Multicomponent Exercise Training Combined with Nutritional Counselling Improves Physical Function, Biochemical and Anthropometric Profiles in Obese Children: A Pilot Study

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
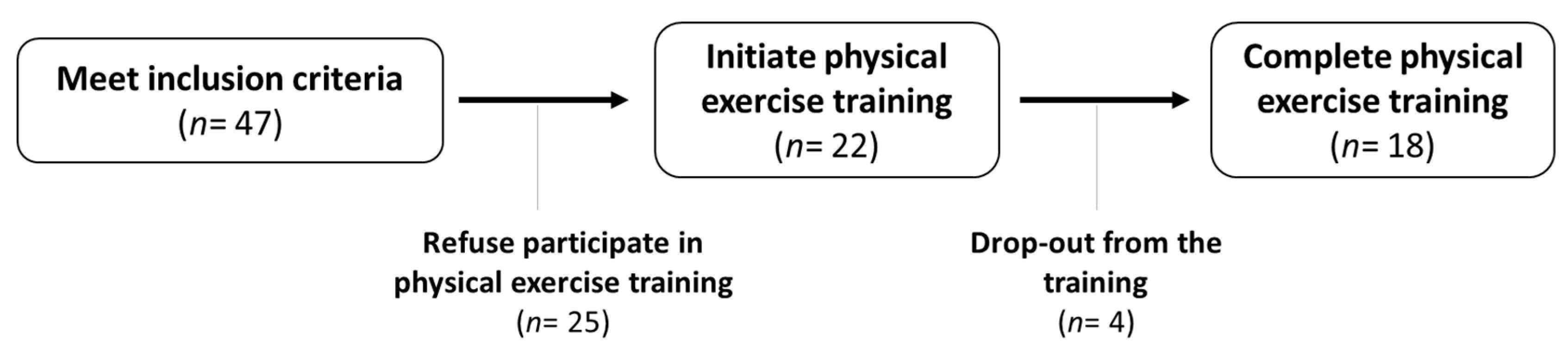
2.1. Study Design and Participants
2.2. Body Composition and Biochemical Assement
2.3. Physical Function Assement
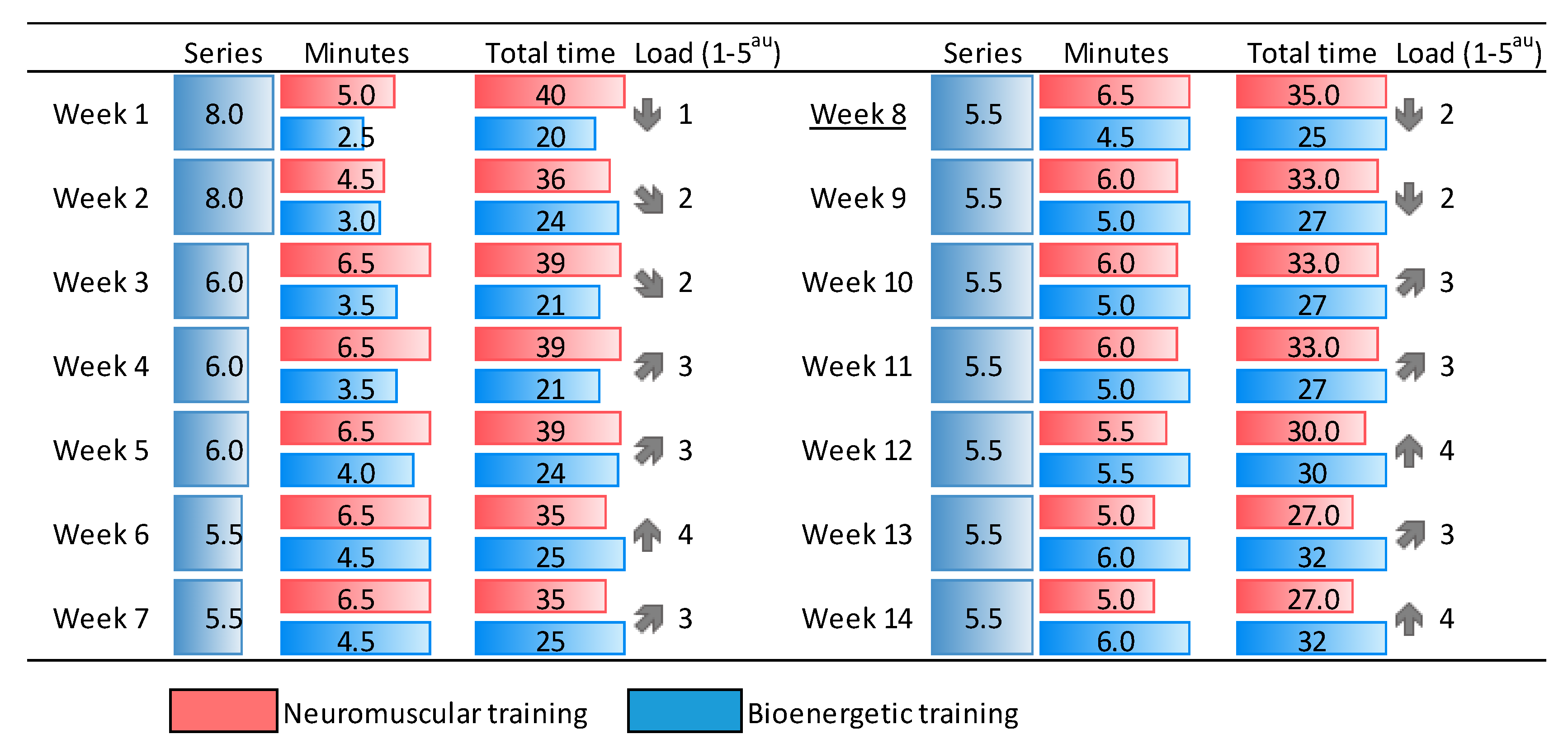
2.4. Multimodal Intervention
2.5. Statistical Analysis
3. Results
3.1. Body Composition and Biochemical Paramaters
3.2. Physical Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kumar, S.; Kelly, A.S. Review of Childhood Obesity: From Epidemiology, Etiology, and Comorbidities to Clinical Assessment and Treatment. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2017; pp. 251–265. [Google Scholar]
- Garvey, W.; Mechanick, J.; Brett, E. American College of Endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr. Pr. 2016, 22 (Suppl. S3), 1–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Global Status Report on Noncommunicable Diseases 2014; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Atay, Z.; Bereket, A. Current status on obesity in childhood and adolescence: Prevalence, etiology, co-morbidities and management. Obes. Med. 2016, 3, 1–9. [Google Scholar] [CrossRef]
- Weiss, R.; Dziura, J.; Burgert, T.S.; Tamborlane, W.V.; Taksali, S.E.; Yeckel, C.W.; Allen, K.; Lopes, M.; Savoye, M.; Morrison, J. Obesity and the metabolic syndrome in children and adolescents. N. Engl. J. Med. 2004, 350, 2362–2374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitaker, R.C.; Wright, J.A.; Pepe, M.S.; Seidel, K.D.; Dietz, W.H. Predicting obesity in young adulthood from childhood and parental obesity. N. Engl. J. Med. 1997, 337, 869–873. [Google Scholar] [CrossRef] [PubMed]
- WHO. Report of the Commission on Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Kelley, G.A.; Kelley, K.S.; Pate, R.R. Exercise and adiposity in overweight and obese children and adolescents: A systematic review with network meta-analysis of randomised trials. BMJ Open 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Corrêa Marson, E.; Sudatti Delevatti, R.; Konig Garcia-Prado, A.; Netto, N.; Martins Kruel, L.F. Effects of aerobic, resistance, and combined exercise training on insulin resistance markers in overweight or obese children and adolescents: A systematic review and meta-analysis. Prev. Med. 2016, 93, 211–218. [Google Scholar] [CrossRef]
- 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; US Department of Health and Human Services: Washington, DC, USA, 2018; p. 779.
- Del Valle Soto, M.; Marqueta, P.M.; De Teresa Galván, C.; Bonafonte, L.F.; Luengo, E.; Aurrekoetxea, T.G. Prescripción de ejercicio físico en la prevención y tratamiento de la hipertensión arterial. Documento de Consenso de la Sociedad Española de Medicina del Deporte (SEMED-FEMEDE). Arch. Med. Deporte Rev. Fed. Española Med. Deporte Confed. Iberoam. Med. Deporte 2015, 32, 281–313. [Google Scholar]
- Reed, J.L.; Pipe, A.L. Practical approaches to prescribing physical activity and monitoring exercise intensity. Can. J. Cardiol. 2016, 32, 514–522. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- Myers, J.; Kokkinos, P.; Nyelin, E. Physical activity, cardiorespiratory fitness, and the metabolic syndrome. Nutrients 2019, 11, 1652. [Google Scholar] [CrossRef] [Green Version]
- Son, W.-M.; Sung, K.-D.; Bharath, L.P.; Choi, K.-J.; Park, S.-Y. Combined exercise training reduces blood pressure, arterial stiffness, and insulin resistance in obese prehypertensive adolescent girls. Clin. Exp. Hypertens. 2017, 39, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Sanchez-Gonzalez, M.A.; Son, W.-M.; Kwak, Y.-S.; Park, S.-Y. The effects of a 12-week combined exercise training program on arterial stiffness, vasoactive substances, inflammatory markers, metabolic profile, and body composition in obese adolescent girls. Pediatr. Exerc. Sci. 2018, 30, 480–486. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Xie, G.; Wang, J.; Yang, S. Cardiovascular risk factors significantly correlate with autonomic nervous system activity in children. Can. J. Cardiol. 2012, 28, 477–482. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine and the American Diabetes Association: Joint position statement. Exercise and type 2 diabetes. Med. Sci. Sports Exerc. 2010, 42, 2282–2303. [CrossRef] [PubMed]
- Barrow, D.R.; Abbate, L.M.; Paquette, M.R.; Driban, J.B.; Vincent, H.K.; Newman, C.; Messier, S.P.; Ambrose, K.R.; Shultz, S. Exercise prescription for weight management in obese adults at risk for osteoarthritis: Synthesis from a systematic review. BMC Musculoskelet. Dis. 2019, 20, 610. [Google Scholar] [CrossRef] [Green Version]
- Chiu, C.-H.; Ko, M.-C.; Wu, L.-S.; Yeh, D.-P.; Kan, N.-W.; Lee, P.-F.; Hsieh, J.-W.; Tseng, C.-Y.; Ho, C.-C. Benefits of different intensity of aerobic exercise in modulating body composition among obese young adults: A pilot randomized controlled trial. Health Qual. Life Outcomes 2017, 15, 168. [Google Scholar] [CrossRef]
- Alves, A.S.R.; Venancio, T.L.; Honorio, S.A.A.; Martins, J.; Manuel, C. Multicomponent training with different frequencies on body composition and physical fitness in obese children. An. Acad. Bras. Ciênc. 2019, 91. [Google Scholar] [CrossRef]
- Cox, C.E. Role of physical activity for weight loss and weight maintenance. Diabetes Spectr. 2017, 30, 157–160. [Google Scholar] [CrossRef] [Green Version]
- ACSM; Riebe, D.; Ehrman, K.J.; Liguori, G.; Magal, M. Benefits and Risks Associated with Physical Activity. In ACSM’s Exercise Testing and Prescription, 10th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2017. [Google Scholar]
- Doak, C.; Visscher, T.; Renders, C.; Seidell, J. The prevention of overweight and obesity in children and adolescents: A review of interventions and programmes. Obes. Rev. 2006, 7, 111–136. [Google Scholar] [CrossRef]
- García-Hermoso, A.; Ramírez-Vélez, R.; Saavedra, J.M. Exercise, health outcomes, and pædiatric obesity: A systematic review of meta-analyses. J. Sci. Med. Sport 2019, 22, 76–84. [Google Scholar] [CrossRef]
- Stoner, L.; Rowlands, D.; Morrison, A.; Credeur, D.; Hamlin, M.; Gaffney, K.; Lambrick, D.; Matheson, A. Efficacy of Exercise Intervention for Weight Loss in Overweight and Obese Adolescents: Meta-Analysis and Implications. Sports Med. 2016, 46, 1737–1751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoelscher, D.M.; Kirk, S.; Ritchie, L.; Cunningham-Sabo, L.; Committee, A.P. Position of the Academy of Nutrition and Dietetics: Interventions for the prevention and treatment of pediatric overweight and obesity. J. Acad. Nutr. Diet. 2013, 113, 1375–1394. [Google Scholar] [CrossRef] [PubMed]
- Pfeifflé, S.; Pellegrino, F.; Kruseman, M.; Pijollet, C.; Volery, M.; Soguel, L.; Bucher Della Torre, S. Current recommendations for nutritional management of overweight and obesity in children and adolescents: A structured framework. Nutrients 2019, 11, 362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bluford, D.A.; Sherry, B.; Scanlon, K.S. Interventions to prevent or treat obesity in preschool children: A review of evaluated programs. Obesity 2007, 15, 1356–1372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ells, L.J.; Rees, K.; Brown, T.; Mead, E.; Al-Khudairy, L.; Azevedo, L.; McGeechan, G.J.; Baur, L.; Loveman, E.; Clements, H. Interventions for treating children and adolescents with overweight and obesity: An overview of Cochrane reviews. Int. J. Obes. (2005) 2018, 42, 1823–1833. [Google Scholar] [CrossRef] [Green Version]
- Morano, M.; Rutigliano, I.; Rago, A.; Pettoello-Mantovani, M.; Campanozzi, A. A multicomponent, school-initiated obesity intervention to promote healthy lifestyles in children. Nutr. Diabetes 2016, 32, 1075–1080. [Google Scholar] [CrossRef]
- WHO. Growth Reference Data for 5–19 Years; WHO Geneva: Geneva, Switzerland, 2007. [Google Scholar]
- Frisancho, R. New norms for upper limb fat and mass area forassessment for nutritional status. Am. J. Clin. Nutr. 1981, 34, 2540–2545. [Google Scholar] [CrossRef]
- McCarthy, H.; Jarrett, K.; Crawley, H. The development of waist circumference percentiles in British children aged 5.0–16.9 y. Eur. J. Clin. Nutr. 2001, 55, 902–907. [Google Scholar] [CrossRef] [Green Version]
- Slaughter, M.H.; Lohman, T.G.; Boileau, R.; Horswill, C.; Stillman, R.; Van Loan, M.; Bemben, D. Skinfold equations for estimation of body fatness in children and youth. Hum. Biol. 1988, 60, 709–723. [Google Scholar]
- Buckinx, F.; Landi, F.; Cesari, M.; Fieding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S. The Authors reply: “Dual energy X-ray absorptiometry: Gold standard for muscle mass?” by Scafoglieri et al. J. Cachexia Sarcopenia Muscle 2018, 9, 788. [Google Scholar] [CrossRef]
- Scafoglieri, A.; Clarys, J.P. Dual energy X-ray absorptiometry: Gold standard for muscle mass? J. Cachexia Sarcopenia Muscle 2018, 9, 786. [Google Scholar] [CrossRef] [PubMed]
- Nana, A.; Slater, G.J.; Hopkins, W.G.; Burke, L.M. Effects of daily activities on dual-energy X-ray absorptiometry measurements of body composition in active people. Med. Sci. Sports Exerc. 2012, 44, 180–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, F.; Artero, E.; Ruiz, J.; Vicente-Rodriguez, G.; Bergman, P.; Hagströmer, M.; Ottevaere, C.; Nagy, E.; Konsta, O.; Rey-López, J.; et al. Reliability of health-related physical fitness tests in European adolescents. The HELENA Study. Int. J. Obes. 2008, 32, S49–S57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, G.; Burton, L.; Hoogenboom, B.J.; Voight, M. Functional movement screening: The use of fundamental movements as an assessment of function-part 1. Int. J. Sports Phys. Ther. 2014, 9, 396–409. [Google Scholar]
- Cook, G.; Burton, L.; Hoogenboom, B.J.; Voight, M. Functional movement screening: The use of fundamental movements as an assessment of function-part 2. Int. J. Sports Phys. Ther. 2014, 9, 549–563. [Google Scholar]
- Molina-Garcia, P.; Migueles, J.; Cadenas-Sanchez, C.; Esteban-Cornejo, I.; Mora-Gonzalez, J.; Rodriguez-Ayllon, M.; Plaza-Florido, A.; Molina-Molina, A.; Garcia-Delgado, G.; D’Hondt, E.; et al. Fatness and fitness in relation to functional movement quality in overweight and obese children. J. Sports Sci. 2019, 37, 878–885. [Google Scholar] [CrossRef]
- Duncan, M.; Stanley, M.; Wright, S. The association between functional movement and overweight and obesity in British primary school children. BMC Sports Sci. Med. Rehabil. 2013, 5, 11. [Google Scholar] [CrossRef] [Green Version]
- Graham, M.; Bush, J.; Olvera, N.; Puyau, M.; Butte, N. Effectiveness of the modified progressive aerobic capacity endurance run test for assessing aerobic fitness in Hispanic children who are obese. J. Strength Cond. Res. 2014, 28, 2880–2887. [Google Scholar] [CrossRef]
- De Onis, M.; Martínez-Costa, C.; Núnez, F.; Nguefack-Tsague, G.; Montal, A.; Brines, J. Association between WHO cut-offs for childhood overweight and obesity and cardiometabolic risk. Public Health Nutr. 2013, 16, 625–630. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Costa, C.; Nunez, F.; Montal, A.; Brines, J. Relationship between childhood obesity cut-offs and metabolic and vascular comorbidities: Comparative analysis of three growth standards. J. Hum. Nutr. Diet. 2014, 27, 75–83. [Google Scholar] [CrossRef]
- Atlantis, E.; Barnes, E.; Singh, M.F. Efficacy of exercise for treating overweight in children and adolescents: A systematic review. Int. J. Obes. 2006, 30, 1027–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinehr, T.; Lass, N.; Toschke, C.; Rothermel, J.; Lanzinger, S.; Holl, R.W. Which amount of BMI-SDS reduction is necessary to improve cardiovascular risk factors in overweight children? J. Clin. Endocrinol. Metab. Clin. Exp. 2016, 101, 3171–3179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calcaterra, V.; Larizza, D.; Codrons, E.; De Silvestri, A.; Brambilla, P.; Abela, S.; Arpesella, M.; Vandoni, M. Improved metabolic and cardiorespiratory fitness during a recreational training program in obese children. J. Pediatr. Endocrinol. Metab. Clin. Exp. 2013, 26, 271–276. [Google Scholar] [CrossRef] [PubMed]
- González-Gil, E.; Gracia-Marco, L.; Santabárbara, J.; Molnar, D.; Amaro-Gahete, F.J.; Gottrand, F.; Arouca, A.; Kafatos, A.; Widhalm, K.; Manios, Y. Inflammation and insulin resistance according to body composition in European adolescents: The HELENA study. Nutr. Hosp. 2017, 34, 1033–1043. [Google Scholar] [CrossRef]
- González-Gil, E.; Santabarbara, J.; Ruiz, J.; Bel-Serrat, S.; Huybrechts, I.; Pedrero-Chamizo, R.; Gottrand, F.; Kafatos, A.; Widhalm, K.; Manios, Y. Ideal cardiovascular health and inflammation in European adolescents: The HELENA study. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 447–455. [Google Scholar] [CrossRef] [Green Version]
- García-Hermoso, A.; Cerrillo-Urbina, A.; Herrera-Valenzuela, T.; Cristi-Montero, C.; Saavedra, J.; Martínez-Vizcaíno, V. Is high-intensity interval training more effective on improving cardiometabolic risk and aerobic capacity than other forms of exercise in overweight and obese youth? A meta-analysis. Obes. Rev. 2016, 17, 531–540. [Google Scholar] [CrossRef]
- Lavelle, H.; Mackay, D.; Pell, J. Systematic review and meta-analysis of school-based interventions to reduce body mass index. J. Public Health 2012, 34, 360–369. [Google Scholar] [CrossRef] [Green Version]
- Gutin, B.; Litaker, M.; Islam, S.; Manos, T.; Smith, C.; Treiber, F. Body-composition measurement in 9–11-y-old children by dual-energy X-ray absorptiometry, skinfold-thickness measurements, and bioimpedance analysis. Am. J. Clin. Nutr. 1996, 63, 287–292. [Google Scholar] [CrossRef] [Green Version]
- Ellis, K. Measuring body fatness in children and young adults: Comparison of bioelectric impedance analysis, total body electrical conductivity, and dual-energy X-ray absorptiometry. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 1996, 20, 866. [Google Scholar]
- González-Ruiz, K.; Ramirez-Velez, R.; Correa-Bautista, J.E.; Peterson, M.D.; García-Hermoso, A. The effects of exercise on abdominal fat and liver enzymes in pediatric obesity: A systematic review and meta-analysis. Child. Obes. 2017, 13, 272–282. [Google Scholar] [CrossRef]
- Maffeis, C.; Morandi, A. Body composition and insulin resistance in children. Eur. J. Clin. Nutr. 2018, 72, 1239–1245. [Google Scholar] [PubMed]
- Lo, K.; Wong, M.; Khalechelvam, P.; Tam, W. Waist-to-height ratio, body mass index and waist circumference for screening paediatric cardio-metabolic risk factors: A meta-analysis. Obes. Rev. 2016, 17, 1258–1275. [Google Scholar] [CrossRef] [PubMed]
- Saris, W.; Blair, S.; van Baak, M.; Eaton, S.; Davies, P.; Di Pietro, L.; Fogelholm, M.; Rissanen, A.; Schoeller, D.; Swinburn, B.; et al. How much physical activity is enough to prevent un-healthy weight gain? Outcome of the IASO 1st Stock Conferenceand consensus statement. Obes. Rev. 2003, 4, 101–114. [Google Scholar] [PubMed]
- Daniels, S.; Arnett, D.; Eckel, R.; Gidding, S.; Hayman, L.; Kumanyika, S.; Robinson, T.; Scott, B.; Jeor, S.; Williams, C. Overweight in children and adolescents: Pathophysiology, consequences, prevention, and treatment. Circulation 2005, 111, 1999–2012. [Google Scholar] [PubMed] [Green Version]
- Sinaiko, A.R.; Steinberger, J.; Moran, A.; Hong, C.-P.; Prineas, R.J.; Jacobs, D.R., Jr. Influence of insulin resistance and body mass index at age 13 on systolic blood pressure, triglycerides, and high-density lipoprotein cholesterol at age 19. Hypertension 2006, 48, 730–736. [Google Scholar]
- Yajnik, C.S.; Katre, P.A.; Joshi, S.M.; Kumaran, K.; Bhat, D.S.; Lubree, H.G.; Memane, N.; Kinare, A.S.; Pandit, A.N.; Bhave, S.A. Higher glucose, insulin and insulin resistance (HOMA-IR) in childhood predict adverse cardiovascular risk in early adulthood: The Pune Children’s Study. Diabetologia 2015, 58, 1626–1636. [Google Scholar] [CrossRef] [Green Version]
- Morano, M.; Colella, D.; Rutigliano, I.; Fiore, P.; Pettoello-Mantovani, M.; Campanozzi, A. Changes in actual and perceived physical abilities in clinically obese children: A 9-month multi-component intervention study. PLoS ONE 2012, 7, e50782. [Google Scholar] [CrossRef] [Green Version]
- Watson, L.A.; Baker, M.C.; Chadwick, P.M. Kids just wanna have fun: Children’s experiences of a weight management programme. Br. J. Health Psychol. 2016, 21, 407–420. [Google Scholar] [CrossRef]
- Gråstén, A.; Yli-Piipari, S. The Patterns of Moderate to Vigorous Physical Activity and Physical Education Enjoyment Through a 2-Year School-Based Program. J. School Health 2019, 89, 88–98. [Google Scholar] [CrossRef]
- Saavedra, J.M.; García-Hermoso, A.; Escalante, Y.; Domínguez, A.M. Self-determined motivation, physical exercise and diet in obese children: A three-year follow-up study. Int. J. Clin. Health Psychol. Rev. 2014, 14, 195–201. [Google Scholar] [CrossRef] [Green Version]
- Han, A.; Fu, A.; Cobley, S.; Sanders, R.H. Effectiveness of exercise intervention on improving fundamental movement skills and motor coordination in overweight/obese children and adolescents: A systematic review. J. Sci. Med. Sport 2018, 21, 89–102. [Google Scholar] [CrossRef] [PubMed]
- Julian, V.; Thivel, D.; Miguet, M.; Pereira, B.; Costes, F.; Coudeyre, E.; Duclos, M.; Richard, R. Eccentric cycling is more efficient in reducing fat mass than concentric cycling in adolescents with obesity. Scand. J. Med. Sci. Sports 2019, 29, 4–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Johansson, L.; Brissman, M.; Morinder, G.; Westerståhl, M.; Marcus, C. Reference values and secular trends for cardiorespiratory fitness in children and adolescents with obesity. Acta Paediatr. 2020, 1665–1671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pienaar, A.; Du Toit, D.; Truter, L. The effect of a multidisciplinary physical activity intervention on the body composition and physical fitness of obese children. J. Sports Med. Phys. Fit. 2013, 53, 415–427. [Google Scholar]
- De Miguel-Etayo, P.; Gracia-Marco, L.; Ortega, F.; Intemann, T.; Foraita, R.; Lissner, L.; Oja, L.; Barba, G.; Michels, N.; Tornaritis, M. Physical fitness reference standards in European children: The IDEFICS study. Int. J. Obes. 2014, 38, S57–S66. [Google Scholar] [CrossRef] [Green Version]
- Abraham, A.; Sannasi, R.; Nair, R. Normative values for the Funtional Movement Screen in adolescent school aged children. Int. J. Sports Phys. Ther. 2015, 10, 29–36. [Google Scholar]
- García-Hermoso, A.; Saavedra, J.M.; Escalante, Y.; Domínguez, A.M. Effects of a long-term physical exercise program with and without diet on obese boys after six-month detraining. World J. Pediatr. 2014, 10, 38–45. [Google Scholar] [CrossRef]
- Aikenhead, A.; Knai, C.; Lobstein, T. Do Surgical Interventions to Treat Obesity in Children and Adolescents Have Long-Versus Short-Term Advantages and Are They Cost-Effective; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]



{kind=link}
{kind=link}
| Participants (n = 22) | Baseline | |
|---|---|---|
| Age (years) | 10.9 (1.7) (Range 8–14) | |
| Gender (%) | Female | n = 13 (59%) |
| Male | n = 9 (41%) | |
| Tanner stage (%) | Prepubertal | n = 11 (50%) |
| Pubertal | n = 11 (50%) | |
| Baseline | Post-Intervention | p Value | |
|---|---|---|---|
| z BMI | 3 (0.4) | 2.7 (0.4) | <0.001 |
| z WC | 6.8 (1.4) | 6.3 (1.2) | <0.05 a |
| z MUAC | 3.4 (1) | 3 (0.9) | <0.01 |
| z TRI | 3 (0.8) | 2.4 (0.7) | <0.001 |
| z SUB | 3.7 (0.8) | 3.2 (1.1) | <0.01 |
| WHtR | 0.64 (0.04) | 0.61 (0.03) | <0.001 |
| Body fat (Slaughter, %) | 44.6 (6.9) | 40.7 (5.5) | <0.001 b |
| Body fat (DXA, %) | 46 (4.4) | 43.6 (4.6) | <0.001 |
| Trunk fat (DXA, %) | 45.3 (4.4) | 42.6 (5.1) | <0.01 |
| Baseline | Post-Intervention | p Value | d | |
|---|---|---|---|---|
| Cholesterol (mg/dL) (n = 17) | 165 (34) | 157 (31) | Ns | −0.25 |
| HDL-C (mg/dL) (n = 17) | 50 (10) | 49 (14) | Ns a | −0.08 |
| LDL-C (mg/dL) (n = 17) | 108 (27) | 100 (24) | <0.05 | −0.31 |
| Triglycerides (mg/dL) (n = 17) | 79 (36) | 84 (47) | Ns | 0.12 |
| Uric acid (mg/dL) (n = 16) | 4.9 (1.2) | 4.9 (1.5) | Ns | 0 |
| GGT (U/L) (n = 15) | 23 (12) | 18 (8.2) | <0.01 | −0.49 |
| ALT (U/L) (n = 18) | 25 (12) | 21 (9) | <0.05 | −0.38 |
| Glycated hemoglobin (%) (n = 14) | 5.3 (0.1) | 5.3 (0.2) | Ns | 0 |
| C-reactive protein (mg/dL) (n = 16) | 4 (3.2) | 2.2 (1.9) | <0.05 | −0.68 |
| Glucose (mg/dL) (n = 17) | 95 (6) | 94 (6) | Ns | −0.17 |
| Insulin (µU/mL) (n = 17) | 24 (17) | 20 (8) | Ns a | −0.3 |
| HOMA-IR (n = 17) | 5.6 (3.9) | 4.6 (2.1) | <0.05 a | −0.32 |
| Baseline | Post-Intervention | p-Value | d | |
|---|---|---|---|---|
| Handgrip_right (kg) | 23.13 (4.98) | 23.89 (5.47) | Ns | 0.15 |
| Handgrip_left (kg) | 20.44 (5.54) | 20.36 (7) | Ns | −0.01 |
| Broad jump (cm) (n = 17) | 124.73 (16.58) | 126.5 (13.81) | Ns | 0.12 |
| mPACER test (laps) (n = 16) | 18.81 (3.6) | 23.81 (6.35) | 0.003 | 0.97 |
| mPACER test (km/h) (n = 16) | 8.47 (0.62) | 8.94 (0.4) | 0.006 | 0.9 |
| FMS_7 (n = 17) | 8.76 (1.82) | 10.7 (2.28) | <0.001 | 0.94 |
| FMS_4 (n = 17) | 5.35 (1.58) | 6.94 (1.44) | <0.001 | 1.05 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cordellat, A.; Padilla, B.; Grattarola, P.; García-Lucerga, C.; Crehuá-Gaudiza, E.; Núñez, F.; Martínez-Costa, C.; Blasco-Lafarga, C. Multicomponent Exercise Training Combined with Nutritional Counselling Improves Physical Function, Biochemical and Anthropometric Profiles in Obese Children: A Pilot Study. Nutrients 2020, 12, 2723. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092723
Cordellat A, Padilla B, Grattarola P, García-Lucerga C, Crehuá-Gaudiza E, Núñez F, Martínez-Costa C, Blasco-Lafarga C. Multicomponent Exercise Training Combined with Nutritional Counselling Improves Physical Function, Biochemical and Anthropometric Profiles in Obese Children: A Pilot Study. Nutrients. 2020; 12(9):2723. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092723
Chicago/Turabian StyleCordellat, Ana, Beatriz Padilla, Paula Grattarola, Consolación García-Lucerga, Elena Crehuá-Gaudiza, Francisco Núñez, Cecilia Martínez-Costa, and Cristina Blasco-Lafarga. 2020. "Multicomponent Exercise Training Combined with Nutritional Counselling Improves Physical Function, Biochemical and Anthropometric Profiles in Obese Children: A Pilot Study" Nutrients 12, no. 9: 2723. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092723