Creatine Supply Attenuates Ischemia-Reperfusion Injury in Lung Transplantation in Rats

 , ,
, ,  and
and
Abstract
:1. Introduction
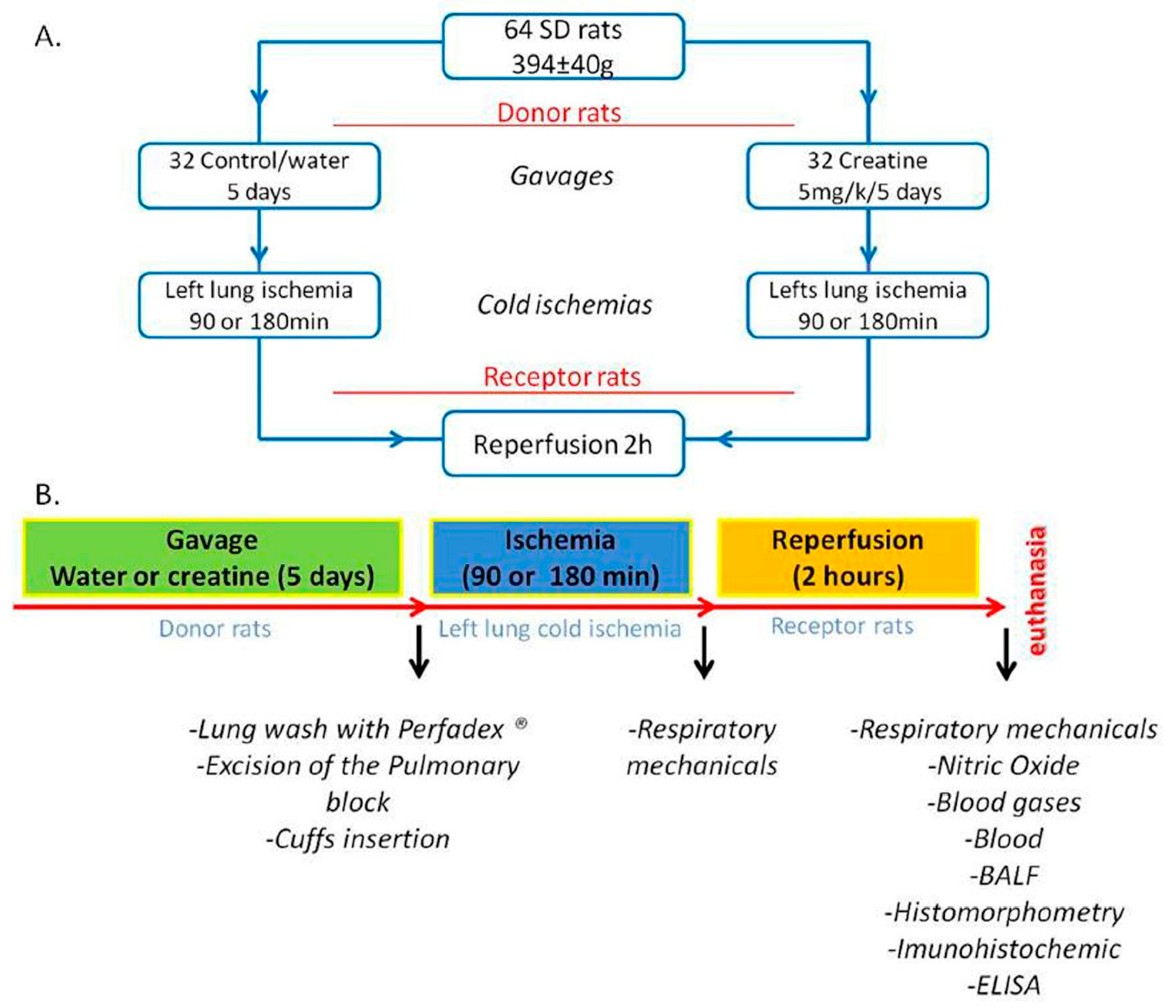
2. Materials and Methods
2.1. Animals
2.2. Groups
2.3. Creatine Supplementation
2.4. Surgical Procedures
2.5. Respiratory Mechanics
2.6. Exhaled Nitric Oxide (NOex)
2.7. Blood Gases
2.8. Peripheral Blood Cell Count and Euthanasia
2.9. Bronchoalveolar Lavage Fluid (BALF) and Inflammatory Mediators
2.10. Histomorphometric and Immunohistochemistry Study
2.11. Statistical Analysis
3. Results
3.1. Respiratory Mechanics
3.2. NOex Concentration
3.3. Creatinine and Blood Gas Concentration
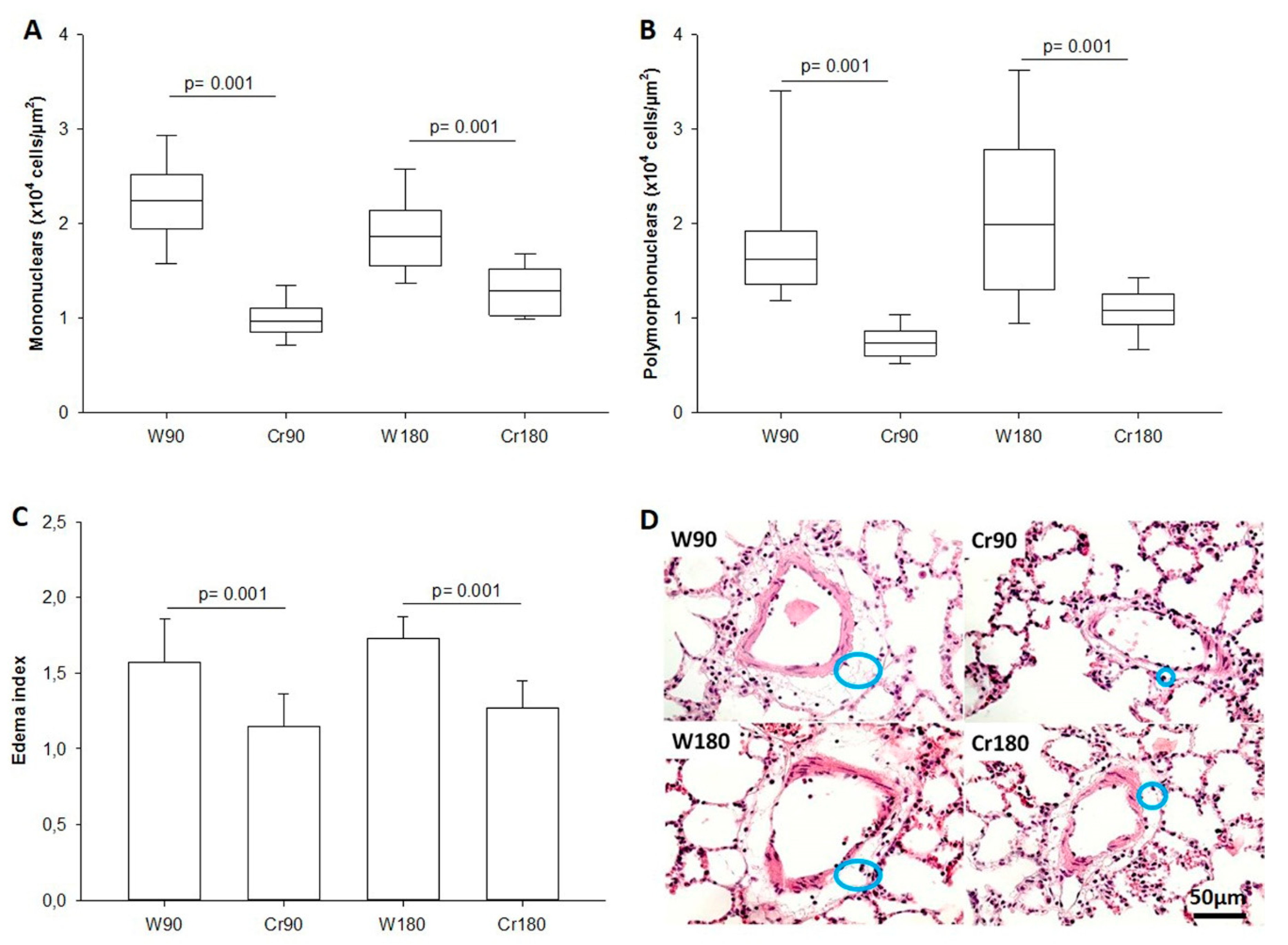
3.4. Inflammatory Cells in the Peripheral Blood and BALF
3.5. Lung Parenchyma Inflammation and Edema Index
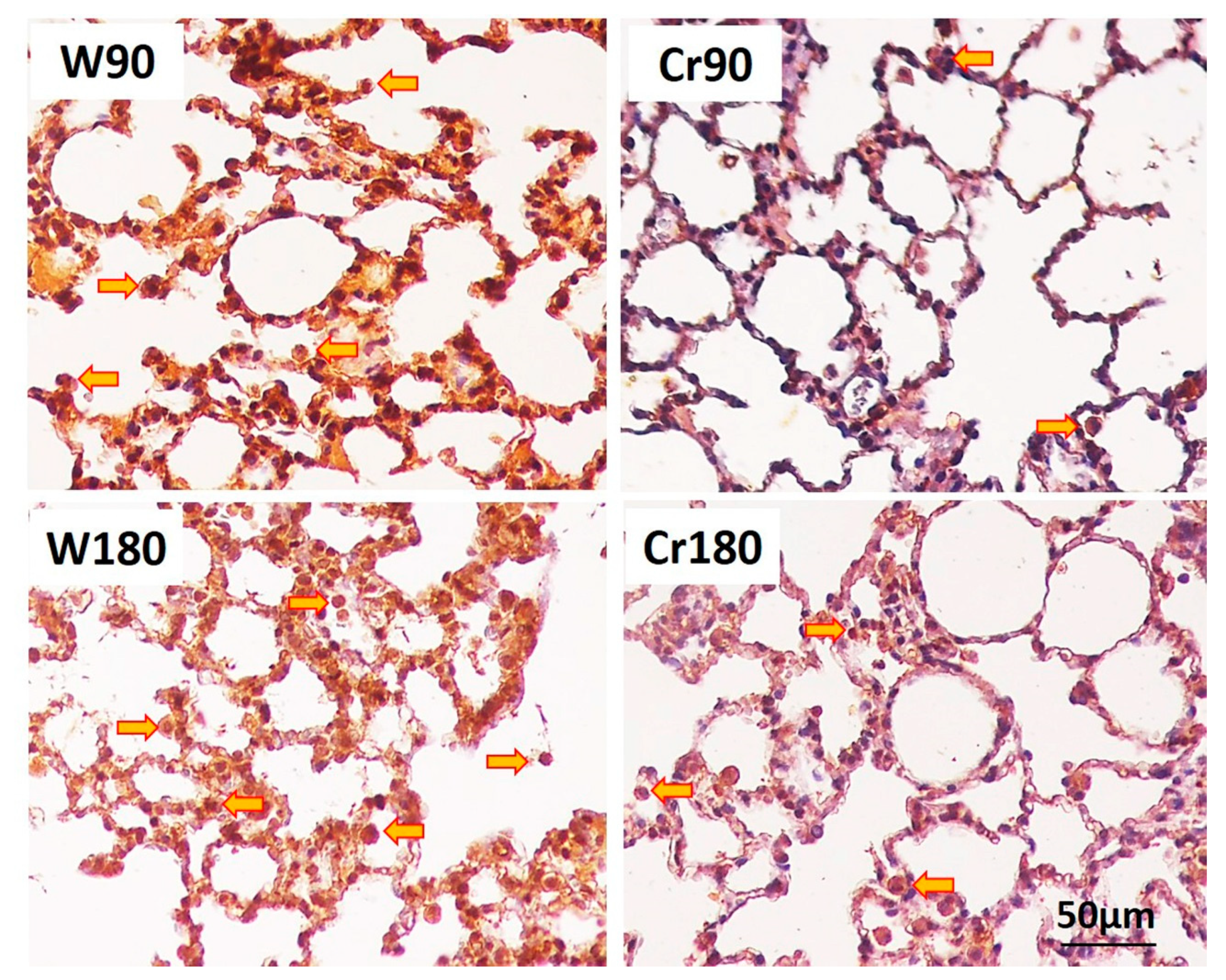
3.6. Proliferation, Apoptosis, and Immune Response
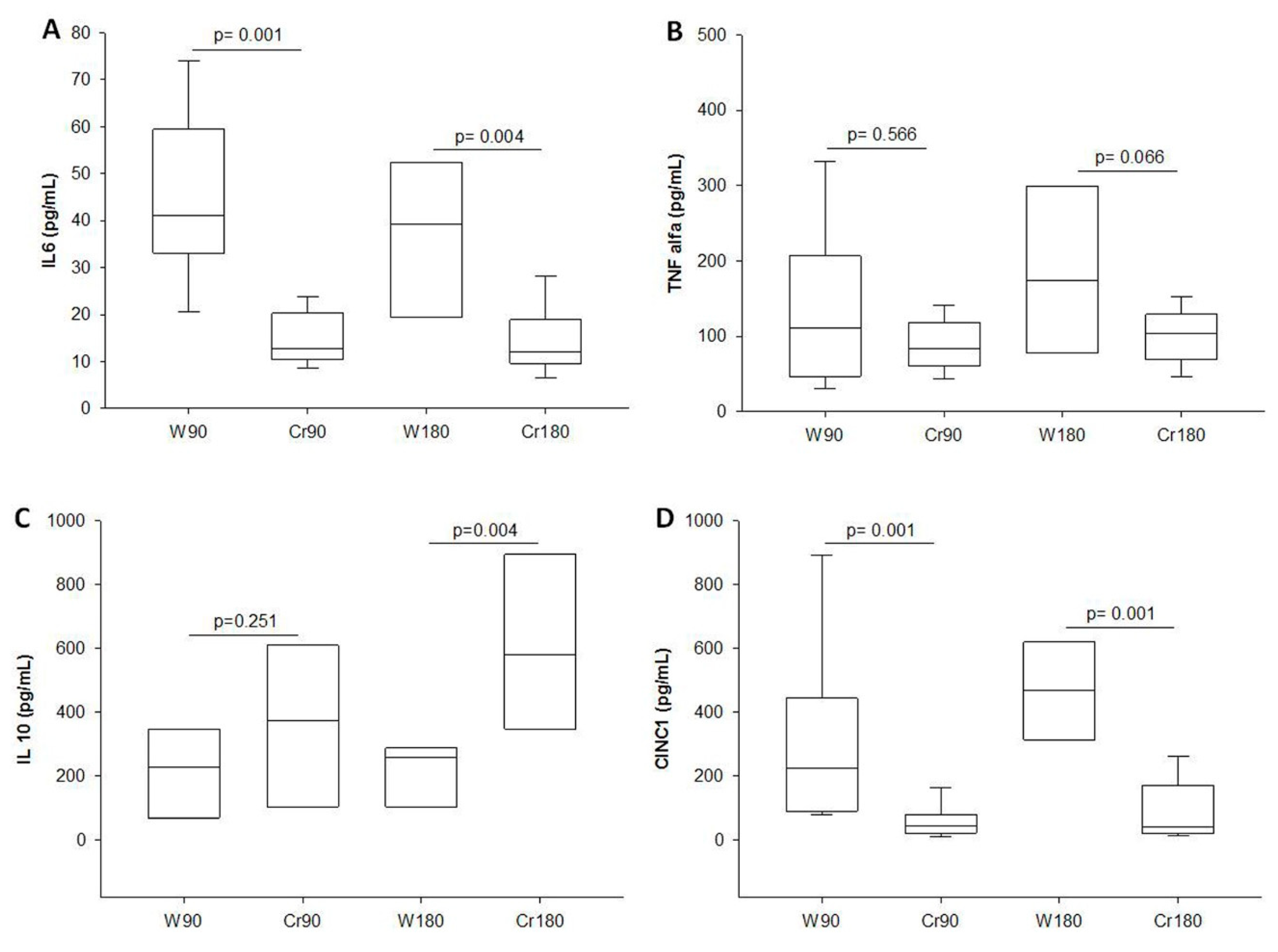
3.7. Levels of Inflammatory Mediators in BALF
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| W 90 Mean (±SD) | Cr 90 Mean (±SD) | p | W 180 Mean (±SD) | Cr 180 Mean (±SD) | p | |
|---|---|---|---|---|---|---|
| Plasma Creatinine (mg/dL) | 0.37 (±0.04) | 0.58 (±0.08) | 0.002 * | 0.39 (±0.02) | 0.54 (±0.17) | 0.008 * |
| Lung mechanics | ||||||
| RAW (cmH2O.s/mL) | 0.084 (±0.02) | 0.071 (±0.02) | 0.129 | 0.083 (±0.02) | 0.080 (±0.01) | 0.463 |
| GTIS (cmH2O/mL) | 0.234 (±0.04) | 0.209 (±0.04) | 0.123 | 0.194 (±0.05) | 0.215 (±0.03) | 0.242 |
| HTIS (cmH2O/mL) | 1.442 (±0.15) | 1.359 (±0.09) | 0.192 | 1.440 (±0.09) | 1.367 (±0.09) | 0.062 |
References
- Simonneau, G.; Gatzoulis, M.A.; Adatia, I.; Celermajer, D.; Denton, C.; Ghofrani, A.; Gomez Sanchez, M.A.; Krishna Kumar, R.; Landzberg, M.; Machado, R.F.; et al. Updated clinical classification of pulmonary hypertension. J. Am. Coll. Cardiol. 2013, 62, D34–D41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E., Jr.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef] [PubMed]
- Yusen, R.D.; Edwards, L.B.; Dipchand, A.I.; Goldfarb, S.B.; Kucheryavaya, A.Y.; Levvey, B.J.; Lund, L.H.; Meiser, B.; Rossano, J.W.; Stehlik, J. The Registry of the International Society for Heart and Lung Transplantation: Thirty-third Adult Lung and Heart-Lung Transplant Report-2016; Focus Theme: Primary Diagnostic Indications for Transplant. J. Heart Lung Transplant. 2016, 35, 1170–1184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laubach, V.E.; Sharma, A.K. Mechanisms of lung ischemia-reperfusion injury. Curr. Opin. Organ. Transplant. 2016, 21, 246–252. [Google Scholar] [CrossRef] [Green Version]
- Zhao, G.; Al-Mehdi, A.B.; Fisher, A.B. Anoxia-reoxygenation versus ischemia in isolated rat lungs. Am. J. Physiol. 1997, 273, L1112–L1117. [Google Scholar] [CrossRef]
- Inci, I.; Zhai, W.; Arni, S.; Hillinger, S.; Vogt, P.; Weder, W. N-acetylcysteine attenuates lung ischemia-reperfusion injury after lung transplantation. Ann. Thorac. Surg. 2007, 84, 240–246, discussion 246. [Google Scholar] [CrossRef]
- Lawler, J.M.; Barnes, W.S.; Wu, G.; Song, W.; Demaree, S. Direct antioxidant properties of creatine. Biochem. Biophys. Res. Commun. 2002, 290, 47–52. [Google Scholar] [CrossRef]
- Almeida, F.M.; Oliveira-Junior, M.C.; Souza, R.A.; Petroni, R.C.; Soto, S.F.; Soriano, F.G.; Carvalho, P.T.; Albertini, R.; Damaceno-Rodrigues, N.R.; Lopes, F.D.; et al. Creatine supplementation attenuates pulmonary and systemic effects of lung ischemia and reperfusion injury. J. Heart Lung Transplant. 2016, 35, 242–250. [Google Scholar] [CrossRef]
- Balestrino, M.; Sarocchi, M.; Adriano, E.; Spallarossa, P. Potential of creatine or phosphocreatine supplementation in cerebrovascular disease and in ischemic heart disease. Amino Acids 2016, 48, 1955–1967. [Google Scholar] [CrossRef]
- Wyss, M.; Kaddurah-Daouk, R. Creatine and creatinine metabolism. Physiol. Rev. 2000, 80, 1107–1213. [Google Scholar] [CrossRef]
- Vieira, R.P.; Duarte, A.C.; Claudino, R.C.; Perini, A.; Santos, A.B.; Moriya, H.T.; Arantes-Costa, F.M.; Martins, M.A.; Carvalho, C.R.; Dolhnikoff, M. Creatine supplementation exacerbates allergic lung inflammation and airway remodeling in mice. Am. J. Respir. Cell Mol. Biol. 2007, 37, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Vieira, R.P.; Duarte, A.C.; Santos, A.B.; Medeiros, M.C.; Mauad, T.; Martins, M.A.; Carvalho, C.R.; Dolhnikoff, M. Exercise reduces effects of creatine on lung. Int. J. Sports Med. 2009, 30, 684–690. [Google Scholar] [CrossRef] [PubMed]
- Abreu, M.M.; Pazetti, R.; Almeida, F.M.; Correia, A.T.; Parra, E.R.; Silva, L.P.; Vieira, R.P.; Pego-Fernandes, P.M.; Jatene, F.B. Methylene blue attenuates ischemia--reperfusion injury in lung transplantation. J. Surg. Res. 2014, 192, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Xavier, A.M.; Pego-Fernandes, P.M.; Correia, A.T.; Pazetti, R.; Monteiro, R.; Canzian, M.; Jatene, F.B. Influence of cyclosporine A on mucociliary system after lung transplantation in rats. Acta Cir. Bras. 2007, 22, 465–469. [Google Scholar] [CrossRef] [Green Version]
- Hantos, Z.; Adamicza, A.; Govaerts, E.; Daroczy, B. Mechanical impedances of lungs and chest wall in the cat. J. Appl. Physiol. 1992, 73, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Almeida, F.M.; Saraiva-Romanholo, B.M.; Vieira, R.P.; Moriya, H.T.; Ligeiro-de-Oliveira, A.P.; Lopes, F.D.; Castro-Faria-Neto, H.C.; Mauad, T.; Martins, M.A.; Pazetti, R. Compensatory lung growth after bilobectomy in emphysematous rats. PLoS ONE 2017, 12, e0181819. [Google Scholar] [CrossRef]
- Ellington, W.R. Phosphocreatine represents a thermodynamic and functional improvement over other musclephosphagens. J. Exp. Biol. 1989, 143, 177–194. [Google Scholar]
- Kitzenberg, D.; Colgan, S.P.; Glover, L.E. Creatine kinase in ischemic and inflammatory disorders. Clin. Transl. Med. 2016, 5, 31. [Google Scholar] [CrossRef] [Green Version]
- Wallimann, T.; Wyss, M.; Brdiczka, D.; Nicolay, K.; Eppenberger, H.M. Intracellular compartmentation, structure and function of creatine kinase isoenzymes in tissues with high and fluctuating energy demands: The ‘phosphocreatine circuit’ for cellular energy homeostasis. Biochem. J. 1992, 281 Pt 1, 21–40. [Google Scholar] [CrossRef] [Green Version]
- Wallimann, T.; Tokarska-Schlattner, M.; Schlattner, U. The creatine kinase system and pleiotropic effects of creatine. Amino Acids 2011, 40, 1271–1296. [Google Scholar] [CrossRef] [Green Version]
- Dreyer, N.; Muhlfeld, C.; Fehrenbach, A.; Pech, T.; von Berg, S.; Nagib, R.; Richter, J.; Wittwer, T.; Wahlers, T.; Ochs, M. Exogenous surfactant application in a rat lung ischemia reperfusion injury model: Effects on edema formation and alveolar type II cells. Respir. Res. 2008, 9, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, M.; Fernandez, L.G.; Doctor, A.; Sharma, A.K.; Zarbock, A.; Tribble, C.G.; Kron, I.L.; Laubach, V.E. Alveolar macrophage activation is a key initiation signal for acute lung ischemia-reperfusion injury. Am. J. Physiol. Lung Cell Mol. Physiol. 2006, 291, L1018–L1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eguiluz-Gracia, I.; Schultz, H.H.; Sikkeland, L.I.; Danilova, E.; Holm, A.M.; Pronk, C.J.; Agace, W.W.; Iversen, M.; Andersen, C.; Jahnsen, F.L.; et al. Long-term persistence of human donor alveolar macrophages in lung transplant recipients. Thorax 2016, 71, 1006–1011. [Google Scholar] [CrossRef] [Green Version]
- Kopecky, B.J.; Frye, C.; Terada, Y.; Balsara, K.R.; Kreisel, D.; Lavine, K.J. Role of donor macrophages after heart and lung transplantation. Am. J. Transplant. 2020, 20, 1225–1235. [Google Scholar] [CrossRef]
- Tatham, K.C.; O’Dea, K.P.; Romano, R.; Donaldson, H.E.; Wakabayashi, K.; Patel, B.V.; Thakuria, L.; Simon, A.R.; Sarathchandra, P.; Marczin, N.; et al. Intravascular donor monocytes play a central role in lung transplant ischaemia-reperfusion injury. Thorax 2018, 73, 350–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, L.; Zhao, X.; Zhang, B.; Kang, L.; Song, W.; Zhao, B.; Xie, W.; Chen, L.; Hu, X. Slc6a8-Mediated Creatine Uptake and Accumulation Reprogram Macrophage Polarization via Regulating Cytokine Responses. Immunity 2019, 51, 272–284.e7. [Google Scholar] [CrossRef] [PubMed]
- den Hengst, W.A.; Gielis, J.F.; Lin, J.Y.; Van Schil, P.E.; De Windt, L.J.; Moens, A.L. Lung ischemia-reperfusion injury: A molecular and clinical view on a complex pathophysiological process. Am. J. Physiol. Heart Circ. Physiol. 2010, 299, H1283–H1299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, M.; Drubbel, V.; Hendriks, J.M.; Van Schil, P.E. Red blood cell accumulation in a rat model of pulmonary ischemia/reperfusion injury. J. Cardiovasc. Surg. 2009, 50, 351–356. [Google Scholar]
- Eppinger, M.J.; Deeb, G.M.; Bolling, S.F.; Ward, P.A. Mediators of ischemia-reperfusion injury of rat lung. Am. J. Pathol. 1997, 150, 1773–1784. [Google Scholar]
- Lockinger, A.; Schutte, H.; Walmrath, D.; Seeger, W.; Grimminger, F. Protection against gas exchange abnormalities by pre-aerosolized PGE1, iloprost and nitroprusside in lung ischemia-reperfusion. Transplantation 2001, 71, 185–193. [Google Scholar] [CrossRef]
- Allison, R.C.; Kyle, J.; Adkins, W.K.; Prasad, V.R.; McCord, J.M.; Taylor, A.E. Effect of ischemia reperfusion or hypoxia reoxygenation on lung vascular permeability and resistance. J. Appl. Physiol. 1990, 69, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Bhabra, M.S.; Hopkinson, D.N.; Shaw, T.E.; Hooper, T.L. Attenuation of lung graft reperfusion injury by a nitric oxide donor. J. Thorac. Cardiovasc. Surg. 1997, 113, 327–333. [Google Scholar] [CrossRef] [Green Version]
- Jurmann, M.J.; Dammenhayn, L.; Schaefers, H.J.; Haverich, A. Pulmonary reperfusion injury: Evidence for oxygen-derived free radical mediated damage and effects of different free radical scavengers. Eur. J. Cardiothorac. Surg. 1990, 4, 665–670. [Google Scholar] [CrossRef]
- Nakamura, K.; Kageyama, S.; Kupiec-Weglinski, J.W. Innate immunity in ischemia-reperfusion injury and graft rejection. Curr. Opin. Organ. Transplant. 2019, 24, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.K.; Fernandez, L.G.; Awad, A.S.; Kron, I.L.; Laubach, V.E. Proinflammatory response of alveolar epithelial cells is enhanced by alveolar macrophage-produced TNF-alpha during pulmonary ischemia-reperfusion injury. Am. J. Physiol. Lung Cell Mol. Physiol. 2007, 293, L105–L113. [Google Scholar] [CrossRef]
- Merry, H.E.; Phelan, P.; Doaks, M.; Zhao, M.; Mulligan, M.S. Functional roles of tumor necrosis factor-alpha and interleukin 1-Beta in hypoxia and reoxygenation. Ann. Thorac. Surg. 2015, 99, 1200–1205. [Google Scholar] [CrossRef]
- Hamilton, B.C.; Kukreja, J.; Ware, L.B.; Matthay, M.A. Protein biomarkers associated with primary graft dysfunction following lung transplantation. Am. J. Physiol. Lung Cell Mol. Physiol. 2017, 312, L531–L541. [Google Scholar] [CrossRef] [Green Version]
- Strieter, R.M.; Belperio, J.A.; Keane, M.P. Cytokines in innate host defense in the lung. J. Clin. Investig. 2002, 109, 699–705. [Google Scholar] [CrossRef]
- Mittal, M.; Siddiqui, M.R.; Tran, K.; Reddy, S.P.; Malik, A.B. Reactive oxygen species in inflammation and tissue injury. Antioxid. Redox Signal. 2014, 20, 1126–1167. [Google Scholar] [CrossRef] [Green Version]
- Andrade, C.F.; Kaneda, H.; Der, S.; Tsang, M.; Lodyga, M.; Chimisso Dos Santos, C.; Keshavjee, S.; Liu, M. Toll-like receptor and cytokine gene expression in the early phase of human lung transplantation. J. Heart. Lung Transplant. 2006, 25, 1317–1323. [Google Scholar] [CrossRef]
- Andrade, C.F.; Waddell, T.K.; Keshavjee, S.; Liu, M. Innate immunity and organ transplantation: The potential role of toll-like receptors. Am. J. Transplant. 2005, 5, 969–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuzaki, Y.; Waddell, T.K.; Puskas, J.D.; Hirai, T.; Nakajima, S.; Slutsky, A.S.; Patterson, G.A. Amelioration of post-ischemic lung reperfusion injury by prostaglandin E1. Am. Rev. Respir. Dis. 1993, 148, 882–889. [Google Scholar] [CrossRef]
- Chatkin, M.; Menezes, A.M.; Albernaz, E.; Victora, C.G.; Barros, F.C. Asthmatic children’s risk factors for emergency room visits, Brazil. Rev. Saude Publica 2000, 34, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Fink, M.P. Role of reactive oxygen and nitrogen species in acute respiratory distress syndrome. Curr. Opin. Crit. Care 2002, 8, 6–11. [Google Scholar] [CrossRef]
- Katsiki, N.; Manes, C. Is there a role for supplemented antioxidants in the prevention of atherosclerosis? Clin. Nutr. 2009, 28, 3–9. [Google Scholar] [CrossRef] [PubMed]







| Weight | W 90 Mean (±SD) | Cr 90 Mean (±SD) | p | W 180 Mean (±SD) | Cr 180 Mean (±SD) | p |
|---|---|---|---|---|---|---|
| Animal (g) | 395.6 (±38.6) | 397.6 (±35.7) | 0.869 | 390.4 (±55.5) | 394.5 (±32.3) | 0.884 |
| Lung (mg) | 3040.7 (±732.9) | 3064.3 (±733.3) | 0.930 | 3176.8 (±378.8) | 3069 (±474.1) | 0.540 |
| Heart (mg) | 1203.0 (±99.8) | 1212.9 (± 119.0) | 0.807 | 1216.5 (±103.8) | 1202.7 (±101.3) | 0.724 |
| Lung Mechanics | W 90 Median (25–75%) | Cr 90 Median (25–75%) | p | W 180 Median (25–75%) | Cr 180 Median (25–75%) | p |
|---|---|---|---|---|---|---|
| Immediate reperfusion | ||||||
| RAW (cmH2O.s/mL) | 0.071 (0.06–0.11) | 0.089 (0.08–0.12) | 0.009 * | 0.089 (0.07–0.10) | 0.101 (0.08–0.11) | 0.044 * |
| GTIS (cmH2O/mL) | 0.329 (0.31–0.37) | 0.322 (0.29–0.33) | 0.038 * | 0.372 (0.31–0.38) | 0.299 (0.27–0.31) | 0.001 * |
| HTIS (cmH2O/mL) | 1.974 (1.80–2.04) | 1.650 (1.56–1.80) | 0.003 * | 1.881 (1.66–2.31) | 1.717 (1.58–1.84) | 0.021 * |
| Final reperfusion | ||||||
| RAW (cmH2O.s/mL) | 0.098 (0.07–0.15) | 0.092 (0.08–0.12) | 0.674 | 0.096 (0.07–0.15) | 0.103 (0.09–0.11) | 0.554 |
| GTIS (cmH2O/mL) | 0.359 (0.32–0.41) | 0.325 (0.29–0.35) | 0.060 | 0.361 (0.35–0.37) | 0.334 (0.29–0.35) | 0.003 * |
| HTIS (cmH2O/mL) | 2.312 (1.79–3.11) | 1.741 (1.60–2.32) | 0.021 * | 2.033 (1.69–2.51) | 1.739 (1.63–1.85) | 0.049 * |
| W 90 Mean (±SD) | Cr 90 Mean (±SD) | p | W 180 Mean (±SD) | Cr 180 Mean (±SD) | p | |
|---|---|---|---|---|---|---|
| Plasma Creatinine (mg/dL) | 0.76 (±0.04) | 0.84 (±0.07) | 0.011 * | 0.74 (±0.07) | 0.85 (±0.06) | 0.011 * |
| Blood gas | ||||||
| pCO2 (mmHg) | 32.38 (±12.06) | 17.97 (±8.79) | 0.006 * | 31.37 (±7.06) | 24.67 (±7.67) | 0.075 |
| pO2 (mmHg) | 74.18 (±23.73) | 113.70 (±25.02) | 0.002 * | 58.85 (±33.42) | 115.62 (±24.86) | 0.001 * |
| cLactate (mmol/dL) | 7.33 (±1.85) | 8.08 (±2.38) | 0.459 | 6.12 (±2.60) | 8.74 (±3.19) | 0.080 |
| Inflammatory Cells | W 90 Mean (±SD) | Cr 90 Mean (±SD) | p | W 180 Mean (±SD) | Cr 180 Mean (±SD) | p |
|---|---|---|---|---|---|---|
| Peripheral blood cells (×104 cells/mL) | ||||||
| Total cells | 122.25 (±42.82) | 64.75 (±32.47) | 0.003 * | 170.35 (±46.89) | 63.75 (±16.17) | 0.001 * |
| Neutrophils | 51.51 (±26.85) | 25.79 (±15.10) | 0.021 * | 78.16 (±47.94) | 23.98 (±9.74) | 0.022 * |
| Monocytes | 21.89 (±10.58) | 11.48 (±7.81) | 0.017 * | 26.72 (±7.34) | 10.88 (±4.93) | 0.001 * |
| Lymphocytes | 47.64 (±25.31) | 26.85 (±13.71) | 0.076 | 64.50 (±18.82) | 28.24 (±9.27) | 0.001 * |
| BALF cells (×104 cells/mL) | ||||||
| Total cells | 122.77 (±58.42) | 49.44 (±10.13) | 0.001 * | 133.12 (±75.06) | 49.44 (±14.88) | 0.001 * |
| Neutrophils | 11.32 (±10.78) | 3.86 (±1.91) | 0.017 * | 17.85 (±11.82) | 4.25 (±2.34) | 0.001 * |
| Macrophages | 85.19 (±48.84) | 33.22 (±7.60) | 0.001 * | 79.34 (±42.37) | 26.96 (±12.23) | 0.002 * |
| Lymphocytes | 14.22 (±13.82) | 5.09 (±4.39) | 0.112 | 22.79 (±24.62) | 12.68 (±6.42) | 0.810 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida, F.M.; Battochio, A.S.; Napoli, J.P.; Alves, K.A.; Balbin, G.S.; Oliveira-Junior, M.; Moriya, H.T.; Pego-Fernandes, P.M.; Vieira, R.P.; Pazetti, R. Creatine Supply Attenuates Ischemia-Reperfusion Injury in Lung Transplantation in Rats. Nutrients 2020, 12, 2765. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092765
Almeida FM, Battochio AS, Napoli JP, Alves KA, Balbin GS, Oliveira-Junior M, Moriya HT, Pego-Fernandes PM, Vieira RP, Pazetti R. Creatine Supply Attenuates Ischemia-Reperfusion Injury in Lung Transplantation in Rats. Nutrients. 2020; 12(9):2765. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092765
Chicago/Turabian StyleAlmeida, Francine M., Angela S. Battochio, João P. Napoli, Katiusa A. Alves, Grace S. Balbin, Manoel Oliveira-Junior, Henrique T. Moriya, Paulo M. Pego-Fernandes, Rodolfo P. Vieira, and Rogerio Pazetti. 2020. "Creatine Supply Attenuates Ischemia-Reperfusion Injury in Lung Transplantation in Rats" Nutrients 12, no. 9: 2765. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092765