Comparative Effect of Statins and Omega-3 Supplementation on Cardiovascular Events: Meta-Analysis and Network Meta-Analysis of 63 Randomized Controlled Trials Including 264,516 Participants


Abstract
:1. Introduction
2. Methods
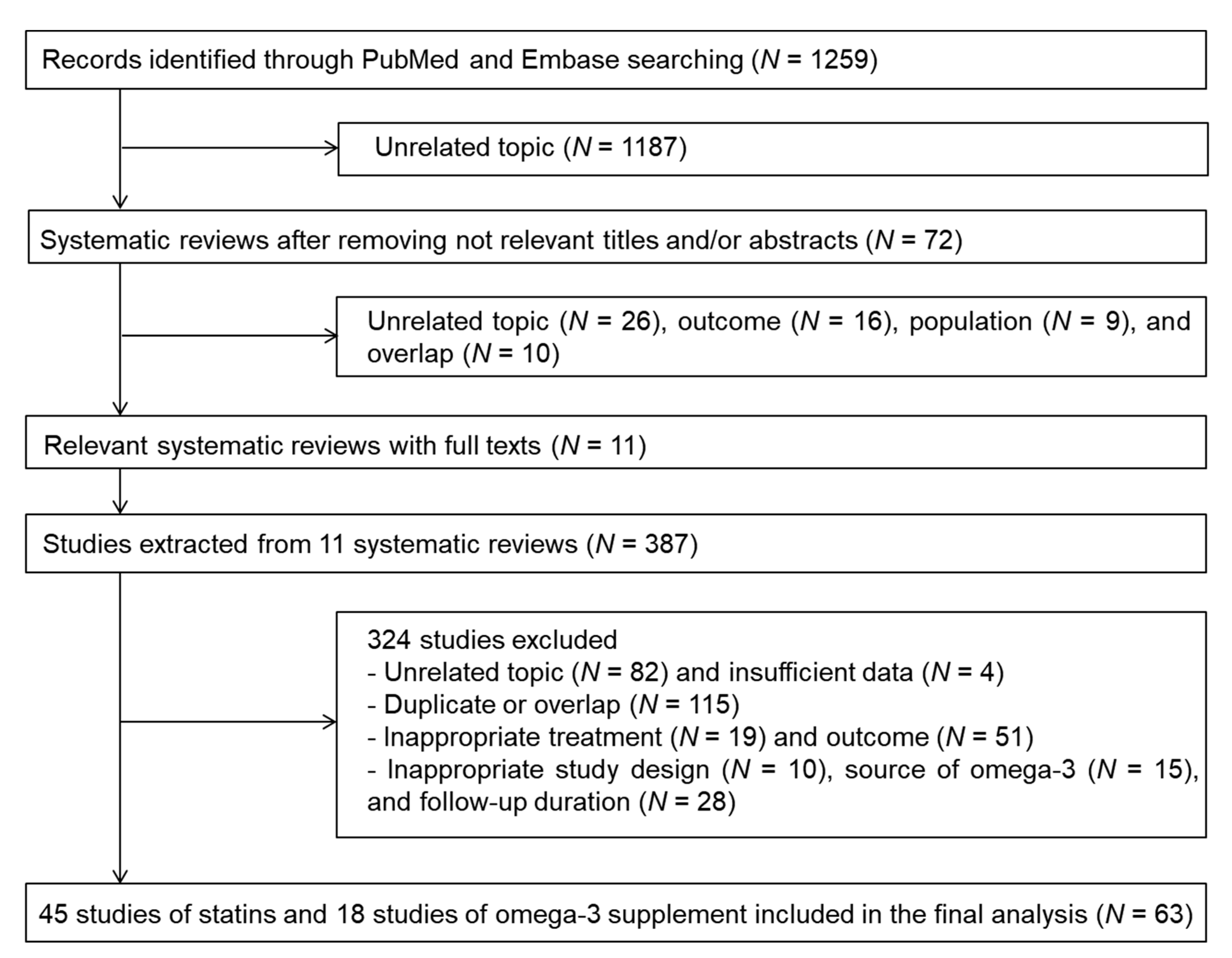
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Statistical Analysis
3. Results
3.1. Study Characteristics
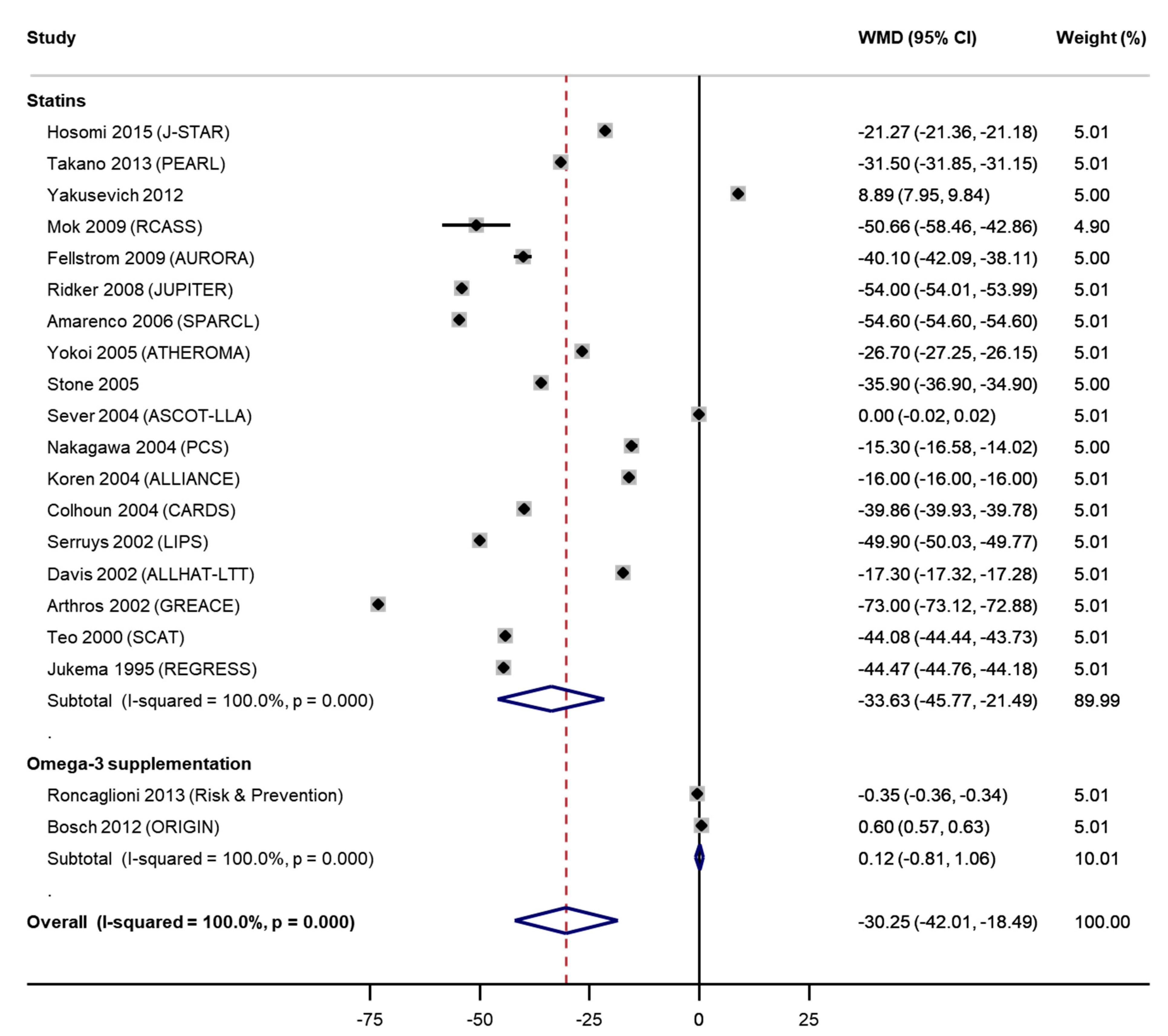
3.2. Meta-Analysis of Direct Estimates
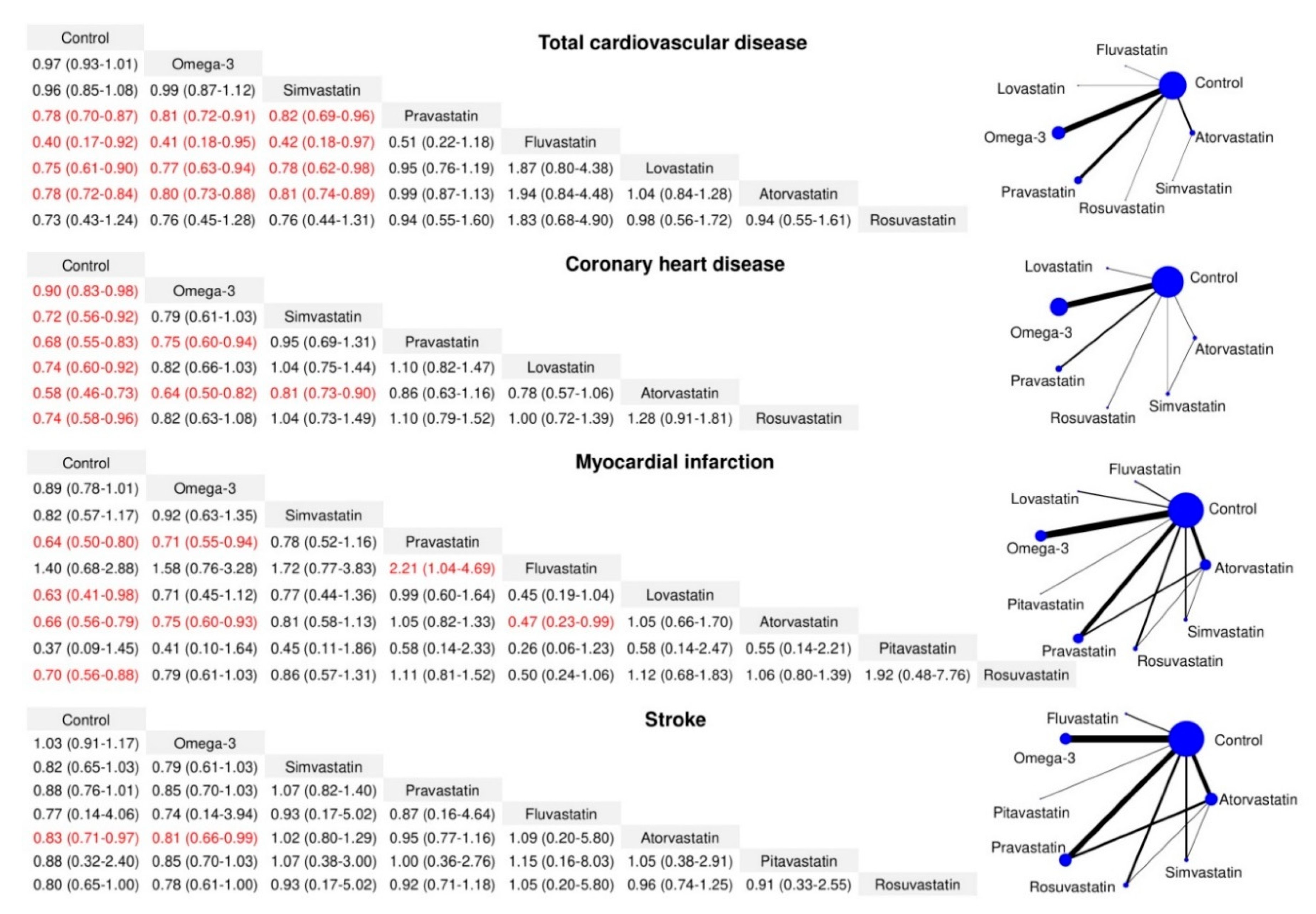
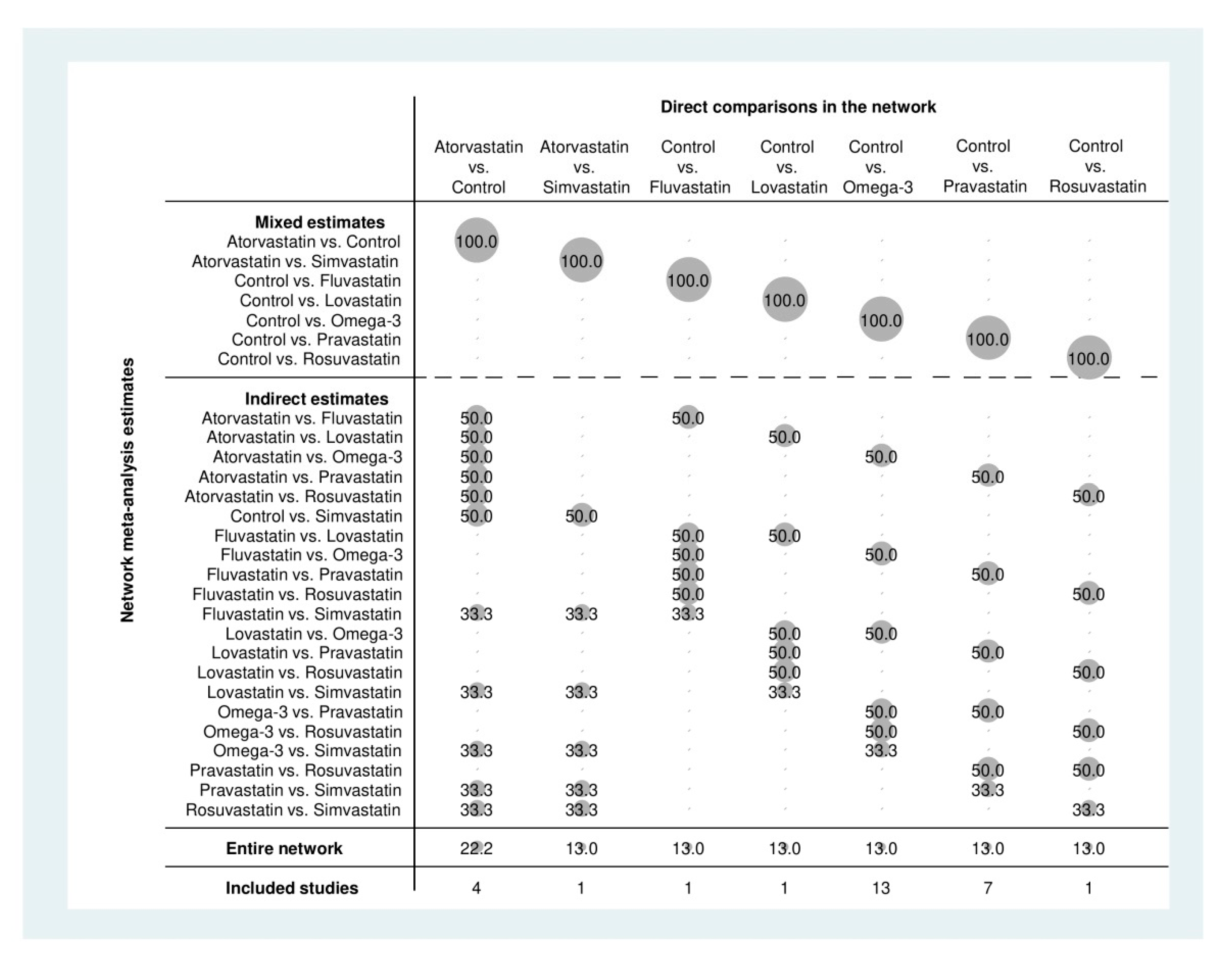
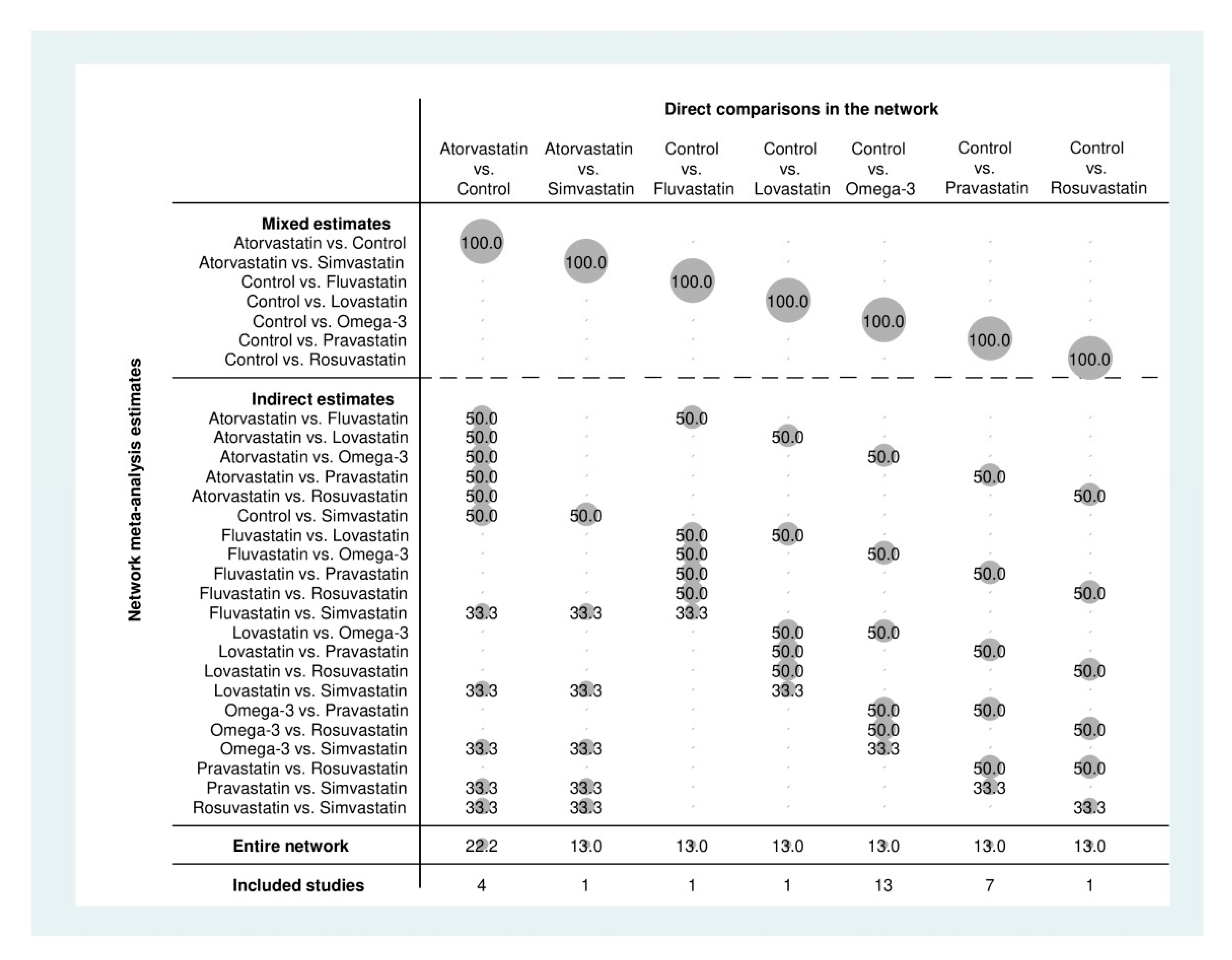
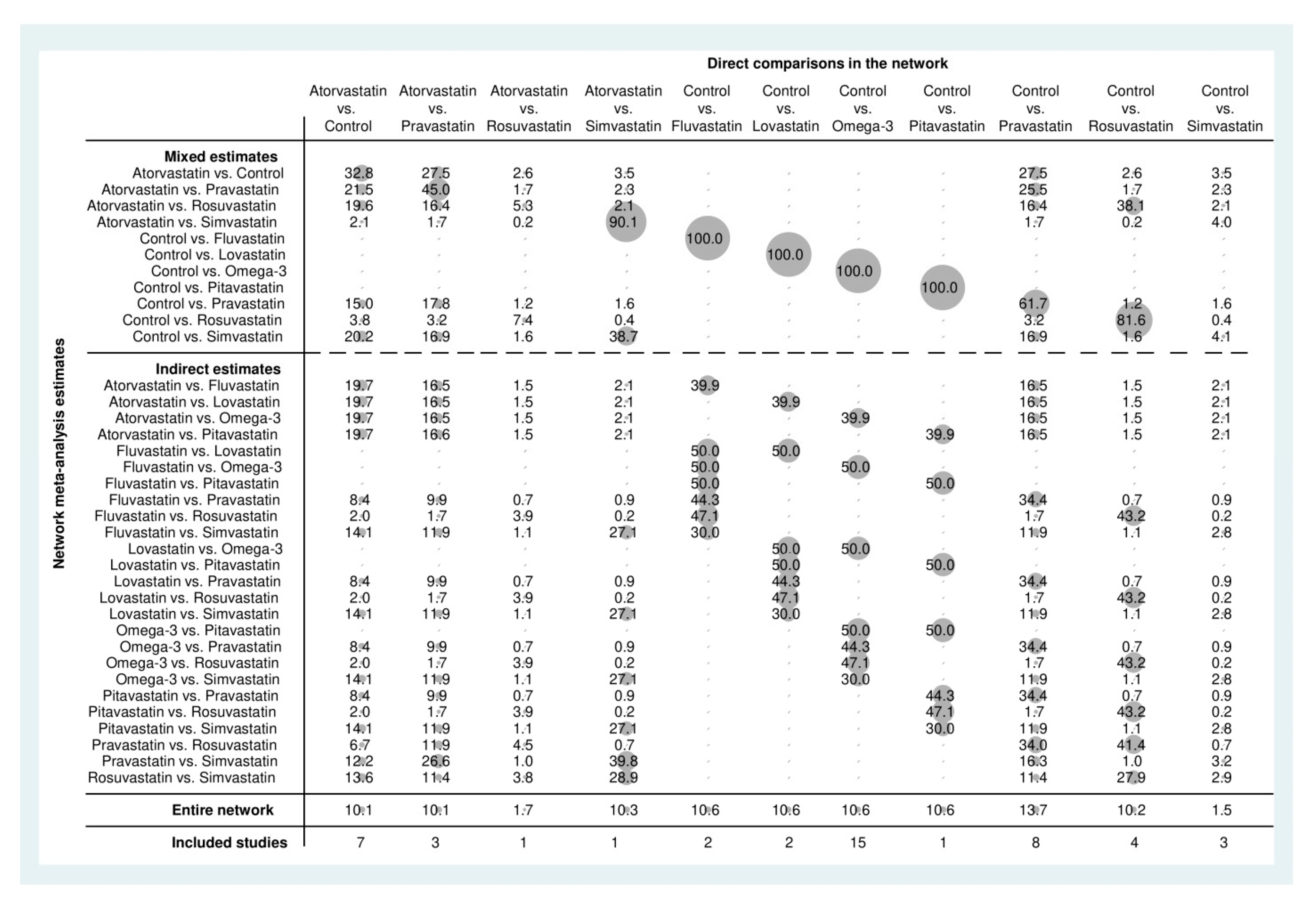
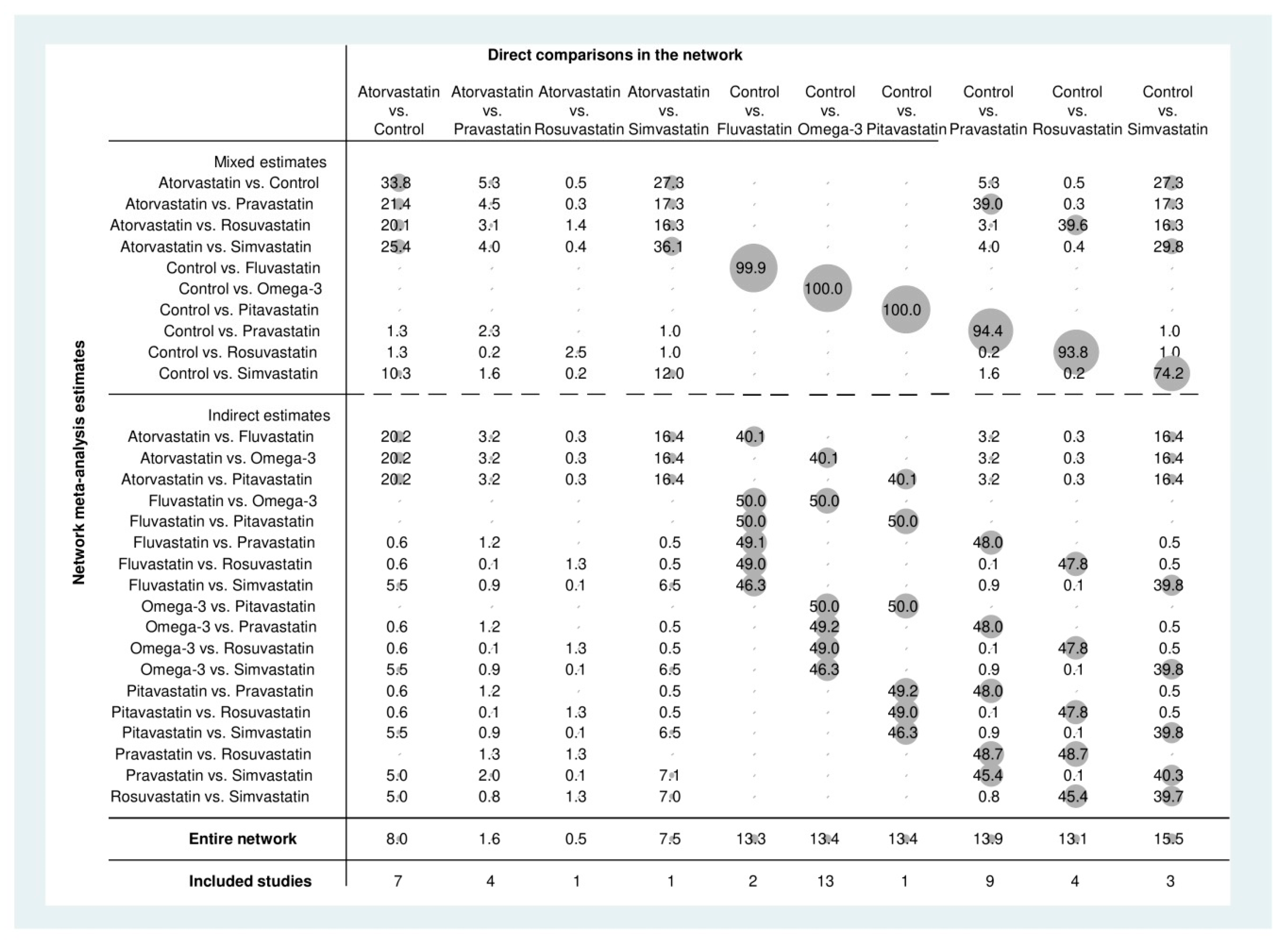
3.3. Network Meta-Analysis of Direct and Indirect Estimates
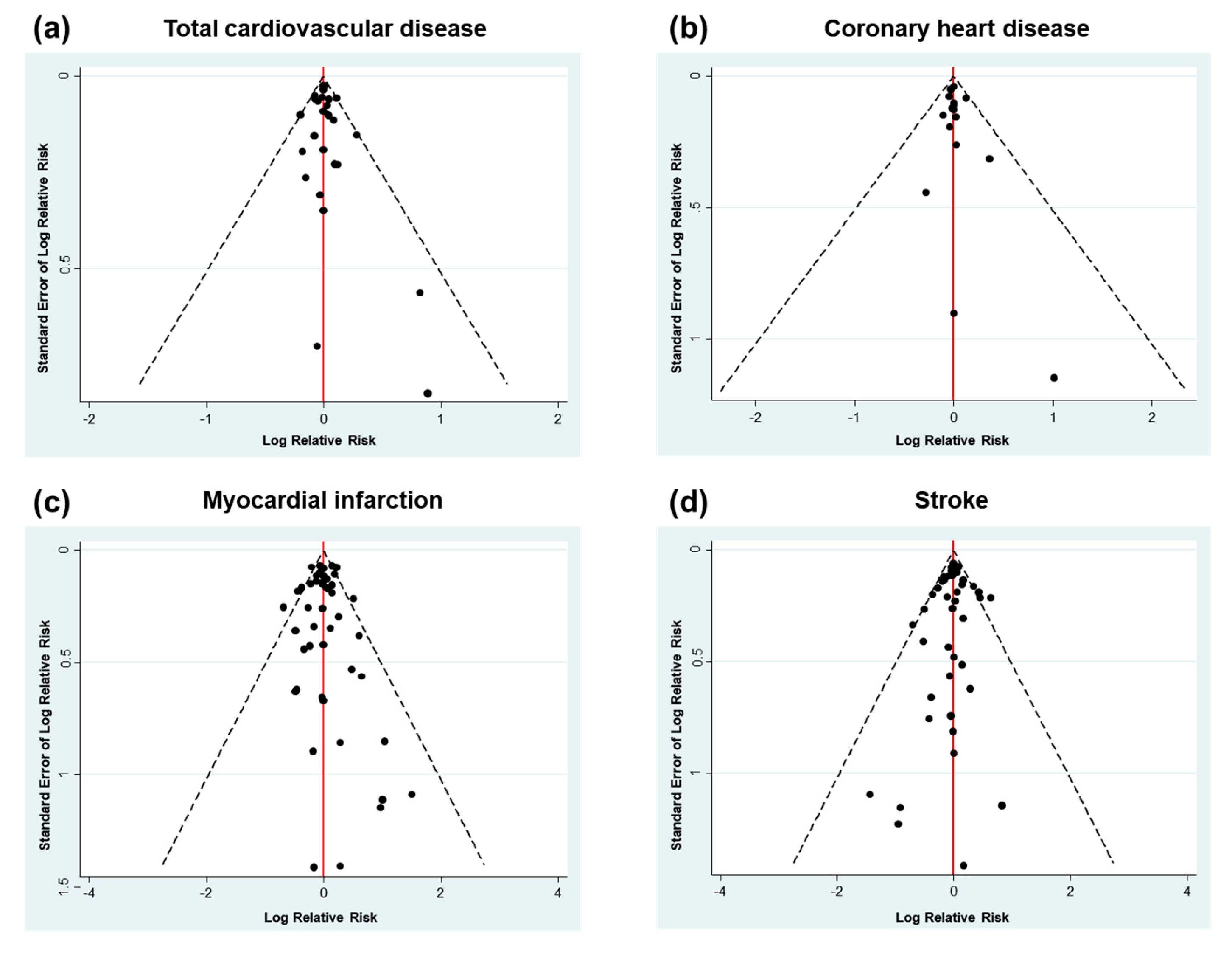
3.4. Publication Bias and Contribution Plot
3.5. Treatment Ranking
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A







References
- Farley, A.; McLafferty, E.; Hendry, C. The cardiovascular system. Nurs. Stand. 2012, 27, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.; Manmathan, G.; Wilkinson, P. Primary prevention of cardiovascular disease: A review of contemporary guidance and literature. JRSM Cardiovasc. Dis. 2017, 6, 2048004016687211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruan, Y.; Guo, Y.; Zheng, Y.; Huang, Z.; Sun, S.; Kowal, P.; Shi, Y.; Wu, F. Cardiovascular disease (CVD) and associated risk factors among older adults in six low-and middle-income countries: Results from SAGE Wave 1. BMC Public Health 2018, 18, 778. [Google Scholar] [CrossRef] [Green Version]
- Rosiek, A.; Leksowski, K. The risk factors and prevention of cardiovascular disease: The importance of electrocardiogram in the diagnosis and treatment of acute coronary syndrome. Ther. Clin. Risk Manag. 2016, 12, 1223–1229. [Google Scholar] [CrossRef] [Green Version]
- KSoLA. Dyslipidemia Fact Sheets in Korea. 2018. Available online: https://www.lipid.or.kr/file/Dyslipidemia%20Fact%20Sheets%20in%20Korea%202018.pdf (accessed on 21 December 2019).
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: A report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the management of blood cholesterol: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J. Am. Coll. Cardiol. 2019, 73, 3168–3209. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corra, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The sixth joint task force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Chou, R.; Dana, T.; Blazina, I.; Daeges, M.; Jeanne, T.L. Statins for prevention of cardiovascular disease in adults: Evidence report and systematic review for the US preventive services task force. J. Am. Med. Acad. 2016, 316, 2008–2024. [Google Scholar] [CrossRef]
- Hu, Y.; Hu, F.B.; Manson, J.E. Marine omega-3 supplementation and cardiovascular disease: An updated meta-analysis of 13 randomized controlled trials involving 127 477 participants. J. Am. Heart Assoc. 2019, 8, e013543. [Google Scholar] [CrossRef]
- Brouwer, I.A.; Zock, P.L.; Camm, A.J.; Bocker, D.; Hauer, R.N.; Wever, E.F.; Dullemeijer, C.; Ronden, J.E.; Katan, M.B.; Lubinski, A.; et al. Effect of fish oil on ventricular tachyarrhythmia and death in patients with implantable cardioverter defibrillators: The Study on Omega-3 Fatty Acids and Ventricular Arrhythmia (SOFA) randomized trial. J. Am. Med. Acad. 2006, 295, 2613–2619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dangour, A.D.; Allen, E.; Elbourne, D.; Fasey, N.; Fletcher, A.E.; Hardy, P.; Holder, G.E.; Knight, R.; Letley, L.; Richards, M.; et al. Effect of 2-y n-3 long-chain polyunsaturated fatty acid supplementation on cognitive function in older people: A randomized, double-blind, controlled trial. Am. J. Clin. Nutr. 2010, 91, 1725–1732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macchia, A.; Grancelli, H.; Varini, S.; Nul, D.; Laffaye, N.; Mariani, J.; Ferrante, D.; Badra, R.; Figal, J.; Ramos, S.; et al. Omega-3 fatty acids for the prevention of recurrent symptomatic atrial fibrillation: Results of the FORWARD (Randomized Trial to Assess Efficacy of PUFA for the Maintenance of Sinus Rhythm in Persistent Atrial Fibrillation) trial. J. Am. Coll. Cardiol. 2013, 61, 463–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsen, D.W.; Albrektsen, G.; Landmark, K.; Moen, S.; Aarsland, T.; Woie, L. Effects of a high-dose concentrate of n-3 fatty acids or corn oil introduced early after an acute myocardial infarction on serum triacylglycerol and HDL cholesterol. Am. J. Clin. Nutr. 2001, 74, 50–56. [Google Scholar] [CrossRef]
- Raitt, M.H.; Connor, W.E.; Morris, C.; Kron, J.; Halperin, B.; Chugh, S.S.; McClelland, J.; Cook, J.; MacMurdy, K.; Swenson, R.; et al. Fish oil supplementation and risk of ventricular tachycardia and ventricular fibrillation in patients with implantable defibrillators: A randomized controlled trial. J. Am. Med. Acad. 2005, 293, 2884–2891. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Wood, S. Package “mgcv”: Mixed GAM Computation Vehicle with Automatic Smoothness Estimation, Version 1.8-31. Available online: https://cran.r-project.org/web/packages/mgcv/mgcv.pdf (accessed on 21 July 2020).
- Shim, S.; Yoon, B.H.; Shin, I.S.; Bae, J.M. Network meta-analysis: Application and practice using Stata. Epidemiol. Health 2017, 39, e2017047. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Chaimani, A.; Higgins, J.P.; Mavridis, D.; Spyridonos, P.; Salanti, G. Graphical tools for network meta-analysis in STATA. PLoS ONE 2013, 8, e76654. [Google Scholar] [CrossRef]
- Naci, H.; Brugts, J.J.; Fleurence, R.; Tsoi, B.; Toor, H.; Ades, A.E. Comparative benefits of statins in the primary and secondary prevention of major coronary events and all-cause mortality: A network meta-analysis of placebo-controlled and active-comparator trials. Eur. J. Prev. Cardiol. 2013, 20, 641–657. [Google Scholar] [CrossRef]
- Taylor, F.; Huffman, M.D.; Macedo, A.F.; Moore, T.H.M.; Burke, M.; Davey Smith, G.; Ward, K.; Ebrahim, S. Statins for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2013, 2013, CD004816. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Zhang, B. Statins for the prevention of stroke: A meta-analysis of randomized controlled trials. PLoS ONE 2014, 9, e92388. [Google Scholar] [CrossRef] [PubMed]
- Balk, E.M.; Adams, G.P.; Langberg, V.; Halladay, C.; Chung, M.; Lin, L.; Robertson, S.; Yip, A.; Steele, D.; Smith, B.T.; et al. Omega-3 fatty acids and cardiovascular disease: An updated systematic review. Evid. Rep. Technol. Assess. Full Rep. 2016, 223, 1–1252. [Google Scholar] [CrossRef]
- Zhong, P.; Wu, D.; Ye, X.; Wu, Y.; Li, T.; Tong, S.; Liu, X. Secondary prevention of major cerebrovascular events with seven different statins: A multi-treatment meta-analysis. Drug Des. Dev. Ther. 2017, 11, 2517–2526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdelhamid, A.S.; Brown, T.J.; Brainard, J.S.; Biswas, P.; Thorpe, G.C.; Moore, H.J.; Deane, K.H.; AlAbdulghafoor, F.K.; Summerbell, C.D.; Worthington, H.V.; et al. Omega-3 fatty acids for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2018, 7, CD003177. [Google Scholar] [CrossRef] [PubMed]
- Aung, T.; Halsey, J.; Kromhout, D.; Gerstein, H.C.; Marchioli, R.; Tavazzi, L.; Geleijnse, J.M.; Rauch, B.; Ness, A.; Galan, P.; et al. Associations of omega-3 fatty acid supplement use with cardiovascular disease risks: Meta-analysis of 10 trials involving 77917 individuals. J. Am. Med. Acad. Cardiol. 2018, 3, 225–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bielecka-Dabrowa, A.; Bytyci, I.; Von Haehling, S.; Anker, S.; Jozwiak, J.; Rysz, J.; Hernandez, A.V.; Bajraktari, G.; Mikhalidis, D.P.; Banach, M. Association of statin use and clinical outcomes in heart failure patients: A systematic review and meta-analysis. Lipids Health Dis. 2019, 18, 188. [Google Scholar] [CrossRef] [Green Version]
- Tramacere, I.; Boncoraglio, G.B.; Banzi, R.; Del Giovane, C.; Kwag, K.H.; Squizzato, A.; Moja, L. Comparison of statins for secondary prevention in patients with ischemic stroke or transient ischemic attack: A systematic review and network meta-analysis. BMC Med. 2019, 17, 67. [Google Scholar] [CrossRef] [Green Version]
- Yebyo, H.G.; Aschmann, H.E.; Kaufmann, M.; Puhan, M.A. Comparative effectiveness and safety of statins as a class and of specific statins for primary prevention of cardiovascular disease: A systematic review, meta-analysis, and network meta-analysis of randomized trials with 94,283 participants. Am. Heart J. 2019, 210, 18–28. [Google Scholar] [CrossRef]
- Hosomi, N.; Nagai, Y.; Kohriyama, T.; Ohtsuki, T.; Aoki, S.; Nezu, T.; Maruyama, H.; Sunami, N.; Yokota, C.; Kitagawa, K.; et al. The Japan Statin Treatment Against Recurrent Stroke (J-STARS): A multicenter, randomized, open-label, parallel-group study. EBio Med. 2015, 2, 1071–1078. [Google Scholar] [CrossRef] [Green Version]
- Ford, I.; Murray, H.; McCowan, C.; Packard, C.J. Long-term safety and efficacy of lowering low-density lipoprotein cholesterol with statin therapy: 20-year follow-up of West of Scotland Coronary Prevention Study. Circulation 2016, 133, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.L.; Teo, K.; Dumesnil, J.G.; Ni, A.; Tam, J.; Investigators, A. Effect of lipid lowering with rosuvastatin on progression of aortic stenosis: Results of the aortic stenosis progression observation: Measuring effects of rosuvastatin (ASTRONOMER) trial. Circulation 2010, 121, 306–314. [Google Scholar] [CrossRef] [Green Version]
- Yakusevich, V.V.; Malygin, A.Y.; Lychenko, S.V.; Petrochenko, A.S.; Kabanov, A.V. The efficacy of high-dose simvastatin in acute period of ischemic stroke. Ration. Pharmacother. Card. 2012, 8, 4–16. [Google Scholar] [CrossRef] [Green Version]
- Yokoyama, M.; Origasa, H.; Matsuzaki, M.; Matsuzawa, Y.; Saito, Y.; Ishikawa, Y.; Oikawa, S.; Sasaki, J.; Hishida, H.; Itakura, H.; et al. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): A randomised open-label, blinded endpoint analysis. Lancet 2007, 369, 1090–1098. [Google Scholar] [CrossRef]
- Tavazzi, L.; Maggioni, A.P.; Marchioli, R.; Barlera, S.; Franzosi, M.G.; Latini, R.; Lucci, D.; Nicolosi, G.L.; Porcu, M.; Tognoni, G.; et al. Effect of rosuvastatin in patients with chronic heart failure (the GISSI-HF trial): A randomised, double-blind, placebo-controlled trial. Lancet 2008, 372, 1231–1239. [Google Scholar] [CrossRef] [PubMed]
- Long-Term Intervention with Pravastatin in Ischaemic Disease Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N. Engl. J. Med. 1998, 339, 1349–1357. [Google Scholar] [CrossRef] [Green Version]
- Teo, K.K.; Burton, J.R.; Buller, C.E.; Plante, S.; Catellier, D.; Tymchak, W.; Dzavik, V.; Taylor, D.; Yokoyama, S.; Montague, T.J. Long-term effects of cholesterol lowering and angiotensin-converting enzyme inhibition on coronary atherosclerosis: The Simvastatin/Enalapril Coronary Atherosclerosis Trial (SCAT). Circulation 2000, 102, 1748–1754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokoi, H.; Nobuyoshi, M.; Mitsudo, K.; Kawaguchi, A.; Yamamoto, A.; Investigators, A.S. Three-year follow-up results of angiographic intervention trial using an HMG-CoA reductase inhibitor to evaluate retardation of obstructive multiple atheroma (ATHEROMA) study. Circ. J. 2005, 69, 875–883. [Google Scholar] [CrossRef] [Green Version]
- Wanner, C.; Krane, V.; Marz, W.; Olschewski, M.; Mann, J.F.; Ruf, G.; Ritz, E.; German, D.; Dialysis Study, I. Atorvastatin in patients with type 2 diabetes mellitus undergoing hemodialysis. N. Engl. J. Med. 2005, 353, 238–248. [Google Scholar] [CrossRef]
- Stone, P.H.; Lloyd-Jones, D.M.; Kinlay, S.; Frei, B.; Carlson, W.; Rubenstein, J.; Andrews, T.C.; Johnstone, M.; Sopko, G.; Cole, H.; et al. Effect of intensive lipid lowering, with or without antioxidant vitamins, compared with moderate lipid lowering on myocardial ischemia in patients with stable coronary artery disease: The Vascular Basis for the Treatment of Myocardial Ischemia Study. Circulation 2005, 111, 1747–1755. [Google Scholar] [CrossRef] [Green Version]
- Takano, H.; Mizuma, H.; Kuwabara, Y.; Sato, Y.; Shindo, S.; Kotooka, N.; Fujimatsu, D.; Kobayashi, Y.; Inoue, T.; Node, K.; et al. Effects of pitavastatin in Japanese patients with chronic heart failure: The Pitavastatin Heart Failure Study (PEARL Study). Circ. J. 2013, 77, 917–925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gissi, P.I. Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: Results of the GISSI-Prevenzione trial. Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico. Lancet 1999, 354, 447–455. [Google Scholar]
- Tavazzi, L.; Maggioni, A.P.; Marchioli, R.; Barlera, S.; Franzosi, M.G.; Latini, R.; Lucci, D.; Nicolosi, G.L.; Porcu, M.; Tognoni, G.; et al. Effect of n-3 polyunsaturated fatty acids in patients with chronic heart failure (the GISSI-HF trial): A randomised, double-blind, placebo-controlled trial. Lancet 2008, 372, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Sever, P.S.; Dahlof, B.; Poulter, N.R.; Wedel, H.; Beevers, G.; Caulfield, M.; Collins, R.; Kjeldsen, S.E.; Kristinsson, A.; McInnes, G.T.; et al. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial—Lipid Lowering Arm (ASCOT-LLA): A multicentre randomised controlled trial. Drugs 2004, 64 (Suppl. S2), 43–60. [Google Scholar] [CrossRef]
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.; Genest, J.; Gotto, A.M., Jr.; Kastelein, J.J.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; MacFadyen, J.G.; et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N. Engl. J. Med. 2008, 359, 2195–2207. [Google Scholar] [CrossRef] [Green Version]
- Riegger, G.; Abletshauser, C.; Ludwig, M.; Schwandt, P.; Widimsky, J.; Weidinger, G.; Welzel, D. The effect of fluvastatin on cardiac events in patients with symptomatic coronary artery disease during one year of treatment. Atherosclerosis 1999, 144, 263–270. [Google Scholar] [CrossRef]
- Shepherd, J.; Blauw, G.J.; Murphy, M.B.; Bollen, E.L.; Buckley, B.M.; Cobbe, S.M.; Ford, I.; Gaw, A.; Hyland, M.; Jukema, J.W.; et al. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): A randomised controlled trial. Lancet 2002, 360, 1623–1630. [Google Scholar] [CrossRef]
- Serruys, P.W.; de Feyter, P.; Macaya, C.; Kokott, N.; Puel, J.; Vrolix, M.; Branzi, A.; Bertolami, M.C.; Jackson, G.; Strauss, B.; et al. Fluvastatin for prevention of cardiac events following successful first percutaneous coronary intervention: A randomized controlled trial. J. Am. Med. Acad. 2002, 287, 3215–3222. [Google Scholar] [CrossRef]
- Sawayama, Y.; Shimizu, C.; Maeda, N.; Tatsukawa, M.; Kinukawa, N.; Koyanagi, S.; Kashiwagi, S.; Hayashi, J. Effects of probucol and pravastatin on common carotid atherosclerosis in patients with asymptomatic hypercholesterolemia. Fukuoka Atherosclerosis Trial (FAST). J. Am. Coll. Cardiol. 2002, 39, 610–616. [Google Scholar] [CrossRef] [Green Version]
- Risk & Prevention Study Collaborative, G.; Roncaglioni, M.C.; Tombesi, M.; Avanzini, F.; Barlera, S.; Caimi, V.; Longoni, P.; Marzona, I.; Milani, V.; Silletta, M.G.; et al. n-3 fatty acids in patients with multiple cardiovascular risk factors. N. Engl. J. Med. 2013, 368, 1800–1808. [Google Scholar] [CrossRef] [Green Version]
- Rauch, B.; Schiele, R.; Schneider, S.; Diller, F.; Victor, N.; Gohlke, H.; Gottwik, M.; Steinbeck, G.; Del Castillo, U.; Sack, R.; et al. OMEGA, a randomized, placebo-controlled trial to test the effect of highly purified omega-3 fatty acids on top of modern guideline-adjusted therapy after myocardial infarction. Circulation 2010, 122, 2152–2159. [Google Scholar] [CrossRef] [Green Version]
- Makuuchi, H.; Furuse, A.; Endo, M.; Nakamura, H.; Daida, H.; Watanabe, M.; Ohashi, Y.; Hosoda, Y.; Hosoda, S.; Yamaguchi, H.; et al. Effect of pravastatin on progression of coronary atherosclerosis in patients after coronary artery bypass surgery. Circ. J. 2005, 69, 636–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kjekshus, J.; Apetrei, E.; Barrios, V.; Bohm, M.; Cleland, J.G.; Cornel, J.H.; Dunselman, P.; Fonseca, C.; Goudev, A.; Grande, P.; et al. Rosuvastatin in older patients with systolic heart failure. N. Engl. J. Med. 2007, 357, 2248–2261. [Google Scholar] [CrossRef]
- Liem, A.H.; van Boven, A.J.; Veeger, N.J.; Withagen, A.J.; Robles de Medina, R.M.; Tijssen, J.G.; van Veldhuisen, D.J. Effect of fluvastatin on ischaemia following acute myocardial infarction: A randomized trial. Eur. Heart J. 2002, 23, 1931–1937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plehn, J.F.; Davis, B.R.; Sacks, F.M.; Rouleau, J.L.; Pfeffer, M.A.; Bernstein, V.; Cuddy, T.E.; Moye, L.A.; Piller, L.B.; Rutherford, J.; et al. Reduction of stroke incidence after myocardial infarction with pravastatin: The Cholesterol and Recurrent Events (CARE) study. The Care Investigators. Circulation 1999, 99, 216–223. [Google Scholar] [CrossRef]
- Koren, M.J.; Hunninghake, D.B.; Investigators, A. Clinical outcomes in managed-care patients with coronary heart disease treated aggressively in lipid-lowering disease management clinics: The alliance study. J. Am. Coll. Cardiol. 2004, 44, 1772–1779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knopp, R.H.; d’Emden, M.; Smilde, J.G.; Pocock, S.J. Efficacy and safety of atorvastatin in the prevention of cardiovascular end points in subjects with type 2 diabetes: The Atorvastatin Study for Prevention of Coronary Heart Disease Endpoints in non-insulin-dependent diabetes mellitus (ASPEN). Diabetes Care 2006, 29, 1478–1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kromhout, D.; Giltay, E.J.; Geleijnse, J.M.; Alpha Omega Trial, G. n-3 fatty acids and cardiovascular events after myocardial infarction. N. Engl. J. Med. 2010, 363, 2015–2026. [Google Scholar] [CrossRef]
- Jukema, J.W.; Bruschke, A.V.; van Boven, A.J.; Reiber, J.H.; Bal, E.T.; Zwinderman, A.H.; Jansen, H.; Boerma, G.J.; van Rappard, F.M.; Lie, K.I.; et al. Effects of lipid lowering by pravastatin on progression and regression of coronary artery disease in symptomatic men with normal to moderately elevated serum cholesterol levels. The Regression Growth Evaluation Statin Study (REGRESS). Circulation 1995, 91, 2528–2540. [Google Scholar] [CrossRef]
- Ostadal, P.; Alan, D.; Vejvoda, J.; Kukacka, J.; Macek, M.; Hajek, P.; Mates, M.; Kvapil, M.; Kettner, J.; Wiendl, M.; et al. Fluvastatin in the first-line therapy of acute coronary syndrome: Results of the multicenter, randomized, double-blind, placebo-controlled trial (the FACS-trial). Trials 2010, 11, 61. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, H.; Arakawa, K.; Itakura, H.; Kitabatake, A.; Goto, Y.; Toyota, T.; Nakaya, N.; Nishimoto, S.; Muranaka, M.; Yamamoto, A.; et al. Primary prevention of cardiovascular disease with pravastatin in Japan (MEGA Study): A prospective randomised controlled trial. Lancet 2006, 368, 1155–1163. [Google Scholar] [CrossRef]
- Nakagawa, T.; Kobayashi, T.; Awata, N.; Sato, S.; Reiber, J.H.; Nakajima, H.; Toyama, Y.N.; Hiraoka, H.; Kato, O.; Kirino, M.; et al. Randomized, controlled trial of secondary prevention of coronary sclerosis in normocholesterolemic patients using pravastatin: Final 5-year angiographic follow-up of the Prevention of Coronary Sclerosis (PCS) study. Int. J. Cardiol. 2004, 97, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Mok, V.C.; Lam, W.W.; Chen, X.Y.; Wong, A.; Ng, P.W.; Tsoi, T.H.; Yeung, V.; Liu, R.; Soo, Y.; Leung, T.W.; et al. Statins for asymptomatic middle cerebral artery stenosis: The Regression of Cerebral Artery Stenosis study. Cerebrovasc. Dis. 2009, 28, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Einvik, G.; Klemsdal, T.O.; Sandvik, L.; Hjerkinn, E.M. A randomized clinical trial on n-3 polyunsaturated fatty acids supplementation and all-cause mortality in elderly men at high cardiovascular risk. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 588–592. [Google Scholar] [CrossRef] [PubMed]
- Galan, P.; Kesse-Guyot, E.; Czernichow, S.; Briancon, S.; Blacher, J.; Hercberg, S.; Group, S.F.O.C. Effects of B vitamins and omega 3 fatty acids on cardiovascular diseases: A randomised placebo controlled trial. Br. Med. J. 2010, 341, c6273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furberg, C.D.; Pitt, B.; Byington, R.P.; Park, J.S.; McGovern, M.E. Reduction in coronary events during treatment with pravastatin. PLAC I and PLAC II Investigators. Pravastatin Limitation of Atherosclerosis in the Coronary Arteries. Am. J. Cardiol. 1995, 76, 60C–63C. [Google Scholar] [CrossRef]
- Furberg, C.D.; Adams, H.P., Jr.; Applegate, W.B.; Byington, R.P.; Espeland, M.A.; Hartwell, T.; Hunninghake, D.B.; Lefkowitz, D.S.; Probstfield, J.; Riley, W.A.; et al. Effect of lovastatin on early carotid atherosclerosis and cardiovascular events. Asymptomatic Carotid Artery Progression Study (ACAPS) Research Group. Circulation 1994, 90, 1679–1687. [Google Scholar] [CrossRef] [Green Version]
- Heart Protection Study Collaborative, G.; Jonathan, E.; Derrick, B.; Emma, L.; Sarah, P.; John, D.; Jane, A.; Rory, C. C-reactive protein concentration and the vascular benefits of statin therapy: An analysis of 20,536 patients in the Heart Protection Study. Lancet 2011, 377, 469–476. [Google Scholar] [CrossRef] [Green Version]
- Yusuf, S.; Bosch, J.; Dagenais, G.; Zhu, J.; Xavier, D.; Liu, L.; Pais, P.; Lopez-Jaramillo, P.; Leiter, L.A.; Dans, A.; et al. Cholesterol lowering in intermediate-risk persons without cardiovascular disease. N. Engl. J. Med. 2016, 374, 2021–2031. [Google Scholar] [CrossRef] [Green Version]
- Downs, J.R.; Clearfield, M.; Weis, S.; Whitney, E.; Shapiro, D.R.; Beere, P.A.; Langendorfer, A.; Stein, E.A.; Kruyer, W.; Gotto, A.M., Jr. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: Results of AFCAPS/TexCAPS. Air Force/Texas Coronary Atherosclerosis Prevention Study. J. Am. Med. Acad. 1998, 279, 1615–1622. [Google Scholar] [CrossRef]
- Officers, A.; Coordinators for the, A.C.R.G.T.A.; Lipid-Lowering Treatment to Prevent Heart Attack, T. Major outcomes in moderately hypercholesterolemic, hypertensive patients randomized to pravastatin vs usual care: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT-LLT). J. Am. Med. Acad. 2002, 288, 2998–3007. [Google Scholar] [CrossRef]
- Colhoun, H.M.; Betteridge, D.J.; Durrington, P.N.; Hitman, G.A.; Neil, H.A.; Livingstone, S.J.; Thomason, M.J.; Mackness, M.I.; Charlton-Menys, V.; Fuller, J.H.; et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): Multicentre randomised placebo-controlled trial. Lancet 2004, 364, 685–696. [Google Scholar] [CrossRef]
- Investigators, O.T.; Bosch, J.; Gerstein, H.C.; Dagenais, G.R.; Diaz, R.; Dyal, L.; Jung, H.; Maggiono, A.P.; Probstfield, J.; Ramachandran, A.; et al. n-3 fatty acids and cardiovascular outcomes in patients with dysglycemia. N. Engl. J. Med. 2012, 367, 309–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bestehorn, H.P.; Rensing, U.F.; Roskamm, H.; Betz, P.; Benesch, L.; Schemeitat, K.; Blumchen, G.; Claus, J.; Mathes, P.; Kappenberger, L.; et al. The effect of simvastatin on progression of coronary artery disease. The Multicenter coronary Intervention Study (CIS). Eur. Heart J. 1997, 18, 226–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karam, J.G.; Loney-Hutchinson, L.; McFarlane, S.I. Stroke prevetion by aggressive reduction in cholestrol levels investigators. High-dose atorvastatin after stroke or transient ischemic attack: The Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators. J. Cardiometab. Syndr. 2008, 3, 68–69. [Google Scholar] [CrossRef]
- Athyros, V.G.; Papageorgiou, A.A.; Mercouris, B.R.; Athyrou, V.V.; Symeonidis, A.N.; Basayannis, E.O.; Demitriadis, D.S.; Kontopoulos, A.G. Treatment with atorvastatin to the National Cholesterol Educational Program goal versus ’usual’ care in secondary coronary heart disease prevention. The GREek Atorvastatin and Coronary-heart-disease Evaluation (GREACE) study. Curr. Med. Res. Opin. 2002, 18, 220–228. [Google Scholar] [CrossRef]
- Writing Group for the, A.R.G.; Bonds, D.E.; Harrington, M.; Worrall, B.B.; Bertoni, A.G.; Eaton, C.B.; Hsia, J.; Robinson, J.; Clemons, T.E.; Fine, L.J.; et al. Effect of long-chain omega-3 fatty acids and lutein + zeaxanthin supplements on cardiovascular outcomes: Results of the Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. J. Am. Med. Acad. Intern. Med. 2014, 174, 763–771. [Google Scholar] [CrossRef]
- Cannon, C.P.; Braunwald, E.; McCabe, C.H.; Rader, D.J.; Rouleau, J.L.; Belder, R.; Joyal, S.V.; Hill, K.A.; Pfeffer, M.A.; Skene, A.M.; et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N. Engl. J. Med. 2004, 350, 1495–1504. [Google Scholar] [CrossRef]
- Deedwania, P.; Stone, P.H.; Bairey Merz, C.N.; Cosin-Aguilar, J.; Koylan, N.; Luo, D.; Ouyang, P.; Piotrowicz, R.; Schenck-Gustafsson, K.; Sellier, P.; et al. Effects of intensive versus moderate lipid-lowering therapy on myocardial ischemia in older patients with coronary heart disease: Results of the Study Assessing Goals in the Elderly (SAGE). Circulation 2007, 115, 700–707. [Google Scholar] [CrossRef] [Green Version]
- Izawa, A.; Kashima, Y.; Miura, T.; Ebisawa, S.; Kitabayashi, H.; Yamamoto, H.; Sakurai, S.; Kagoshima, M.; Tomita, T.; Miyashita, Y.; et al. Assessment of lipophilic vs. hydrophilic statin therapy in acute myocardial infarction—ALPS-AMI study. Circ. J. 2015, 79, 161–168. [Google Scholar] [CrossRef] [Green Version]
- Nicholls, S.J.; Ballantyne, C.M.; Barter, P.J.; Chapman, M.J.; Erbel, R.M.; Libby, P.; Raichlen, J.S.; Uno, K.; Borgman, M.; Wolski, K.; et al. Effect of two intensive statin regimens on progression of coronary disease. N. Engl. J. Med. 2011, 365, 2078–2087. [Google Scholar] [CrossRef] [Green Version]
- Nissen, S.E.; Tuzcu, E.M.; Schoenhagen, P.; Brown, B.G.; Ganz, P.; Vogel, R.A.; Crowe, T.; Howard, G.; Cooper, C.J.; Brodie, B.; et al. Effect of intensive compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis: A randomized controlled trial. J. Am. Med. Acad. 2004, 291, 1071–1080. [Google Scholar] [CrossRef]
- Pedersen, T.R.; Faergeman, O.; Kastelein, J.J.; Olsson, A.G.; Tikkanen, M.J.; Holme, I.; Larsen, M.L.; Bendiksen, F.S.; Lindahl, C.; Szarek, M.; et al. High-dose atorvastatin vs usual-dose simvastatin for secondary prevention after myocardial infarction: The IDEAL study: A randomized controlled trial. J. Am. Med. Acad. 2005, 294, 2437–2445. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T., Jr.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Ascend Study Collaborative Group; Bowman, L.; Mafham, M.; Wallendszus, K.; Stevens, W.; Buck, G.; Barton, J.; Murphy, K.; Aung, T.; Haynes, R.; et al. Effects of n-3 fatty acid supplements in diabetes mellitus. N. Engl. J. Med. 2018, 379, 1540–1550. [Google Scholar] [CrossRef]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Albert, C.M.; Gordon, D.; Copeland, T.; et al. Marine n-3 fatty acids and prevention of cardiovascular disease and cancer. N. Engl. J. Med. 2019, 380, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M. Primary prevention of cardiovascular disease with statins: Assessing the evidence base behind clinical guidance. Clin. Pharm. 2016, 8. [Google Scholar] [CrossRef]
- Bird, J.K.; Calder, P.C.; Eggersdorfer, M. The role of n-3 long chain polyunsaturated fatty acids in cardiovascular disease prevention, and interactions with statins. Nutrients 2018, 10, 775. [Google Scholar] [CrossRef] [Green Version]
- Colussi, G.; Catena, C.; Novello, M.; Bertin, N.; Sechi, L.A. Impact of omega-3 polyunsaturated fatty acids on vascular function and blood pressure: Relevance for cardiovascular outcomes. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 191–200. [Google Scholar] [CrossRef]
- Gelosa, P.; Cimino, M.; Pignieri, A.; Tremoli, E.; Guerrini, U.; Sironi, L. The role of HMG-CoA reductase inhibition in endothelial dysfunction and inflammation. Vasc. Health Risk Manag. 2007, 3, 567–577. [Google Scholar]
- Kwak, S.M.; Myung, S.K.; Lee, Y.J.; Seo, H.G.; Korean Meta-analysis Study, G. Efficacy of omega-3 fatty acid supplements (eicosapentaenoic acid and docosahexaenoic acid) in the secondary prevention of cardiovascular disease: A meta-analysis of randomized, double-blind, placebo-controlled trials. Arch. Intern. Med. 2012, 172, 686–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizos, E.C.; Ntzani, E.E.; Bika, E.; Kostapanos, M.S.; Elisaf, M.S. Association between omega-3 fatty acid supplementation and risk of major cardiovascular disease events: A systematic review and meta-analysis. J. Am. Med. Acad. 2012, 308, 1024–1033. [Google Scholar] [CrossRef] [PubMed]
- Hooper, L.; Al-Khudairy, L.; Abdelhamid, A.S.; Rees, K.; Brainard, J.S.; Brown, T.J.; Ajabnoor, S.M.; O’Brien, A.T.; Winstanley, L.E.; Donaldson, D.H.; et al. Omega-6 fats for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2018, 7, CD011094. [Google Scholar] [CrossRef] [Green Version]
- Czernichow, S.; Thomas, D.; Bruckert, E. n-6 Fatty acids and cardiovascular health: A review of the evidence for dietary intake recommendations. Br. J. Nutr. 2010, 104, 788–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erkkila, A.; de Mello, V.D.; Riserus, U.; Laaksonen, D.E. Dietary fatty acids and cardiovascular disease: An epidemiological approach. Prog. Lipid Res. 2008, 47, 172–187. [Google Scholar] [CrossRef]
- Ramsden, C.E.; Hibbeln, J.R.; Majchrzak, S.F.; Davis, J.M. n-6 fatty acid-specific and mixed polyunsaturate dietary interventions have different effects on CHD risk: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2010, 104, 1586–1600. [Google Scholar] [CrossRef] [Green Version]
- DiNicolantonio, J.J.; O’Keefe, J.H. Omega-6 vegetable oils as a driver of coronary heart disease: The oxidized linoleic acid hypothesis. Open Heart 2018, 5, e000898. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Age (Years) | Follow-Up (Years) | MI (%) | Hypertension (%) | Diabetes (%) | Smoker (%) | Intervention Arm | Comparison Arm | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Treatment | N | Total CVD | CHD | MI | Stroke | Treatment | N | Total CVD | CHD | MI | Stroke | |||||||
| Manson 2019 (VITAL) [88] | 67.1 | 5.3 | 49.8 | 13.7 | 7.2 | EPA+DHA | 12,933 | 308 | 145 | 148 | 527 | Control | 12,938 | 370 | 200 | 142 | 567 | |
| Bhatt 2019 (REDUCE-IT) [86] | 64 | 4.9 | 58.6 | Icosapent Ethyl | 4069 | 250 | Control | 4090 | 355 | |||||||||
| Bowman 2018 (ASCEND) [87] | 63.3 | 7.4 | 0 | 49.4 | 100 | 53.8 | EPA+DHA | 7740 | 186 | 252 | Control | 7740 | 200 | 251 | ||||
| Yusuf 2016 (HOPE-3) [71] | 63.8 | 5.6 | 0 | 37.9 | 5.8 | 27.7 | Rosuvastatin | 6361 | 105 | 45 | 70 | Control | 6344 | 140 | 69 | 99 | ||
| Ford 2016 (WOSCOPS) [33] | 55 | 4.9 | 0 | 44 | Pravastatin | 3302 | 194 | Control | 3293 | 223 | ||||||||
| Izawa 2015 (ALPS-AMI) [82] | 66 | 2 | 63.2 | Pravastatin | 253 | 5 | Atorvastatin | 255 | 1 | |||||||||
| Hosomi 2015 (J-STAR) [32] | 4.9 | 76 | 23.4 | 53.6 | Pravastatin | 780 | 5 | Control | 785 | 12 | ||||||||
| Bonds 2014 (AREDS2) [79] | 74 | 4.8 | 7 | 5.9 | 13 | 56.6 | EPA+DHA | 2147 | 183 | 28 | 28 | 48 | Control | 2056 | 187 | 30 | 30 | 41 |
| Takano 2013 (PEARL) [43] | 62.6 | 3 | 25.1 | 45.3 | 27.4 | Pitavastatin | 288 | 3 | 8 | Control | 286 | 8 | 9 | |||||
| Roncaglioni 2013 (Risk & Prevention) [52] | 64 | 5 | 84.6 | 59.9 | 21.7 | EPA+DHA | 6239 | 620 | 310 | 80 | 80 | Control | 6266 | 630 | 324 | 90 | 60 | |
| Macchia 2013 (FORWARD) [14] | 66.1 | 91.4 | 12.9 | 42.2 | EPA+DHA | 289 | 4 | 1 | 3 | Control | 297 | 4 | 1 | 3 | ||||
| Yakusevich 2012 [35] | 65.7 | 1 | 9.8 | 77.6 | 9.8 | Simvastatin | 86 | 4 | 5 | Control | 97 | 5 | 7 | |||||
| Bosch 2012 (ORIGIN) [75] | 63.5 | 6.2 | 79.5 | 12.4 | EPA+DHA | 6281 | 2055 | 344 | 314 | Control | 6255 | 2087 | 316 | 336 | ||||
| Nicholls 2011 (SATURN) [83] | 57.6 | 2 | 24.4 | 70.4 | 15.3 | 32.3 | Atorvastatin | 519 | 11 | 2 | Rosuvastatin | 520 | 11 | 3 | ||||
| Emberson 2011 (MRC/BHF) [70] | 64 | 5 | 43.5 | 30.4 | 74.8 | Simvastatin | 10,269 | 444 | Control | 10,267 | 585 | |||||||
| Ostadal 2010 (FACS) [62] | 62.1 | 1 | 7.7 | 51.3 | 19.2 | 29.2 | Fluvastatin | 78 | 10 | 2 | 1 | Control | 78 | 21 | 4 | 3 | ||
| Kromhout 2010 (AlphaOmega) [60] | 69 | 3.4 | 100 | 89.7 | 21 | 16.9 | EPA+DHA | 2404 | 170 | 122 | 89 | 11 | Control | 2433 | 185 | 132 | 102 | 10 |
| Galan 2010 (SU.FOL.OM3) [67] | 61.4 | 4.7 | 46 | 72.8 | EPA+DHA | 1253 | 81 | 51 | 32 | 29 | Control | 1248 | 76 | 53 | 28 | 28 | ||
| Einvik 2010 (DO IT) [66] | 70 | 3 | 28 | 14.5 | 34 | EPA+DHA | 282 | 32 | 11 | 11 | Control | 281 | 36 | 9 | 9 | |||
| Dangour 2010 (OPAL) [13] | 75 | 2 | 3.9 | 55.9 | EPA+DHA | 434 | 7 | Control | 433 | 8 | ||||||||
| Chan 2010 (ASTRONOMER) [34] | 58 | 3.5 | 48.3 | Rosuvastatin | 134 | 35 | Control | 135 | 44 | |||||||||
| Rauch 2009 (OMEGA) [53] | 64 | 1 | 14.4 | 66.5 | 27 | 36.7 | EPA+DHA | 1919 | 199 | 547 | 87 | 27 | Control | 1885 | 165 | 568 | 78 | 13 |
| Mok 2009 (RCASS) [65] | 63 | 2 | 69.2 | 91.2 | 26.4 | Simvastatin | 113 | 2 | Control | 114 | 3 | |||||||
| Fellstrom 2009 (AURORA) [33] | 64.2 | 3.8 | 10.2 | 26.4 | 15.5 | Rosuvastatin | 1389 | 91 | 53 | Control | 1384 | 107 | 45 | |||||
| Tavazzi 2008 (GISSI-HF) [45] | 68 | 3.9 | 14.2 | 54.6 | 28.3 | 14.2 | EPA+DHA | 3494 | 1635 | 107 | 122 | Control | 3481 | 1687 | 129 | 103 | ||
| Tavazzi 2008 (GISSI-HF) [37] | 68 | 3.9 | 54.3 | 14.1 | Atorvastatin | 2285 | 61 | 82 | Control | 2289 | 70 | 66 | ||||||
| Ridker 2008 (JUPITER) [47] | 66 | 1.9 | 0 | 15.8 | Rosuvastatin | 8901 | 31 | 33 | Control | 8901 | 69 | 64 | ||||||
| Yokoyama 2007 (JELIS) [36] | 61 | 4.6 | 5.6 | 35.5 | 16.3 | 18.9 | EPA | 9326 | 262 | 71 | 166 | Control | 9319 | 324 | 93 | 162 | ||
| Kjekshus 2007 (CORONA) [55] | 73 | 2.7 | 60 | 63 | 29.5 | 8.6 | Rosuvastatin | 2514 | 131 | 126 | Control | 2497 | 154 | 138 | ||||
| Deedwania 2007 (SAGE) [81] | 72.5 | 1 | 45.9 | 64.5 | 23.2 | 59.4 | Atorvastatin | 446 | 16 | 1 | Pravastatin | 445 | 16 | 3 | ||||
| Nakamura 2006 (MEGA) [63] | 58.3 | 5.3 | 41.8 | 20.8 | 20.6 | Pravastatin | 3866 | 125 | 66 | 17 | 50 | Control | 3966 | 172 | 101 | 33 | 62 | |
| Knopp 2006 (ASPEN) [59] | 61 | 4 | 16.4 | 55.1 | 100 | 12.4 | Atorvastatin | 1211 | 297 | Control | 1199 | 313 | ||||||
| Brouwer 2006 (SOFA) [12] | 61.5 | 1 | 62.6 | 50.7 | 15.9 | 67 | EPA+DHA | 273 | 65 | 1 | Control | 273 | 62 | 3 | ||||
| Amarenco 2006 (SPARCL) [77] | 62.7 | 4.9 | 59 | Atorvastatin | 2365 | 530 | 123 | 43 | 265 | Control | 2366 | 687 | 204 | 82 | 311 | |||
| Yokoi 2005 (ATHEROMA) [40] | 59.3 | 3 | 45.5 | 42 | 18.8 | Pravastatin | 142 | 23 | 2 | 5 | Control | 146 | 25 | 4 | 4 | |||
| Wanner 2005 [41] | 65.7 | 4 | 17.6 | 100 | 40.4 | Atorvastatin | 619 | 205 | 93 | 60 | Control | 636 | 246 | 112 | 45 | |||
| Stone 2005 [42] | 1 | 38.9 | 62.4 | 16.5 | 69.5 | Atorvastatin | 96 | 1 | Control | 103 | 1 | |||||||
| Raitt 2005 [16] | 62.5 | 2 | 55.5 | 50.5 | EPA+DHA | 100 | 2 | 1 | 1 | Control | 100 | 5 | 3 | 3 | ||||
| Pedersen 2005 (IDEAL) [85] | 61.7 | 4.8 | 28 | 58.4 | 12 | 79.1 | Atorvastatin | 4439 | 1176 | 898 | 267 | 151 | Simvastatin | 4449 | 1370 | 1059 | 321 | 174 |
| Makuuchi 2005 (PCABG) [54] | 58.9 | 4.5 | 62 | 51.5 | 33.3 | 41.9 | Pravastatin | 152 | 26 | 1 | 4 | Control | 151 | 36 | 4 | 3 | ||
| Sever 2004 (ASCOT-LLA) [46] | 63 | 5 | 100 | 24.6 | 32.7 | Atorvastatin | 5168 | 389 | 89 | Control | 5137 | 486 | 121 | |||||
| Nissen 2004 (REVERSAL) [84] | 56.2 | 1.5 | 68.5 | 18.9 | 26.3 | Atorvastatin | 253 | 4 | 1 | Pravastatin | 249 | 7 | 1 | |||||
| Nakagawa 2004 (PCS) [64] | 55 | 5.4 | 59.2 | 17.5 | 67.5 | Pravastatin | 54 | 13 | 2 | 3 | Control | 66 | 19 | 3 | 4 | |||
| Koren 2004 (ALLIANCE) [58] | 61.2 | 4.5 | 57.8 | 22.1 | 19.5 | Atorvastatin | 1217 | 408 | 52 | 35 | Control | 1225 | 443 | 94 | 39 | |||
| Colhoun 2004 (CARDS) [74] | 62 | 3.9 | 100 | 65.3 | Atorvastatin | 1428 | 21 | Control | 1410 | 39 | ||||||||
| Cannon 2004 (PROVE IT-TIMI) [80] | 58.2 | 2 | 18.5 | 50.2 | 17.6 | Atorvastatin | 2099 | 139 | 21 | Pravastatin | 2063 | 153 | 21 | |||||
| Shepherd 2002 (PROSPER) [49] | 75.3 | 3.2 | 13.4 | 61.9 | 10.7 | 26.8 | Pravastatin | 2891 | 454 | 77 | 135 | Control | 2913 | 523 | 102 | 131 | ||
| Serruys 2002 (LIPS) [50] | 60 | 3.9 | 44.4 | 38.6 | 12 | 71.5 | Fluvastatin | 844 | 2 | Control | 833 | 1 | ||||||
| Sawayama 2002 (FAST) [51] | 66.3 | 2 | 39.6 | 25 | 57.8 | Pravastatin | 83 | 4 | 4 | Control | 81 | 11 | 11 | |||||
| Liem 2002 (FLORIDA) [56] | 60.5 | 1 | 11.5 | Fluvastatin | 265 | 21 | Control | 275 | 13 | |||||||||
| Davis 2002 (ALLHAT-LTT) [73] | 66.4 | 4.8 | 35.1 | 23.2 | Pravastatin | 5170 | 209 | Control | 5185 | 231 | ||||||||
| Arthros 2002 (GREACE) [78] | 58.5 | 3 | 81.2 | 42.9 | 19.6 | Atorvastatin | 800 | 21 | 9 | Control | 800 | 51 | 17 | |||||
| Nilsen 2001 [15] | 64 | 1.5 | 23.3 | 24.3 | 10.3 | 75.7 | EPA+DHA | 150 | 42 | 17 | Control | 150 | 36 | 12 | ||||
| Teo 2000 (SCAT) [39] | 61 | 4 | 70 | 36 | 11 | 82 | Simvastatin | 230 | 11 | 4 | Control | 230 | 10 | 7 | ||||
| Valagussa 1999 (GISSI-P) [44] | 59.4 | 3.5 | 12 | 35.6 | 14.8 | 77.2 | EPA+DHA | 2836 | 44 | Control | 2828 | 41 | ||||||
| Riegger 1999 [48] | 59.8 | 1 | 35.6 | 29.3 | 5.5 | 9.6 | Fluvastatin | 187 | Control | 178 | ||||||||
| Plehn 1999 (CARE) [57] | 5 | 100 | 42.7 | 14.1 | 16.1 | Pravastatin | 2081 | 92 | Control | 2078 | 124 | |||||||
| Tonkin 1998 (LIPID) [38] | 62 | 6.1 | 41.7 | 8.7 | 73.3 | Pravastatin | 4512 | 336 | 169 | Control | 4502 | 463 | 204 | |||||
| Downs 1998 (AFCAPS/TexCAPS) [72] | 58 | 5.2 | 21.9 | 2.3 | 12.4 | Lovastatin | 3304 | 194 | 163 | 57 | Control | 3301 | 255 | 215 | 95 | |||
| Bestehorn 1997 (CIS) [76] | 49.8 | 2.3 | 84.3 | Simvastatin | 129 | 1 | Control | 125 | 5 | |||||||||
| Jukema 1995 (REGRESS) [61] | 56 | 2 | 47.4 | 27.8 | 0.1 | 88 | Pravastatin | 450 | 59 | Control | 434 | 93 | ||||||
| Furberg 1995 (PLAC-I & II) [68] | 58 | 3 | 48.5 | 40.5 | 0.7 | 15.5 | Pravastatin | 281 | 14 | 9 | Control | 278 | 29 | 24 | ||||
| Furberg 1994 (ACAPS) [69] | 62 | 2.8 | 28.8 | 56.5 | Lovastatin | 460 | 5 | Control | 459 | 5 | ||||||||
| Study | Baseline Measurement | Change Difference | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intervention Arm | Comparison Arm | |||||||||||
| TC (mg/dL) | TG (mg/dL) | HDL-C (mg/dL) | LDL-C (mg/dL) | TC (mg/dL) | TG (mg/dL) | HDL-C (mg/dL) | LDL-C (mg/dL) | TC (mg/dL) | TG (mg/dL) | HDL-C (mg/dL) | LDL-C (mg/dL) | |
| Manson 2019 (VITAL) [88] | ||||||||||||
| Bhatt 2019 (REDUCE-IT) [86] | 216.5 | 40.0 | 74.0 | 216.0 | 40.0 | 76.0 | −32.5 | 0 | −5.0 | |||
| Bowman 2018 (ASCEND) [87] | ||||||||||||
| Yusuf 2016 (HOPE-3) [71] | 201.5 | 128.8 | 44.7 | 127.8 | 201.3 | 126.5 | 44.9 | 127.9 | −21.2 | −34.6 | ||
| Ford 2016 (WOSCOPS) [33] | 272.0 | 162.0 | 44.0 | 192.0 | 272.0 | 164.0 | 44.0 | 192.0 | ||||
| Izawa 2015 (ALPS-AMI) [82] | 204.1 | 142.9 | 47.6 | 130.2 | 203.2 | 130.8 | 48.0 | 131.0 | −0.6 | |||
| Hosomi 2015 (J-STAR) [32] | 210.8 | 142.6 | 53.8 | 129.5 | 209.6 | 141.7 | 53.0 | 129.5 | −23.2 | −9.7 | 0.8 | −21.3 |
| Bonds 2014 (AREDS2) [79] | ||||||||||||
| Takano 2013 (PEARL) [43] | 203.2 | 50.7 | 125.2 | 201.2 | 50.8 | 125.5 | 2.0 | −31.5 | ||||
| Roncaglioni 2013 (Risk & Prevention) [52] | 215.6 | 150.0 | 50.9 | 131.8 | 216.4 | 150.0 | 51.2 | 132.5 | −0.5 | −8.1 | 0.6 | −0.4 |
| Macchia 2013 (FORWARD) [14] | ||||||||||||
| Yakusevich 2012 [35] | 211.5 | 102.7 | 85.1 | 201.9 | 91.2 | 86.2 | −29.4 | −11.5 | 8.9 | |||
| Bosch 2012 (ORIGIN) [75] | 189.0 | 46.0 | 112.0 | 190.0 | 46.0 | 112.0 | −1.1 | −14.5 | 0.1 | 0.6 | ||
| Nicholls 2011 (SATURN) [83] | 193.5 | 130.0 | 44.7 | 119.9 | 144.1 | 110.0 | 48.6 | 70.2 | −44.7 | −30.0 | 2.1 | −42.1 |
| Emberson 2011 (MRC/BHF) [70] | −32.9 | |||||||||||
| Ostadal 2010 (FACS) [62] | 212.7 | 208.8 | −56.2 | |||||||||
| Kromhout 2010 (AlphaOmega) [60] | 182.5 | 145.3 | 49.9 | 110.2 | 182.9 | 147.9 | 49.5 | 110.2 | ||||
| Galan 2010 (SU.FOL.OM3) [67] | 174.0 | 106.3 | 46.4 | 104.4 | 175.9 | 106.3 | 46.4 | 102.5 | ||||
| Einvik 2010 (DO IT) [66] | 243.6 | 150.6 | 54.1 | 158.1 | 239.8 | 150.6 | 54.1 | 154.7 | ||||
| Dangour 2010 (OPAL) [13] | ||||||||||||
| Chan 2010 (ASTRONOMER) [34] | 206.1 | 108.9 | 61.5 | 123.0 | 203.8 | 116.9 | 59.9 | 120.6 | 1.9 | −66.9 | ||
| Rauch 2009 (OMEGA) [53] | ||||||||||||
| Mok 2009 (RCASS) [65] | 226.2 | 118.7 | 45.6 | 151.6 | 227.0 | 125.8 | 44.9 | 150.4 | −54.5 | −11.5 | −50.7 | |
| Fellstrom 2009 (AURORA) [33] | 176.0 | 157.0 | 45.0 | 100.0 | 174.0 | 154.0 | 45.0 | 99.0 | −46 | −24.2 | 0 | −40.1 |
| Tavazzi 2008 (GISSI-HF) [45] | ||||||||||||
| Tavazzi 2008 (GISSI-HF) [37] | 122.2 | 121.0 | −0.1 | |||||||||
| Ridker 2008 (JUPITER) [47] | 186.0 | 118.0 | 49.0 | 108.0 | 185.0 | 118.0 | 49.0 | 108.0 | −19.0 | 0 | −54.0 | |
| Yokoyama 2007 (JELIS) [36] | 274.9 | 153.2 | 58.8 | 181.4 | 274.9 | 154.1 | 58.4 | 181.7 | 0 | −7.6 | 0 | |
| Kjekshus 2007 (CORONA) [55] | 178.0 | 48.0 | 137.0 | 176.0 | 47.0 | 136.0 | −42.0 | 2.0 | −63.0 | |||
| Deedwania 2007 (SAGE) [81] | 225.8 | 164.4 | 45.5 | 147.5 | 221.9 | 157.1 | 46.4 | 144.0 | −18.3 | −19.3 | −2.6 | −23.0 |
| Nakamura 2006 (MEGA) [63] | 242.5 | 127.5 | 57.6 | 156.6 | 242.5 | 127.5 | 57.6 | 156.6 | −20.5 | −14.2 | 19.3 | −20.7 |
| Knopp 2006 (ASPEN) [59] | 194.0 | 147.0 | 47.0 | 113.0 | 194.0 | 145.0 | 47.0 | 114.0 | −35.5 | −20.2 | 1.1 | −33.0 |
| Brouwer 2006 (SOFA) [12] | ||||||||||||
| Amarenco 2006 (SPARCL) [77] | 211.4 | 144.2 | 50.0 | 132.7 | 212.3 | 143.2 | 50.0 | 133.7 | −60.3 | −34.5 | 1.1 | −54.6 |
| Yokoi 2005 (ATHEROMA) [40] | 226.2 | 181.1 | 49.1 | 143.3 | 224.8 | 167.1 | 50.0 | 142.0 | −27.8 | −14.2 | 0.5 | −26.7 |
| Wanner 2005 [41] | 218.0 | 261.0 | 36.0 | 127.0 | 220.0 | 267.0 | 36.0 | 125.0 | −50.0 | |||
| Stone 2005 [42] | 228.0 | 149.0 | 44.0 | 149.0 | 230.0 | 151.0 | 43.0 | 151.0 | −35.9 | |||
| Raitt 2005 [16] | ||||||||||||
| Pedersen 2005 (IDEAL) [85] | 196.8 | 151.1 | 46.0 | 121.6 | 195.9 | 146.6 | 46.1 | 121.4 | −24.3 | −23.2 | −0.4 | −20.0 |
| Makuuchi 2005 (PCABG) [54] | 213.7 | 166.3 | 41.4 | 141.4 | 214.4 | 154.2 | 41.3 | 141.1 | −29.3 | −30.5 | 2.4 | −20.3 |
| Sever 2004 (ASCOT-LLA) [46] | 211.9 | 147.0 | 50.7 | 133.0 | 211.9 | 146.1 | 50.7 | 133.0 | −38.7 | −18.6 | 0.8 | 0 |
| Nissen 2004 (REVERSAL) [84] | 231.8 | 197.2 | 42.3 | 150.2 | 232.6 | 197.7 | 42.9 | 150.2 | −35.4 | −16.9 | −0.9 | −31.5 |
| Nakagawa 2004 (PCS) [64] | 200.1 | 141.9 | 43.0 | 128.7 | 200.5 | 143.9 | 43.3 | 128.3 | −17 | −7.9 | 0.4 | −15.3 |
| Koren 2004 (ALLIANCE) [58] | 226.0 | 197.0 | 40.0 | 147.0 | 225.0 | 198.0 | 41.0 | 146.0 | −20.0 | −12.0 | 0 | −16.0 |
| Colhoun 2004 (CARDS) [74] | 207.3 | 150.6 | 53.8 | 117.6 | 206.9 | 147.9 | 54.9 | 116.8 | −45.3 | −28.4 | 2.3 | −39.9 |
| Cannon 2004 (PROVE IT-TIMI) [80] | 181.0 | 158.0 | 38.0 | 106.0 | 180.0 | 154.0 | 39.0 | 106.0 | 0.3 | −33.0 | ||
| Shepherd 2002 (PROSPER) [49] | 220.4 | 132.9 | 50.3 | 146.9 | 220.4 | 132.9 | 50.3 | 146.9 | −34.8 | |||
| Serruys 2002 (LIPS) [50] | 200.0 | 160.0 | 38.0 | 131.0 | 199.0 | 160.0 | 37.0 | 132.0 | −1.0 | 0 | 0.3 | −49.9 |
| Sawayama 2002 (FAST) [51] | 251.5 | 168.7 | 56.7 | 160.7 | 255.2 | 135.8 | 56.5 | 171.6 | −1.8 | 15.3 | −43.1 | |
| Liem 2002 (FLORIDA) [56] | 204.9 | 150.6 | 46.4 | 135.3 | 208.8 | 141.7 | 46.4 | 139.2 | −45.4 | −29.2 | 1.8 | −40.9 |
| Davis 2002 (ALLHAT-LTT) [73] | 223.7 | 150.6 | 47.6 | 145.6 | 223.7 | 152.8 | 47.4 | 145.5 | −18.9 | 0.2 | 3.4 | −17.3 |
| Arthros 2002 (GREACE) [78] | 257.0 | 184.0 | 39.0 | 180.0 | 255.0 | 178.0 | 39.0 | 179.0 | −82.0 | −56.0 | 2.0 | −73.0 |
| Nilsen 2001 [15] | 229.7 | 145.3 | 41.8 | 231.6 | 137.3 | 44.9 | −11.3 | −52.9 | 4.8 | |||
| Teo 2000 (SCAT) [39] | 202.2 | 163.9 | 38.3 | 131.1 | 198.4 | 156.8 | 37.5 | 128.8 | −48.0 | −31.9 | 1.9 | −44.1 |
| Valagussa 1999 (GISSI-P) [44] | 210.2 | 162.6 | 41.5 | 137.3 | 211.6 | 161.9 | 41.7 | 138.5 | 2.6 | −6.3 | −0.2 | 4.2 |
| Riegger 1999 [48] | 289.0 | 189.0 | 53.0 | 198.0 | 284.0 | 183.0 | 56.0 | 193.0 | −36.4 | −37.9 | ||
| Plehn 1999 (CARE) [57] | 209.0 | 156.0 | 39.0 | 139.0 | 209.0 | 155.0 | 39.0 | 139.0 | 42.0 | 22.0 | −2.0 | 44.0 |
| Tonkin 1998 (LIPID) [38] | 218.0 | 142.0 | 36.0 | 150.0 | 218.0 | 138.0 | 36.0 | 150.0 | ||||
| Downs 1998 (AFCAPS/TexCAPS) [72] | 225.4 | 168.2 | 36.8 | 153.3 | 209.2 | 166.8 | 37.5 | 153.6 | −60.3 | −29.0 | 1.7 | −40.6 |
| Bestehorn 1997 (CIS) [76] | 240.3 | 44.3 | 164.5 | 243.4 | 43.6 | 167.4 | ||||||
| Jukema 1995 (REGRESS) [61] | 232.8 | 156.8 | 36.0 | 166.3 | 234.0 | 159.4 | 36.0 | 166.7 | −45.2 | −19.5 | 3.1 | −44.5 |
| Furberg 1995 (PLAC-I & II) [68] | 232.0 | 166.0 | 41.0 | 165.0 | 230.0 | 169.0 | 41.0 | 162.0 | ||||
| Furberg 1994 (ACAPS) [69] | 235.2 | 51.7 | 156.5 | 235.3 | 52.2 | 154.6 | ||||||
| N (I2) | Fixed-Effects Model | Random-Effects Model | |
|---|---|---|---|
| Total cardiovasculardisease | |||
| Statins | 14 (30.0%) | 0.81 (0.78–0.85) | 0.81 (0.76–0.86) |
| Atorvastatin | 4 (55.5%) | 0.83 (0.78–0.88) | 0.83 (0.76–0.91) |
| Fluvastatin | 1 (NA) | 0.48 (0.24–0.94) | 0.48 (0.24–0.94) |
| Lovastatin | 1 (NA) | 0.76 (0.63–0.91) | 0.76 (0.63–0.91) |
| Pravastatin | 7 (28.8%) | 0.81 (0.74–0.89) | 0.77 (0.67–0.89) |
| Rosuvastatin | 1 (NA) | 0.80 (0.55–1.16) | 0.80 (0.55–1.16) |
| Omega-3 | 13 (0%) | 0.98 (0.95–1.01) | 0.98 (0.95–1.01) |
| Overall | 27 (59.6%) | 0.92 (0.90–0.94) | 0.89 (0.85–0.94) |
| Coronary heart disease | |||
| Statins | 7 (0%) | 0.69 (0.62–0.77) | 0.70 (0.62–0.77) |
| Atorvastatin | 1 (NA) | 0.60 (0.49–0.75) | 0.60 (0.49–0.75) |
| Lovastatin | 1 (NA) | 0.76 (0.62–0.92) | 0.76 (0.62–0.92) |
| Pravastatin | 3 (0%) | 0.69 (0.56–0.84) | 0.69 (0.56–0.84) |
| Rosuvastatin | 1 (NA) | 0.75 (0.58–0.96) | 0.75 (0.58–0.96) |
| Simvastatin | 1 (NA) | 0.67 (0.11–3.95) | 0.67 (0.11–3.95) |
| Omega-3 | 10 (0%) | 0.90 (0.84–0.96) | 0.90 (0.85–0.96) |
| Overall | 17 (44.6%) | 0.84 (0.79–0.88) | 0.81 (0.75–0.89) |
| Myocardial infarction | |||
| Statins | 27 (51.4%) | 0.74 (0.69–0.79) | 0.69 (0.61–0.78) |
| Atorvastatin | 7 (73.6%) | 0.79 (0.71–0.87) | 0.70 (0.55–0.89) |
| Fluvastatin | 2 (42.6%) | 1.40 (0.76–2.56) | 1.18 (0.40–3.46) |
| Lovastatin | 2 (0%) | 0.62 (0.45–0.85) | 0.62 (0.45–0.85) |
| Pitavastatin | 1 (NA) | 0.37 (0.10–1.39) | 0.37 (0.10–1.39) |
| Pravastatin | 8 (3.1%) | 0.68 (0.60–0.77) | 0.66 (0.56–0.78) |
| Rosuvastatin | 4 (62.9%) | 0.74 (0.64–0.86) | 0.71 (0.55–0.91) |
| Simvastatin | 3 (11.2%) | 0.82 (0.43–1.56) | 0.85 (0.41–1.78) |
| Omega-3 | 15 (45.6%) | 0.88 (0.82–0.94) | 0.89 (0.80–0.99) |
| Overall | 42 (53.8%) | 0.81 (0.77–0.85) | 0.78 (0.72–0.85) |
| Stroke | |||
| Statins | 26 (33.3%) | 0.84 (0.80–0.89) | 0.85 (0.79–0.92) |
| Atorvastatin | 7 (64.9%) | 0.88 (0.79–0.98) | 0.88 (0.71–1.10) |
| Fluvastatin | 2 (11.4%) | 0.75 (0.17–3.31) | 0.77 (0.13–4.38) |
| Pravastatin | 9 (0%) | 0.88 (0.80–0.96) | 0.88 (0.80–0.96) |
| Rosuvastatin | 4 (68.8%) | 0.81 (0.70–0.95) | 0.80 (0.60–1.07) |
| Simvastatin | 3 (0%) | 0.76 (0.67–0.85) | 0.76 (0.67–0.85) |
| Omega-3 | 13 (36.1%) | 1.02 (0.94–1.10) | 0.88 (0.71–1.10) |
| Overall | 39 (46.2%) | 0.90 (0.86–0.94) | 0.91 (0.85–0.98) |
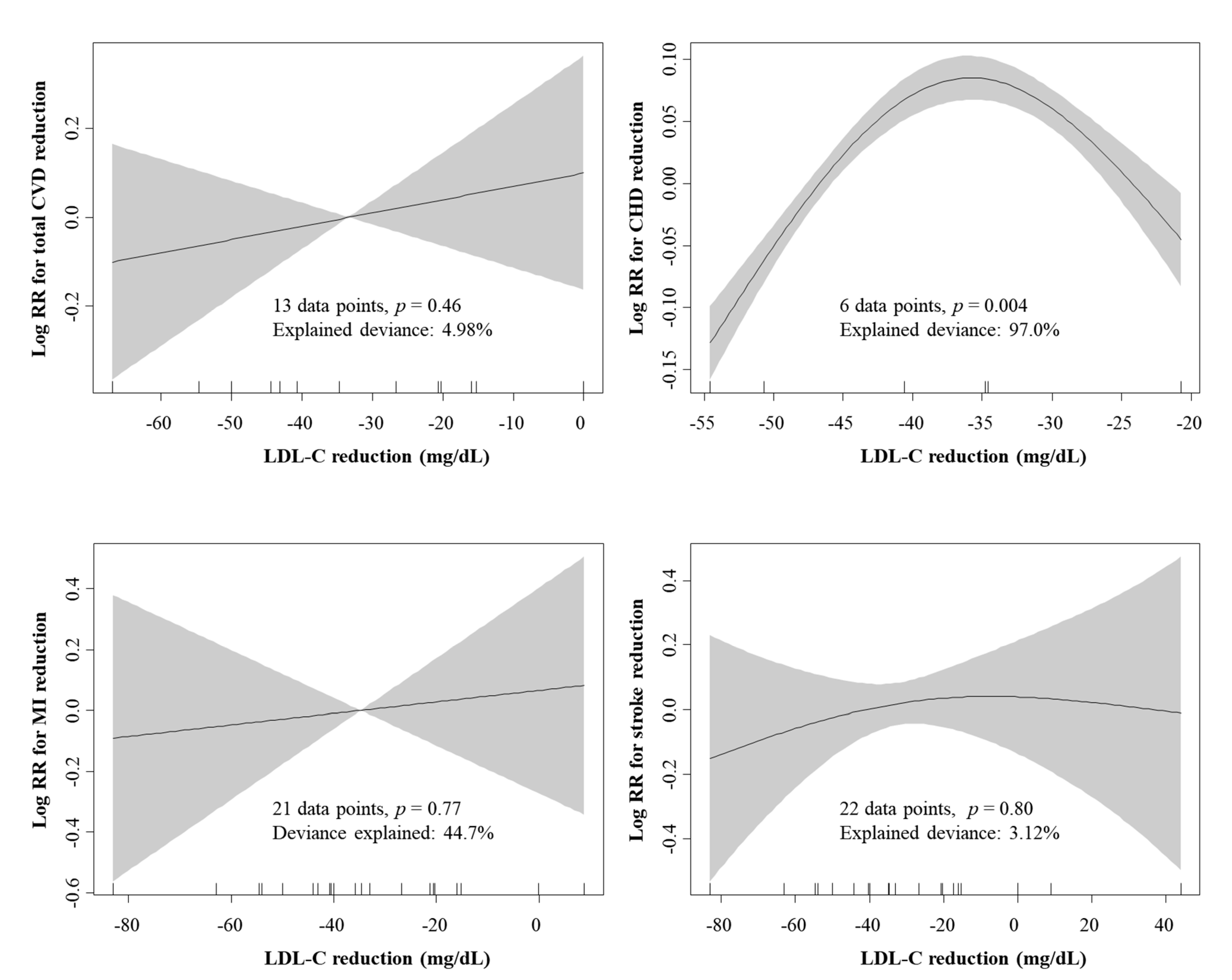
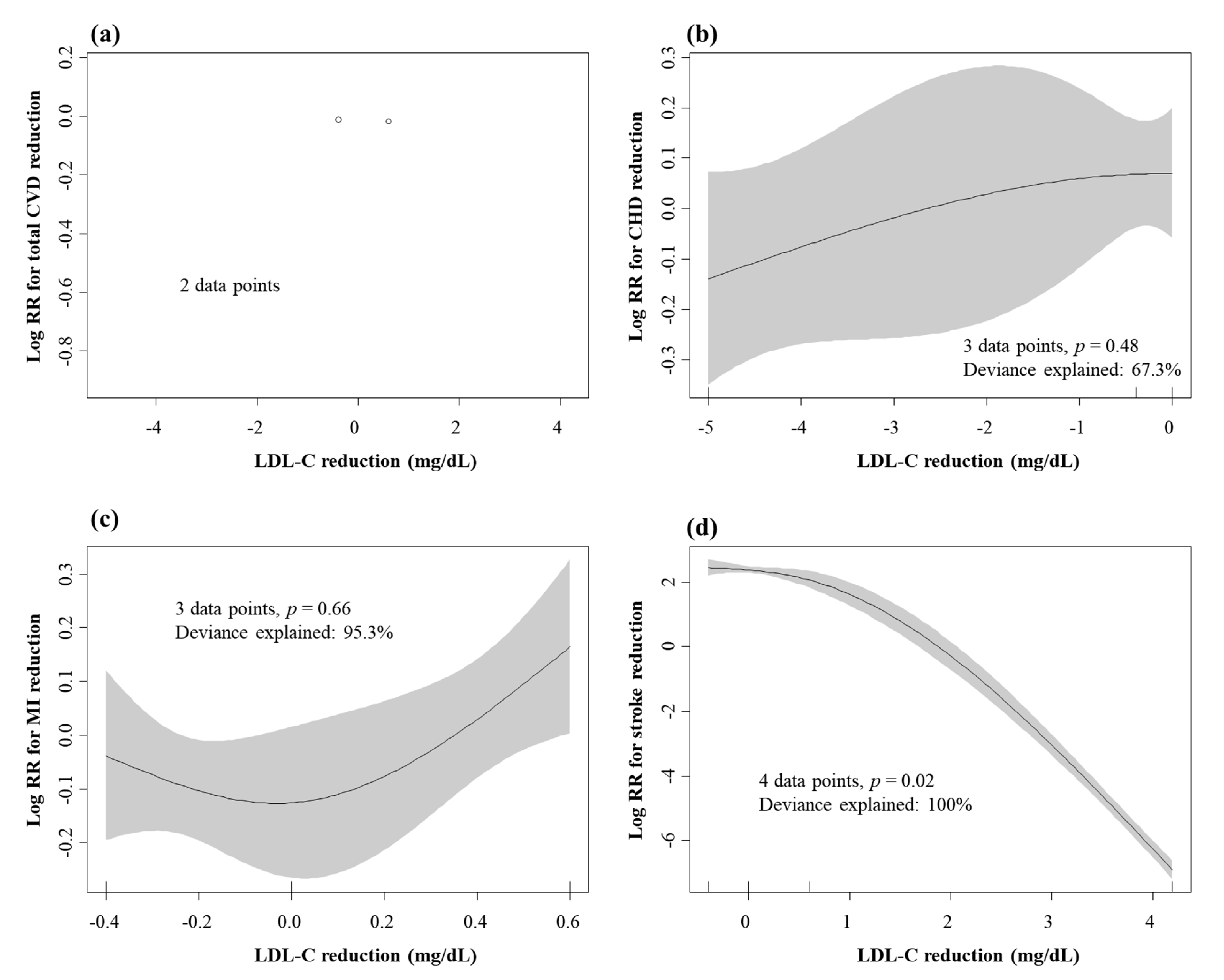
| Covariate | Total Cardiovascular Disease | Coronary Heart Disease | Myocardial Infarction | Stroke | ||||
|---|---|---|---|---|---|---|---|---|
| Coefficient | p-Value | Coefficient | p-Value | Coefficient | p-Value | Coefficient | p-Value | |
| TC | 0.0046 | <0.001 | 0.0042 | 0.047 | 0.0055 | 0.08 | −0.0111 | 0.53 |
| TG | 0.0026 | 0.51 | 0.0098 | 0.004 | 0.0009 | 0.89 | −0.0117 | 0.67 |
| HDL-C | −0.0116 | 0.18 | −0.0065 | 0.64 | −0.0198 | 0.35 | 0.0480 | 0.67 |
| LDL-C | 0.0034 | 0.004 | 0.0044 | 0.048 | 0.0048 | 0.09 | −0.0126 | 0.36 |
| 1st | 2nd | 3rd | 4th | 5th | 6th | 7th | 8th | 9th | SUCRA | |
|---|---|---|---|---|---|---|---|---|---|---|
| Total cardiovasculardisease | ||||||||||
| Control | 0 | 0 | 0 | 0 | 0.3 | 5.3 | 33.2 | 61.3 | 0.1 | |
| Omega-3 | 0 | 0 | 0 | 0.2 | 7.5 | 43.3 | 44.3 | 4.7 | 0.2 | |
| Simvastatin | 0 | 0 | 0.1 | 0.8 | 13.2 | 45.5 | 19.6 | 20.7 | 0.2 | |
| Pravastatin | 0.7 | 11.4 | 27.2 | 34.6 | 25.8 | 0.3 | 0 | 0 | 0.6 | |
| Fluvastatin | 85.4 | 7.1 | 1.7 | 1.5 | 2.1 | 0.6 | 0.3 | 1.3 | 0.9 | |
| Lovastatin | 3.6 | 32.0 | 30.1 | 17.5 | 15.6 | 1.0 | 0.2 | 0.1 | 0.7 | |
| Atorvastatin | 0.7 | 11.3 | 31.5 | 37.5 | 19.0 | 0 | 0 | 0 | 0.6 | |
| Rosuvastatin | 9.7 | 38.3 | 9.5 | 7.9 | 16.5 | 3.9 | 2.4 | 11.9 | 0.6 | |
| Coronary heart disease | ||||||||||
| Control | 0 | 0 | 0 | 0 | 0 | 2.5 | 97.5 | 0 | ||
| Omega-3 | 0 | 0 | 0.1 | 1.2 | 14.8 | 83.3 | 0.7 | 0.2 | ||
| Simvastatin | 0 | 26.8 | 26.1 | 24.6 | 18.8 | 3.4 | 0.3 | 0.6 | ||
| Pravastatin | 13.3 | 31.6 | 28.0 | 17.9 | 8.8 | 0.4 | 0 | 0.7 | ||
| Lovastatin | 3.2 | 12.3 | 21.7 | 29.5 | 29.1 | 3.9 | 0.3 | 0.5 | ||
| Atorvastatin | 78.1 | 15.9 | 4.9 | 1.2 | 0 | 0 | 0 | 1 | ||
| Rosuvastatin | 5.4 | 13.5 | 19.4 | 25.6 | 28.6 | 6.4 | 1.2 | 0.5 | ||
| Myocardial infarction | ||||||||||
| Control | 0 | 0 | 0 | 0 | 0.1 | 1.4 | 18.8 | 66.5 | 13.2 | 0.1 |
| Omega-3 | 0 | 0 | 0.1 | 0.8 | 7.4 | 33.0 | 49.5 | 8.5 | 0.7 | 0.3 |
| Simvastatin | 1.0 | 3.7 | 5.8 | 10.1 | 18.0 | 29.2 | 17.4 | 11.6 | 3.3 | 0.4 |
| Pravastatin | 8.4 | 30.1 | 28.2 | 19.0 | 10.6 | 3.3 | 0.4 | 0 | 0 | 0.7 |
| Fluvastatin | 0.2 | 0.8 | 0.7 | 0.9 | 2.0 | 3.6 | 5.4 | 7.4 | 78.9 | 0.1 |
| Lovastatin | 13.3 | 32.8 | 13.5 | 12.0 | 13.4 | 9.3 | 3.7 | 1.8 | 0.3 | 0.7 |
| Atorvastatin | 2.8 | 16.0 | 30.9 | 30.9 | 16.5 | 2.7 | 0.2 | 0 | 0 | 0.7 |
| Pitavastatin | 72.7 | 6.0 | 2.9 | 2.7 | 3.5 | 3.0 | 2.1 | 4.0 | 3.6 | 0.9 |
| Rosuvastatin | 2.1 | 10.6 | 17.9 | 23.6 | 28.5 | 14.4 | 2.6 | 0.3 | 0 | 0.6 |
| Stroke | ||||||||||
| Control | 0 | 0 | 0.1 | 1.2 | 13.3 | 38.1 | 37.2 | 10.1 | 0.2 | |
| Omega-3 | 0 | 0 | 0.4 | 2.3 | 8.0 | 21.7 | 39.6 | 28.0 | 0.2 | |
| Simvastatin | 10.9 | 23.4 | 23.1 | 19.5 | 13.0 | 6.6 | 2.4 | 1.1 | 0.7 | |
| Pravastatin | 1.9 | 8.0 | 16.8 | 27.3 | 28.2 | 14.7 | 2.2 | 0.7 | 0.5 | |
| Fluvastatin | 42.2 | 8.2 | 2.9 | 2.6 | 3.4 | 3.0 | 6.1 | 31.5 | 0.6 | |
| Atorvastatin | 5.5 | 18.2 | 28.3 | 25.2 | 16.3 | 5.6 | 0.6 | 0.2 | 0.6 | |
| Pitavastatin | 25.9 | 15.5 | 4.6 | 4.7 | 5.5 | 5.2 | 10.6 | 28.0 | 0.5 | |
| Rosuvastatin | 13.5 | 26.6 | 23.7 | 17.1 | 12.3 | 5.2 | 1.2 | 0.4 | 0.7 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoang, T.; Kim, J. Comparative Effect of Statins and Omega-3 Supplementation on Cardiovascular Events: Meta-Analysis and Network Meta-Analysis of 63 Randomized Controlled Trials Including 264,516 Participants. Nutrients 2020, 12, 2218. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082218
Hoang T, Kim J. Comparative Effect of Statins and Omega-3 Supplementation on Cardiovascular Events: Meta-Analysis and Network Meta-Analysis of 63 Randomized Controlled Trials Including 264,516 Participants. Nutrients. 2020; 12(8):2218. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082218
Chicago/Turabian StyleHoang, Tung, and Jeongseon Kim. 2020. "Comparative Effect of Statins and Omega-3 Supplementation on Cardiovascular Events: Meta-Analysis and Network Meta-Analysis of 63 Randomized Controlled Trials Including 264,516 Participants" Nutrients 12, no. 8: 2218. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082218