Ricci, G.; Ralli, M.; Gambacorta, V.; De Lucia, A.; Minni, A.; Pirozzi, C.; Paccone, M.; Pastore, V.; Di Stadio, A. The effects of oral supplements with Sambucus nigra, Zinc, Tyndallized Lactobacillus acidophilus (HA122), Arabinogalactans, vitamin D, vitamin E and vitamin C in otitis media with effusion in children: A randomized controlled trial. Eur. Rev. Med. Pharm. Sci. 2019, 23, 6360–6370. [Google Scholar]
- Stelter, K. Tonsillitis and sore throat in children. GMS Curr. Top. Otorhinolaryngol. Head Neck Surg. 2014, 13. [Google Scholar] [CrossRef]
- Siani, A.; Strazzullo, P.; Russo, L.; Guglielmi, S.; Iacoviello, L.; Ferrara, L.A.; Mancini, M. Controlled trial of long-term oral potassium supplements in patients with mild hypertension. Br. Med. J. (Clin. Res. Ed.) 1987, 294, 1453–1456. [Google Scholar] [CrossRef] [Green Version]
- Minutolo, M.; Chiaiese, P.; Di Matteo, A.; Errico, A.; Corrado, G. Accumulation of Ascorbic Acid in Tomato Cell Culture: Influence of the Genotype, Source Explant and Time of In Vitro Cultivation. Antioxidants 2020, 7, 222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elenius, V.; Palomares, O.; Waris, M.; Turunen, R.; Puhakka, T.; Rückert, B.; Vuorinen, T.; Allander, T.; Vahlberg, T.; Akdis, M.; et al. The relationship of serum vitamins A, D, E and LL-37 levels with allergic status, tonsillar virus detection and immune response. PLoS ONE 2017, 12, e0172350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaik-Dasthagirisaheb, Y.B.; Varvara, G.; Murmura, G.; Saggini, A.; Caraffa, A.; Antinolfi, P.; Tete, S.; Tripodi, D.; Conti, F.; Cianchetti, E.; et al. Role of vitamins D, E and C in immunity and inflammation. J. Biol. Regul. Homeost Agents 2013, 27, 291–295. [Google Scholar] [PubMed]
- Bergman, P.; Lindh, A.U.; Bjorkhem-Bergman, L.; Lindh, J.D. Vitamin D and Respiratory Tract Infections: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2013, 8, e65835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Zhuo, Q.; Yuan, W.; Wang, J.; Wu, T. Vitamin A for preventing acute lower respiratory tract infections in children up to seven years of age. Cochrane Database Syst Rev. 2008. [Google Scholar] [CrossRef]
- Vandenplas, Y.; Veereman-Wauters, G.; De Greef, E.; Peeters, S.; Casteels, A.; Mahler, T.; Devreker, T.; Hauser, B. Probiotics and prebiotics in prevention and treatment of diseases in infants and children. J. Pediatr. 2011, 87, 292–300. [Google Scholar] [CrossRef] [Green Version]
- Muhamed, P.K.; Vadstrup, S. [Zinc is the most important trace element]. Ugeskr. Laeger 2014, 17, V11120654. [Google Scholar]
- Sirisinha, S. The pleiotropic role of vitamin A in regulating mucosal immunity. Asian Pac. J. Allergy Immunol. 2015, 33, 71–89. [Google Scholar]
- Amazan, D.; Cordero, G.; Lopez-Bote, C.J.; Lauridsen, C.; Rey, A.I. Effects of oral micellized natural vitamin E (D-alpha-tocopherol) v. synthetic vitamin E (DL-alpha-tocopherol) in feed on alpha-tocopherol levels, stereoisomer distribution, oxidative stress and the immune response in piglets. Animal 2014, 8, 410–419. [Google Scholar] [CrossRef] [Green Version]
- Braicu, C.; Mehterov, N.; Vladimirov, B.; Sarafian, V.; Nabavi, S.M.; Atanasov, A.G.; Berindan-Neagoe, I. Nutrigenomics in cancer: Revisiting the effects of natural compounds. Semin. Cancer Biol. 2017, 46, 84–106. [Google Scholar] [CrossRef]
- Prado Acosta, M.; Geoghegan, E.M.; Lepenies, B.; Ruzal, S.; Kielian, M.; Martinez, M.G. Surface (S) Layer Proteins of Lactobacillus acidophilus Block Virus Infection via DC-SIGN Interaction. Front. Microbiol. 2019, 10, 810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inturri, R.; Stivala, A.; Furneri, P.M.; Blandino, G. Growth and adhesion to HT-29 cells inhibition of Gram-negatives by Bifidobacterium longum BB536 e Lactobacillus rhamnosus HN001 alone and in combination. Eur. Rev. Med. Pharm. Sci. 2016, 20, 4943–4949. [Google Scholar]
- Principi, N.; Esposito, S. Severe influenza in children: Incidence and risk factors. Expert Rev. Anti. Infect. Ther. 2016, 14, 961–968. [Google Scholar] [CrossRef] [PubMed]
- Frei, R.; Akdis, M.; O’Mahony, L. Prebiotics, probiotics, synbiotics, and the immune system: Experimental data and clinical evidence. Curr. Opin. Gastroenterol. 2015, 31, 153–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Angelo, C.; Reale, M.; Costantini, E. Microbiota and Probiotics in Health and HIV Infection. Nutrients 2017, 9, 615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loftis, L. Acute infectious upper airway obstructions in children. Semin. Pediatr. Infect. Dis. 2006, 17, 5–10. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group A | T0 | T1 | T2 |
|---|---|---|---|
| Episodes of tonsillitis | 6.5 (SD: 1; CI 95%:4–8) | 3.9 (SD: 1; CI 95%:2–5) | 2.8 (SD: 0.9; CI 95%:1–4) |
| Mackenzie Score | 3.6 (SD: 0.5; CI 95%:3–4) | 2.5 (SD: 1; CI 95%:1–4) | 2.2 (SD: 0.7; CI 95%: 1–3) |
| Episodes of fever | 4 (SD: 1 CI 95%: 4–8) | 2 (SD: 0.7; CI 95%: 1–3) | 1 (SD: 0.6; CI 95%: 0–2) |
| Group B | T0 | T1 | T2 |
|---|---|---|---|
| Episodes of tonsillitis | 5,2 (SD: 1.2 CI 95%: 4–8) | 4 (SD: 1.1; CI 95%: 2–7) | 3.3 (SD: 0.9; CI 95%: 2–5) |
| Mackenzie Score | 3.5 (SD: 0,6 CI 95%:2–4) | 3 (SD: 0.6; CI 95%:2–4) | 2.5 (SD: 0.5; CI 95%:2–4) |
| Episodes of fever | 4 (SD 0.1 CI 95%: 4–8) | 2,3 (SD: 0.7; CI 95%:1–3) | 1.7 (SD: 0.8; CI 95%:1–3) |
| Control Group | T0 | T1 | T2 |
|---|---|---|---|
| Episodes of tonsillitis | 4.5 (SD: 0.9 CI 95%: 3–6) | 4.1 (SD: 0.9 CI 95%:2–5) | 4.1 (SD: 1; CI 95%:2–6) |
| Mackenzie Score | 3 (SD: 0.5 CI 95%:2–4) | 3 (SD: 0.6 CI 95%:2–4) | 3 (SD: 0.6 CI 95%:2–4) |
| Episodes of fever | 2.6 (SD: 0.8 CI 95%: 4–8) | 2.4 (SD: 0.6 CI 95%:2–4) | 2.2 (SD: 0.8 CI 95%:1–4) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Stadio, A.; della Volpe, A.; Korsch, F.M.; De Lucia, A.; Ralli, M.; Martines, F.; Ricci, G. Difensil Immuno Reduces Recurrence and Severity of Tonsillitis in Children: A Randomized Controlled Trial. Nutrients 2020, 12, 1637. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061637
Di Stadio A, della Volpe A, Korsch FM, De Lucia A, Ralli M, Martines F, Ricci G. Difensil Immuno Reduces Recurrence and Severity of Tonsillitis in Children: A Randomized Controlled Trial. Nutrients. 2020; 12(6):1637. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061637
Chicago/Turabian StyleDi Stadio, Arianna, Antonio della Volpe, Fiammetta M. Korsch, Antonietta De Lucia, Massimo Ralli, Francesco Martines, and Giampietro Ricci. 2020. "Difensil Immuno Reduces Recurrence and Severity of Tonsillitis in Children: A Randomized Controlled Trial" Nutrients 12, no. 6: 1637. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061637